Cytoreductive surgery (CRS) is the cornerstone of treating advanced ovarian cancer. Approximately 60–70% of patients with advanced ovarian cancer will have involvement in the upper abdomen or the supracolic compartment of the abdominal cavity. Though the involvement of this region results in poorer survival compared, complete cytoreduction benefits overall survival, making upper-abdominal cytoreduction an essential component of CRS for advanced ovarian cancer. The upper abdomen constitutes several vital organs and large blood vessels draped with the parietal or visceral peritoneum, common sites of disease in ovarian cancer. A surgeon treating advanced ovarian cancer should be well versed in upper-abdominal cytoreduction techniques, including diaphragmatic peritonectomy and diaphragm resection, lesser omentectomy, splenectomy with or without distal pancreatectomy, liver resection, cholecystectomy, and suprarenal retroperitoneal lymphadenectomy. Other procedures such as clearance of the periportal region, Glisson’s capsulectomy, clearance of the superior recess of the lesser sac, and Morrison’s pouch are essential as these regions are often involved in ovarian cancer.
1. Introduction
This excerpt describes the surgical anatomy of the upper abdomen in the context of performing cytoreductive surgery for peritoneal cancer spread from ovarian cancer. Epithelial ovarian cancer (EOC) continues to be diagnosed in an advanced stage in over 70% of patients, and approximately 60–70% of these patients will have involvement in the upper abdomen or the supracolic compartment of the abdominal cavity
[1][2][3]. Over time, upper-abdominal cytoreductive surgery (CRS) has become an essential component of the skill set of surgical and gynecological oncologists treating advanced EOC
[4][5]. The most common surgical procedures to clear the tumor from the upper abdomen include diaphragmatic peritonectomy and diaphragm resection, lesser omentectomy, splenectomy with or without distal pancreatectomy, liver resection, cholecystectomy, and suprarenal retroperitoneal lymphadenectomy. Other procedures such as clearance of the periportal region, Glisson’s capsulectomy, clearance of the superior recess of the lesser sac, and Morrison’s pouch are essential as these regions are often involved in ovarian cancer
[6].
Advanced EOC is a peritoneal disease that often has a miliary or plaque-like morphology and is not detected on preoperative imaging
[7]. A thorough exploration of the abdominal cavity to identify all disease sites is essential to avoid missing disease in some areas and thus perform what could be termed a ‘pseudo-complete’ cytoreduction
[8][9]. There is limited information about the patterns of peritoneal dissemination or disease distribution in the scientific literature, which increases the dependence on surgical exploration and visual inspection performed during surgery
[10]. The upper abdomen, in particular, could be challenging to explore for surgeons unfamiliar with the anatomy.
2. Surgical Anatomy of the Upper Abdomen
The upper abdomen could be defined in two ways. Considering the anatomy of the peritoneal cavity and its spaces, the supracolic compartment could be regarded as the ‘upper abdomen’
[11]. The peritoneal cancer index devised by Paul Sugarbaker divides the abdominal cavity into 13 anatomical regions, of which regions 1, 2, and 3 could jointly be considered the upper-abdominal regions
[12].
2.1. Peritoneal Ligaments and Spaces
The upper-abdominal cavity or supracolic compartment comprises several ligaments and spaces
[13]. The falciform and triangular ligaments are the suspensory ligaments of the liver that bind the bare area. The hepatoduodenal ligament (containing the common bile duct, hepatic artery, and portal vein) and the gastrohepatic ligament (which includes the left gastric artery and the coronary vein) form the lesser omentum
[13]. The gastrosplenic ligament connects the greater curve of the stomach to the spleen and contains the short gastric vessels. The splenorenal ligament has the pancreatic tail. Ovarian cancer could involve any of these structures and the surgeon should be familiar with their anatomy.
The supramesocolic compartment is divided into the left and right subphrenic spaces by the falciform ligament on the anterior aspect of the liver. The sub-hepatic space, including the lesser sac, is located under the liver. The right subphrenic space is located under the right diaphragm; it communicates inferiorly with the right paracolic space and is separated from the left subphrenic space by the falciform ligament
[14]. The right sub-hepatic space continues medially through the foramen of Winslow (Epiploic foramen) to the lesser sac (Bursa Omentalis)
[14].
The lesser sac is a potentially large cavity with various recesses communicating with the left subphrenic space cranially and into the greater omentum caudally. The lesser sac contains a superior recess (located above the peritoneal reflection of the left gastric artery) close to the caudate lobe and a larger inferior recess between the stomach and the pancreatic body. The superior and inferior recesses are separated by a peritoneal fold that accompanies the left gastric artery. Sometimes, the inferior recess communicates with a potential space between the leaves of the greater omentum
[14].
2.2. Anatomical Boundaries from the Surgical Viewpoint
The peritoneal regions lying in each region and their boundaries are described in
Table 1. More details can be found online in the PROMISE internet application (
www.e-promise.org).
[15]2.3. Regional Nodes
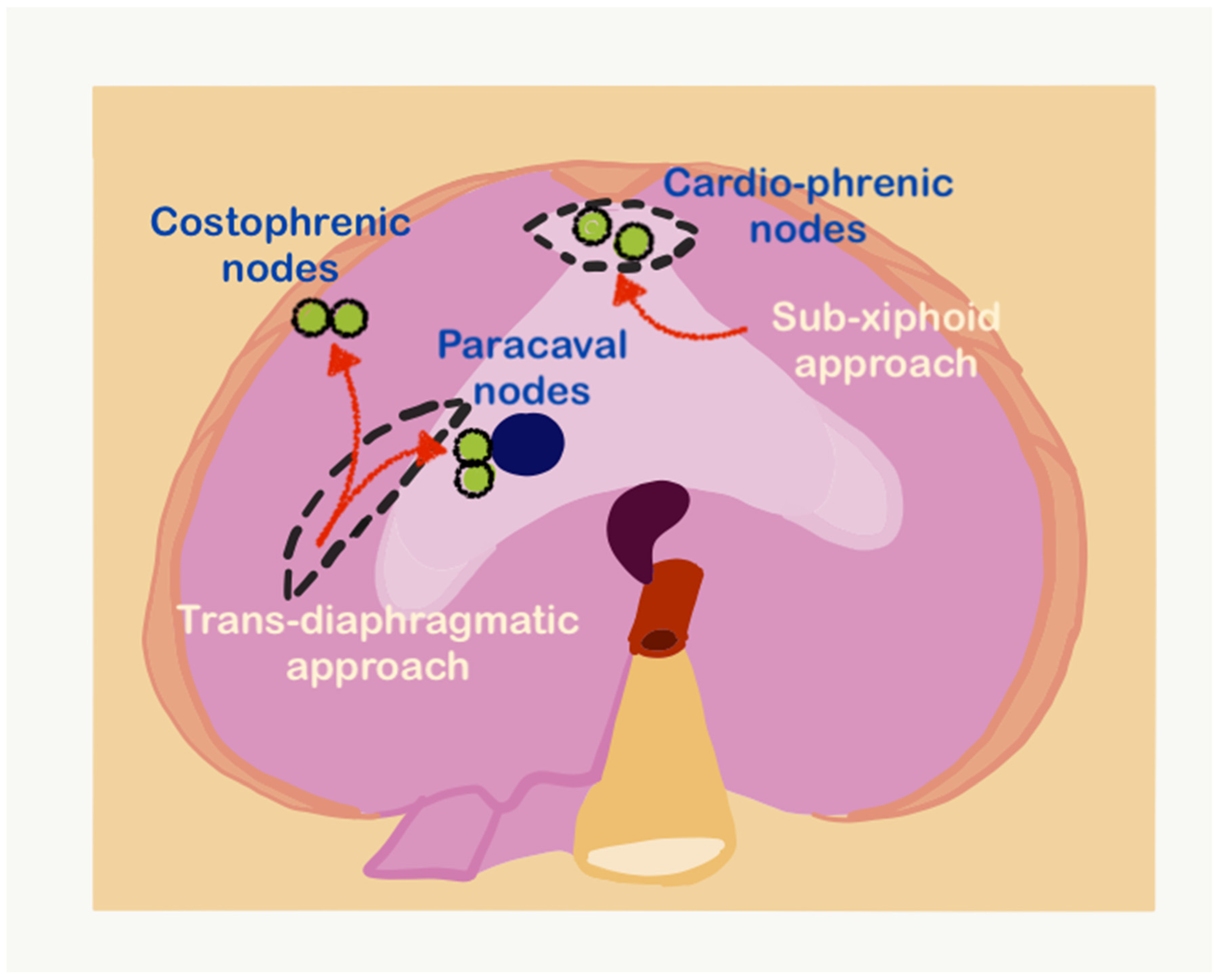
Several nodal stations in the upper abdomen could be involved in advanced ovarian cancer. Some of these nodes are involved secondary to the primary tumor as part of retroperitoneal lymphadenopathy and these include the suprarenal retroperitoneal or paraaortic nodes such as the superior mesenteric and celiac axis nodes. The other nodes are the omental nodes along the lesser and greater curves, the left gastric nodes, periportal nodes, and pericardiac nodes. The supradiaphragmatic nodes often dissected during upper-abdominal cytoreduction include the sub-xiphoid or cardiophrenic angle nodes, costophrenic lymph nodes, and paracaval nodes
[18]. It is unclear whether these nodal stations are regional nodes or distant metastases, as their involvement has not been classified in the TNM and FIGO classifications
[19][20].
Figure 1 shows the anatomical location of the supradiaphragmatic nodes.
Figure 1. The sub-xiphoid and transdiaphragmatic approaches for resecting supradiaphragmatic lymph nodes (adapted from
[21] with permission).
 +1 credit
+1 credit