- Subjects: Neurosciences
- |
- Contributor:
- Neuroscientifically Challenged
































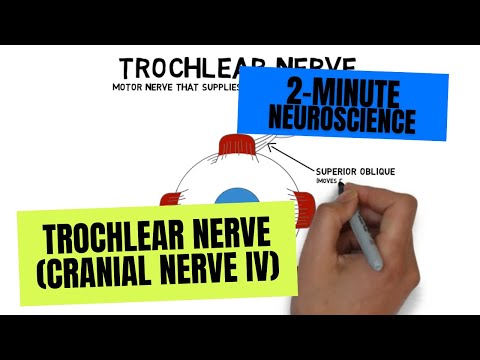



















































- oculomotor nerve
- extraocular muscles
The oculomotor nerve is responsible for supplying 4 of the 6 extraocular muscles: the medial rectus, which moves the eye towards the nose; the superior rectus, which moves the eye upwards; the inferior rectus, which moves the eye downwards; and the inferior oblique, which moves the eye up and out. Additionally, the nerve supplies the levator palpebrae superioris, which is the muscle that elevates the eyelid. It also forms connections with neurons in the ciliary ganglion, which innervate the pupillary sphincter to control the constriction of the pupil and the ciliary muscle, which adjusts the shape of the lens to see clearly at close distances.
Oculomotor nerve fibers originate in the oculomotor nucleus in the midbrain. From here, they travel to the orbit of the eye, along the way separating into branches that control the different extraocular muscles. The fibers that control the pupillary sphincter and ciliary muscle originate in the Edinger-Westphal nucleus and travel with the oculomotor nerve.
Damage to the oculomotor nerve causes deficits in the ipsilateral eye. A common symptom is a deviation of the affected eye to the side and downwards due to the paralysis of the medial rectus and inferior oblique, and the unopposed action of the unaffected extraocular muscles. Medial eye movements may also be impaired due to paralysis of the medial rectus, and vertical eye movements may be impaired due to the paralysis of the superior and inferior recti and inferior oblique. Diplopia, or double-vision, is common. Ptosis, or drooping of the eyelid may occur due to the paralysis of the levator palpebrae superioris. Because the pupillary constriction muscle is impaired, the pupil on the side of the damage may remain dilated, a condition known as mydriasis. And the patient may have a difficult time focusing the lens for close-up vision due to effects on the ciliary muscle. [1]
- Vanderah TW, Gould DJ. Nolte's The Human Brain. 7th ed. Philadelphia, PA: Elsevier; 2016.