Ischemia-reperfusion myocardial damage is a paradoxical tissue injury occurring during percutaneous coronary intervention (PCI) in acute myocardial infarction (AMI) patients. Although this damage could account for up to 50% of the final infarct size, there has been no available pharmacological treatment until now. Oxidative stress contributes to the underlying production mechanism, exerting the most marked injury during the early onset of reperfusion. So far, antioxidants have been shown to protect the AMI patients undergoing PCI to mitigate these detrimental effects; however, no clinical trials to date have shown any significant infarct size reduction. Myocardial ischemia/reperfusion damage results from diverse oxidative stress producing mechanisms. Therefore, it is worthwhile to consider multitarget antioxidant therapies targeting multifactorial AMI. Indeed, this clinical setting involves injurious effects derived from oxygen deprivation, intracellular pH changes and increased concentration of cytosolic Ca2+ and reactive oxygen species, among others. Thus, we will review a brief overview of the We will review some of this pathological cascades involved in ischemia-reperfusion injury pathways and the potential therapeutic effects based on preclinical studies involving a combination ofof some available antioxidants, with particular reference to resveratrol and quercetin, which could contribute to cardioprotection against ischemia-reperfusion injury in myocardial tissue. We will also highlight the upcoming perspectives of these antioxidants for designing future studiesn.
- oxidative stress
- reperfusion injury
- antioxidants
- resveratrol
- quercetin
- cardioprotection
1. Introduction
2. Oxidative Stress
2.1. Oxidative Stress and ROS
2.2. Mechanisms of Ischemia/Reperfusion Cellular Damage
2.3. ROS Production in Ischemia/Reperfusion
3. Intracellular Organelle Dysfunctions Associated with Ischemia/Reperfusion Injury
3.1. Endoplasmic Reticulum Stress (ERS)
3.2. Mitochondrial Dysfunction
3.3. Inflammation Mediated Damage
4. Mechanisms of Cell Death in Ischemia-Reperfusion
Ferroptosis
5. Apoptosis
62. Defense Mechanisms against Oxidativof Ischemia/Reperfusion damage Stress
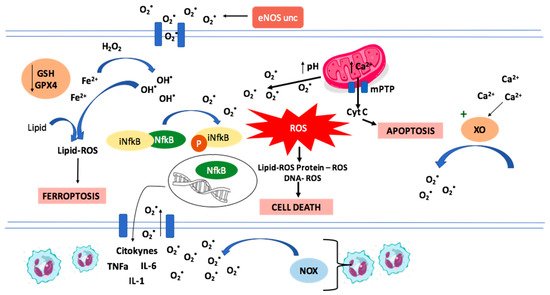
During myocardial ischemia there is an overload in intracellular Ca2+ that cannot be captured by the Ca2+ ATPase (SERCA) in the sarcoplasmic reticulum due to the lack of ATP. The overload of Ca2+ induces enzymatic changes. One of them is the conversion of xanthine dehydrogenase in endothelial cells to xanthine oxidase (XO), an enzyme that generates superoxide anion radicals [18]. Another example is the oxidation of tetrahydrobiopterin and the subsequent uncoupling of endothelial nitric oxide synthase (eNOS), resulting in superoxide production instead of nitric oxide [19]. These changes are related to a burst in ROS production during reperfusion, overwhelming the antioxidant defenses.
There are multiple mechanisms involved in cellular damage and subsequent cellular death during the ischemia/reperfusion (I/R) process. Some of them involves endoplasmic reticulum stress, mitochondrial dysfunction, and inflammation mediated damage. This myocardial cellular injury is mediated through necrosis, apoptosis and even ferroptosis.
7. Nrf2 Signalling Pathway
8. Exogenous Antioxidants with Reported Cardioprotective Effects
94. Resveratrol
Resveratrol is a natural polyphenol with multiple biological activities [
90]. It has a molecular weight of 228.25 g/mol [8] and exists in two isomeric forms (cis and trans), with the trans form being the most common with more therapeutic benefits [91]. This antioxidant is found in many fruits and vegetables, such as grapes, Polygonum cuspidatum and mulberry [92].]. Different studies have evidenced that it has various properties, including anti-inflammatory, antioxidant, anti-diabetic, antihypertensive, anti-cancerous and cardioprotective effects [
90,
92].]. Some of the pathways involved in its cardioprotective protective effects will be reviewed in the next sections
10. Resveratrol Cardioprotective Mechanisms
104.1. SIRT1 Activation
Silent information regulator factor 2-related enzyme 1 (SIRT1) consists of a nicotinamide adenine dinucleotide-dependent deacetylase that regulates oxidative stress-related proteins and other proteins that affect the function of cardiomyocytes. It was proposed that resveratrol activates SIRT1 leading to the activation of a cardioprotective response, reducing the Ca2+ overload in the cytosol and mitochondria [
SIRT1 regulates oxidative stress-related proteins and other proteins that affect the function of cardiomyocytes. Resveratrol was proposed as a SIRT1 activator, resulting in a cardioprotective response via reduction of Ca2+ overload [
95]. According to this theory, a recent study showed that in a rat model of cardiac I/R, 21-day oral treatment with resveratrol decreased the incidence of atrioventricular block and lethality, thus suggesting the usefulness of this natural compound in the prevention of lethal cardiac arrhythmias after reperfusion [
]. Accordingly, recent studies on mice demonstrates that resveratrol determines the increase of SIRT1 levels during I/R injury, resulting in a decrease in the incidence of atrioventricular block and letality, and a decrease of UCP-2 expression, an apoptosis mediator [
90]. Furthermore, it has been demonstrated that intraperitoneal injection of resveratrol in mice determines the increase of SIRT1 levels and a concomitant decrease of UCP-2 expression, thus protecting myocardial tissue against I/R injury in vivo [
,
].
104.2. Ferroptosis Inhibition
The addition of Resveratrol in cell cultures reduced oxidative stress and the content of Fe2+. The effect was explained by changes in the regulation of gene expression, in which resveratrol down-regulated transferrin receptor 1 expression and up-regulated the expression of ferritin heavy chain 1 and GPX4, leading to inhibition of ferroptosis and potentiation of the antioxidant defenses, respectively [
89], in vitro experiments with H9c2 cells and a model of oxygen-glucose deprivation/reoxygenation (OGD/R) demonstrated that OGD/R-induced H9c2 cells showed increased cell death by ferroptosis. The addition of resveratrol in cell cultures reduced oxidative stress and the content of Fe2+. In vivo experiments performed by the same authors in rats ligated and perfused by the left anterior descending branch showed that when resveratrol was administered at the concentration of 50 mg/kg for 14 days, oxidative stress and the content of Fe2+ decreased again. The effect was explained by changes in the regulation of gene expression, in which resveratrol down-regulated transferrin receptor 1 expression and up-regulated the expression of ferritin heavy chain 1 and GPX4, leading to inhibition of ferroptosis and potentiation of the antioxidant defenses, respectively. The consequent reduction in oxidative stress is evidenced by a reduction in malondialdehyde (MDA) production [89].].
104.3. Attenuation of Inflammation and Apoptosis
Different studies have suggested that resveratrol might inhibit apoptosis through multiple ways. One of them is the activation of PI3K/AKT signaling pathway, which down-regulates the expression of apoptotic genes and regulates cell proliferation [
98,
99]. Apparently, PI3K/AKT signaling pathway is inhibited during the I/R process, resulting in potent activation of apoptosis and less viable tissue [], leading to decreased ROS levels, increased catalase and glutathione peroxidase activities, and increased cell viability [
97,100]. Moreover, it has been suggested that resveratrol attenuates apoptosis by reducing caspase 3 expression []. Also, resveratrol could reduce caspase 3 expression [
101]. In another study, Hu et al. []. Moreover, resveratrol attenuates necroptosis after I/R injury by inhibition of TNF-α/RIP1/RIP3/MLKL signaling pathway [
102] indicated that resveratrol attenuates necroptosis after ischemia-reperfusion by inhibition of the tumor necrosis factor-alpha (TNF-α)/receptor-interacting protein kinase 1 (RIP1)/RIP3/mixed-lineage kinase domain-like (MLKL) signaling pathway. The results were that after treatment with different resveratrol concentrations, the expressions of TNF-α, RIP1, RIP3, and p-MLKL/MLKL decreased, as well as necroptosis. Under those circumstances, cell viability increased. All these effects were seen in dose-dependent manners [102]. Xing et al. []. Effects evidenced in a dose-dependent manner. Furthermore, resveratrol treatment resulted in a significant reduction of inflammatory mediators in serum and cardiac tissue cells [
103] measured the levels of serum interleukin-1β (IL-1β), IL-6, and TNF-a in rat myocardial tissue during I/R injury. They also measured the expressions of mRNA and proteins of Toll-like receptor 4 (TLR4), NF-κB, p65, IL-1β, IL-6, and TNF-α. Resveratrol treatment resulted in a significant reduction of serum IL-1β, TNF-α, and IL-6, TLR4, NF-κB, p65, IL-1β, IL-6, and TNF-α mRNA and protein expressions in cardiac tissue cells [103].].
104.4. Nrf2 Activation
The beneficial effects of resveratrol in I/R injury could also be mediated via up-regulation of Keap1/Nrf2 signaling pathway. Nrf2 up-regulates the expression of proteins involved in the antioxidant response. This is suggested due to the reversion of the beneficial effects of resveratrol when a knock down or inhibition of Nrf2 is ensued [
104]. Furthermore, in a rat model of lower-extremity I/R, treatment with resveratrol improved the apoptotic state of the femoral artery and reduced oxidative stress; this effect was abolished by the co-administration of an inhibitor of Nrf2 [104]. These results indicate that resveratrol might attenuate the I/R injury damage through up-regulating Keap1/Nrf2 signaling, mainly for its effects on oxidative stress. This could increase cell viability and decrease the apoptotic rate [104].].
104.5. Reduced Mitochondrial Dysfunction
A recent study suggested that resveratrol via activation of PI3K/AKT signaling pathway, reduced mitochondrial oxidative stress damage, increasing catalase, and glutathione peroxidase activity, and cell viability [
97]. Moreover, resveratrol significantly increases the activity of mitochondrial superoxide dismutase and reduces the levels of malondialdehyde, indicating reduced oxidative damage to the mitochondria. The effects observed after resveratrol addition were reversed using PI3K siRNA, thus suggesting that the protective effect of resveratrol on cardiomyocytes under I/R conditions can be due to PI3K/AKT signaling pathway activation [97].].
104.6. Other Pathways
10.7. Considerations of Safety in the Use of Resveratrol
10.8. Associations between Resveratrol and Other Antioxidants
Resveratrol interferes with many of the mechanisms underlying myocardial I/R injury, but there are others that are not covered by it. In this context, it is reasonable to propose an association of resveratrol with other antioxidant compounds that have their effects on other targets. As an example, vitamin C down-regulates NOX activity and prevent eNOS uncoupling, which could synergize with the increased expression of antioxidant enzymes induced by resveratrol via Nrf2 signaling pathway activation.[
50]. Further, it reduces intracellular Ca2+ overload and prevents the depolarization of the mitochondrial membrane [67]. These two last effects are related to SIRT1 activation by resveratrol, while it has been seen in studies showing that vitamin C also increases the expression of SIRT1 [109]. Even if this could constitute a potential interference between both antioxidants, it is necessary to look further into the molecular mechanisms involved to determine whether it would potentiate or antagonize the effect of resveratrol. It is worth mentioning that vitamin C is a water-soluble vitamin and can be administered intravenously [110].].
115. Quercetin
Quercetin is a flavonoid with anti-aggregating, anti-cancer, anti-inflammatory, anti-aging, and antioxidant properties. It is not toxic even in high doses, and recent studies have shown it to have tremendous potential to reduce myocardial damage that occurs after I/R. Although Que has a low bioavailability, many efforts are being made to increase its solubility [
115]. It also has several other biological effects in addition to its antioxidant properties. It has anti-aggregating, anti-inflammatory, anti-cancer, and anti-aging effects. Furthermore, it is not toxic even in high doses (4000 mg/day) [,
116]. Additionally, recent studies have shown it to have tremendous potential to reduce myocardial damage that occurs after I/R through various mechanisms.].
15.10.1.. Properties of Quercetin against Oxidative Stress
Recent experiments with an animal model of hyperuricemia have demonstrated a reduction in xanthine oxidase expression and enzyme activity by Que treatment (100, 200, 400 mg/Kg) [Quercetin treatment has demonstrated to reduce oxidative stress through several mechanism. It reduces xanthine oxidase expression and activity [
9]. Xanthine oxidase is a molybdo-flavoenzyme found in various species. It is a homodimer with two symmetrical monomers. It has a great affinity for producing ROS because, in each of the monomers, there is a C-terminal molybdo protein that contains four redox centers. In turn, it has an N-terminal domain with two iron–sulfur centers and a central flavin adenine dinucleotide cofactor [118]. Thus, xanthine oxidase stimulates ROS production, which can end up causing oxidative stress injuries [119]. Similarly, Que can attenuate the expression of NOX2 [,
120]. The NADPH oxidase system is a multiprotein complex that produces ROS in different cells and tissues, being of great importance in phagocytic cells [121]. The NADPH oxidase enzyme is composed of several subunits, including the gp91-phox subunit and its counterparts which are commonly known as the NOX family (NOX1, NOX2, NOX3, NOX4, NOX5, DUOX1, and DUOX2) [122] that are found in almost all cells of the organism [123]. In the cardiovascular system, this complex is the main ROS producer, which is achieved through the transfer of an electron from NADPH to O2, resulting in NADP and O2●−. The newly produced O2●− will end up rapidly transforming into H2O2, characterized by being more stable and diffusible [124]. This leads us to think that if we initially inhibit the expression of the enzyme, we will reduce the production of H2O2 and, consequently, decrease the I/R damage produced by ROS in the myocardial tissue. In cardiomyocytes, NADPH oxidase can be activated by various mechanisms and stimulating factors [125]. Among them, one of the stimulants for the enzyme corresponds to I/R, with NOX2 and NOX4 being the ones more activated during myocardial I/R injury [82]. Therefore, the inhibitory effect of Que on NOX can potentially be a great target to ameliorate the injury induced by I/R. In addition, Que combined with Fe2+/Cu+ will significantly inhibit Fenton reaction, another ROS source producing ●OH [], and attenuate the expression of NOX2, which is one of the more active isoforms of NOX during I/R injury. Also, quercetin can significantly inhibit Fenton reaction, another relevant source of ROS [
126]. Fenton reaction consists of the electron transfer from Fe2+/Cu+ metallic ion to H2O2, which produces Fe3+/Cu2+, OH− and ●OH. It has been shown that ●OH has a very strong oxidability in acid solutions [127]. Then also, H2O2 can restore Fe2+/Cu+ from Fe3+/Cu2+, which produces HOO● and H+. Fe2+/Cu+ can be oxidized by O2 again, which forms O2●−. In I/R damage, an acidic environment is created due to anaerobic glycolysis, which then facilitates the production of the Fenton reaction. Selenium is an antioxidant and a component of selenoproteins, including glutathione peroxidases (GPX), thioredoxin reductases (TrxR) and methionine sulfoxide reductase 2, thereby modulating redox activity []. Moreover, quercetin administration increased the selenoprotein TrxR2, which acts as an antioxidant and an indirect redox activity modulator [82,
128]. Accordingly, it has been observed that after Que administration at a dose of 50 mg/kg for eight weeks, the selenoprotein TrxR2 increased in the Que group compared to the control [82].].
Quercetin is recognized as a significant antioxidant, preventing damage to cardiomyocytes as measured by oxidative stress, avoiding ROS increase and progression of damage after I/R. Moreover, ROS removal may increase NO bioavailability and restoration of endothelial function after I/R damage [129]. The mechanisms whereby Que exerts its antioxidant activity consist of eliminating ROS through its ability to react with the free radicals O2●−, HO●, NO, alkoxy and peroxyl. It also occurs when the hydroxyl attached to the benzene ring transfers a hydrogen atom or an electron to the free radical, resulting in the formation of more stable molecules [130]. Quercetin also acts through indirect mechanisms, restoring inherent antioxidant systems of the body, such as enzymatic systems dependent or not on antioxidants, such as vitamins C and E, and reduced glutathione (GSH) [59], the latter decreasing after I/R injury, which indicates the depletion of the antioxidant system. Thus, it can eliminate ROS and restore the function of the intrinsic antioxidant system [131].15.10.2. Anti-Inflammatory and Anti-Apoptotic Effects
Acute inflammatory reactions are intensified in cardiomyocytes following I/R injury. This is due to the neutrophilic granulocytes, which are the ones that explain most of the reduced exudation and even the diffusion of these neutrophils through the blood vessels. Thus, it can be generated more damage to the injured tissue [132]. In the I/R period, leukocytes can alter the function of endotheliocytes and reduce the relaxation capacity of the coronary arteries [Acute inflammatory reactions are intensified in cardiomyocytes following I/R injury. This is due to the neutrophilic granulocytes, which are the ones that explain most of the reduced exudation and even the diffusion of these neutrophils through the blood vessels. Inflammation alter the function of endotheliocytes, reduce the relaxation capacities of coronary arteries, and promote coagulation [
133]. They also promote coagulation and pro-inflammatory effects that further aggravate the mechanical obstruction of capillaries. This will cause a decrease in blood flow and incomplete perfusion of the coronary arteries, which are the main causes of neutrophil conglutination in the vascular walls [134]. The binding of leukocytes to endotheliocytes plays an important role in the inflammatory reaction, which is accompanied by cardiomyocyte apoptosis. Increased permeability of the plasmalemma leads to cytochrome C release that further aggravates myocardial apoptosis [135]. In this context, Que has been shown to improve inflammation and apoptosis in the myocardium. A recent I/R injury model was made through the ligation of the left coronary artery, after which Que was administered (2, 10 and 20 mg/kg orally) and diltiazem (15 mg/kg orally) for five days. This treatment caused the inhibition of the expression of TNF-α, IL-6 and IL-1β (important biomarkers of inflammatory reactions) in serum and cardiomyocytes. This indicates that Que treatment after I/R can alleviate inflammation and apoptosis. In agreement with these findings, Que diminishes the infarct size, as shown with 2,3,4-triphenyltetrazolium chloride (TTC) staining, as well as myocardial contractility, demonstrating that Que is capable of mitigating the inflammation and restoring myocardial function []. Quercetin has been shown to improve inflammation and apoptosis of the myocardial tissue, resulting in a decrease of the final infarct size [
131].].
15.10.3. Vasodilatory Effects
It is known that during a period of ischemia, the coronary arteries are usually obstructed by emboli. Although blood flow can be quickly restored through interventional therapies, there are multiple findings that show that G-protein-coupled receptors are altered after I/R injury [136]. The administration of Que has been shown to improve vasoconstriction caused by ET-1, one of the types of endothelin, which is one of the most potent vasoconstrictors distributed in the endothelium of blood vessels (as well as in many other tissues and cells) [137].1.10.4. 3. Associations between Quercetin and Other Antioxidants
Although Que acts by reducing oxidative stress, there are many mechanisms enhancing I/R damage that are still functioning. Therefore, it is proposed to associate Que with other antioxidants to produce synergy and further reduction of oxidative damage. There are multiple possible associations between Que and other antioxidants that could enhance the cardioprotective effect. One of the associations that have been studied is the combination between Que and α-tocopherol, which was studied in rats that were induced AMI by isoproterenol and were previously administered a combination of Que (10 mg/Kg) and α-tocopherol (10 mg/Kg) for 14 days. The combined pretreatment normalized all biochemical parameters and minimized ECG alterations. Therefore, Que and α-tocopherol exhibited enhanced cardioprotective effects against isoproterenol-induced cardiotoxicity because they eliminate free radicals, improve antioxidation, and maintain Ca2+ levels. Furthermore, the study showed that the combined pretreatment was more effective than the sole one [Not many associations have been tested, one of them is quercetin and α-tocopherol in rats. The combined pretreatment normalized all biochemical parameters and minimized ECG alterations, exhibiting enhanced cardioprotective effects against isoproterenol-induced cardiotoxicity. Furthermore, the combined pretreatment was more effective than each of them separately [
138]. There are other molecules with which the association with Que has been studied to demonstrate its cardio-supporting effect, such as lycopene, another natural phytocompound with antioxidant effects. In an animal model study in which cardiac toxicity was induced by isoproterenol (ISO), free radicals and oxidative stress increased in myocardial tissue. The combination of Que with lycopene prevented all the side effects of cardiotoxicity, significantly decreasing the myocardial damage, reducing oxidative stress, and slowing the levels of expression of antioxidant genes, a participant in pathways related to the Nrf2, HO-1, NQO1, GSTµ, SOD, SOD2, CAT and BCL-2 genes []. The combination of quercetin and lycopene in an animal model also prevented myocardial damage induced by isoproterenol, reducing oxidative stress [
139]. Evidence of the association of quercetin with clinical drugs was not found.].
26. Discussion
Oxidative stress constitutes an essential mechanism of damage involved in I/R injury in acute myocardial infarction. Even if multiple individual antioxidants have been tested to prevent or minimize this damage, an effective treatment is not available. This problem might be related to the fact that oxidative stress results from different pathways that lead to an imbalance between ROS generation and antioxidant activity. Some of these mechanisms are mitochondrial dysfunction, activation of the inflammatory response, decreased antioxidant activity and activation of pro-oxidant enzymes, such as xanthine oxidase, uncoupled eNOS, NOX, and others. The comprehension of oxidative stress mechanisms makes us realize that the treatment alternatives based on monotherapy are not the appropriate solution, a view that has not been changed for more than a decade. It is of interest that several isolated beneficial effects could be joined to improve the cardioprotective effects occurring in I/R settings, such as percutaneous coronary intervention following AMI. Thus, some antioxidants are iron chelators (deferoxamine), some are ROS scavengers (N-acetylcysteine), some activate the Nrf2 antioxidant response pathway (naringenin, melatonin, sulforaphane), and others exert influence on alternative edges of ROS production, resulting in effects that could be synergic and beneficial (Oxidative stress constitutes an essential mechanism of damage involved in I/R injury in acute myocardial infarction. Even if multiple individual antioxidants have been tested to prevent or minimize this damage, an effective treatment is not available. This problem might be related to the fact that oxidative stress results from different pathways that lead to an imbalance between ROS generation and antioxidant activity. The comprehension of oxidative stress mechanisms makes us realize that the treatment alternatives based on monotherapy are not the appropriate solution, a view that has not been changed for more than a decade. Thus, some antioxidants are iron chelators (deferoxamine), some are ROS scavengers (N-acetylcysteine), some activate the Nrf2 antioxidant response pathway (naringenin, melatonin, sulforaphane), and others exert influence on alternative edges of ROS production, resulting in effects that could be synergic and beneficial (
Table 1). In the case of resveratrol and quercetin, these molecules have several cardioprotective effects making them suitable to be included as part of a multitarget therapy.
It is important to note that resveratrol and quercetin molecular sites of action are still not fully elucidated, but there are many proven targets. In the case of resveratrol, activation of Nrf2 and SIRT1 occurs through increased antioxidant proteins expression and PGC-1α deacetylation [
140]. In addition, resveratrol also activates the PI3K/AKT pathway during I/R injury, resulting in decreased mitochondrial pathway-mediated apoptosis [
97]. As mentioned, resveratrol is also capable of reducing ferroptosis by decreasing Fe2+ concentration, which could be involved in inducing changes in the regulation of gene expression, but the exact target remains to be fully elucidated.].
On the other hand, quercetin exerts its protective effects mainly through the inhibition of ROS-producing enzymes, such as NADPH oxidase and xanthine oxidase. The exact mechanism whereby this is achieved has been only partially described. A recent study shows that NOX may be inhibited for the enhanced expression of the antioxidant enzyme heme oxygenase-1 (HO-1) by quercetin [
141]. In the case of xanthine oxidase, quercetin acts as a reversible inhibitor of the enzyme action [
142].
Another relevant aspect is that there are some concerns about the water solubility of these compounds, which could make us question whether the suitability can be successfully administered intravenously. To solve this problem, different strategies have been designed to increase their water solubility. In the case of resveratrol, showing cardioprotective efficacy at low concentrations, it has been reported its administration with complexes with β-cyclodextrin and hydroxypropyl-β-cyclodextrin [143], complexes that could slow down resveratrol metabolism and increase bioavailability [144]. Furthermore, solubilization of resveratrol could be increased with micellar solutions of bile acids, an effect attributed to the smallest membranolytic potential achieved through the formation of bile acids derivatives with resveratrol [145]. On the other hand, multiple studies aim to increase Que solubility by various mechanisms and thus increase its application properties. One of them is the nanoformulation method, which improves solubility, bioavailability, and circulation time, among other effects [146]. In turn, Que solubility and its thermal degradation in ethanol expanded with CO2 and ethyl lactate were studied [147]. On the other hand, co-crystallization has recently gained attention as a means of improving the physicochemical characteristics of a compound, and each of these cocrystals exhibited pharmacokinetic properties that are far superior to those of Que alone [148]. Finally, all these solutions sustain the research that has been done about these two antioxidants and their potential cardioprotective effects. The improvement of solubility with different agents makes it possible to continue considering resveratrol as a suitable potential part of therapy against I/R injury. The evidence leads us to think that if the solubility of Que is increased, its therapeutic effects could be promisingly improved.37. Concluding Remarks
Ischemia/reperfusion injury occurring in AMI patients undergoing PCI is a complex process involving pathophysiological cascades leading to cellular disturbances ranging from metabolic changes to cell death. The administration of several antioxidant molecules could give rise to an additive or synergistic pharmacological effect, leading to an improvement of previous studies on antioxidants that use them on monotherapy. tudies about associations of these compounds with others that have previously shown cardioprotective effects could be analyzed in isolated heart rat Langendorff model and, subsequently, in clinical trials aimed to reduce the infarct size due to the increased efficacy of this therapeutic association. This could lead to a better prognosis and quality of life after an acute myocardial infarction, decreasing complications, such as heart failure and arrhythmias, and reducing the associated costs.
Even if effective clinical treatment for I/R injury has not been found yet, resveratrol and quercetin constitute attractive natural pharmacological agents to be used in a combined therapy aimed to reduce cardiac tissue damage and infarct size due to their cardioprotective effects. Randomized double-blind clinical trials should be made to test the therapeutic efficacy as well as safety of these associations.