Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Cristina Maria Marginean | -- | 1703 | 2023-07-14 09:56:42 | | | |
| 2 | Fanny Huang | Meta information modification | 1703 | 2023-07-17 08:06:56 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Marginean, C.M.; Pirscoveanu, D.; Popescu, M.; Vasile, C.M.; Docea, A.O.; Mitruț, R.; Mărginean, I.C.; Iacob, G.A.; Firu, D.M.; Mitruț, P. Etiological Factors of Acute on Chronic Liver Failure. Encyclopedia. Available online: https://encyclopedia.pub/entry/46804 (accessed on 23 July 2026).
Marginean CM, Pirscoveanu D, Popescu M, Vasile CM, Docea AO, Mitruț R, et al. Etiological Factors of Acute on Chronic Liver Failure. Encyclopedia. Available at: https://encyclopedia.pub/entry/46804. Accessed July 23, 2026.
Marginean, Cristina Maria, Denisa Pirscoveanu, Mihaela Popescu, Corina Maria Vasile, Anca Oana Docea, Radu Mitruț, Iulia Cristina Mărginean, George Alexandru Iacob, Dan Mihai Firu, Paul Mitruț. "Etiological Factors of Acute on Chronic Liver Failure" Encyclopedia, https://encyclopedia.pub/entry/46804 (accessed July 23, 2026).
Marginean, C.M., Pirscoveanu, D., Popescu, M., Vasile, C.M., Docea, A.O., Mitruț, R., Mărginean, I.C., Iacob, G.A., Firu, D.M., & Mitruț, P. (2023, July 14). Etiological Factors of Acute on Chronic Liver Failure. In Encyclopedia. https://encyclopedia.pub/entry/46804
Marginean, Cristina Maria, et al. "Etiological Factors of Acute on Chronic Liver Failure." Encyclopedia. Web. 14 July, 2023.
Copy Citation
Acute-on-chronic liver failure (ACLF) is a syndrome characterized by acute and severe decompensation of chronic liver disease (CLD) correlated with multiple organ failure, poor prognosis, and increased mortality. In 40–50% of ACLF cases, the trigger is not recognized; for many of these patients, bacterial translocation associated with systemic inflammation is thought to be the determining factor; in the other 50% of patients, sepsis, alcohol consumption, and reactivation of chronic viral hepatitis are the most frequently described trigger factors. Other conditions considered precipitating factors are less common, including acute alcoholic hepatitis, major surgery, TIPS insertion, or inadequate paracentesis without albumin substitution.
acute-on-chronic liver failure
liver cirrhosis
gut microbiome
1. Introduction
Acute-on-chronic liver failure (ACLF) represents a condition characterized by acute decompensation of underlying chronic liver disease (CLD) correlated with multiple organ failure, poor prognosis, and increased mortality.
The EASL (European Association for the Study of the Liver), NACSELD (North American Consortium for the Study of End-Stage Liver Disease), and APASL (Asia Pacific Association for the Study of the Liver) have proposed different definitions of ACLF syndrome; all are based on clinical features, associated with alterations of biological liver tests combined with organ failure [1][2].
More than 13 distinct definitions of ACLF have been advanced so far, but the definitions from APASL and the European Association for the Study of Chronic Liver Failure (EASL-CLIF) Consortium are universally recognized [3][4].
Thus, the consensus of the Asia-Pacific Association for the Study of the Liver (APASL) defined ACLF as acute liver injury manifested by jaundice (total bilirubin ≥ 5 mg/dL) and coagulopathy (INR ≥ 1.5), which evolves within four weeks with ascites with/without encephalopathy in a patient previously diagnosed with CLD.
According to the EASL-CLIF criteria, ACLF emerges in patients with previously compensated or decompensated liver cirrhosis who develop other organ failures. The EASL-CLIF criteria exclude patients previously diagnosed with HCC (hepatocellular carcinoma), HIV (Human Immunodeficiency Virus), or severe comorbidities [5]. The EASL-CLIF criteria, compared to the NACLSELD and APASL criteria, define a relatively enlarged spectrum of disease severities, including ACLF disease phases with better prognosis (phases 1/2) and outcomes, as well as advanced phases with multiple organ failure, high short-term mortality, and poor prognosis [4][6].
The NACSELD criteria were defined initially for patients hospitalized with decompensated cirrhosis and bacterial infections, excluding previous malignancies, HIV, or previous organ transplantation [5]. These criteria completed the EASL-CLIF criteria; therefore, ACLF was defined by the presence of at least two extrahepatic organ failures, including shock, the need for vasopressors despite adequate intravenous fluid therapy, encephalopathy stage 3/4, renal replacement, and/or mechanical ventilation [1]. The NACSELD definition does not differentiate between distinct disease phases and stages of ACLF, so it may underdiagnose ACLF.
The APASL criteria used a wide disease spectrum focusing on liver failure as central to the ACLF definition [2]. The APASL and ACLF definitions were derived from acute liver failure, which develops in patients with preexisting chronic liver disease or liver cirrhosis, but these definitions exclude patients with decompensated cirrhosis or a history of infection [3][5]. Therefore, patients with acute hepatic injury, such as reactivation of viral hepatitis, drug-induced liver injury, or surgical procedures, and those with cirrhosis without any previous infections or variceal hemorrhage meet the APASL ACLF criteria if these factors can lead to jaundice and coagulopathy and are followed by ascites or hepatic encephalopathy within four weeks. Although the APASL definition presumes the existence of underlying chronic liver disease, unlike the EASL-CLIF criteria, it does not distinguish between ACLF with or without cirrhosis [5][7].
Despite the worldwide diversity of ACLF definitions related to diagnosis, precipitating factors, underlying comorbidities, organ failure, and management, patients with ACLF have an invariably poor prognosis. The most recently and exhaustive guideline for the current data in ACLF was elaborated in 2022 by Bajaj et al., and it represents the official practice recommendation of the American College of Gastroenterology, being structured on statements considered useful and clinically relevant. The guideline provides a list of recommendations regarding definitions, diagnosis, key pathogenetic mechanisms, precipitating factors, and a complex therapeutic approach [5].
2. Etiological Factors of ACLF
In 40–50% of ACLF cases, the trigger has not been recognized. For many of these patients, bacterial translocation and systemic inflammation are thought to be the determining factors [8]; in the other 50% of patients, sepsis, alcohol consumption, and reactivation of chronic viral hepatitis (B, C, E) [2] are the most described precipitating factors. Other precipitating conditions are less common (approximately 8%), including acute alcoholic hepatitis, surgery, or TIPS insertion. Paracentesis without albumin substitution has also been described [4][9]. The main acute precipitating factors in ACLF, according to Gawande et al., are listed in Table 1 [10].
Table 1. Acute precipitating factors in ACLF (adaptation after Gawande et al. [10]).
| Precipitating Factor | Prevalence |
|---|---|
| Alcohol | 48.08% |
| Sepsis | 16.35% |
| Gastrointestinal bleeding | 19.13% |
| HBV | 8.2% |
| HEV | 7.21% |
| Tuberculostatic treatment | 6.25% |
| Autoimmune hepatitis | 0.96% |
| Unknown | 3.85% |
Evidence on ACLF caused by acute hepatic insults of a viral etiology is still being researched, further studies being essential for a concluding evaluation of etiology, outcome, organ failure, and mortality predictors. Hepatitis viruses are some of the main etiological factors for acute hepatic insults resulting in ACLF. Hepatotropic viral infections include hepatitis B virus reactivation, (HBV) superinfection with hepatitis A virus (HAV), hepatitis E virus (HEV), or more rarely, reactivation of HCV infection.
HBV reactivation has been recognized as a common factor involved in ACLF development [11][12][13]. Studies have suggested that 15–37% of patients with HBV infection develop acute exacerbations within four years [14], as well as episodes of ACLF; the mortality rate for these patients is between 30% and 70% [4][15]. In the Asia-Pacific region, hepatitis B appears to be the most common cause of ACLF. In China, 80% of ACLF cases are due to hepatitis B, and reactivation of HBV as an acute hepatic insult is found in more than 50% of cases [16].
HAV infection can occasionally cause liver failure in patients with or without preexisting chronic liver disease. Over time, a series of studies highlighted HAV as an acute insult in ACLF and provided evidence of increased short-term mortality [2][17].
Agrawal et al. reported the presence of ACLF and HAV as an acute insult that occurred in patients with underlying liver cirrhosis secondary to NAFLD (non-alcoholic fatty liver disease) [18]. Kahraman et al. also reported a human immunodeficiency virus (HIV)-positive case in a patient who developed ACLF due to an acute HAV infection with liver cirrhosis due to NAFLD [19]. Duseja et al. emphasized that HAV infection in patients with the pre-existing chronic liver disease could be responsible for worsening ACLF [20].
Other authors have investigated the role of HAV infection in patients with chronic hepatitis or liver cirrhosis secondary to HBV infection, suggesting that the association of HAV superinfection with HBV patients occasionally leads to ACLF, in HBV patients both with and without liver cirrhosis [21][22][23]. Some studies have associated HAV infection in HCV infection with increased mortality [24][25], although there have been several contrary opinions suggesting that HAV superinfection is associated with decreased HCV replication, which could lead to HCV clearance. [26][27][28].
Therefore, it is currently suggested that HAV infection, as an acute insult, precipitates the development of ACLF in patients with any chronic liver disease, especially liver cirrhosis, an important role being apparently attributed to host genetic factors determining different individual susceptibility [29][30].
Many studies have reported HEV as one of the leading causes of ACLF in Asia and Africa, where HEV is endemic. The mortality rate of HEV-related ACLF is nearly 35% [31]. HEV-related acute hepatitis in patients having underlying cirrhosis may complicate and worsen the primary disease and can result in ACLF. A majority of these patients may need early transplantation [32][33][34].
The evidence that, generally, HCV infection rarely causes ACLF has been supported by numerous previous studies [35][36][37][38][39][40], but a reactivation of HCV infection is recognized to be one of the precipitating factors in ACLF induction [9], considering the possibility that an acute HCV infection can result in acute fulminant liver failure [3][41][42][43].
Bacterial products, such as muramyl-dipeptides, bacterial DNA, lipopolysaccharides, and peptidoglycans, are translocated from a permeable intestine into the blood continuously or discontinuously; therefore, they could initiate initial organ dysfunction [44]. Bacterial translocation, the most important trigger of systemic inflammation, relies on the existence of ascites [45].
Gastrointestinal bleeding is also a precipitating factor in triggering ACLF. Patients with ACLF have a significantly increased bleeding history compared to patients without ACLF [46][47]. Rebleeding doubles the risk of ACLF, and these patients present a very high risk of death, so TIPS insertion could notably improve outcomes in critically decompensated cirrhotic patients [47][48][49]; therefore, TIPS has been recommended by the recent international guidelines and Baveno [50][51].
Host response is likely the main factor in determining ACLF severity and prognosis. The host immune reaction and the inflammatory cascade are of significance in this condition. The similarity between systemic inflammation determined by sepsis and ACLF motivates the idea that both conditions could have similar pathogenic mechanisms. Comparing patients with sepsis and patients with ACLF, Wasmuth et al. [52] formulated the hypothesis of “sepsis-like immune paralysis” based on extremely reduced TNF-α pro-duction and decreased HLA-DR monocyte expression in patients with both sepsis and ACLF, with this cellular immune damage contributing to high mortality.
Current studies have identified that ACLF can occur in patients with both compensated and decompensated cirrhosis, as well as in patients with previous CLD without cirrhosis. Table 2 presents the prevalence of ACLF in different CLD etiologies, according to data published in an exhaustive study conducted in 80,389 patients by Mahmud et al. [53].
Table 2. Prevalence of ACLF based on etiology of CLD (according to data published by Mahmud et al. [53]).
| Etiology | Total Patients | ACLF |
|---|---|---|
| Hepatitis C | 13,959 | 809 (5.79%) |
| Hepatitis B | 1967 | 145 (7.37%) |
| Alcohol | 23,484 | 1798 (7.65%) |
| Hepatitis C + Alcohol | 22,343 | 1791 (8.01%) |
| NAFLD | 15,893 | 929 (5.84%) |
| Other | 2737 | 181 (6.61%) |
NAFLD, non-alcoholic fatty liver disease.
The World Gastroenterology Organization (WGO) formulated a classification of ACLF relying on the underlying liver disease: patients with underlying CLD and non-cirrhotic ACLF type A; patients with prior compensated cirrhosis and ACLF type B; and patients with prior decompensated cirrhosis and ACLF type C (Figure 1) [54][55].
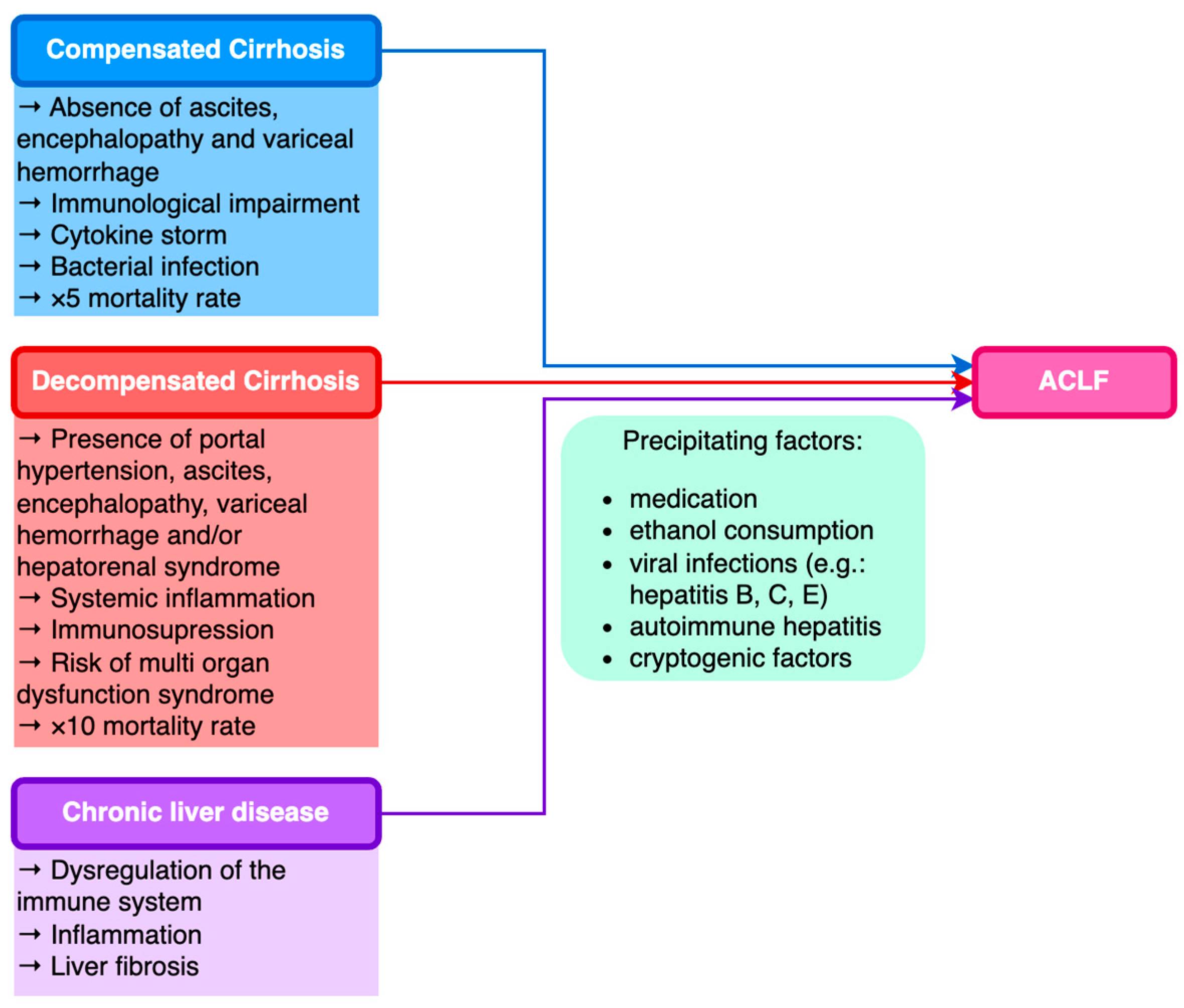
Figure 1. Classification of ACLF based on underlying chronic liver disease.
Recent studies have revealed that ACLF represents 5% of all patients suffering from liver cirrhosis who are hospitalized, the average cost of hospitalization for these patients being three times higher than the cost for cirrhotic patients without complications and approximately five times higher than the cost for patients hospitalized for heart failure [56].
The global mortality rate according to EASL-CLIF is 30% to 50%. Mortality rates in the United States, according to NACSELD in decompensated patients, were 27%, 49%, 64%, and 77%, the percentage increasing directly with the number of organs affected (1, 2, 3, or 4 organ failures, respectively) [57][58].
References
- O’Leary, J.G.; Reddy, K.R.; Garcia-Tsao, G.; Biggins, S.W.; Wong, F.; Fallon, M.B.; Subramanian, R.M.; Kamath, P.S.; Thuluvath, P.; Vargas, H.E.; et al. NACSELD Acute-on-Chronic Liver Failure (NACSELD-ACLF) Score Predicts 30-Day Survival in Hospitalized Patients with Cirrhosis. Hepatology 2018, 67, 2367–2374.
- Sarin, S.K.; Choudhury, A.; Sharma, M.K.; Maiwall, R.; Al Mahtab, M.; Rahman, S.; Saigal, S.; Saraf, N.; Soin, A.S.; Devarbhavi, H.; et al. Acute-on-Chronic Liver Failure: Consensus Recommendations of the Asian Pacific Association for the Study of the Liver (APASL): An Update. Hepatol. Int. 2019, 13, 353–390.
- Sarin, S.K.; Kedarisetty, C.K.; Abbas, Z.; Amarapurkar, D.; Bihari, C.; Chan, A.C.; Chawla, Y.K.; Dokmeci, A.K.; Garg, H.; Ghazinyan, H.; et al. Acute-on-Chronic Liver Failure: Consensus Recommendations of the Asian Pacific Association for the Study of the Liver (APASL) 2014. Hepatol. Int. 2014, 8, 453–471.
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-Chronic Liver Failure Is a Distinct Syndrome That Develops in Patients with Acute Decompensation of Cirrhosis. Gastroenterology 2013, 144, 1426–1437.
- Bajaj, J.S.; O’Leary, J.G.; Lai, J.C.; Wong, F.; Long, M.D.; Wong, R.J.; Kamath, P.S. Acute-on-Chronic Liver Failure Clinical Guidelines. Off. J. Am. Coll. Gastroenterol. ACG 2022, 117, 225.
- Engelmann, C.; Thomsen, K.L.; Zakeri, N.; Sheikh, M.; Agarwal, B.; Jalan, R.; Mookerjee, R.P. Validation of CLIF-C ACLF Score to Define a Threshold for Futility of Intensive Care Support for Patients with Acute-on-Chronic Liver Failure. Crit. Care 2018, 22, 254.
- Engelmann, C.; Berg, T. Clinical Practice Guidelines for Acute-on-Chronic Liver Failure: Are We Ready for Reaching Global Consensus? Hepatobiliary Surg. Nutr. 2023, 12, 239–243.
- Trebicka, J.; Reiberger, T.; Laleman, W. Gut-Liver Axis Links Portal Hypertension to Acute-on-Chronic Liver Failure. Visc. Med. 2018, 34, 270–275.
- Kim, T.Y.; Kim, D.J. Acute-on-Chronic Liver Failure. Clin. Mol. Hepatol. 2013, 19, 349–359.
- Gawande, A.; Gupta, G.K.; Gupta, A.; Wanjari, S.J.; Goel, V.; Rathore, V.; Bhardwaj, H.; Nijhawan, S. Acute-on-Chronic Liver Failure: Etiology of Chronic and Acute Precipitating Factors and Their Effect on Mortality. J. Clin. Exp. Hepatol. 2019, 9, 699–703.
- Li, H.; Chen, L.-Y.; Zhang, N.; Li, S.-T.; Zeng, B.; Pavesi, M.; Amorós, À.; Mookerjee, R.P.; Xia, Q.; Xue, F.; et al. Characteristics, Diagnosis and Prognosis of Acute-on-Chronic Liver Failure in Cirrhosis Associated to Hepatitis B. Sci. Rep. 2016, 6, 25487.
- Yin, S.; Wang, S.J.; Gu, W.Y.; Zhang, Y.; Chen, L.Y.; Li, H. Risk of Different Precipitating Events for Progressing to Acute-on-Chronic Liver Failure in HBV-Related Cirrhotic Patients. J. Dig. Dis. 2017, 18, 292–301.
- Shi, Y.; Yang, Y.; Hu, Y.; Wu, W.; Yang, Q.; Zheng, M.; Zhang, S.; Xu, Z.; Wu, Y.; Yan, H.; et al. Acute-on-chronic Liver Failure Precipitated by Hepatic Injury Is Distinct from That Precipitated by Extrahepatic Insults. Hepatology 2015, 62, 232.
- Kumar, M.; Chauhan, R.; Gupta, N.; Hissar, S.; Sakhuja, P.; Sarin, S.K. Spontaneous Increases in Alanine Aminotransferase Levels in Asymptomatic Chronic Hepatitis B Virus-Infected Patients. Gastroenterology 2009, 136, 1272–1280.
- Sarin, S.K.; Kumar, A.; Almeida, J.A.; Chawla, Y.K.; Fan, S.T.; Garg, H.; de Silva, H.J.; Hamid, S.S.; Jalan, R.; Komolmit, P.; et al. Acute-on-Chronic Liver Failure: Consensus Recommendations of the Asian Pacific Association for the Study of the Liver (APASL). Hepatol. Int. 2009, 3, 269–282.
- Wan, Z.; Wu, Y.; Yi, J.; You, S.; Liu, H.; Sun, Z.; Zhu, B.; Zang, H.; Li, C.; Liu, F.; et al. Combining Serum Cystatin C with Total Bilirubin Improves Short-Term Mortality Prediction in Patients with HBV-Related Acute-On-Chronic Liver Failure. PLoS ONE 2015, 10, e0116968.
- Radha Krishna, Y.; Saraswat, V.A.; Das, K.; Himanshu, G.; Yachha, S.K.; Aggarwal, R.; Choudhuri, G. Clinical Features and Predictors of Outcome in Acute Hepatitis A and Hepatitis E Virus Hepatitis on Cirrhosis. Liver Int. 2009, 29, 392–398.
- Agrawal, S.; Rana, B.S.; Mitra, S.; Duseja, A.; Das, A.; Dhiman, R.K.; Chawla, Y. A Case of Acute-on-Chronic Liver Failure (ACLF) Due to An Uncommon Acute And Chronic Event. J. Clin. Exp. Hepatol. 2018, 8, 95–97.
- Kahraman, A.; Miller, M.; Gieseler, R.K.; Gerken, G.; Scolaro, M.J.; Canbay, A. Non-Alcoholic Fatty Liver Disease in HIV-Positive Patients Predisposes for Acute-on-Chronic Liver Failure: Two Cases. Eur. J. Gastroenterol. Hepatol. 2006, 18, 101.
- Duseja, A.; Chawla, Y.K.; Dhiman, R.K.; Kumar, A.; Choudhary, N.; Taneja, S. Non-Hepatic Insults Are Common Acute Precipitants in Patients with Acute on Chronic Liver Failure (ACLF). Dig. Dis. Sci. 2010, 55, 3188–3192.
- Zhang, X.; Ke, W.; Xie, J.; Zhao, Z.; Xie, D.; Gao, Z. Comparison of Effects of Hepatitis E or A Viral Superinfection in Patients with Chronic Hepatitis B. Hepatol. Int. 2010, 4, 615–620.
- Fu, J.; Guo, D.; Gao, D.; Huang, W.; Li, Z.; Jia, B. Clinical Analysis of Patients Suffering from Chronic Hepatitis B Superinfected with Other Hepadnaviruses. J. Med. Virol. 2016, 88, 1003–1009.
- Beisel, C.; Addo, M.M.; Schulze zur Wiesch, J. Seroconversion of HBsAG Coincides with Hepatitis A Super-Infection: A Case Report. World J. Clin. Cases 2020, 8, 1651–1655.
- Spada, E.; Genovese, D.; Tosti, M.E.; Mariano, A.; Cuccuini, M.; Proietti, L.; Giuli, C.D.; Lavagna, A.; Crapa, G.E.; Morace, G.; et al. An Outbreak of Hepatitis A Virus Infection with a High Case-Fatality Rate among Injecting Drug Users. J. Hepatol. 2005, 43, 958–964.
- Lefilliatre, P.; Villeneuve, J.-P. Fulminant Hepatitis A in Patients with Chronic Liver Disease. Can. J. Public Health 2000, 91, 168–170.
- Sagnelli, E.; Coppola, N.; Pisaturo, M.; Pisapia, R.; Onofrio, M.; Sagnelli, C.; Catuogno, A.; Scolastico, C.; Piccinino, F.; Filippini, P. Clinical and Virological Improvement of Hepatitis B Virus—Related or Hepatitis C Virus—Related Chronic Hepatitis with Concomitant Hepatitis A Virus Infection. Clin. Infect. Dis. 2006, 42, 1536–1543.
- Deterding, K.; Tegtmeyer, B.; Cornberg, M.; Hadem, J.; Potthoff, A.; Böker, K.H.W.; Tillmann, H.L.; Manns, M.P.; Wedemeyer, H. Hepatitis A Virus Infection Suppresses Hepatitis C Virus Replication and May Lead to Clearance of HCV. J. Hepatol. 2006, 45, 770–778.
- Cacopardo, B.; Nunnari, G.; Nigro, L. Clearance of HCV RNA Following Acute Hepatitis A Superinfection. Dig. Liver Dis. 2009, 41, 371–374.
- Kashyap, P.; Deka, M.; Medhi, S.; DUTTA, S.; Kashyap, K.; Kumari, N. Association of Toll-like Receptor 4 with Hepatitis A Virus Infection in Assam. Acta Virol. 2018, 62, 58–62.
- Rubicz, R.; Yolken, R.; Drigalenko, E.; Carless, M.A.; Dyer, T.D.; Kent Jr, J.; Curran, J.E.; Johnson, M.P.; Cole, S.A.; Fowler, S.P.; et al. Genome-Wide Genetic Investigation of Serological Measures of Common Infections. Eur. J. Hum. Genet. 2015, 23, 1544–1548.
- Kumar, A.; Saraswat, V.A. Hepatitis E and Acute-on-Chronic Liver Failure. J. Clin. Exp. Hepatol. 2013, 3, 225–230.
- Choi, J.W.; Son, H.J.; Lee, S.S.; Jeon, H.; Cho, J.-K.; Kim, H.J.; Cha, R.R.; Lee, J.M.; Kim, H.J.; Jung, W.T.; et al. Acute Hepatitis E Virus Superinfection Increases Mortality in Patients with Cirrhosis. BMC Infect. Dis. 2022, 22, 62.
- Kmush, B.; Wierzba, T.; Krain, L.; Nelson, K.; Labrique, A.B. Epidemiology of Hepatitis E in Low- and Middle-Income Countries of Asia and Africa. Semin. Liver Dis. 2013, 33, 015–029.
- Artru, F.; Louvet, A.; Ruiz, I.; Levesque, E.; Labreuche, J.; Ursic-Bedoya, J.; Lassailly, G.; Dharancy, S.; Boleslawski, E.; Lebuffe, G.; et al. Liver Transplantation in the Most Severely Ill Cirrhotic Patients: A Multicenter Study in Acute-on-Chronic Liver Failure Grade 3. J. Hepatol. 2017, 67, 708–715.
- Kanda, T.; Matsumoto, N.; Ishii, T.; Arima, S.; Shibuya, S.; Honda, M.; Sasaki-Tanaka, R.; Masuzaki, R.; Kanezawa, S.; Nishizawa, T.; et al. Chronic Hepatitis C: Acute Exacerbation and Alanine Aminotransferase Flare. Viruses 2023, 15, 183.
- Kanda, T.; Yokosuka, O.; Imazeki, F.; Saisho, H. Acute Hepatitis C Virus Infection, 1986-2001: A Rare Cause of Fulminant Hepatitis in Chiba, Japan. Hepatogastroenterology 2004, 51, 556–558.
- Liang, T.J.; Jeffers, L.; Reddy, R.K.; Silva, M.O.; Cheinquer, H.; Findor, A.; De Medina, M.; Yarbough, P.O.; Reyes, G.R.; Schiff, E.R. Fulminant or Subfulminant Non-A, Non-B Viral Hepatitis: The Role of Hepatitis C and E Viruses. Gastroenterology 1993, 104, 556–562.
- Jain, A.; Kar, P.; Madan, K.; Das, U.P.; Budhiraja, S.; Gopalkrishna, V.; Sharma, J.K.; Das, B.C. Hepatitis C Virus Infection in Sporadic Fulminant Viral Hepatitis in North India: Cause or Co-Factor? Eur. J. Gastroenterol. Hepatol. 1999, 11, 1231–1237.
- Maheshwari, A.; Ray, S.; Thuluvath, P.J. Acute Hepatitis C. Lancet 2008, 372, 321–332.
- Rao, A.; Rule, J.A.; Cerro-Chiang, G.; Stravitz, R.T.; McGuire, B.M.; Lee, G.; Fontana, R.J.; Lee, W.M. Role of Hepatitis C Infection in Acute Liver Injury/Acute Liver Failure in North America. Dig. Dis. Sci. 2023, 68, 304–311.
- Younis, B.B.; Arshad, R.; Khurhsid, S.; Masood, J.; Nazir, F.; Tahira, M. Fulminant Hepatic Failure (FHF) Due to Acute Hepatitis C. Pak. J. Med. Sci. 2015, 31, 1009–1011.
- Sagnelli, E.; Pisaturo, M.; Stanzione, M.; Messina, V.; Alessio, L.; Sagnelli, C.; Starace, M.; Pasquale, G.; Coppola, N. Clinical Presentation, Outcome, and Response to Therapy among Patients with Acute Exacerbation of Chronic Hepatitis C. Clin. Gastroenterol. Hepatol. 2013, 11, 1174–1180.e11.
- Thiel, A.M.; Rissland, J.; Lammert, F.; Casper, M. Acute liver failure as a rare case of a frequent disease. Z. Gastroenterol. 2018, 56, 255–258.
- Trebicka, J.; Amoros, A.; Pitarch, C.; Titos, E.; Alcaraz-Quiles, J.; Schierwagen, R.; Deulofeu, C.; Fernandez-Gomez, J.; Piano, S.; Caraceni, P.; et al. Addressing Profiles of Systemic Inflammation Across the Different Clinical Phenotypes of Acutely Decompensated Cirrhosis. Front. Immunol. 2019, 10, 476.
- Wiest, R.; Lawson, M.; Geuking, M. Pathological Bacterial Translocation in Liver Cirrhosis. J. Hepatol. 2014, 60, 197–209.
- Trebicka, J.; Gu, W.; Ibáñez-Samaniego, L.; Hernández-Gea, V.; Pitarch, C.; Garcia, E.; Procopet, B.; Giráldez, Á.; Amitrano, L.; Villanueva, C.; et al. Rebleeding and Mortality Risk Are Increased by ACLF but Reduced by Pre-Emptive TIPS. J. Hepatol. 2020, 73, 1082–1091.
- Costa, D.; Simbrunner, B.; Jachs, M.; Hartl, L.; Bauer, D.; Paternostro, R.; Schwabl, P.; Scheiner, B.; Stättermayer, A.F.; Pinter, M.; et al. Systemic Inflammation Increases across Distinct Stages of Advanced Chronic Liver Disease and Correlates with Decompensation and Mortality. J. Hepatol. 2021, 74, 819–828.
- Hernández-Gea, V.; Procopet, B.; Giráldez, Á.; Amitrano, L.; Villanueva, C.; Thabut, D.; Ibañez-Samaniego, L.; Silva-Junior, G.; Martinez, J.; Genescà, J.; et al. Preemptive-TIPS Improves Outcome in High-Risk Variceal Bleeding: An Observational Study. Hepatology 2019, 69, 282–293.
- Kumar, R.; Kerbert, A.J.C.; Sheikh, M.F.; Roth, N.; Calvao, J.A.F.; Mesquita, M.D.; Barreira, A.I.; Gurm, H.S.; Ramsahye, K.; Mookerjee, R.P.; et al. Determinants of Mortality in Patients with Cirrhosis and Uncontrolled Variceal Bleeding. J. Hepatol. 2021, 74, 66–79.
- European Association for the Study of the Liver. Electronic address: ; European Association for the Study of the Liver EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis. J. Hepatol. 2018, 69, 406–460.
- Gerbes, A.L.; Labenz, J.; Appenrodt, B.; Dollinger, M.; Gundling, F.; Gülberg, V.; Holstege, A.; Lynen-Jansen, P.; Steib, C.J.; Trebicka, J.; et al. Aktualisierte S2k-Leitlinie der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten (DGVS) „Komplikationen der Leberzirrhose“: AWMF-Nr.: 021-017. Z. Gastroenterol. 2019, 57, 611–680.
- Wasmuth, H.E.; Kunz, D.; Yagmur, E.; Timmer-Stranghöner, A.; Vidacek, D.; Siewert, E.; Bach, J.; Geier, A.; Purucker, E.A.; Gressner, A.M.; et al. Patients with Acute on Chronic Liver Failure Display ‘Sepsis-like’ Immune Paralysis. J. Hepatol. 2005, 42, 195–201.
- Mahmud, N.; Kaplan, D.E.; Taddei, T.H.; Goldberg, D.S. Incidence and Mortality of Acute-on-Chronic Liver Failure Using Two Definitions in Patients with Compensated Cirrhosis. Hepatology 2019, 69, 2150–2163.
- Jalan, R.; Yurdaydin, C.; Bajaj, J.S.; Acharya, S.K.; Arroyo, V.; Lin, H.-C.; Gines, P.; Kim, W.R.; Kamath, P.S. Toward an Improved Definition of Acute-on-Chronic Liver Failure. Gastroenterology 2014, 147, 4–10.
- Wlodzimirow, K.A.; Eslami, S.; Abu-Hanna, A.; Nieuwoudt, M.; Chamuleau, R.A.F.M. A Systematic Review on Prognostic Indicators of Acute on Chronic Liver Failure and Their Predictive Value for Mortality. Liver Int. 2013, 33, 40–52.
- Singer, C.E.; Vasile, C.M.; Popescu, M.; Popescu, A.I.S.; Marginean, I.C.; Iacob, G.A.; Popescu, M.D.; Marginean, C.M. Role of Iron Deficiency in Heart Failure—Clinical and Treatment Approach: An Overview. Diagnostics 2023, 13, 304.
- Avolio, A.W.; Gaspari, R.; Teofili, L.; Bianco, G.; Spinazzola, G.; Soave, P.M.; Paiano, G.; Francesconi, A.G.; Arcangeli, A.; Nicolotti, N.; et al. Postoperative Respiratory Failure in Liver Transplantation: Risk Factors and Effect on Prognosis. PLoS ONE 2019, 14, e0211678.
- Mattos, D.Â.Z.; Mattos, D.A.A. Letter to the Editor: Acute-on-Chronic Liver Failure: Conceptual Divergences. Hepatology 2019, 70, 1076.
More
Information
Subjects:
Gastroenterology & Hepatology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.3K
Entry Collection:
Gastrointestinal Disease
Revisions:
2 times
(View History)
Update Date:
17 Jul 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No