 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Diego Matías Vergara | -- | 6448 | 2022-05-06 16:25:10 | | | |
| 2 | Diego Matías Vergara | -4527 word(s) | 1921 | 2022-06-26 04:41:56 | | | | |
| 3 | Diego Matías Vergara | Meta information modification | 1921 | 2022-06-26 04:43:45 | | | | |
| 4 | Amina Yu | -368 word(s) | 1553 | 2022-06-27 04:18:42 | | | | |
| 5 | Amina Yu | Meta information modification | 1553 | 2022-06-27 04:20:31 | | |
Video Upload Options
Ischemia-reperfusion myocardial damage is a paradoxical tissue injury occurring during percutaneous coronary intervention (PCI) in acute myocardial infarction (AMI) patients. Although this damage could account for up to 50% of the final infarct size, there has been no available pharmacological treatment until now. Oxidative stress contributes to the underlying production mechanism, exerting the most marked injury during the early onset of reperfusion. So far, antioxidants have been shown to protect the AMI patients undergoing PCI to mitigate these detrimental effects; however, no clinical trials to date have shown any significant infarct size reduction. Myocardial ischemia/reperfusion damage results from diverse oxidative stress producing mechanisms.
1. Introduction
2. Mechanisms of Ischemia/Reperfusion damage
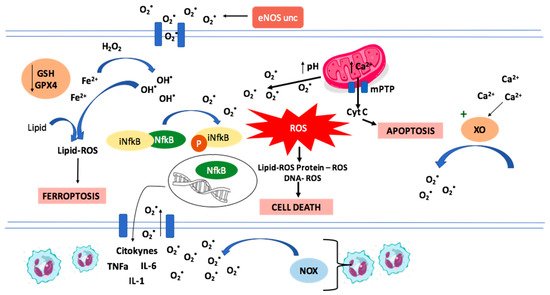
During myocardial ischemia there is an overload in intracellular Ca2+ that cannot be captured by the Ca2+ ATPase (SERCA) in the sarcoplasmic reticulum due to the lack of ATP. The overload of Ca2+ induces enzymatic changes. One of them is the conversion of xanthine dehydrogenase in endothelial cells to xanthine oxidase (XO), an enzyme that generates superoxide anion radicals [5]. Another example is the oxidation of tetrahydrobiopterin and the subsequent uncoupling of endothelial nitric oxide synthase (eNOS), resulting in superoxide production instead of nitric oxide [6]. These changes are related to a burst in ROS production during reperfusion, overwhelming the antioxidant defenses.
There are multiple mechanisms involved in cellular damage and subsequent cellular death during the ischemia/reperfusion (I/R) process. Some of them involves endoplasmic reticulum stress, mitochondrial dysfunction, and inflammation mediated damage. This myocardial cellular injury is mediated through necrosis, apoptosis and even ferroptosis.
3. Defense Mechanisms against Oxidative Stress
4. Resveratrol
Resveratrol is a natural polyphenol with multiple biological activities [8]. Different one have evidenced that it has various properties, including anti-inflammatory, antioxidant, anti-diabetic, antihypertensive, anti-cancerous and cardioprotective effects [8][9]. Some of the pathways involved in its cardioprotective protective effects will be reviewed.
SIRT1 regulates oxidative stress-related proteins and other proteins that affect the function of cardiomyocytes. Resveratrol was proposed as a SIRT1 activator, resulting in a cardioprotective response via reduction of Ca2+ overload [10]. Accordingly, recent studies on mice demonstrates that resveratrol determines the increase of SIRT1 levels during I/R injury, resulting in a decrease in the incidence of atrioventricular block and letality, and a decrease of UCP-2 expression, an apoptosis mediator [8][11].
4.2. Ferroptosis Inhibition
The addition of Resveratrol in cell cultures reduced oxidative stress and the content of Fe2+. The effect was explained by changes in the regulation of gene expression, in which resveratrol down-regulated transferrin receptor 1 expression and up-regulated the expression of ferritin heavy chain 1 and GPX4, leading to inhibition of ferroptosis and potentiation of the antioxidant defenses, respectively [12].
4.3. Attenuation of Inflammation and Apoptosis
Different studies have suggested that resveratrol might inhibit apoptosis through multiple ways. One of them is the activation of PI3K/AKT signaling pathway, which down-regulates the expression of apoptotic genes and regulates cell proliferation [13][14], leading to decreased ROS levels, increased catalase and glutathione peroxidase activities, and increased cell viability [15]. Also, resveratrol could reduce caspase 3 expression [16]. Moreover, resveratrol attenuates necroptosis after I/R injury by inhibition of TNF-α/RIP1/RIP3/MLKL signaling pathway [17]. Effects evidenced in a dose-dependent manner. Furthermore, resveratrol treatment resulted in a significant reduction of inflammatory mediators in serum and cardiac tissue cells [18].
4.4. Nrf2 Activation
The beneficial effects of resveratrol in I/R injury could also be mediated via up-regulation of Keap1/Nrf2 signaling pathway. Nrf2 up-regulates the expression of proteins involved in the antioxidant response. This is suggested due to the reversion of the beneficial effects of resveratrol when a knock down or inhibition of Nrf2 is ensued [19].
4.5. Reduced Mitochondrial Dysfunction
A recent study suggested that resveratrol via activation of PI3K/AKT signaling pathway, reduced mitochondrial oxidative stress damage, increasing catalase, and glutathione peroxidase activity, and cell viability [15].
4.6. Associations between Resveratrol and Other Antioxidants
Resveratrol interferes with many of the mechanisms underlying myocardial I/R injury, but there are others that are not covered by it. In this context, it is reasonable to propose an association of resveratrol with other antioxidant compounds that have their effects on other targets. As an example, vitamin C down-regulates NOX activity and prevent eNOS uncoupling, which could synergize with the increased expression of antioxidant enzymes induced by resveratrol via Nrf2 signaling pathway activation.[7].
5. Quercetin
Quercetin is a flavonoid with anti-aggregating, anti-cancer, anti-inflammatory, anti-aging, and antioxidant properties. It is not toxic even in high doses, and recent studies have shown it to have tremendous potential to reduce myocardial damage that occurs after I/R. Although Que has a low bioavailability, many efforts are being made to increase its solubility [20][21].
5.1. Properties of Quercetin against Oxidative Stress
Quercetin treatment has demonstrated to reduce oxidative stress through several mechanism. It reduces xanthine oxidase expression and activity [22] [23], and attenuate the expression of NOX2, which is one of the more active isoforms of NOX during I/R injury. Also, quercetin can significantly inhibit Fenton reaction, another relevant source of ROS [24]. Moreover, quercetin administration increased the selenoprotein TrxR2, which acts as an antioxidant and an indirect redox activity modulator [25] [26].
5.2. Anti-Inflammatory and Anti-Apoptotic Effects
Acute inflammatory reactions are intensified in cardiomyocytes following I/R injury. This is due to the neutrophilic granulocytes, which are the ones that explain most of the reduced exudation and even the diffusion of these neutrophils through the blood vessels. Inflammation alter the function of endotheliocytes, reduce the relaxation capacities of coronary arteries, and promote coagulation [27]. Quercetin has been shown to improve inflammation and apoptosis of the myocardial tissue, resulting in a decrease of the final infarct size [28].
5.3. Associations between Quercetin and Other Antioxidants
Not many associations have been tested, one of them is quercetin and α-tocopherol in rats. The combined pretreatment normalized all biochemical parameters and minimized ECG alterations, exhibiting enhanced cardioprotective effects against isoproterenol-induced cardiotoxicity. Furthermore, the combined pretreatment was more effective than each of them separately [29]. The combination of quercetin and lycopene in an animal model also prevented myocardial damage induced by isoproterenol, reducing oxidative stress [30].
6. Concluding Remarks
Ischemia/reperfusion injury occurring in AMI patients undergoing PCI is a complex process involving pathophysiological cascades leading to cellular disturbances ranging from metabolic changes to cell death. The administration of several antioxidant molecules could give rise to an additive or synergistic pharmacological effect, leading to an improvement of previous studies on antioxidants that use them on monotherapy. tudies about associations of these compounds with others that have previously shown cardioprotective effects could be analyzed in isolated heart rat Langendorff model and, subsequently, in clinical trials aimed to reduce the infarct size due to the increased efficacy of this therapeutic association. This could lead to a better prognosis and quality of life after an acute myocardial infarction, decreasing complications, such as heart failure and arrhythmias, and reducing the associated costs.
Even if effective clinical treatment for I/R injury has not been found yet, resveratrol and quercetin constitute attractive natural pharmacological agents to be used in a combined therapy aimed to reduce cardiac tissue damage and infarct size due to their cardioprotective effects. Randomized double-blind clinical trials should be made to test the therapeutic efficacy as well as safety of these associations.
References
- World Health Organization. Cardiovascular Diseases. 2019. Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 (accessed on 10 November 2021).
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; Alkatheeri, R.; Alblooshi, F.M.K.; Almatrooshi, M.E.A.H.; Alzaabi, M.E.H.; Al Darmaki, R.S.; et al. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 2020, 12, e9349.
- Yellon, D.M.; Hausenloy, D.J. Myocardial reperfusion injury. N. Engl. J. Med. 2007, 357, 1121–1135.
- Rodrigo, R.; González-Montero, J.; Sotomayor, C.G. Novel Combined Antioxidant Strategy against Hypertension, Acute Myocardial Infarction and Postoperative Atrial Fibrillation. Biomedicines 2021, 9, 620.
- Sasaki, M.; Joh, T. Oxidative stress and ischemia-reperfusion injury in gastrointestinal tract and antioxidant, protective agents. J. Clin. Biochem. Nutr. 2007, 40, 1–12.
- Raedschelders, K.; Ansley, D.M.; Chen, D.D. The cellular and molecular origin of reactive oxygen species generation during myocardial ischemia and reperfusion. Pharmacol. Ther. 2012, 133, 230–255.
- Rodrigo, R.; Libuy, M.; Feliú, F.; Hasson, D. Molecular basis of cardioprotective effect of antioxidant vitamins in myocardial infarction. Biomed. Res. Int. 2013, 2013, 437613.
- Li, T.; Tan, Y.; Ouyang, S.; He, J.; Liu, L. Resveratrol protects against myocardial ischemia-reperfusion injury via attenuating ferroptosis. Gene 2021, 808, 145968.
- Pastor, R.F.; Restani, P.; Di Lorenzo, C.; Orgiu, F.; Teissedre, P.L.; Stockley, C.; Ruf, J.C.; Quini, C.I.; Garcìa Tejedor, N.; Gargantini, R.; et al. Resveratrol, human health and winemaking perspectives. Crit. Rev. Food Sci. Nutr. 2019, 59, 1237–1255.
- Sulaiman, M.; Matta, M.J.; Sunderesan, N.R.; Gupta, M.P.; Periasamy, M.; Gupta, M. Resveratrol, an activator of SIRT1, upregulates sarcoplasmic calcium ATPase and improves cardiac function in diabetic cardiomyopathy. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, H833–H843.
- Deng, M.; Wang, D.; He, S.; Xu, R.; Xie, Y. SIRT1 confers protection against ischemia/reperfusion injury in cardiomyocytes via regulation of uncoupling protein 2 expression. Mol. Med. Rep. 2017, 16, 7098–7104.
- Lochner, A.; Marais, E.; Huisamen, B. Melatonin and cardioprotection against ischaemia/reperfusion injury: What’s new? A review. J. Pineal Res. 2018, 65, e12490.
- Pompura, S.L.; Dominguez-Villar, M. The PI3K/AKT signaling pathway in regulatory T-cell development, stability, and function. J. Leukoc. Biol. 2018, 103, 1065–1076.
- Zhang, X.; Huang, L.F.; Hua, L.; Feng, H.K.; Shen, B. Resveratrol protects myocardial apoptosis induced by ischemia-reperfusion in rats with acute myocardial infarction via blocking P13K/Akt/e-NOS pathway. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1789–1796.
- Yu, D.; Xiong, J.; Gao, Y.; Li, J.; Zhu, D.; Shen, X.; Sun, L.; Wang, X. Resveratrol activates PI3K/AKT to reduce myocardial cell apoptosis and mitochondrial oxidative damage caused by myocardial ischemia/reperfusion injury. Acta Histochem. 2021, 123, 151739.
- Ge, L.; Li, C.; Wang, Z.; Zhang, Y.; Chen, L. Suppression of Oxidative Stress and Apoptosis in Electrically Stimulated Neonatal Rat Cardiomyocytes by Resveratrol and Underlying Mechanisms. J. Cardiovasc. Pharmacol. 2017, 70, 396–404.
- Hu, Y.; Pan, H.; Peng, J.; He, J.; Tang, M.; Yan, S.; Rong, J.; Li, J.; Zheng, Z.; Wang, H.; et al. Resveratrol inhibits necroptosis by mediating the TNF-α/RIP1/RIP3/MLKL pathway in myocardial hypoxia/reoxygenation injury. Acta Biochim. Biophys. Sin. 2021, 53, 430–437.
- Xing, Z.; He, Q.; Xiong, Y.; Zeng, X. Systematic Pharmacology Reveals the Antioxidative Stress and Anti-Inflammatory Mechanisms of Resveratrol Intervention in Myocardial Ischemia-Reperfusion Injury. Evid. Based Complement. Altern. Med. 2021, 2021, 5515396.
- Song, X.; Liu, Z.; Zeng, R.; Shao, J.; Zheng, Y.; Ye, W. Resveratrol Alleviates Vascular Endothelial Damage Caused by Lower-Extremity Ischemia Reperfusion (I/R) through Regulating Keap1/Nrf2 Signaling-Mediated Oxidative Stress. Evid. Based Complement. Altern. Med. 2021, 2021, 5556603.
- Zhang, L.; Dong, M.; Xu, G.; Tian, Y.; Tang, H.; Wang, Y. Metabolomics Reveals that Dietary Ferulic Acid and Quercetin Modulate Metabolic Homeostasis in Rats. J. Agric. Food Chem. 2018, 66, 1723–1731.
- Jiang, W.; Zhang, H.; Wu, J.; Zhai, G.; Li, Z.; Luan, Y.; Garg, S. Well-Designed Quercetin Delivery System for Chemo-Photothermal Therapy. ACS Appl. Mater. Interfaces 2018, 10, 34513–34523.
- Huang, J.; Wang, S.; Zhu, M.; Chen, J.; Zhu, X. Effects of genistein, apigenin, quercetin, rutin and astilbin on serum uric acid levels and xanthine oxidase activities in normal and hyperuricemic mice. Food Chem. Toxicol. 2011, 49, 1943–1947.
- Wan, L.L.; Xia, J.; Ye, D.; Liu, J.; Chen, J.; Wang, G. Effects of quercetin on gene and protein expression of NOX and NOS after myocardial ischemia and reperfusion in rabbit. Cardiovasc. Ther. 2009, 27, 28–33.
- Jomova, K.; Lawson, M.; Drostinova, L.; Lauro, P.; Poprac, P.; Brezova, V.; Michalik, M.; Lukeš, V.; Valko, M. Protective role of quercetin against copper(II)-induced oxidative stress: A spectroscopic, theoretical and DNA damage study. Food Chem. Toxicol. 2017, 110, 340–350.
- Zhang, J.; Huang, L.; Shi, X.; Yang, L.; Hua, F.; Ma, J.; Zhu, W.; Liu, X.; Xuan, R.; Shen, Y.; et al. Metformin protects against myocardial ischemia-reperfusion injury and cell pyroptosis via AMPK/NLRP3 inflammasome pathway. Aging 2020, 12, 24270–24287.
- Steinbrenner, H.; Speckmann, B.; Klotz, L.O. Selenoproteins: Antioxidant selenoenzymes and beyond. Arch. Biochem. Biophys. 2016, 595, 113–119.
- Akhlaghi, M.; Bandy, B. Mechanisms of flavonoid protection against myocardial ischemia-reperfusion injury. J. Mol. Cell. Cardiol. 2009, 46, 309–317.
- Tang, S.T.; Wang, F.; Shao, M.; Wang, Y.; Zhu, H.Q. MicroRNA-126 suppresses inflammation in endothelial cells under hyperglycemic condition by targeting HMGB1. Vascul. Pharmacol. 2017, 88, 48–55.
- Punithavathi, V.R.; Stanely Mainzen Prince, P. The cardioprotective effects of a combination of quercetin and α-tocopherol on isoproterenol-induced myocardial infarcted rats. J. Biochem. Mol. Toxicol. 2011, 25, 28–40.
- Chen, L.; Wu, X.; Wang, W.; Wang, X.; Ma, J. Quercetin with lycopene modulates enzymic antioxidant genes pathway in isoproterenol cardiotoxicity in rats. Libyan J. Med. 2021, 16, 1943924.
- Kim, E.N.; Lim, J.H.; Kim, M.Y.; Ban, T.H.; Jang, I.A.; Yoon, H.E.; Park, C.W.; Chang, Y.S.; Choi, B.S. Resveratrol, an Nrf2 activator, ameliorates aging-related progressive renal injury. Aging 2018, 10, 83–99.
- Luo, M.; Tian, R.; Yang, Z.; Peng, Y.Y.; Lu, N. Quercetin suppressed NADPH oxidase-derived oxidative stress via heme oxygenase-1 induction in macrophages. Arch. Biochem. Biophys. 2019, 671, 69–76.
- Zhang, C.; Wang, R.; Zhang, G.; Gong, D. Mechanistic insights into the inhibition of quercetin on xanthine oxidase. Int. J. Biol. Macromol. 2018, 112, 405–412.


