Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Christoph Nienaber | -- | 1411 | 2022-10-28 16:26:38 | | | |
| 2 | Dean Liu | Meta information modification | 1411 | 2022-10-31 02:53:23 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Yuan, X.; Mitsis, A.; Nienaber, C.A. Epidemiology and Classification of Aortic Dissection. Encyclopedia. Available online: https://encyclopedia.pub/entry/31843 (accessed on 09 August 2026).
Yuan X, Mitsis A, Nienaber CA. Epidemiology and Classification of Aortic Dissection. Encyclopedia. Available at: https://encyclopedia.pub/entry/31843. Accessed August 09, 2026.
Yuan, Xun, Andreas Mitsis, Christoph A. Nienaber. "Epidemiology and Classification of Aortic Dissection" Encyclopedia, https://encyclopedia.pub/entry/31843 (accessed August 09, 2026).
Yuan, X., Mitsis, A., & Nienaber, C.A. (2022, October 28). Epidemiology and Classification of Aortic Dissection. In Encyclopedia. https://encyclopedia.pub/entry/31843
Yuan, Xun, et al. "Epidemiology and Classification of Aortic Dissection." Encyclopedia. Web. 28 October, 2022.
Copy Citation
The aorta is the largest artery in the body, delivering oxygenated blood from the left ventricle to all organs. Dissection of the aorta is a lethal condition caused by a tear in the intimal layer of the aorta, followed by blood loss within the aortic wall and separation of the layers to full dissection. The aorta can be affected by a wide range of causes including acute conditions such as trauma and mechanical damage; and genetic conditions such as arterial hypertension, dyslipidaemia, and connective tissue disorders; all increasing the risk of dissection. Both rapid diagnostic recognition and advanced multidisciplinary treatment are critical in managing aortic dissection patients.
aortic dissection
diagnosis
TEVAR
prognosis
1. Introduction
The aorta is the body’s largest blood vessel, and its primary function is to carry oxygen and blood from the left ventricle to other organs of the body. Anatomically, the aorta is divided into four parts: the ascending aorta (which starts from the heart and from which coronary arteries arise), the aortic arch (which bends over the heart and turns towards the posterior thoracic wall), the descending thoracic aorta (which extends through the posterior thoracic cavity in vicinity of the spine) and finally, the abdominal aorta (which runs below the diaphragm) [1][2]. Clinically, aortic dissection is classified by the location of the dissection and/or origin of the intimal tear and the expanse of the dissection. Stanford type A (or DeBakey type I and II) involves the ascending aorta, while Stanford type B (or DeBakey IIIa and IIIb) involves the descending thoracic and abdominal aorta [3][4].
The aortic wall comprises three layers: the thin tunica intima which faces the bloodstream, the thick musculo-elastic tunica media, and the outer fibrous tunica adventitia (Figure 1). In acute aortic dissection, a tear in the intima layer results in blood entry to the media layer, developing in an intimal flap and dividing the original vessel into true and false lumen. A broad range of diseases can affect the aorta, including acute (such as trauma and hypertensive emergencies) or chronic conditions (such as chronic arterial hypertension, connective tissue disorders, inflammatory vasculitis and atherosclerosis). Aortic dissection is considered a complex vascular scenario that benefits in terms of prognosis from a rapid diagnosis and advanced teamwork including cardiac surgeons, cardiologists, vascular interventionists, and radiologists.

Figure 1. The structure of aortic wall. In aortic dissection, a tear in the intima layer results in blood entry to the media layer, developing in an intimal flap and dividing the original vessel into true and false lumen.
2. Epidemiology
Population-based studies in the US and Europe indicate an incidence of 2.6 to 3.5 cases per 100,000 person-years [5][6]. Another study from the UK observed 92,728 patients over 10 years, and reported a higher incidence (6 per 100,000 person-years) of acute aortic dissection [7], which is similar to data from Sweden with an incidence of 7.2 per 100,000 person-years [8]. The real-world incidence may be underestimated due to omission of pre-admission deaths in all studies. Interestingly, the demographic forecasts from the UK Office for National Statistics predicts that the incidence of aortic dissection will rise from 3892 in 2010 to 6893 in 2050 in both men and women, with the majority occurring in individuals over 75 [7][9]. The number of cases of acute aortic dissection seems to be rising in Western countries, possibly related to increased awareness of the disease, as well as access to the use of advanced imaging techniques (particularly CT) in emergency departments [10][11][12].
The frequency of acute aortic dissection is notably higher in males, in particular those who are older [8][13]. Women are usually older than men at presentation, with a mean age of 72 years vs. 64 years in men [14][15]. Despite the higher rates of aortic dissection being in men, it is women who have a higher mortality rate. Data from the International Registry of Aortic Dissection (IRAD) indicates that women with aortic dissection typically present at hospital later than men with worse clinical status (coma and tamponade). The data also show they have different types of symptoms and show less typical clinical presentation [16]. These data may partly be explained in a different analysis; after age-adjustment, women have higher rates of mortality then men and more often suffer pre-hospital death [8][16].
3. Classification
Aortic dissection can be categorized in different ways in terms of anatomy and symptom onset. The two most frequent anatomic classification systems are: DeBakey classification, which is based on the site of origin of the intimal tear [4]; and Stanford classification, which specifies the involvement, or lack thereof, of the ascending aorta [3]. DeBakey classification precisely describes the site of the dissected segment or diseased lesion: Type I dissections usually originate from the ascending aorta and have the most extensive involvement including the ascending aorta, aortic arch, descending aorta and further; Type II dissections originate from and are only limited to the ascending aorta; Type III dissections originate from the descending aorta after the left subclavian artery orifice, and affects the descending aorta (Type IIIa) and/or distal abdominal aorta (Type IIIb) [4]. Stanford classification helps indicate different management for dissection cases in clinical practise: Type A dissections involve the ascending aorta (DeBakey type I and II), usually requiring swift surgery; while Type B dissections only involve the descending aorta (DeBakey type III) and can be managed endovascularly or medically [3][17] (Figure 2). Recently, a unique group, so-called non-A non-B, which does not completely fit DeBakey and Standford classification has been identified. These patients develop a dissection originating from the aortic arch, or the descending aorta and retrogradely involve the arch, without involving the ascending aorta. Several studies suggest that arch dissections could lead to organ malperfusion and aortic rupture, which require prompt intervention and careful management [18][19]. A new classification system, which includes the type of dissection (adapting Stanford system A, B or non-A non-B), the location of the primary entry tear, and the presence of malperfusion (TEM) has been introduced, but is yet awaiting community acceptance [19].
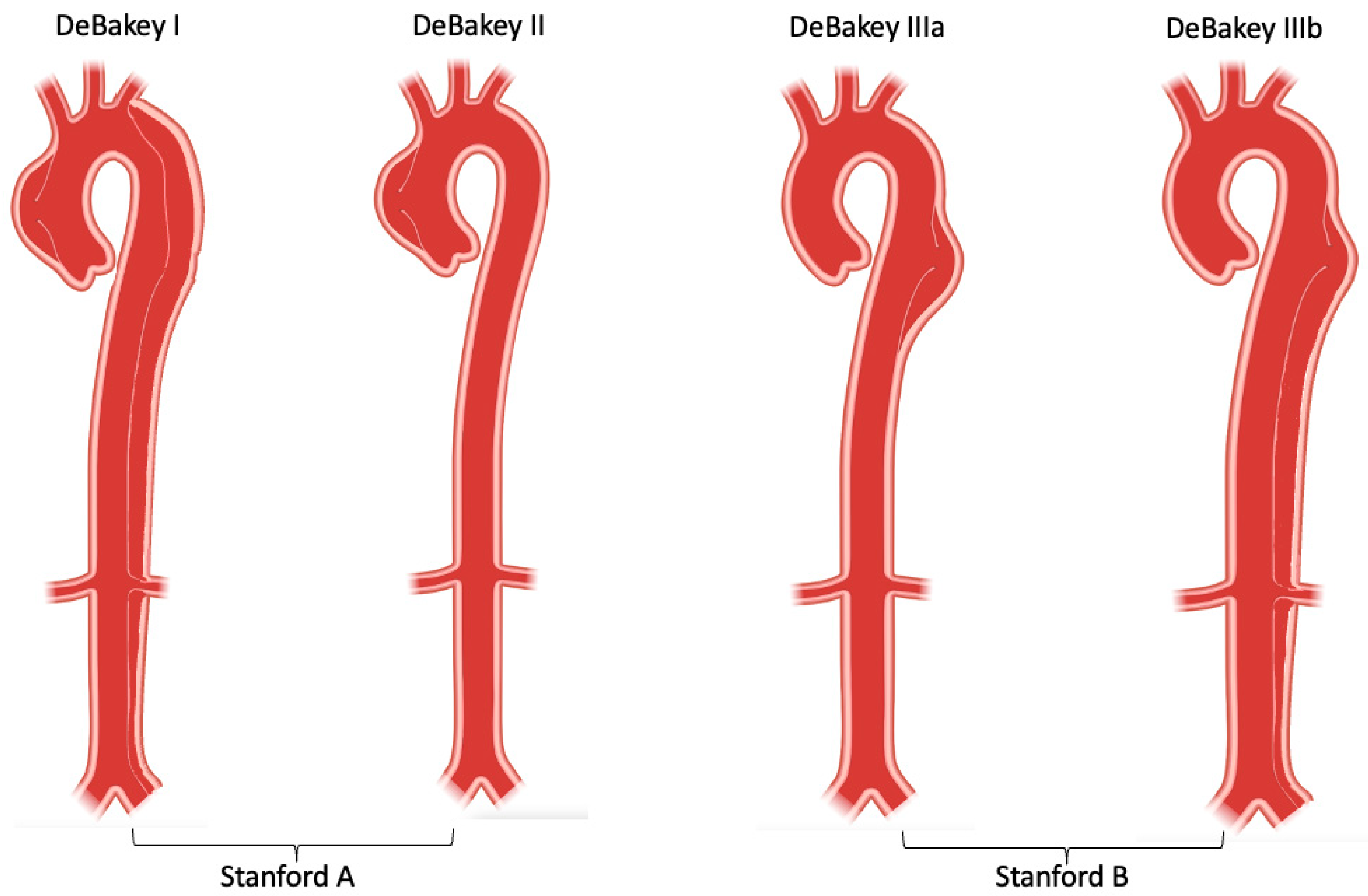
Figure 2. DeBakey and Stanford aortic dissection classification.
Clinically, type B aortic dissection are considered complicated or uncomplicated depending on high-risk features. Almost a quarter of type B patients present with some high-risk features such as signs of imminent rupture, evidence of organ or limb ischemia, refractory hypertension, hypotension (systolic blood pressure < 90 mmHg), and cardiogenic shock, which require early intervention to treat malperfusion or ischemia so as to avoid death [20]. Uncomplicated type B dissection is traditionally treated medically with close, regular surveillance. However, more and more studies show that morbidity and mortality could be as high as 30% and 42%, respectively, after 5 years of conservative management in uncomplicated type B dissection [21][22][23]. The INSTEAD-XL trial demonstrated significant survival benefit in the TEVAR group compared with medical only [24]. The ADSORB trail showed the feasibility and safety of TEVAR treatment for uncomplicated type B dissections in acute phase [25]. An imaging analysis of the ADSORB trial helped identify uncomplicated type B dissection patients who are at high-risk of developing aortic events, and also revealed better false lumen thrombosis in the TEVAR group than medical only (90.3% vs. 31.0%) [26]. As the vascular community understand the natural progress of type B dissection better, the term “uncomplicated” is under debate, and more point-based, outcome-oriented category systems are yet to be introduced [27][28][29].
Based on the period of onset of symptoms and diagnosis, the binary classification of the acute period (<2 weeks) and chronic period (>2 weeks) has been in use for decades [30]. As diagnostic technology and management improved, a new temporal classification based on patient survival rates from IRAD was introduced. According to the time of symptom onset, aortic dissections can be classified into hyperacute (<24 h), acute (2–7 days), sub-acute (8–30 days), and chronic (>30 days) phases [31]. Following symptom onset, survival continues to decrease considerably up to 30 days after presentation and falls into what has been traditionally considered the “chronic” phase of aortic dissection. This finding appears to be present in both Type A and Type B aortic dissections irrespective of the treatment strategy. Of note, this time approximately relates with the average length of hospital stay in these patients, meaning that close to discharge, even relatively “stable” patients have significant mortality risk. For these patients, continued surveillance is paramount. Attention should be given to aggressive use of both medical and nonmedical treatment modalities beyond the hyperacute and acute time periods, and into the traditional chronic phase. To sum up, stratifying aortic dissection into these four chronological groups offers a more sophisticated assessment of survival as it evolves over the first 60 days following symptom onset. This classification indicates patient survival rate and outcome, ultimately helping individual decision-making for early and late treatment decisions regarding the management plan of acute aortic dissection [31].
References
- Nienaber, C.A.; Clough, R.E. Management of acute aortic dissection. Lancet 2015, 385, 800–811.
- Nienaber, C.A.; Clough, R.E.; Sakalihasan, N.; Suzuki, T.; Gibbs, R.; Mussa, F.; Jenkins, M.P.; Thompson, M.M.; Evangelista, A.; Yeh, J.S.; et al. Aortic dissection. Nat. Rev. Dis. Prim. 2016, 2, 16071.
- Daily, P.O.; Trueblood, H.W.; Stinson, E.B.; Wuerflein, R.D.; Shumway, N.E. Management of acute aortic dissections. Ann. Thorac. Surg. 1970, 10, 237–247.
- Debakey, M.E.; Henly, W.S.; Cooley, D.A.; Morris, G.C., Jr.; Crawford, E.S.; Beall, A.C., Jr. Surgical Management of Dissecting Aneurysms of the Aorta. J. Thorac. Cardiovasc. Surg. 1965, 49, 130–149.
- Clouse, W.D.; Hallett, J.W., Jr.; Schaff, H.V.; Spittell, P.C.; Rowland, C.M.; Ilstrup, D.M.; Melton, L.J., 3rd. Acute aortic dissection: Population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin. Proc. 2004, 79, 176–180.
- Meszaros, I.; Morocz, J.; Szlavi, J.; Schmidt, J.; Tornoci, L.; Nagy, L.; Szep, L. Epidemiology and clinicopathology of aortic dissection. Chest 2000, 117, 1271–1278.
- Howard, D.P.; Banerjee, A.; Fairhead, J.F.; Perkins, J.; Silver, L.E.; Rothwell, P.M.; Oxford Vascular, S. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the Oxford Vascular Study. Circulation 2013, 127, 2031–2037.
- Smedberg, C.; Steuer, J.; Leander, K.; Hultgren, R. Sex differences and temporal trends in aortic dissection: A population-based study of incidence, treatment strategies, and outcome in Swedish patients during 15 years. Eur. Heart J. 2020, 41, 2430–2438.
- Howard, D.P.; Sideso, E.; Handa, A.; Rothwell, P.M. Incidence, risk factors, outcome and projected future burden of acute aortic dissection. Ann. Cardiothorac. Surg. 2014, 3, 278–284.
- Evangelista, A.; Isselbacher, E.M.; Bossone, E.; Gleason, T.G.; Eusanio, M.D.; Sechtem, U.; Ehrlich, M.P.; Trimarchi, S.; Braverman, A.C.; Myrmel, T.; et al. Insights From the International Registry of Acute Aortic Dissection: A 20-Year Experience of Collaborative Clinical Research. Circulation 2018, 137, 1846–1860.
- Pape, L.A.; Awais, M.; Woznicki, E.M.; Suzuki, T.; Trimarchi, S.; Evangelista, A.; Myrmel, T.; Larsen, M.; Harris, K.M.; Greason, K.; et al. Presentation, Diagnosis, and Outcomes of Acute Aortic Dissection: 17-Year Trends From the International Registry of Acute Aortic Dissection. J. Am. Coll. Cardiol. 2015, 66, 350–358.
- Olsson, C.; Thelin, S.; Stahle, E.; Ekbom, A.; Granath, F. Thoracic aortic aneurysm and dissection: Increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006, 114, 2611–2618.
- DeMartino, R.R.; Sen, I.; Huang, Y.; Bower, T.C.; Oderich, G.S.; Pochettino, A.; Greason, K.; Kalra, M.; Johnstone, J.; Shuja, F.; et al. Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004689.
- Melvinsdottir, I.H.; Lund, S.H.; Agnarsson, B.A.; Sigvaldason, K.; Gudbjartsson, T.; Geirsson, A. The incidence and mortality of acute thoracic aortic dissection: Results from a whole nation study. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2016, 50, 1111–1117.
- McClure, R.S.; Brogly, S.B.; Lajkosz, K.; Payne, D.; Hall, S.F.; Johnson, A.P. Epidemiology and management of thoracic aortic dissections and thoracic aortic aneurysms in Ontario, Canada: A population-based study. J. Thorac. Cardiovasc. Surg. 2018, 155, 2254–2264.e4.
- Huckaby, L.V.; Sultan, I.; Trimarchi, S.; Leshnower, B.; Chen, E.P.; Brinster, D.R.; Myrmel, T.; Estrera, A.L.; Montgomery, D.G.; Korach, A.; et al. Sex-Based Aortic Dissection Outcomes From the International Registry of Acute Aortic Dissection. Ann. Thorac. Surg. 2022, 113, 498–505.
- Yuan, X.; Mitsis, A.; Ghonem, M.; Iakovakis, I.; Nienaber, C.A. Conservative management versus endovascular or open surgery in the spectrum of type B aortic dissection. J. Vis. Surg. 2018, 4, 59.
- Rylski, B.; Perez, M.; Beyersdorf, F.; Reser, D.; Kari, F.A.; Siepe, M.; Czerny, M. Acute non-A non-B aortic dissection: Incidence, treatment and outcome. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2017, 52, 1111–1117.
- Sievers, H.H.; Rylski, B.; Czerny, M.; Baier, A.L.M.; Kreibich, M.; Siepe, M.; Beyersdorf, F. Aortic dissection reconsidered: Type, entry site, malperfusion classification adding clarity and enabling outcome prediction. Interact Cardiovasc. Thorac. Surg. 2020, 30, 451–457.
- Mitsis, A.; Yuan, X.; Cambronero-cortinas, E.; Nienaber, C.A. New developments in the treatment of type B aortic dissection. Ital. J. Vascualr Endovasc. Surg. 2017, 24, 118–126.
- Kato, N.; Shimono, T.; Hirano, T.; Suzuki, T.; Ishida, M.; Sakuma, H.; Yada, I.; Takeda, K. Midterm results of stent-graft repair of acute and chronic aortic dissection with descending tear: The complication-specific approach. J. Thorac. Cardiovasc. Surg. 2002, 124, 306–312.
- Bogdan, Y.; Hines, G.L. Management of acute complicated and uncomplicated type B dissection of the aorta: Focus on endovascular stent grafting. Cardiol. Rev. 2010, 18, 234–239.
- Acosta, S.; Blomstrand, D.; Gottsater, A. Epidemiology and long-term prognostic factors in acute type B aortic dissection. Ann. Vasc. Surg. 2007, 21, 415–422.
- Nienaber, C.A.; Kische, S.; Rousseau, H.; Eggebrecht, H.; Rehders, T.C.; Kundt, G.; Glass, A.; Scheinert, D.; Czerny, M.; Kleinfeldt, T.; et al. Endovascular repair of type B aortic dissection: Long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ. Cardiovasc. Interv. 2013, 6, 407–416.
- Brunkwall, J.; Kasprzak, P.; Verhoeven, E.; Heijmen, R.; Taylor, P.; Trialists, A.; Alric, P.; Canaud, L.; Janotta, M.; Raithel, D.; et al. Endovascular repair of acute uncomplicated aortic type B dissection promotes aortic remodelling: 1 year results of the ADSORB trial. Eur. J. Vasc. Endovasc. Surg. 2014, 48, 285–291.
- Kamman, A.V.; Brunkwall, J.; Verhoeven, E.L.; Heijmen, R.H.; Trimarchi, S.; Kasprzak, P.; Alric, P.; Schumacher, H.; Fabiani, J.N.; Eckstein, H.-H.; et al. Predictors of aortic growth in uncomplicated type B aortic dissection from the Acute Dissection Stent Grafting or Best Medical Treatment (ADSORB) database. J. Vasc. Surg. 2017, 65, 964–971.e3.
- Matsushita, A.; Tabata, M.; Mihara, W.; Shimamoto, T.; Komiya, T.; Takanashi, S.; Tobaru, T.; Nakao, T.; Nakamura, S.; Sato, Y. Risk score system for late aortic events in patients with uncomplicated type B aortic dissection. J. Thorac. Cardiovasc. Surg. 2020, 159, 2173–2183.e1.
- Sailer, A.M.; van Kuijk, S.M.; Nelemans, P.J.; Chin, A.S.; Kino, A.; Huininga, M.; Schmidt, J.; Mistelbauer, G.; Baumler, K.; Chiu, P.; et al. Computed Tomography Imaging Features in Acute Uncomplicated Stanford Type-B Aortic Dissection Predict Late Adverse Events. Circ. Cardiovasc. Imaging 2017, 10, e005709.
- Ante, M.; Mylonas, S.; Skrypnik, D.; Bischoff, M.S.; Rengier, F.; Brunkwall, J.; Bockler, D. Prevalence of the Computed Tomographic Morphological DISSECT Predictors in Uncomplicated Stanford Type B Aortic Dissection. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 525–533.
- DeBakey, M.E.; Beall, A.C., Jr.; Cooley, D.A.; Crawford, E.S.; Morris, G.C., Jr.; Garrett, H.E.; Howell, J.F. Dissecting aneurysms of the aorta. Surg. Clin. North Am. 1966, 46, 1045–1055.
- Booher, A.M.; Isselbacher, E.M.; Nienaber, C.A.; Trimarchi, S.; Evangelista, A.; Montgomery, D.G.; Froehlich, J.B.; Ehrlich, M.P.; Oh, J.K.; Januzzi, J.L.; et al. The IRAD classification system for characterizing survival after aortic dissection. Am. J. Med. 2013, 126, 730.e19–730.e24.
More
Information
Subjects:
Primary Health Care
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
2.6K
Entry Collection:
Hypertension and Cardiovascular Diseases
Revisions:
2 times
(View History)
Update Date:
04 Nov 2022
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No