Ischemia-reperfusion myocardial damage is a paradoxical tissue injury occurring during percutaneous coronary intervention (PCI) in acute myocardial infarction (AMI) patients. Although this damage could account for up to 50% of the final infarct size, there has been no available pharmacological treatment until now. Oxidative stress contributes to the underlying production mechanism, exerting the most marked injury during the early onset of reperfusion. So far, antioxidants have been shown to protect the AMI patients undergoing PCI to mitigate these detrimental effects; however, no clinical trials to date have shown any significant infarct size reduction. Therefore, it is worthwhile to consider multitarget antioxidant therapies targeting multifactorial AMyocardial ischemia/I. Indeed, this clinical setting involves injurious effects derived from oxygen deprivation, intracellular pH changes and increased concentration of cytosolic Ca2+ and reactive oxygen species, among others. Thus, we will review a brief overview of the pathological cascades involved in ischemia-reperfusion damage results from diverse oxidative stress producing mechanisminjury and the potential therapeutic effects based on preclinical studies involving a combination of antioxidants, with particular reference to resveratrol and quercetin, which could contribute to cardioprotection against ischemia-reperfusion injury in myocardial tissue. We will also highlight the upcoming perspectives of these antioxidants for designing future studies.
1. Introduction
ECardiov
en if treatascular disease is the most common cause of morbidity and mortality worldwide, with 17.9 million deaths every year, according to updated WHO data from the year 2017, which represents 31% of all registered deaths in the world [1]. Am
ong cardiovascular dise
nt for ischeases, stroke and acute myocardial infarct (AMI) are the main causes of death, the latter being responsible for around 9 million deaths each year [2]. AMI is produced by either partial or com
plete occlusi
a-reperfuon of the coronary arterial circulation. It is mainly caused by atheromatous plaques that are vulnerable to rupture or erosion causing thrombotic alterations that block blood flow to cardiac tissue [3]. The current gold s
tandard treatment for AMI i
on (I/R) is percutaneous coronary intervention (PCI), a procedure whose objective is to restore the arrival of blood flow to the ischemic heart tissue [4]. Paradoxically, the restoration
j of blood flow to ischemic myocardial tissue induces additional damage. Studies in animal models of AMI have suggested that myocardial reperfu
rsion is responsible for up to 50% of the final infarct size [3]. One of the key
factors involved is oxidative stress, wh
as not been ich influences myocardial reperfusion via multiple pathological mechanisms. Consequently, the antioxidant defense system could become overwhelmed, thus resulting in oxidative damage and, ultimately, cell death [5]. Numerous attempts have been perfo
rmed to redu
nd yet, resveratrce myocardial tissue damage after ischemia-reperfusion (I/R) by enhancing the antioxidant defense system with antioxidant treatments. Accordingly, the administration of molecules such as vitamin C, vitamin E, N-acetylcysteine, deferoxamine and polyphenols, among others, has been studied [6]. Ho
wever, these therapies have l
and quercetin coned to suboptimal and inconsistent results. As a consequence, until today, there is no reliable therapy against I/R damage for these patients. It still remains a challenge to find an effective therapeutic strategy that can prevent such damage and decrease infarct size after reperfusion by PCI.
2. Oxidative Stress
2.1. Oxidative Stress and ROS
Oxidative stress
result
itute atts from the imbalance between free radicals production and the antioxidant defense system [10]. Under
oxida
ctive natural ptive stress conditions, two kinds of reactive species are produced, reactive oxygen species (ROS), such as radical anion superoxide, hydrogen peroxide, hydroxyl radical and reactive nitrogen species (RNS), which include nitric oxide radical, nitrogen dioxide radical, and peroxynitrite [11].
ROS can be formed by enzymatic or non-enzymatic mediated processes. Enzymatic ROS sources include reduced nicotinamide adenine dinucleotide ph
ospha
rmacologte oxidase (NADPH oxidase or NOX), xanthine oxidase (XO), uncoupled endothelial nitric oxide synthase (eNOS), among others [12]. In addi
tion, an example of the non-enzymatic
al agents to be used in a combine mechanisms of ROS production is the direct generation of hydroxyl radicals via Fenton and Haber–Weiss reactions, both of which depend on the availability of transition metal ions such as free iron in the form of labile iron pool (LIP). The hydroxyl radical is highly reactive and of low specificity, making it capable of damaging more biomolecules than any other ROS [13].
2.2. Mechanisms of Ischemia/Reperfusion Cellular Damage
The mechanisms accounting for I/R damage tare depicted in Figure 1.
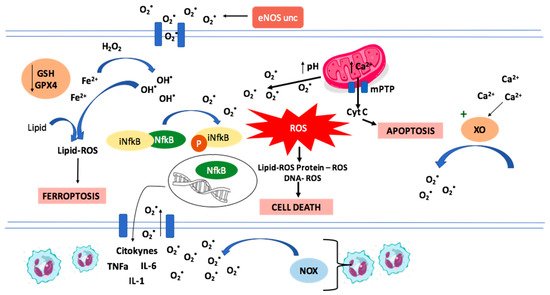
Figure 1. Representation of mechanisms involved in Ischemia/Reperfusion damage. The increase in intracellular calcium concentration is related to the activation of xanthine oxidase, a pro-oxidant enzyme. The increase in intramitochondrial calcium and the pH increase during reperfusion lead to the opening of mPTP and the loss of mitochondrial transmembrane potential, associated with ROS production. Reactive oxygen species activate the NFκB transcription factor, promoting inflammation and neutrophil migration to the injury zone and increasing ROS production by NADPH oxidase. Another ROS source is the uncoupled eNOS. Reactive oxygen species peroxidize lipids, proteins, and DNA, triggering cell death, together with apoptosis that happens from the release of cytochrome c through mPTP and ferroptosis that occurs in the context of a decrease in GSH and GPX4 activity, with accumulation of lipid peroxidation products.
2.3. ROS Production in Ischemia/Reperfusion
The
occlusion of a cor
apy aimonary artery branch inhibits blood flow to myocardial tissue causing regional ischemia [14]. During myocardial ischemia, the
d
to reduce cardiac tissue damaecrease in the oxygen supply in cardiac tissue causes a marked reduction of oxygen supply to the mitochondrial electron transport chain, leading to a shift from aerobic to anaerobic cellular respiration. Consequently, a decrease in ATP production ensues, accompanied by lactic acid accumulation and a decrease in cellular pH [15]. The pH acidification increases the Na+ influx throug
h the
Na
+/H+ exchan
ger, and
ithe lack of ATP decreases the activity of the Na+/K+ pump, leadin
g to an increase in intracellular Na+ that activates the Ca2+/Na+ exchanger to f
unction in a
rct siz reverse direction, thus exchanging intracellular Na+ with extracellular Ca2+ [16]. As a result, there is an overload in intracellular Ca2+ that cannot be captured by the Ca2+ ATPase (SERCA) in the
sarcoplasmic reticulum due to t
he lack of ATP [17]. The
overload of i
r ntracellular Ca2+ induc
es enzymes cha
rdioprotective enges. One of them is the conversion of xanthine dehydrogenase in endothelial cells to xanthine oxidase (XO), an enzyme that generates superoxide anion radicals, contributing to the induction of oxidative stress [18]. Furthermore, during cardiac ischemia, tetrahydrobiopterin, a cof
actor of
ects. Randomiz endothelial eNOS, is oxidized, causing eNOS to get uncoupled and produce superoxide instead of nitric oxide. These changes are related to a burst in ROS production that has been found once reperfusion has restored oxygen supply to the myocardial tissue [19]. Exace
rbation of oxid
double-blind ative stress during reperfusion overwhelms the endogenous antioxidant defenses, causing direct damage by lipid peroxidation, DNA oxidation and protein carbonylation, effects that can progress until cell death [19,20]. The main effec
tors of this damage are peroxynitrite and hydroxyl
inica radicals generated from Fenton/Haber–Weiss reactions and [19].
Other ROS sources in cardiac tissue exposed to ischemia-reperfusion are NADPH oxidase in neutrophil
s, trials smitochondrial electron transport chain (mETC), cytochrome P450, lipooxygenase (LOX), cyclooxygenase, and monoamine oxidase [21].
3. Intracellular Organelle Dysfunctions Associated with Ischemia/Reperfusion Injury
3.1. Endoplasmic Reticulum Stress (ERS)
Endoplasmic reticulum stress h
as been described as another potential mechanism o
uld be made to test the therapf I/R injury. It results from the accumulation of unfolded proteins in the endoplasmic reticulum, leading to an imbalance in calcium ion homeostasis and the activation of the unfolded protein response (UPR), a signaling pathway aimed to counteract the stress conditions effects otherwise leading to cell apoptosis [22]. Protein kinase-like ER kinase (PERK) is one of the
sensors of stress that activate and coordinate the cell response following UPR activation. In particu
tic efficacy as well alar, PERK may participate via the ERS-PERK signaling pathway in mediating the translocation and activation of the pro-survival nuclear factor erythroid 2-related factor 2 (Nrf2), suggesting that its influence on cell survival may be closely associated with regulating Nrf2/ARE signaling pathway [23].
3.2. Mitochondrial Dysfunction
Mitochondrial permeability trans
ition safety of these pore (mPTP) is a protein channel located in the inner mitochondrial membrane involved in necrotic and apoptotic cell death. When mPTP opens, it can induce the uncoupling of oxidative phosphorylation. Under ischemic conditions, the acid pH induced by lactate accumulation has an inhibitory effect on the mPTP, causing it to close [24]. La
ter, within the firs
sot few minutes of reperfusion [25], the intrac
ellular acidi
ationc pH is restored to physiological values due to the reabsorption of lactate, and a mitochondrial Ca2+ overload ens
ues [1][26].
Furthermore, mPTP opens due to mitochondrial oxidative stress [27], uncoupling the oxidative phosphorylation Eand decreasing intracellular ATP av
en ailability, which can induce cell death through the mitochondrial pathway [26]. In addi
tion, mPTP-induced cell death could be caused by the transport of
treatment for molecules less than 1.5 kDa by mPTP, which collapses the mitochondrial membrane potential. Other consequences of mPTP opening are mitochondrial matrix swelling and the release of mitochondrial proteins, activating cell death mechanisms, such as apoptosis, necrosis, and necroptosis [28]. Moreover, the loss of mitochondrial potential generates a rise in ROS production [29].
3.3. Inflammation Mediated Damage
The mechanism of I/R injury
his usually considered sterile. However, it displays a
s not been found yet series of inflammatory reactions resembling infectious processes such as inducing cytokines and chemokines production with infiltration of immune system cells [30,
31]. This inflammator
esveratrol and quercetin constitute y response is thought to function as a double-edged sword: on one side, it enables the removal of cell debris and promotes wound healing. Damage-associated molecular pattern (DAMP) mediated signaling can also exacerbate the inflammatory state in a disproportional matter, thereby leading to additional tissue damage. After reperfusion, neutrophil and monocyte become activated by many damage signals released by necrotic cells. The primary immune response expands tissue damage by inducing neutrophil, NLRP3-inflammasome [32] a
nd Toll-like recept
tractivor 9-pathogen recognition receptor activation [33], which conve
rge naturaon the activation of the myeloid differentiation primary response gene 88 (MyD88) and nuclear factor-κB (NF-κB) pathways [3] which in turn pol
arize pharmaT lymphocyte towards a pro-inflammatory phenotype.
4. Mechanisms of Cell Death in Ischemia-Reperfusion
Ferroptosis
Ferroptosis is a significant mec
hanism o
logicf injury in myocardial infarction and can be a promising target to reduce infarct size [42]. Ferroptosis consists of a
n iron-dependent, non-apoptotic form of cell
adeath [43]. It is a reg
ulate
nts to bd form of necrosis that is driven by oxidative stress and is characterized by the accumulation of lipid peroxidation products and ROS derived from iron metabolism.
Glutathione
peroxidase 4 (GPX4) is the key regu
slator of ferroptosis [43]. This e
nzyme transforms phospholipid
in a cohydroperoxides to lipid alcohols using reduced GSH, which inhibits ferroptosis and explains why it mostly happens when cellular GSH levels are low, or GPX4 is inhibited [44]. Inhibition of GPX4 activity can lead to the accum
bulation of lipid peroxides, which is a marker of ferroptosis [43]. During I/R, in
trace
d therapy allular reduced glutathione (GSH) decreases, as well as the activity of GPX4. Thus, lipid peroxides cannot be reduced by GPX4, and Fe2+ oxi
dizes lipids in a Fenton-like m
eanner, resulting in a large amount of ROS concentration, which promotes ferroptosis.
Thus, iron metabolism is one of the main pathways of ischemia-reperfusion injury involved
in cell deat
h [42]. In animal mo
dels reduce of coronary artery ligation-induced myocardia
c til I/R injury, it has been observed that ferroptosis inhibition may repair cell damage and infarct size [43]. Iron is
trans
ue damage anported inside cardiomyocytes after recognition by the transferrin receptor 1 (TfR1) [45], and
Ferri
ntin (FT) is the main iron storage protein [13]. It is of
interest to remar
ct size dk that ferrous ionic free iron is a key ferroptosis inducer; therefore, this deleterious process could be inhibited by iron chelators [46].
5. Apoptosis
Stu
die
to theis performed in in vivo animal models have demonstrated the important role of apoptosis in cell death following I/R, particularly during the phase of reperfusion [47]. Ener
gy cardioprotective efrestoration characterizing reperfusion promotes the apoptotic process. Experiments in isolated rat hearts demonstrated that mitochondrial dysfunction and caspase activation occur after global ischemia and that caspase activation is dependent on the time of ischemia [48]. The opening of
the
cts mPTP and the changes in the mitochondrial transmembrane potential promote the release of pro-apoptotic proteins such as cytochrome c to the cytosol (23), leading to apoptotic cell death [49].
6. Defense Mechanisms against Oxidative Stress
Antioxidant systems regulate redox homeostasis by controlling the intracellular R
andomized double-blind clinOS levels and their interaction with biological molecules. This system has enzymatic and non-enzymatic mechanisms involved. Enzymes constitute the first line of antioxidative cellular defense; they are superoxide dismutase (SOD), glutathione peroxidase (GPX) and catalase (CAT). Non-enzymatic antioxidants can be exogenous or endogenous and include molecules such as vitamin C, vitamin E, reduced glutathione (GSH), carotenoids, flavonoids and polyphenols, among many others [50,51].
Anti
oxidants ac
al trials t by many mechanisms. Some of them are ROS scavenging or of their precursors, inhibiting ROS production, attenuating the catalysis of ROS generation via chelating metal ions, enhancing endogenous antioxidant generation, repairing the oxidative damage inflicted on the macromolecules and reducing apoptotic cell death by up-regulating the anti-apoptotic gene Bcl-2 [50]. Antioxidant enzymes
are encoded by several hou
ld bsekeeping genes largely controlled by Nrf2 [52].
7. Nrf2 Signalling Pathway
Nrf2 is a transcription factor conside
red an essential maderegulator for maintaining the redox balance [53] via inducing endogenous ant
o test ioxidant enzymes in response to oxidative stress [54]. Kelch-like ECH-associat
ed protein 1 (Keap1) is a cullin3-dependent E3 ubiquitin ligation substrate [55] and a suppressor protein th
at physically binds Nrf2 and re
therapeutains it in the cytoplasm so that it can be rapidly ubiquitinated and go to proteasomal degradation by the Cu3-Rbk1 complex [56]. Under oxidati
ve stress c
efonditions, intracellular ROS levels increase, and Keap1 undergoes conformational changes [57] that impair its ability to interact with Nrf
2, thus facilitati
cacy as well as sang the complex dissociation and preventing Nrf2 proteasomal degradation. Consequently, Nrf2 translocates into the nucleus and binds to the antioxidant response elements (ARE), located in the promoter region of target genes encoding antioxidant proteins, thereby enhancing their expression [36,58]
In summary, Nrf2/Kety of these associap1/ARE corresponds to a relevant signaling pathway that can attenuate myocardial infarct size after myocardial ischemia and reperfusion by up-regulation of antioxidant, anti-inflammatory, and autophagy mechanisms, which leads to a cardioprotective effect.
8. Exogenous Antioxidants with Reported Cardioprotective Effects
The potentia
l usefulness of antio
nsxidants as protective tools against [2]I/R damage has attracted enormous interest.
EClinical and experimental studies hav
en if treatment for I/R inje been performed to determine the ability of natural or synthetic compounds with antioxidant and anti-inflammatory properties to counteract the mechanisms responsible for tissue alteration during I/R and to identify the involved molecular pathways [66].
9. Resveratrol
Resveratrol is a natur
al poly
has phenol with multiple biological activities [90]. It has a molecular weight of 228.25 g/mol [8] an
d exists in two iso
t beenmeric forms (cis and trans), with the trans form being the most common with more therapeutic benefits [91]. This antioxidant is found
in many
et, res fruits and vegetables, such as grapes, Polygonum cuspidatum and mulberry [92].
Resveratrol
beca
nd querme of interest during the early 1990s when a French paradox study mentioned that it was beneficial for health [91]. Since
t
in constitute attractive nathen, this molecule has been the subject of numerous studies, and many physiological effects have been assigned to it. Different studies have evidenced that it has various properties, including anti-inflammatory, antioxidant, anti-diabetic, antihypertensive, anti-cancerous and cardioprotective effects [90,92].
10. Resveratrol Cardioprotective Mechanisms
10.1. SIRT1 Activation
Silent information regulator factor 2-related enzyme 1 (SIRT1) consists of a nicotinamide adenine dinucleotide-dependent deacetylase that regulates oxidative stress-related proteins and other proteins that affect the function of cardiomyocytes. It was proposed that resveratrol activates SIRT1 leading to the activation of a cardioprotective response, reducing the Ca2+ overload in the cytosol and mitochondria [95]. According to this theory, a recent study showed that in a rat model of cardiac I/R, 21-day oral treatment with resveratrol decreased the incidence of atrioventricular block and lethality, thus suggesting the usefulness of this natural compound in the prevention of lethal cardiac arrhythmias after reperfusion [90]. Furthermore, it has been demonstrated that intraperitoneal injection of resveratrol in mice determines the increase of SIRT1 levels and a concomitant decrease of UCP-2 expression, thus protecting myocardial tissue against I/R injury in vivo [96].
10.2. Ferroptosis Inhibition
In a recent stu
dy carr
al ied out by Li et al. [89], in vitro exp
eriments with
armacolo H9c2 cells and a model of oxygen-glucose deprivation/reoxygenation (OGD/R) demonstrated that OGD/R-induced H9c2 cells showed increased cell death by ferroptosis. The addition of resveratrol in cell cultures reduced oxidative stress and the content of Fe2+. In vivo experiments performed by the same authors in rats lig
ated and perfused by the left anteri
cal agentor descending branch showed that when resveratrol was administered at the concentration of 50 mg/kg for 14 days, oxidative stress and the content of Fe2+ decreas
ed to be used in a combined therapagain. The effect was explained by changes in the regulation of gene expression, in which resveratrol down-regulated transferrin receptor 1 expression and up-regulated the expression of ferritin heavy chain 1 and GPX4, leading to inhibition of ferroptosis and potentiation of the antioxidant defenses, respectively. The consequent reduction in oxidative stress is evidenced by a reduction in malondialdehyde (MDA) production [89].
10.3. Attenuation of Inflammation and Apoptosis
There are multiple way
s aiin which resveratrol might inhibit apoptosis. Yu et al. [97] studied rats the antioxidant and anti-apoptotic effects of resveratrol in m
yocardial I/R injury. Compared to
reduce cardiac tissue damage and inthe control, the resveratrol group showed decreased ROS levels, increased catalase and glutathione peroxidase activities, and increased cell viability by apoptosis inhibition. Further, a decrease in lactate dehydrogenase (LDH) and plasma creatine kinase MB (CK-MB) levels were found. They suggested that these effects were mediated by the activation of the PI3K/AKT signaling pathway, which down-regulates the expression of apoptotic genes and regulates cell proliferation [98,99]. Apparently, PI3K/AKT signaling pathway is inhibited during the I/R process, resulting in potent activation of
a
poptosis and less viable tissue [97,100]. Moreover, it has been suggested that r
esveratrol attenuates apoptosis by reduc
ing caspase 3 expression [101]. In anot
her s
tudy, Hu et al. [102] i
zndicate
due to their cardioprotective ed that resveratrol attenuates necroptosis after ischemia-reperfusion by inhibition of the tumor necrosis factor-alpha (TNF-α)/receptor-interacting protein kinase 1 (RIP1)/RIP3/mixed-lineage kinase domain-like (MLKL) signaling pathway. The results were that after treatment with different resveratrol concentrations, the expressions of TNF-α, RIP1, RIP3, and p-MLKL/MLKL decreased, as well as necroptosis. Under those circumstances, cell viability increased. All these effects
were seen in dose-dependent manners [102].
Xing et al. [103] measured the levels of serum interleukin-1β (IL-1β), IL-6, and TNF-a in rat myocardial tissue during I/R
injury. They a
ndolso measured the expressions of mRNA and proteins of Toll-like receptor 4 (TLR4), NF-κB, p65, IL-1β, IL-6, and TNF-α. Resveratrol treatm
ent resulted i
zed n a significant reduction of serum IL-1β, TNF-α, and
IL-6, TLR4, NF-κB, p65, IL-1β, IL-6, and TNF-α mRNA and pro
tein expressions in cardiac tissu
e cells [103].
10.4. Nrf2 Activation
As indicated b
efore, Nrf2 up-regul
e-blind clinicalates the expression of proteins involved in the antioxidant response. Using an in vitro hypoxia–reoxygenation (HR) model on HUVEC, it has been demonstrated that the increased cell viability and the reduced apoptotic rate and oxidative stress observed in cells treated with resveratrol were significantly reversed by knocking down Nrf2 [104]. Furt
rials should be mahermore, in a rat model of lower-extremity I/R, treatment with resveratrol improved the apoptotic state of the femoral artery and reduced oxidative stress; this effect was abolished by the co-administration of an inhibitor of Nrf2 [104]. These results ind
icate
to test the therathat resveratrol might attenuate the I/R injury damage through up-regulating Keap1/Nrf2 signaling, mainly for its effects on oxidative stress. This could increase cell viability and decrease the apoptotic rate [104].
10.5. Reduced Mitochondrial Dysfunction
A recent study demonstrated that the addition of resveratrol in an in vitro I/R model obtained with p
rimary rat cardiomyocyte
utic es decreased lactate dehydrogenase and creatine kinase MB release and ROS production and increased cell viability and catalase and glutathione peroxidase activities [97]. Moreover, resveratrol signif
icantly increases the activity of
icacy as well a mitochondrial superoxide dismutase and reduces the levels of malondialdehyde, indicating reduced oxidative damage to the mitochondria. The effects observed after resveratrol addition were reversed using PI3K siRNA, thus suggesting that the protective effect of resveratrol on cardiomyocytes under I/R conditions can be due to PI3K/AKT signaling pathway activation [97].
10.6. Other Pathways
It has
also been proposed that res
averatrol could reduce oxidative stress and protect myocardial cells via activating the VEGF-β/antioxidant signaling pathway [105]. Particularly, experiments conducted on rat hearts and on H9c2 cells showed that af
te
tyr treatment with resveratrol, a marked improvement of left ventricular function and a reduction of infarct size ex vivo, and decreased cell death and apoptosis of
H9c2 these ascells during I/R occurred. The treatment with resveratrol was associat
ioned with the up-regulation of VEGF-β mRNA and protein levels
, [3]which caused the activation of Akt and the inhibition of GSK3β. The inhibition of VEGF-β inhibited the cardioprotective effects of resveratrol [105]. O
f in
e of the key faterest, the treatment of cardiomyocytes with isorhapontigenin (ISO), a resveratrol analog, was able to counteract angiotensin (Ang) II-induced cardiac hypertrophy by inhibiting Ang-II-dependent phosphorylation of PKC, Erk1/2, JNK, and p38. The same authors also observed that pretreatment with ISO down-modulated Ang II-mediated NF-κB activation by affecting the degradation and phosphorylation of IκBα [106].
10.7. Considerations of Safety in the Use of Resveratrol
Resveratrol is one of the potential therapeutic
agent
ors is for the prevention of I/R heart tissue damage, but there are some issues that must be addressed. Shaito et al. [91] reviewed the poten
tial adv
olved is oxidative sterse effects of the use of resveratrol. Resveratrol showed a beneficial effect at low doses, and the optimal dosage with safer and higher potency is still under research. Resveratrol presents a hormetic effect, and high doses have toxic effects, including inhibition of p450 cytochromes, which leads to interaction with several drugs and pro-oxidant effects [107]. We should pay attention to this dose-dependent effect on the re
dox s
s, wtate (antioxidant at low doses and pro-oxidant at high ones), given the fact that we are focused on an antioxidant activity [91].
10.8. Associations between Resveratrol and Other Antioxidants
Different pathways and mechanich influences myosms participate in the generation of I/R injury. Even though resveratrol interferes with many of those mechanisms to reduce and/or prevent I/R damage, others are not covered by it. Therefore, it is reasonable to think that it would be beneficial to propose an association of resveratrol with other natural antioxidants, looking for a synergic effect able to reduce the damage as much as possible. Until now, associations of resveratrol with other antioxidants or clinical drugs have not been studied. As a result, in the search for the most beneficial multitarget therapeutic scheme, we propose that there could be a synergistic effect between vitamin C and deferoxamine.
Resveratrol is assoc
ia
rdial reperfusion via multiplted with activating the Nrf2 signaling pathway, which leads to an increased expression of antioxidant enzymes, potentiating the antioxidant response. Theoretically, the balance would be even more inclined to favor this response if we decrease the function of pro-oxidant enzymes. In this context, adding vitamin C would be beneficial as it down-regulates NADPH oxidase activity and prevents eNOS uncoupling [50]. Furthe
r, it reduces intracellular Ca2+ overload and p
revents the depola
tholrization of the mitochondrial membrane [67]. These two
last effects are related to SIRT1 activation by resveratrol, while it has been seen in studies showing
ica that vitamin C also increases the expression of SIRT1 [109]. Even if this coul
d mecconstitute a potential interference between both antioxidants, it is necessary to look further into the molecular mechanisms
. Numerous involved to determine whether it would potentiate or antagonize the effect of resveratrol. It is worth mentioning that vitamin C is a water-soluble vitamin and can be administered intravenously [110].
11. Quercetin
Quercetin (Que) is a fla
vonoid wit
temh the following chemical formula C15H10O7 [111].
Flavonoids are comp
ounds wit
s have been peh very different conformations. They are hydrophobic, as they have two benzene rings and a pyran ring between them [112]. Flavonoids exist in most plants and account for
65–75% of
or our daily flavonoid intake [113], m
ainly in ve
d to reduce mgetables and fruits, and also have a strong antioxidant property attributed to the presence of five hydroxyl groups, together with the pyrocatechol, which makes them good scavengers of free radicals [114]. Unfortunately
, despite being very pro
cardial tissue damage after iscmising, Que is a molecule with low bioavailability due to its low aqueous solubility. However, many efforts have been devoted to increasing its solubility to obtain analogs with potentially improved properties. Quercetin can be rapidly hydrolyzed in the digestive tract by the enzyme β-glucosidase, which will facilitate its absorption through the intestinal mucosa, to be finally transferred to all the rest of the organism through portal circulation [115]. It also h
as several other biological effects in addition to its antioxidant prope
mia-rerties. It has anti-aggregating, anti-inflammatory, anti-cancer, and anti-aging effects. Furthermore, it is not toxic even in high doses (4000 mg/day) [116]. Additionally, recent studies have shown it to have tremendous p
ote
rfusintial to reduce myocardial damage that occurs after I/R through various mechanisms.
1.10.1. Properties of Quercetin against Oxidative Stress
Recent experiments with an animal mo
del of hyperuricemia have demon
(I/R) strated a reduction in xanthine oxidase expression and enzyme activity by Que treatment (100, 200, 400 mg/Kg) [9]. Xanthine oxidase is a molyb
do-flavoenzy
enhancing the antioxidant defenme found in various species. It is a homodimer with two symmetrical monomers. It has a great affinity for producing ROS because, in each of the monomers, there is a C-terminal molybdo protein that contains four redox centers. In turn, it has an N-terminal domain with two iron–sulfur centers and a central flavin adenine dinucleotide cofactor [118]. Thus
, xanthine
soxidase stimulates ROS production, which can end up causing oxidative stress injuries [119].
Similarly
, Que can attenuate the expres
sion of NOX2 [120]. The NADPH oxidase system
wis a multiprotei
th antion complex that produces ROS in different cells and tissues, being of great importance in phagocytic cells [121]. The NADPH oxida
se en
t treatmzyme is composed of several subunits, including the gp91-phox subunit and its counterparts which are commonly known as the NOX family (NOX1, NOX2, NOX3, NOX4, NOX5, DUOX1, and DUOX2) [122] that are
foun
tsd in almost all cells of the organism [123].
In the cardiovascular system, this complex is the main ROS producer, which is achieved through the transfer of an electron from NA
DPH to O2, resulting in NADP and O2●−. The newly produc
ed O2●− will end up rapidly transforming into H2O2, c
haracterized by being mor
die stable and diffusible [124]. This leads us to thin
gk that if we initially
, the inhibit the expression of the enzyme, we will reduce the production of H2O2 a
nd
ministratio, consequently, decrease the I/R damage produced by ROS in the myocardial tissue. In cardiomyocytes, NADPH oxidase can be activated by various mechanisms and stimulating factors [125]. Amon
g of molthem, one of the stimulants for the enzyme corresponds to I/R, with NOX2 and NOX4 being the ones more activated during myocardial I/R injury [82]. Therefore, the inhibitory effec
t of Qu
lee on NOX can potentially be a great target to ameliorate the injury induced by I/R.
In addition, Que combined with Fe2+/Cu+ will s
ignificantly sucinhibit Fenton reaction, another ROS source producing ●OH [126]. Fenton reaction consists of th
e as electron transfer from Fe2+/Cu+ metallic ion to H2O2, which produces Fe3+/Cu2+, OH− and ●OH. It has been shown that ●OH has a v
ery strong oxi
tadability in acid solutions [127]. Then also, H2O2 can restore Fe2+/Cu+ from
Fe3+/Cu2+, whi
ch produces HOO● an
d H+. Fe2+/C
u+ can be oxidized by O2 again,
which forms O2●−. In I/R damage, an acidic envi
ronment
a is created due to anaerobic glycolysis, which then facilitates the production of the Fenton reaction.
Selenium
i
n E, N-acetylcys an antioxidant and a component of selenoproteins, including glutathione peroxidases (GPX), thioredoxin reductases (TrxR) and methionine sulfoxide reductase 2, thereby modulating redox activity [128]. Accordingly, it has
been observed t
eine, dehat after Que administration at a dose of 50 mg/kg for eight weeks, the selenoprotein TrxR2 increased in the Que group compared to the control [82].
Quercetin is recognized as a signif
icant antioxidant, preventing damage
roxamine and p to cardiomyocytes as measured by oxidative stress, avoiding ROS increase and progression of damage after I/R. Moreover, ROS removal may increase NO bioavailability and restoration of endothelial function after I/R damage [129]. The mechanisms whereby Que exerts its antioxidant activity consist of eliminating ROS thro
ugh its abil
yity to react with the free radicals O2●−, HO●, NO, alkoxy and p
eroxyl. It also occurs when
ols, amo the hydroxyl attached to the benzene ring transfers a hydrogen atom or an electron to the free radical, resulting in the formation of more stable molecules [130]. Quercetin
also acts throug
others, has been h indirect mechanisms, restoring inherent antioxidant systems of the body, such as enzymatic systems dependent or not on antioxidants, such as vitamins C and E, and reduced glutathione (GSH) [59], the latter decreas
ing aft
udieder I/R injury, which indicates the depletion [4]of the antioxidant system.
Thus, it can eliminate RO
ne oS and restore the function of the
kintrinsic antioxidant system [131].
1.10.2. Anti-Inflammatory and Anti-Apoptotic Effects
Acute
inflammatory
factors involved is reactions are intensified in cardiomyocytes following I/R injury. This is due to the neutrophilic granulocytes, which are the ones that explain most of the reduced exudation and even the diffusion of these neutrophils through the blood vessels. Thus, it can be generated more damage to the injured tissue [132]. In the I/R perio
d, leukocytes can alter the function of endotheliocytes and reduce the relax
iation capacity of the coronary arteries [133]. They also promote coagulation and
pro-inflammat
ive stressory effects that further aggravate the mechanical obstruction of capillaries. This will cause a decrease in blood flow and incomplete perfusion of the coronary arteries, which
influeare the main causes of neutrophil conglutination in the vascular walls [134]. The bin
ding of leukoc
es myocardial reperfusioytes to endotheliocytes plays an important role in the inflammatory reaction, which is accompanied by cardiomyocyte apoptosis. Increased permeability of the plasmalemma leads to cytochrome C release that further aggravates myocardial apoptosis [135]. In
this context, Que has been shown to improv
ia multiple pathological mechanie inflammation and apoptosis in the myocardium. A recent I/R injury model was made through the ligation of the left coronary artery, after which Que was administered (2, 10 and 20 mg/kg orally) and diltiazem (15 mg/kg orally) for five days. This treatment caused the inhibition of the expression of TNF-α, IL-6 and IL-1β (important biomarkers of inflammatory reactions) in serum and cardiomyocytes. This indicates that Que treatment after I/R can alleviate inflammation and apoptosis. In agreement with these findings, Que diminishes the infarct size, as shown with 2,3,4-triphenyltetrazolium chloride (TTC) staining, as well as myocardial contractility, demonstrating that Que is capable of mitigating the inflammation and restoring myocardial function [131].
1.10.3. Vasodilatory Effects
It is
known that during a period of ischem
s. Numerous atteia, the coronary arteries are usually obstructed by emboli. Although blood flow can be quickly restored through interventional therapies, there are multiple findings that show that G-protein-coupled receptors are altered after I/R injury [136]. The adm
inistration of Que has been shown to imp
ts have rove vasoconstriction caused by ET-1, one of the types of endothelin, which is one of the most potent vasoconstrictors distributed in the endothelium of blood vessels (as well as in many other tissues and cells) [137].
1.10.4. Associations between Quercetin and Other Antioxidants
Although Que acts b
y re
en performed to reduce myocardial tissue damagducing oxidative stress, there are many mechanisms enhancing I/R damage that are still functioning. Therefore, it is proposed to associate Que with other antioxidants to produce synergy and further reduction of oxidative damage. There are multiple possible associations between Que and other antioxidants that could enhance the cardioprotective effect. One of the associations that have been studied is the combination between Que and α-tocopherol, which was studied in rats that were induced AMI by isoproterenol and were previously administered a combination of Que (10 mg/Kg) and α-tocopherol (10 mg/Kg) for 14 days. The combined pretreatment normalized all biochemical parameters and minimized ECG alterations. Therefore, Que and α-tocopherol exhibited enhanced cardioprotective effects against isoproterenol-induced cardiotoxicity because they eliminate free radicals, improve antioxidation, and maintain Ca2+ levels. Furthermore, the study showed that the combined pretreatme
nt aftewas more effective than the sole one [138]. Ther
e ischemia-reperfusion (I/R) by enhancare other molecules with which the association with Que has been studied to demonstrate its cardio-supporting effect, such as lycopene, another natural phytocompound with antioxidant effects. In an animal model study in which cardiac toxicity was induced by isoproterenol (ISO), free radicals and oxidative stress increased in myocardial tissue. The combination of Que with lycopene prevented all the side effects of cardiotoxicity, significantly decreasing the
antioxidant defensmyocardial damage, reducing oxidative stress, and slowing the levels of expression of antioxidant genes, a participant in pathways related to the Nrf2, HO-1, NQO1, GSTµ, SOD, SOD2, CAT and BCL-2 genes [139]. Evide
nce systemof the association of quercetin with
antclinical drugs was not found.
2. Discussion
Oxi
dative stress co
nstitutes an essential mechanism of damage involved in I/R injury in acute myocardial infarction. Even if multiple individual antioxidant
treatments. Accordingly, the administrs have been tested to prevent or minimize this damage, an effective treatment is not available. This problem might be related to the fact that oxidative stress results from different pathways that lead to an imbalance between ROS generation and antioxidant activity. Some of these mechanisms are mitochondrial dysfunction, activation of the inflammatory response, decreased antioxidant activity and activation of
molecules such as vitamin C, vitamin E, pro-oxidant enzymes, such as xanthine oxidase, uncoupled eNOS, NOX, and others. The comprehension of oxidative stress mechanisms makes us realize that the treatment alternatives based on monotherapy are not the appropriate solution, a view that has not been changed for more than a decade. It is of interest that several isolated beneficial effects could be joined to improve the cardioprotective effects occurring in I/R settings, such as percutaneous coronary intervention following AMI. Thus, some antioxidants are iron chelators (deferoxamine), some are ROS scavengers (N-acetylcysteine
, deferox), some activate the Nrf2 antioxidant response pathway (naringenin, melatonin, sulforaphane), and others exert influence on alternative edges of ROS production, resulting in effects that could be synergic and beneficial (Table 1). In the case of resveratrol and quercetin, these molecules have several ca
rdioprotective effects m
ine and polyaking them suitable to be included as part of a multitarget therapy.
It is imp
ortant to note th
enols, among othersat resveratrol and quercetin molecular sites of action are still not fully elucidated, but there are many proven targets. In the case of resveratrol, activation of Nrf2 and SIRT1 occurs through increased antioxidant proteins expression and PGC-1α deacetylation [140]. In addition,
resveratrol also activates th
as e PI3K/AKT pathway during I/R injury, resulting in decreased mitochondrial pathway-mediated apoptosis [97]. As mentioned, resveratrol is also capab
le
en s of reducing ferroptosis by decreasing Fe2+ concent
ration, which cou
dild be involved
2. Mechanisms of Ischemia/Reperfusion damage
During myocardial ischemia there is an overload in intracellular Ca2+ that cannot be captured by the Ca2+ ATPase (SERCA) in the sarcoplasmic reticulum due to the lack of ATP. The overload of Ca2+ induces enzymatic changes. One of them is the conversion of xanthine dehydrogenase in endothelial cells to xanthine oxidase (XO), an enzyme that generates superoxide anion radicals [5]. Another example is the oxidation of tetrahydrobiopterin and the subsequent uncoupling of endothelial nitric oxide synthase (eNOS), resulting in superoxide production instead of nitric oxide [6]. These changes are related to a burst in ROS production during reperfusion, overwhelming the antioxidant defenses.
There are multiple mechanisms involved in cellular damage and subsequent cellular death during the ischemia/reperfusion (I/R) process. Some of them involves endoplasmic reticulum stress, mitochondrial dysfunction, and inflammation mediated damage. This myocardial cellular injury is mediated through necrosis, apoptosis and even ferroptosis.
Figure 1. Representation of mechanisms involved in Ischemia/Reperfusion damage.
3. Defense Mechanisms against Oxidative Stress
A in inducing changes in
t
ioxidahe regulation of gene expression, but the exact target remains to be fully elucidated.
On
t
systems regulate redox homeosthe other hand, quercetin exerts its protective effects mainly through the inhibition of ROS-producing enzymes, such as NADPH oxidase and xanthine oxidase. The exact mechanism whereby this is achieved has been only partially described. A recent study shows that NOX may be inhibited for the enhanced expression of the antioxidant enzyme heme oxygenase-1 (HO-1) by quercetin [141]. In the cas
e of xanthi
s by cone oxidase, quercetin acts as a reversible inhibitor of the enzyme action [142].
An
ot
rolling the intracellular ROS levels and their inher relevant aspect is that there are some concerns about the water solubility of these compounds, which could make us question whether the suitability can be successfully administered intravenously. To solve this problem, different strategies have been designed to increase their water solubility. In the case of resveratrol, showing cardioprotective efficacy at low concentrations, it has been reported its administration with complexes with β-cyclodextrin and hydroxypropyl-β-cyclodextrin [143], complexes t
hat could slow down re
ractsveratrol metabolism and increase bioavailability [144]. Furthermore, solubi
lization
with biological of resveratrol could be increased with micellar solutions of bile acids, an effect attributed to the smallest membranolytic potential achieved through the formation of bile acids derivatives with resveratrol [145]. On the other hand, m
ultiple studies aim to increase Que sol
ecules. This sysubility by various mechanisms and thus increase its application properties. One of them is the nanoformulation method, which improves solubility, bioavailability, and circulation time, among other effects [146]. In t
urn, Que
m ha solubility and its thermal degradation in ethanol expanded with CO2 and ethyl lactate were s
tudied [147]. On the
other han
zymatic and non-d, co-crystallization has recently gained attention as a means of improving the physicochemical characteristics of a compound, and each of these cocrystals exhibited pharmacokinetic properties that are far superior to those of Que alone [148]. Finally, all these solutions sustain the research that has been done about these two antioxidants and their potential cardioprotective effects. The improvemen
zt of solubility
matic me with different agents makes it possible to continue considering resveratrol as a suitable potential part of therapy against I/R injury. The evidence leads us to think that if the solubility of Que is increased, its therapeutic effects could be promisingly improved.
3. Concluding Remarks
Isch
emia
nism/reperfusion injury occurring in AMI patients undergoing PCI is a complex process involv
ed. Antiing pathophysiological cascades leading to cellular disturbances ranging from metabolic changes to cell death. Although oxidative stress is involved in several of these injury mechanisms, antioxidan
ts, which can be endogenous or exogeneous, act by various mechanisms, such as ROS scavenging, inhibition of ROS production, metal ion ct therapeutic interventions so far have not been successful in protecting myocardial tissue against the harmful effects. Likely, the use of the most frequent monotherapies in a multifactorial process could explain the lack of consistency between the experimental studies and the clinical data. The paradigm of a multitarget therapy based on an association of different antioxidant molecules should be expected to improve the abrogation of oxidative damage and related effects derived from ROS burst, particularly occurring early at the onset of reperfusion. Thus, the administration of several antioxidant molecules could give rise to an additive or synergistic pharmacological effect. Some compounds, such as N-acetylcysteine, ascorbate and deferoxamine, have been tested as monotherapies in other clinical settings associated with increased ROS, showing lightly protective effects, as well as those caused by other naturally occurring antioxidant molecules. Among the latter, cardioprotective properties have been found in the case of resveratrol and Que, among others, having efficacy at low concentrations suitable to avoid adverse events. Therefore, these compounds could also be considered in this association, but following a better characterization of their pharmacokinetic properties, solubility at the required doses and studies about the appropriate design of formulations. Studies about associations of these compounds with others that have previously shown cardioprotective effects could be analyzed in isolated heart rat Langendorff model and, subsequently, in clinical trials aimed to reduce the infarct size due to the increased efficacy of this therapeutic association. This could lead to a better prognosis and quality of life after an acute myocardial infarction, decreasing complications, such as heart failure and arrhythmias, and also reducing the associated costs.
Th
e e
lation, enhancing of endogenous antiovidence supports that resveratrol is safe to be used in low doses. It has strong antioxidant effects, in which Nrf2 and SIRT1 activation are involved, thereby increasing the antioxidant response and decreasing inflammation and ferroptosis. Taken together, these effects could be beneficial as part of a multitarget therapy. Nevertheless, further studies are still lacking to implement a therapeutic scheme that includes resveratrol involving association with other antioxidant
generation, reparation os, specifically with vitamin C, which inactivates the NOX, reducing ROS production, and the iron chelator deferoxamine, reducing ferroptosis and cell death. We propose resveratrol might show a synergic effect with these antioxidants due to a theoretical potentiation of oxidative
damage istress reduction. Quercetin has multiple beneficial effects, particularly through its antioxidant activity could account for an enhanced cardioprotective effect.
To date, the association
of
licted on the macromole resveratrol and other antioxidants has not been studied, as well as there is no evidence of the combination of resveratrol or quercetin with clinical drugs. This is a topic that could be interesting to investigate, considering the beneficial and antioxidant properties of some drugs, such as melatonin, rosuvastatin and N-acetylcysteine, that are exposed in Table 2. In this c
ase, being synthetic antioxidants, it woul
es and red be important to consider what happens with the side effects of the drug in use.
Even if treatment for I/R injury has not been found
yet, resveratrol and qu
ction of apoptotic cell deathercetin constitute attractive natural pharmacological agents to be used in a combined therapy aimed to reduce cardiac tissue damage and infarct size due to their cardioprotective effects. Randomized double-blind clinical trials should be made to test the [7]therapeutic efficacy as well as safety of these associations.
4. Resveratrol
Resveratrol is a natural polyphenol with multiple biological activities [8]. Different one have evidenced that it has various properties, including anti-inflammatory, antioxidant, anti-diabetic, antihypertensive, anti-cancerous and cardioprotective effects [8][9]. Some of the pathways involved in its cardioprotective protective effects will be reviewed.
SIRT1 regulates oxidative stress-related proteins and other proteins that affect the function of cardiomyocytes. Resveratrol was proposed as a SIRT1 activator, resulting in a cardioprotective response via reduction of Ca2+ overload [10]. Accordingly, recent studies on mice demonstrates that resveratrol determines the increase of SIRT1 levels during I/R injury, resulting in a decrease in the incidence of atrioventricular block and letality, and a decrease of UCP-2 expression, an apoptosis mediator [8][11].
4.2. Ferroptosis Inhibition
The addition of Resveratrol in cell cultures reduced oxidative stress and the content of Fe2+. The effect was explained by changes in the regulation of gene expression, in which resveratrol down-regulated transferrin receptor 1 expression and up-regulated the expression of ferritin heavy chain 1 and GPX4, leading to inhibition of ferroptosis and potentiation of the antioxidant defenses, respectively [12].
4.3. Attenuation of Inflammation and Apoptosis
Different studies have suggested that resveratrol might inhibit apoptosis through multiple ways. One of them is the activation of PI3K/AKT signaling pathway, which down-regulates the expression of apoptotic genes and regulates cell proliferation [13][14], leading to decreased ROS levels, increased catalase and glutathione peroxidase activities, and increased cell viability [15]. Also, resveratrol could reduce caspase 3 expression [16]. Moreover, resveratrol attenuates necroptosis after I/R injury by inhibition of TNF-α/RIP1/RIP3/MLKL signaling pathway [17]. Effects evidenced in a dose-dependent manner. Furthermore, resveratrol treatment resulted in a significant reduction of inflammatory mediators in serum and cardiac tissue cells [18].
4.4. Nrf2 Activation
The beneficial effects of resveratrol in I/R injury could also be mediated via up-regulation of Keap1/Nrf2 signaling pathway. Nrf2 up-regulates the expression of proteins involved in the antioxidant response. This is suggested due to the reversion of the beneficial effects of resveratrol when a knock down or inhibition of Nrf2 is ensued [19].
4.5. Reduced Mitochondrial Dysfunction
A recent study suggested that resveratrol via activation of PI3K/AKT signaling pathway, reduced mitochondrial oxidative stress damage, increasing catalase, and glutathione peroxidase activity, and cell viability [15].
4.6. Associations between Resveratrol and Other Antioxidants
Resveratrol interferes with many of the mechanisms underlying myocardial I/R injury, but there are others that are not covered by it. In this context, it is reasonable to propose an association of resveratrol with other antioxidant compounds that have their effects on other targets. As an example, vitamin C down-regulates NOX activity and prevent eNOS uncoupling, which could synergize with the increased expression of antioxidant enzymes induced by resveratrol via Nrf2 signaling pathway activation.[7].
5. Quercetin
Quercetin is a flavonoid with anti-aggregating, anti-cancer, anti-inflammatory, anti-aging, and antioxidant properties. It is not toxic even in high doses, and recent studies have shown it to have tremendous potential to reduce myocardial damage that occurs after I/R. Although Que has a low bioavailability, many efforts are being made to increase its solubility [20][21].
5.1. Properties of Quercetin against Oxidative Stress
Quercetin treatment has demonstrated to reduce oxidative stress through several mechanism. It reduces xanthine oxidase expression and activity [22] [23], and attenuate the expression of NOX2, which is one of the more active isoforms of NOX during I/R injury. Also, quercetin can significantly inhibit Fenton reaction, another relevant source of ROS [24]. Moreover, quercetin administration increased the selenoprotein TrxR2, which acts as an antioxidant and an indirect redox activity modulator [25] [26].
5.2. Anti-Inflammatory and Anti-Apoptotic Effects
Acute inflammatory reactions are intensified in cardiomyocytes following I/R injury. This is due to the neutrophilic granulocytes, which are the ones that explain most of the reduced exudation and even the diffusion of these neutrophils through the blood vessels. Inflammation alter the function of endotheliocytes, reduce the relaxation capacities of coronary arteries, and promote coagulation [27]. Quercetin has been shown to improve inflammation and apoptosis of the myocardial tissue, resulting in a decrease of the final infarct size [28].
5.3. Associations between Quercetin and Other Antioxidants
Not many associations have been tested, one of them is quercetin and α-tocopherol in rats. The combined pretreatment normalized all biochemical parameters and minimized ECG alterations, exhibiting enhanced cardioprotective effects against isoproterenol-induced cardiotoxicity. Furthermore, the combined pretreatment was more effective than each of them separately [29]. The combination of quercetin and lycopene in an animal model also prevented myocardial damage induced by isoproterenol, reducing oxidative stress [30].
6. Concluding Remarks
Ischemia/reperfusion injury occurring in AMI patients undergoing PCI is a complex process involving pathophysiological cascades leading to cellular disturbances ranging from metabolic changes to cell death. The administration of several antioxidant molecules could give rise to an additive or synergistic pharmacological effect, leading to an improvement of previous studies on antioxidants that use them on monotherapy. tudies about associations of these compounds with others that have previously shown cardioprotective effects could be analyzed in isolated heart rat Langendorff model and, subsequently, in clinical trials aimed to reduce the infarct size due to the increased efficacy of this therapeutic association. This could lead to a better prognosis and quality of life after an acute myocardial infarction, decreasing complications, such as heart failure and arrhythmias, and reducing the associated costs.
Even if effective clinical treatment for I/R injury has not been found yet, resveratrol and quercetin constitute attractive natural pharmacological agents to be used in a combined therapy aimed to reduce cardiac tissue damage and infarct size due to their cardioprotective effects. Randomized double-blind clinical trials should be made to test the therapeutic efficacy as well as safety of these associations.