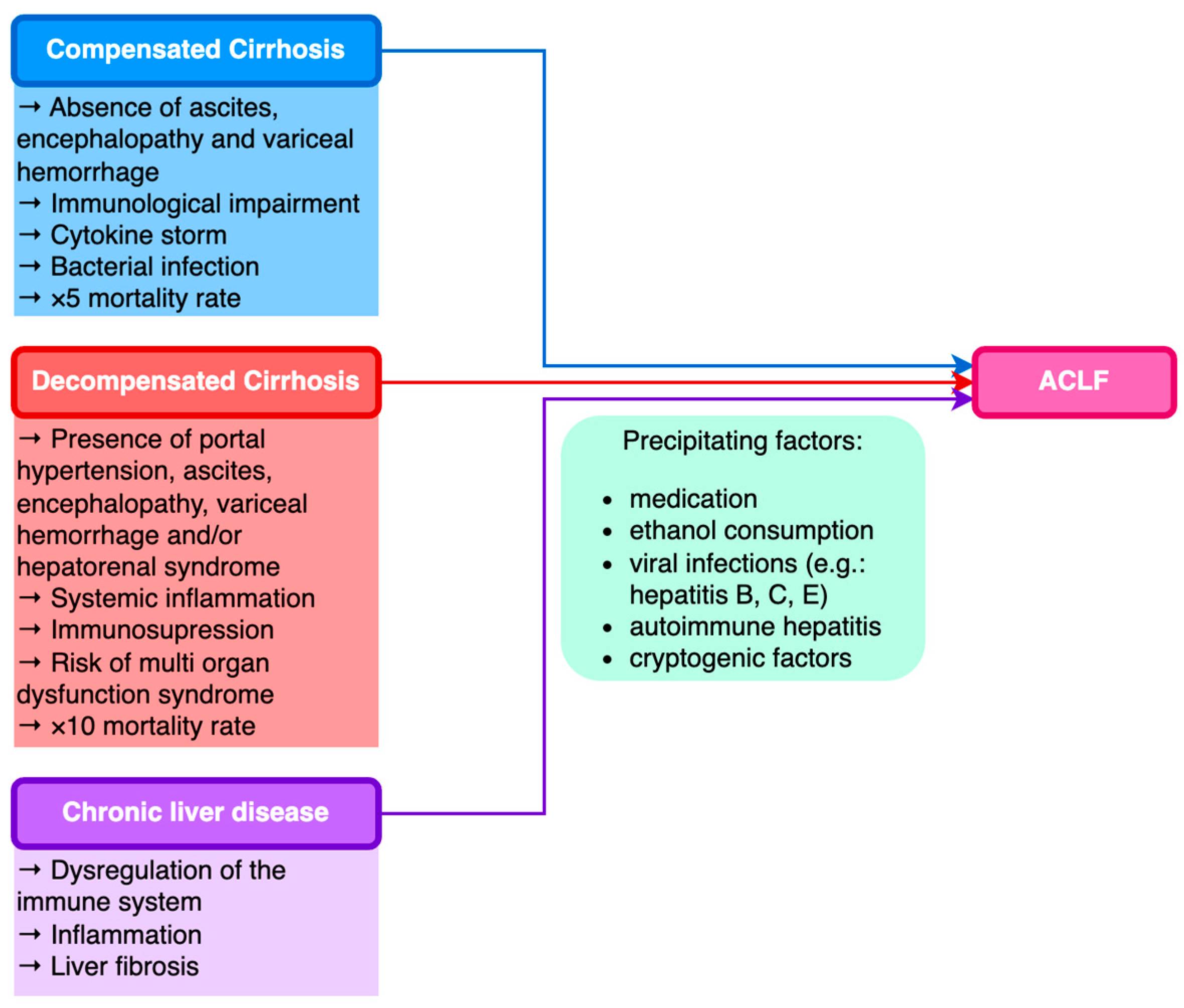
Acute-on-chronic liver failure (ACLF) is a syndrome characterized by acute and severe decompensation of chronic liver disease (CLD) correlated with multiple organ failure, poor prognosis, and increased mortality. In 40–50% of ACLF cases, the trigger is not recognized; for many of these patients, bacterial translocation associated with systemic inflammation is thought to be the determining factor; in the other 50% of patients, sepsis, alcohol consumption, and reactivation of chronic viral hepatitis are the most frequently described trigger factors. Other conditions considered precipitating factors are less common, including acute alcoholic hepatitis, major surgery, TIPS insertion, or inadequate paracentesis without albumin substitution.
- acute-on-chronic liver failure
- liver cirrhosis
- gut microbiome
1. Introduction
2. Etiological Factors of ACLF
| Precipitating Factor | Prevalence |
|---|---|
| Alcohol | 48.08% |
| Sepsis | 16.35% |
| Gastrointestinal bleeding | 19.13% |
| HBV | 8.2% |
| HEV | 7.21% |
| Tuberculostatic treatment | 6.25% |
| Autoimmune hepatitis | 0.96% |
| Unknown | 3.85% |
| Etiology | Total Patients | ACLF |
|---|---|---|
| Hepatitis C | 13,959 | 809 (5.79%) |
| Hepatitis B | 1967 | 145 (7.37%) |
| Alcohol | 23,484 | 1798 (7.65%) |
| Hepatitis C + Alcohol | 22,343 | 1791 (8.01%) |
| NAFLD | 15,893 | 929 (5.84%) |
| Other | 2737 | 181 (6.61%) |
This entry is adapted from the peer-reviewed paper 10.3390/biomedicines11071840
References
- O’Leary, J.G.; Reddy, K.R.; Garcia-Tsao, G.; Biggins, S.W.; Wong, F.; Fallon, M.B.; Subramanian, R.M.; Kamath, P.S.; Thuluvath, P.; Vargas, H.E.; et al. NACSELD Acute-on-Chronic Liver Failure (NACSELD-ACLF) Score Predicts 30-Day Survival in Hospitalized Patients with Cirrhosis. Hepatology 2018, 67, 2367–2374.
- Sarin, S.K.; Choudhury, A.; Sharma, M.K.; Maiwall, R.; Al Mahtab, M.; Rahman, S.; Saigal, S.; Saraf, N.; Soin, A.S.; Devarbhavi, H.; et al. Acute-on-Chronic Liver Failure: Consensus Recommendations of the Asian Pacific Association for the Study of the Liver (APASL): An Update. Hepatol. Int. 2019, 13, 353–390.
- Sarin, S.K.; Kedarisetty, C.K.; Abbas, Z.; Amarapurkar, D.; Bihari, C.; Chan, A.C.; Chawla, Y.K.; Dokmeci, A.K.; Garg, H.; Ghazinyan, H.; et al. Acute-on-Chronic Liver Failure: Consensus Recommendations of the Asian Pacific Association for the Study of the Liver (APASL) 2014. Hepatol. Int. 2014, 8, 453–471.
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-Chronic Liver Failure Is a Distinct Syndrome That Develops in Patients with Acute Decompensation of Cirrhosis. Gastroenterology 2013, 144, 1426–1437.
- Bajaj, J.S.; O’Leary, J.G.; Lai, J.C.; Wong, F.; Long, M.D.; Wong, R.J.; Kamath, P.S. Acute-on-Chronic Liver Failure Clinical Guidelines. Off. J. Am. Coll. Gastroenterol. ACG 2022, 117, 225.
- Engelmann, C.; Thomsen, K.L.; Zakeri, N.; Sheikh, M.; Agarwal, B.; Jalan, R.; Mookerjee, R.P. Validation of CLIF-C ACLF Score to Define a Threshold for Futility of Intensive Care Support for Patients with Acute-on-Chronic Liver Failure. Crit. Care 2018, 22, 254.
- Engelmann, C.; Berg, T. Clinical Practice Guidelines for Acute-on-Chronic Liver Failure: Are We Ready for Reaching Global Consensus? Hepatobiliary Surg. Nutr. 2023, 12, 239–243.
- Trebicka, J.; Reiberger, T.; Laleman, W. Gut-Liver Axis Links Portal Hypertension to Acute-on-Chronic Liver Failure. Visc. Med. 2018, 34, 270–275.
- Kim, T.Y.; Kim, D.J. Acute-on-Chronic Liver Failure. Clin. Mol. Hepatol. 2013, 19, 349–359.
- Gawande, A.; Gupta, G.K.; Gupta, A.; Wanjari, S.J.; Goel, V.; Rathore, V.; Bhardwaj, H.; Nijhawan, S. Acute-on-Chronic Liver Failure: Etiology of Chronic and Acute Precipitating Factors and Their Effect on Mortality. J. Clin. Exp. Hepatol. 2019, 9, 699–703.
- Li, H.; Chen, L.-Y.; Zhang, N.; Li, S.-T.; Zeng, B.; Pavesi, M.; Amorós, À.; Mookerjee, R.P.; Xia, Q.; Xue, F.; et al. Characteristics, Diagnosis and Prognosis of Acute-on-Chronic Liver Failure in Cirrhosis Associated to Hepatitis B. Sci. Rep. 2016, 6, 25487.
- Yin, S.; Wang, S.J.; Gu, W.Y.; Zhang, Y.; Chen, L.Y.; Li, H. Risk of Different Precipitating Events for Progressing to Acute-on-Chronic Liver Failure in HBV-Related Cirrhotic Patients. J. Dig. Dis. 2017, 18, 292–301.
- Shi, Y.; Yang, Y.; Hu, Y.; Wu, W.; Yang, Q.; Zheng, M.; Zhang, S.; Xu, Z.; Wu, Y.; Yan, H.; et al. Acute-on-chronic Liver Failure Precipitated by Hepatic Injury Is Distinct from That Precipitated by Extrahepatic Insults. Hepatology 2015, 62, 232.
- Kumar, M.; Chauhan, R.; Gupta, N.; Hissar, S.; Sakhuja, P.; Sarin, S.K. Spontaneous Increases in Alanine Aminotransferase Levels in Asymptomatic Chronic Hepatitis B Virus-Infected Patients. Gastroenterology 2009, 136, 1272–1280.
- Sarin, S.K.; Kumar, A.; Almeida, J.A.; Chawla, Y.K.; Fan, S.T.; Garg, H.; de Silva, H.J.; Hamid, S.S.; Jalan, R.; Komolmit, P.; et al. Acute-on-Chronic Liver Failure: Consensus Recommendations of the Asian Pacific Association for the Study of the Liver (APASL). Hepatol. Int. 2009, 3, 269–282.
- Wan, Z.; Wu, Y.; Yi, J.; You, S.; Liu, H.; Sun, Z.; Zhu, B.; Zang, H.; Li, C.; Liu, F.; et al. Combining Serum Cystatin C with Total Bilirubin Improves Short-Term Mortality Prediction in Patients with HBV-Related Acute-On-Chronic Liver Failure. PLoS ONE 2015, 10, e0116968.
- Radha Krishna, Y.; Saraswat, V.A.; Das, K.; Himanshu, G.; Yachha, S.K.; Aggarwal, R.; Choudhuri, G. Clinical Features and Predictors of Outcome in Acute Hepatitis A and Hepatitis E Virus Hepatitis on Cirrhosis. Liver Int. 2009, 29, 392–398.
- Agrawal, S.; Rana, B.S.; Mitra, S.; Duseja, A.; Das, A.; Dhiman, R.K.; Chawla, Y. A Case of Acute-on-Chronic Liver Failure (ACLF) Due to An Uncommon Acute And Chronic Event. J. Clin. Exp. Hepatol. 2018, 8, 95–97.
- Kahraman, A.; Miller, M.; Gieseler, R.K.; Gerken, G.; Scolaro, M.J.; Canbay, A. Non-Alcoholic Fatty Liver Disease in HIV-Positive Patients Predisposes for Acute-on-Chronic Liver Failure: Two Cases. Eur. J. Gastroenterol. Hepatol. 2006, 18, 101.
- Duseja, A.; Chawla, Y.K.; Dhiman, R.K.; Kumar, A.; Choudhary, N.; Taneja, S. Non-Hepatic Insults Are Common Acute Precipitants in Patients with Acute on Chronic Liver Failure (ACLF). Dig. Dis. Sci. 2010, 55, 3188–3192.
- Zhang, X.; Ke, W.; Xie, J.; Zhao, Z.; Xie, D.; Gao, Z. Comparison of Effects of Hepatitis E or A Viral Superinfection in Patients with Chronic Hepatitis B. Hepatol. Int. 2010, 4, 615–620.
- Fu, J.; Guo, D.; Gao, D.; Huang, W.; Li, Z.; Jia, B. Clinical Analysis of Patients Suffering from Chronic Hepatitis B Superinfected with Other Hepadnaviruses. J. Med. Virol. 2016, 88, 1003–1009.
- Beisel, C.; Addo, M.M.; Schulze zur Wiesch, J. Seroconversion of HBsAG Coincides with Hepatitis A Super-Infection: A Case Report. World J. Clin. Cases 2020, 8, 1651–1655.
- Spada, E.; Genovese, D.; Tosti, M.E.; Mariano, A.; Cuccuini, M.; Proietti, L.; Giuli, C.D.; Lavagna, A.; Crapa, G.E.; Morace, G.; et al. An Outbreak of Hepatitis A Virus Infection with a High Case-Fatality Rate among Injecting Drug Users. J. Hepatol. 2005, 43, 958–964.
- Lefilliatre, P.; Villeneuve, J.-P. Fulminant Hepatitis A in Patients with Chronic Liver Disease. Can. J. Public Health 2000, 91, 168–170.
- Sagnelli, E.; Coppola, N.; Pisaturo, M.; Pisapia, R.; Onofrio, M.; Sagnelli, C.; Catuogno, A.; Scolastico, C.; Piccinino, F.; Filippini, P. Clinical and Virological Improvement of Hepatitis B Virus—Related or Hepatitis C Virus—Related Chronic Hepatitis with Concomitant Hepatitis A Virus Infection. Clin. Infect. Dis. 2006, 42, 1536–1543.
- Deterding, K.; Tegtmeyer, B.; Cornberg, M.; Hadem, J.; Potthoff, A.; Böker, K.H.W.; Tillmann, H.L.; Manns, M.P.; Wedemeyer, H. Hepatitis A Virus Infection Suppresses Hepatitis C Virus Replication and May Lead to Clearance of HCV. J. Hepatol. 2006, 45, 770–778.
- Cacopardo, B.; Nunnari, G.; Nigro, L. Clearance of HCV RNA Following Acute Hepatitis A Superinfection. Dig. Liver Dis. 2009, 41, 371–374.
- Kashyap, P.; Deka, M.; Medhi, S.; DUTTA, S.; Kashyap, K.; Kumari, N. Association of Toll-like Receptor 4 with Hepatitis A Virus Infection in Assam. Acta Virol. 2018, 62, 58–62.
- Rubicz, R.; Yolken, R.; Drigalenko, E.; Carless, M.A.; Dyer, T.D.; Kent Jr, J.; Curran, J.E.; Johnson, M.P.; Cole, S.A.; Fowler, S.P.; et al. Genome-Wide Genetic Investigation of Serological Measures of Common Infections. Eur. J. Hum. Genet. 2015, 23, 1544–1548.
- Kumar, A.; Saraswat, V.A. Hepatitis E and Acute-on-Chronic Liver Failure. J. Clin. Exp. Hepatol. 2013, 3, 225–230.
- Choi, J.W.; Son, H.J.; Lee, S.S.; Jeon, H.; Cho, J.-K.; Kim, H.J.; Cha, R.R.; Lee, J.M.; Kim, H.J.; Jung, W.T.; et al. Acute Hepatitis E Virus Superinfection Increases Mortality in Patients with Cirrhosis. BMC Infect. Dis. 2022, 22, 62.
- Kmush, B.; Wierzba, T.; Krain, L.; Nelson, K.; Labrique, A.B. Epidemiology of Hepatitis E in Low- and Middle-Income Countries of Asia and Africa. Semin. Liver Dis. 2013, 33, 015–029.
- Artru, F.; Louvet, A.; Ruiz, I.; Levesque, E.; Labreuche, J.; Ursic-Bedoya, J.; Lassailly, G.; Dharancy, S.; Boleslawski, E.; Lebuffe, G.; et al. Liver Transplantation in the Most Severely Ill Cirrhotic Patients: A Multicenter Study in Acute-on-Chronic Liver Failure Grade 3. J. Hepatol. 2017, 67, 708–715.
- Kanda, T.; Matsumoto, N.; Ishii, T.; Arima, S.; Shibuya, S.; Honda, M.; Sasaki-Tanaka, R.; Masuzaki, R.; Kanezawa, S.; Nishizawa, T.; et al. Chronic Hepatitis C: Acute Exacerbation and Alanine Aminotransferase Flare. Viruses 2023, 15, 183.
- Kanda, T.; Yokosuka, O.; Imazeki, F.; Saisho, H. Acute Hepatitis C Virus Infection, 1986-2001: A Rare Cause of Fulminant Hepatitis in Chiba, Japan. Hepatogastroenterology 2004, 51, 556–558.
- Liang, T.J.; Jeffers, L.; Reddy, R.K.; Silva, M.O.; Cheinquer, H.; Findor, A.; De Medina, M.; Yarbough, P.O.; Reyes, G.R.; Schiff, E.R. Fulminant or Subfulminant Non-A, Non-B Viral Hepatitis: The Role of Hepatitis C and E Viruses. Gastroenterology 1993, 104, 556–562.
- Jain, A.; Kar, P.; Madan, K.; Das, U.P.; Budhiraja, S.; Gopalkrishna, V.; Sharma, J.K.; Das, B.C. Hepatitis C Virus Infection in Sporadic Fulminant Viral Hepatitis in North India: Cause or Co-Factor? Eur. J. Gastroenterol. Hepatol. 1999, 11, 1231–1237.
- Maheshwari, A.; Ray, S.; Thuluvath, P.J. Acute Hepatitis C. Lancet 2008, 372, 321–332.
- Rao, A.; Rule, J.A.; Cerro-Chiang, G.; Stravitz, R.T.; McGuire, B.M.; Lee, G.; Fontana, R.J.; Lee, W.M. Role of Hepatitis C Infection in Acute Liver Injury/Acute Liver Failure in North America. Dig. Dis. Sci. 2023, 68, 304–311.
- Younis, B.B.; Arshad, R.; Khurhsid, S.; Masood, J.; Nazir, F.; Tahira, M. Fulminant Hepatic Failure (FHF) Due to Acute Hepatitis C. Pak. J. Med. Sci. 2015, 31, 1009–1011.
- Sagnelli, E.; Pisaturo, M.; Stanzione, M.; Messina, V.; Alessio, L.; Sagnelli, C.; Starace, M.; Pasquale, G.; Coppola, N. Clinical Presentation, Outcome, and Response to Therapy among Patients with Acute Exacerbation of Chronic Hepatitis C. Clin. Gastroenterol. Hepatol. 2013, 11, 1174–1180.e11.
- Thiel, A.M.; Rissland, J.; Lammert, F.; Casper, M. Acute liver failure as a rare case of a frequent disease. Z. Gastroenterol. 2018, 56, 255–258.
- Trebicka, J.; Amoros, A.; Pitarch, C.; Titos, E.; Alcaraz-Quiles, J.; Schierwagen, R.; Deulofeu, C.; Fernandez-Gomez, J.; Piano, S.; Caraceni, P.; et al. Addressing Profiles of Systemic Inflammation Across the Different Clinical Phenotypes of Acutely Decompensated Cirrhosis. Front. Immunol. 2019, 10, 476.
- Wiest, R.; Lawson, M.; Geuking, M. Pathological Bacterial Translocation in Liver Cirrhosis. J. Hepatol. 2014, 60, 197–209.
- Trebicka, J.; Gu, W.; Ibáñez-Samaniego, L.; Hernández-Gea, V.; Pitarch, C.; Garcia, E.; Procopet, B.; Giráldez, Á.; Amitrano, L.; Villanueva, C.; et al. Rebleeding and Mortality Risk Are Increased by ACLF but Reduced by Pre-Emptive TIPS. J. Hepatol. 2020, 73, 1082–1091.
- Costa, D.; Simbrunner, B.; Jachs, M.; Hartl, L.; Bauer, D.; Paternostro, R.; Schwabl, P.; Scheiner, B.; Stättermayer, A.F.; Pinter, M.; et al. Systemic Inflammation Increases across Distinct Stages of Advanced Chronic Liver Disease and Correlates with Decompensation and Mortality. J. Hepatol. 2021, 74, 819–828.
- Hernández-Gea, V.; Procopet, B.; Giráldez, Á.; Amitrano, L.; Villanueva, C.; Thabut, D.; Ibañez-Samaniego, L.; Silva-Junior, G.; Martinez, J.; Genescà, J.; et al. Preemptive-TIPS Improves Outcome in High-Risk Variceal Bleeding: An Observational Study. Hepatology 2019, 69, 282–293.
- Kumar, R.; Kerbert, A.J.C.; Sheikh, M.F.; Roth, N.; Calvao, J.A.F.; Mesquita, M.D.; Barreira, A.I.; Gurm, H.S.; Ramsahye, K.; Mookerjee, R.P.; et al. Determinants of Mortality in Patients with Cirrhosis and Uncontrolled Variceal Bleeding. J. Hepatol. 2021, 74, 66–79.
- European Association for the Study of the Liver. Electronic address: ; European Association for the Study of the Liver EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis. J. Hepatol. 2018, 69, 406–460.
- Gerbes, A.L.; Labenz, J.; Appenrodt, B.; Dollinger, M.; Gundling, F.; Gülberg, V.; Holstege, A.; Lynen-Jansen, P.; Steib, C.J.; Trebicka, J.; et al. Aktualisierte S2k-Leitlinie der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten (DGVS) „Komplikationen der Leberzirrhose“: AWMF-Nr.: 021-017. Z. Gastroenterol. 2019, 57, 611–680.
- Wasmuth, H.E.; Kunz, D.; Yagmur, E.; Timmer-Stranghöner, A.; Vidacek, D.; Siewert, E.; Bach, J.; Geier, A.; Purucker, E.A.; Gressner, A.M.; et al. Patients with Acute on Chronic Liver Failure Display ‘Sepsis-like’ Immune Paralysis. J. Hepatol. 2005, 42, 195–201.
- Mahmud, N.; Kaplan, D.E.; Taddei, T.H.; Goldberg, D.S. Incidence and Mortality of Acute-on-Chronic Liver Failure Using Two Definitions in Patients with Compensated Cirrhosis. Hepatology 2019, 69, 2150–2163.
- Jalan, R.; Yurdaydin, C.; Bajaj, J.S.; Acharya, S.K.; Arroyo, V.; Lin, H.-C.; Gines, P.; Kim, W.R.; Kamath, P.S. Toward an Improved Definition of Acute-on-Chronic Liver Failure. Gastroenterology 2014, 147, 4–10.
- Wlodzimirow, K.A.; Eslami, S.; Abu-Hanna, A.; Nieuwoudt, M.; Chamuleau, R.A.F.M. A Systematic Review on Prognostic Indicators of Acute on Chronic Liver Failure and Their Predictive Value for Mortality. Liver Int. 2013, 33, 40–52.
- Singer, C.E.; Vasile, C.M.; Popescu, M.; Popescu, A.I.S.; Marginean, I.C.; Iacob, G.A.; Popescu, M.D.; Marginean, C.M. Role of Iron Deficiency in Heart Failure—Clinical and Treatment Approach: An Overview. Diagnostics 2023, 13, 304.
- Avolio, A.W.; Gaspari, R.; Teofili, L.; Bianco, G.; Spinazzola, G.; Soave, P.M.; Paiano, G.; Francesconi, A.G.; Arcangeli, A.; Nicolotti, N.; et al. Postoperative Respiratory Failure in Liver Transplantation: Risk Factors and Effect on Prognosis. PLoS ONE 2019, 14, e0211678.
- Mattos, D.Â.Z.; Mattos, D.A.A. Letter to the Editor: Acute-on-Chronic Liver Failure: Conceptual Divergences. Hepatology 2019, 70, 1076.