- Subjects: Neurosciences
- |
- Contributor:
- Neuroscientifically Challenged



















































































- nerve
- medulla
- motor function
- anatomy
This video is adapted from: https://www.youtube.com/watch?v=Kmx8ZYqhGIo
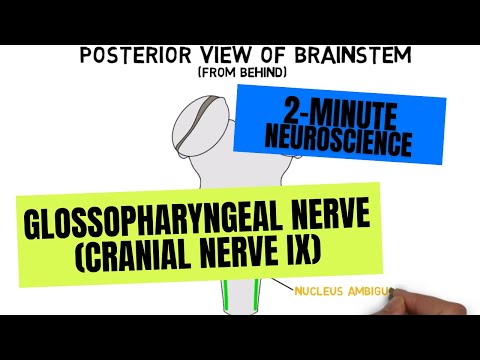
The glossopharyngeal nerve is associated with the tongue and the pharynx, or throat, and has both sensory and motor functions. It carries sensory information about touch, pain, and temperature from the posterior third of the tongue, the upper part of the throat, the tonsils, part of the outer ear, the inner surface of the eardrum, and the eustachian tube. It also conveys sensory information from the carotid body and carotid sinus, structures that detect oxygen, carbon dioxide, and ph levels in the blood along with changes in blood pressure. The nerve also conveys taste information from the posterior ⅓ of the tongue and carries motor signals to the stylopharyngeus muscle, which plays a role in swallowing and speech. And it innervates the parotid gland, the largest of our salivary glands.
The glossopharyngeal nerve is associated with a number of nuclei in the medulla. The fibers that supply the stylopharyngeus muscle originate in the nucleus ambiguus. The sensory fibers that carry taste information, and those that carry sensory information from the carotid body and carotid sinus, synapse in the nucleus solitarius, and the fibers that convey touch and pain synapse in the spinal trigeminal nucleus. The fibers that innervate the parotid gland arise from the inferior salivatory nucleus.
Damage to the glossopharyngeal nerve can cause a variety of symptoms, including a loss of taste on the posterior ⅓ of the tongue, trouble swallowing, and generally decreased sensation on the back of the tongue, the soft palate, and pharynx. Patients may also have a diminished gag reflex, and the uvula will often deviate to the side opposite from where the damage has occurred. In rare cases, patients may experience glossopharyngeal neuralgia, which involves brief but intense pain in the tongue and throat.[1]
- Wilson-Pauwels L, Akesson EJ, Stewart PA, Spacey SD. Cranial Nerves in Health and Disease. 2nd ed. London: BC Decker, Inc; 2002.