 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Thomas Dos'Santos | + 4983 word(s) | 4983 | 2021-04-22 08:17:22 | | | |
| 2 | Conner Chen | -18 word(s) | 4965 | 2021-05-05 08:01:14 | | | | |
| 3 | Conner Chen | -18 word(s) | 4965 | 2021-05-05 08:02:38 | | | | |
| 4 | Conner Chen | Meta information modification | 4965 | 2021-05-05 09:06:01 | | |
Video Upload Options
The Cutting Movement Assessment Score (CMAS) is a recently validated field-based qualitative screening tool to identify athletes that display high-risk postures associated with increased non-contact ACL injury risk during side-step cutting. Side-step cutting is an action associated with non-contact anterior cruciate ligament (ACL) injury with a plethora of negative economical, health, and psychological implications. Although ACL injury risk factors are multifactorial, biomechanical and neuromuscular deficits which contribute to “high-risk” and aberrant movement patterns are linked to ACL injury risk due to increasing knee joint loads and potential ACL loading. Importantly, biomechanical and neuromuscular deficits are modifiable; thus, being able to profile and classify athletes as potentially “high-risk” of injury is a crucial process in ACL injury mitigation.
1. An anterior cruciate ligament injury
An anterior cruciate ligament injury (ACL) is considered one of the most significant and debilitating injuries an athlete can experience, with an abundance of negative economic [1][2][3], psychological [1][4], and health [1][5] implications. ACL injury risk factors are multifactorial (anatomical, hormonal, biomechanical, neuromuscular, environmental) [1][6] and a complex interaction of both internal (within the body) and external (outside the body) factors [6][7][8]. In simplistic terms, ACL injuries occur when a catastrophic applied load exceeds the ligament’s tolerance [7][9], or due to a “fatigue failure” mechanism whereby the accumulation of high magnitudes and repetitive cycles of knee joint loading [10][11][12][13][14]. This process, without adequate rest and repair, can lead to micro damage and subsequent ACL failure [13] from mechanical loads which previously could be tolerated [14][15][16]. Mitigating ACL injury risk therefore is considered highly important in sports medicine and science environments.
Non-contact ACL injuries generally occur during high-impact tasks such as change of directions (COD) (side-step, cut or turn, plant-and-cut manoeuvres) [17][18][19][20][21][22][23][24][25][26], landing (predominantly single-leg weight bearing) [17][19][21][25][27], and deceleration actions [20][21][28]; attributable to the potential generation of high multiplanar knee joint loading (flexion, rotation, abduction and translatory moments) during foot contact [29][30][31][32][33], thus increasing ACL strain [34][35][36][37][38]. These multiplanar knee joint loads are often used as surrogates of non-contact ACL injury risk [29][32][39][40], and are amplified during COD, landings, and decelerations when aberrant and “high-risk” neuromuscular control and biomechanical deficits are displayed (e.g., lateral trunk flexion, knee valgus, etc.) [1][31][32][33][41][42][43]. Importantly, neuromuscular control and biomechanical deficits are modifiable through appropriate training and conditioning [31][32][33][41][42][44][45], which may reduce knee joint loading during high-impact actions and subsequent risk of non-contact ACL injury [1][43][44][45][46]. As such, the mechanism of ACL injury, from a knee joint loading perspective, has been stated as “multiplanar” [6]; highlighting the importance of reducing multiplanar joint loading during high-risk activities to mitigate ACL injury risk [9][47][48].
2. Qualitative Screening: Why Assess Cutting Movement Quality?
Due to the plethora of negative implications associated with non-contact ACL injury, being able to profile and classify athletes as potentially “high-risk” of injury is a crucial process in ACL injury mitigation [1][49]. Side-step cutting (lateral foot plant) is an important high-intensity action performed in numerous sports, and is a pivotal action performed to evade opponents, penetrate defensive lines and gain territorial advantage in sports such as rugby, American football, and handball [50][51][52][53][54]. However, because side-steps are frequently performed movements in sports [50][51][52][53], and performed at high-intensity, and thus have the potential to generate high impact forces and knee joint loads [31][33][55], they are also commonly observed manoeuvres during non-contact ACL injury events [17][18][19][20][21][22][23][24][25][26]. For example, 60–67% of non-contact ACL injuries in rugby [18], American football [26], and handball [19] occur during side-step cutting, while this manoeuvre is also linked with non-contact ACL injury events in soccer [17], badminton [25], and Australian rules football [21]. Consequently, screening tools and field-based interventions that can assist in ACL injury risk mitigation is of great interest, particularly for practitioners working in sports where cutting is the predominant mechanism of non-contact ACL injury.
The ability to predict non-contact ACL injury using screening tools is a contentious issue [56][57][58]; however, much attention has been placed on screening and profiling movement quality because of the adaptable nature of movement biomechanics, which in turn is a modifiable ACL risk factor [1][43][45][57][59]. Additionally, creating “injury-risk profiles” through the identification of “high-risk” biomechanical and neuromuscular control deficits is considered important in terms quantifying relative injury risk [59][60][61]. For example, “high-risk” postures include knee abduction angles (KAA–synonymous with knee valgus angles) [33][40][42][62][63], lateral trunk flexion [31][42][64][65][66], extended knee postures [24][67][68], and hip internal rotation [40][41][63][69] are related to greater multiplanar knee joint loads and subsequent ACL loading [46][70][71].
Figure 1 displays the screening process commonly adopted by practitioners, whereby athletes are typically screened/profiled during a movement to assess their movement quality, joint kinetics, or kinematics against pre-determined criteria or benchmarks. This can be done via three-dimensional (3D) motion and ground reaction force (GRF) analysis whereby joint kinetics and kinematics can be examined and surrogates of injury risk are measured, creating an “injury-risk profile”, and subsequently used to infer potential injury risk. For example, peak KAMs and peak KAAs can be measured during a COD or a drop landing to identify athletes who display values greater than normative data or a threshold to define “high-risk” [39][72][73]. Alternatively, qualitative screening of movement quality may take place using high-speed two-dimensional (2D) cameras, whereby movement is filmed (usually in the frontal and sagittal plane) and aberrant and “high-risk” movement patterns can be identified via visual observations (i.e., visible knee valgus/lateral trunk flexion). Qualitative assessments have been shown to reflect aspects of performance during 3D motion analysis, such as the Landing Error Scoring System (LESS) [74] and Qualitative Analysis of Single Leg Loading (QASLS) [75].
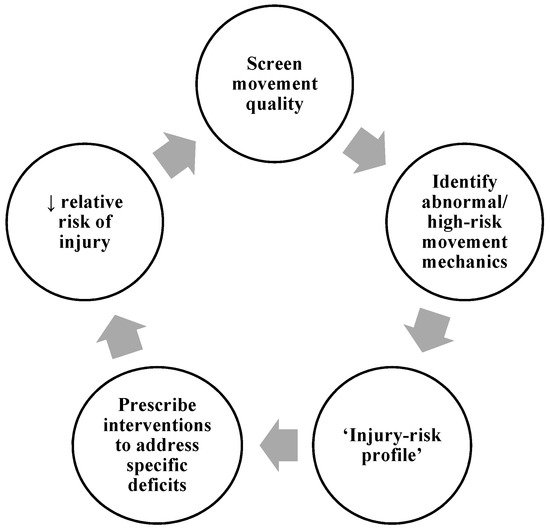
Figure 1. Screening movement quality process.
Irrespective of the screening method, athletes identified as potentially “higher-risk” of injury can therefore be prescribed individualised interventions to address the specific “high-risk” deficits [57][59]. This should theoretically reduce injury risk, and the training intervention’s success is monitored be re-evaluating and screening movement quality at the end of the intervention. Practitioners may continuously go through the process multiple times (normally at the end of mesocycles) during the macrocycle. Therefore, validated and reliable screening tools which assess movement quality are considered integral for practitioners working in strength and conditioning, sports medicine, and sports rehabilitation [59][76].
The optimal method for assessing movement kinetics and kinematics is 3D and GRF analysis [1][57], whereby this approach is used to identify “high-risk” athletes that display poor movement quality (i.e., knee valgus) and high multiplanar knee joint moments (surrogates of non-contact ACL injury risk) [59]. Although insightful and can indeed provide detailed insight into athletes’ movement strategies and surrogates of injury risk, 3D motion and GRF analysis does have its limitations including, cost, complexity, the time required to perform mass screening, and the required laboratory facilities [1][57][72][77][78][79]; thus, restricting its use for practitioners in field-based environments. As such, qualitative screening tools such as the LESS [74][80], Tuck Jump Assessment (TJA) [81][82][83], and QASLS [84][85] have been developed, offering practitioners an easier and cost-effective method to evaluate aberrant movement quality and postures associated with greater ACL injury risk, typically during landing tasks. Although screening landing mechanics during vertical orientated tasks is indeed applicable for jump-landing sports where the landing is the predominant action associated with non-contact ACL injury [27][28][86][87], changing direction is a unilateral and multiplanar movement which is biomechanically distinctly different to landing, thus screening landing lacks specificity to directional changes [57][60][76]. This is pertinent for practitioners who seek to profile athletes who participate in sports (handball, American football, rugby, and soccer) where the side-step cutting is a predominant mechanism of non-contact ACL injury [17][18][19][20][21][22][23][24][25][26]. Furthermore, mixed findings have been observed between “high-risk” postures and knee joint loads between landing and cutting tasks [72][88][89][90], with researchers demonstrating that “injury-risk profiles” are task dependent [72][91][92]. Therefore, it would be more suitable to assess movement mechanics associated with the primary action of injury in that sport [49][57][60]. As such, there is a requirement for a specific field-based qualitative screening tool to evaluate and identify poor movement quality and “high-risk” mechanics specifically for cutting.
3. Introducing the Cutting Movement Assessment Score (CMAS)
The CMAS, initially developed and validated in 2017 [76], is a 9-item qualitative screening tool (Table 1) that assesses hip, knee, foot, and trunk postures during side-step cutting relating to the technical determinants of peak KAMs [30][31][33][40][41][42][63][64][65][68][69][93] (Figure 2) and non-contact ACL injury visual observations [19][24][26]. A detailed rationale and operational definitions for these items are presented in a later section, but briefly these items relate to penultimate foot contact (PFC) braking strategy, and trunk, hip, knee, and foot postures and motions during the final “plant” step (Table 1). The CMAS involves filming athletes (ideally ≥100 Hz) during a side-step cutting task (30–90°) using cameras placed approximately at hip height in the sagittal plane, frontal plane, and if possible with an additional camera 20–45° relative to the cut. Video footage is retrospectively viewed in video analysis software, and the athlete’s cutting trial is screened using the CMAS screening tool. The majority (7-items) of the CMAS criteria follow a dichotomous scale (yes or no), with lateral leg plant distance and frontal/transverse plane trunk positioning involving a description classification, with 3 and 4 possible descriptors, respectively (Table 1). Athletes are awarded a score if they display any of the items of the CMAS criteria (Table 1), and greater scores are typically indicative of suboptimal technique and greater peak KAMs [55][76].
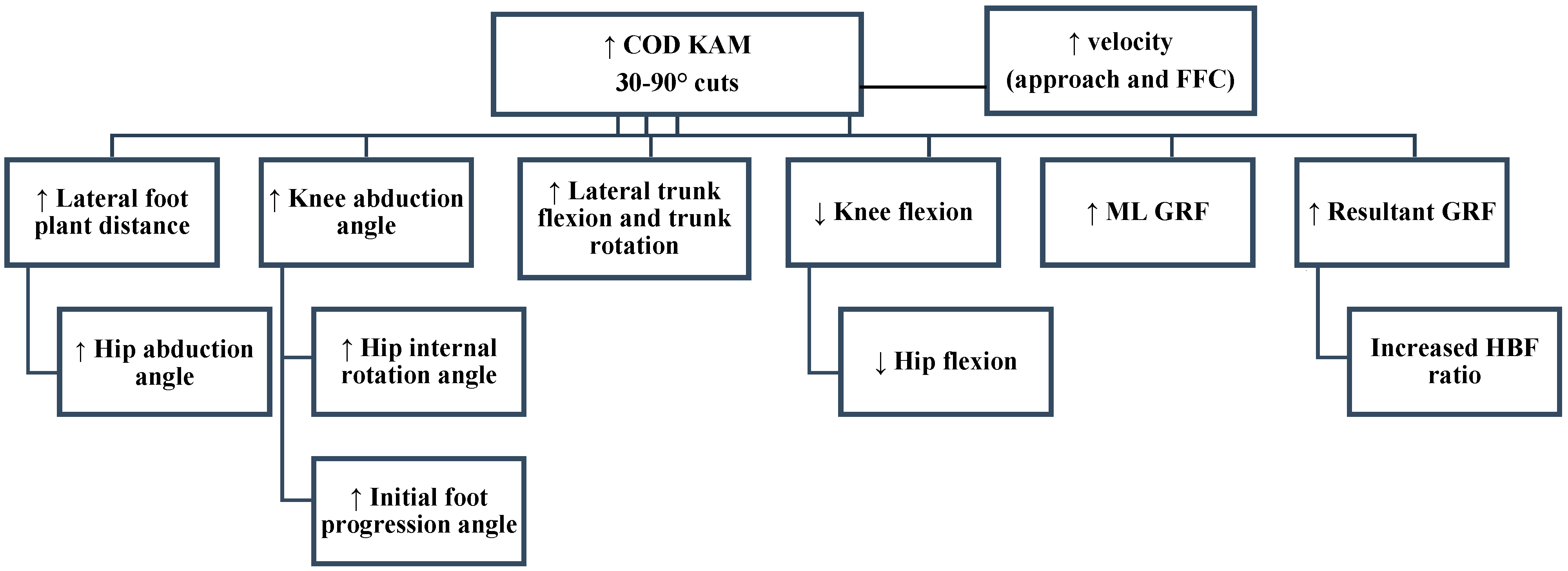
Figure 2. Knee abduction moment (KAM) deterministic model. Adapted from [93]; GRF: Ground reaction force; COD: Change of direction; ML: Medial-lateral; HBF: Horizontal braking force; FFC: Final foot contact.
Table 1. Cutting Movement Assessment Score Tool (CMAS).
| Recommended Camera | Variable | Observation | Score | ||
|---|---|---|---|---|---|
| Penultimate contact | |||||
| Side/20–45° |
|
Y/N | Y = 0/N = 1 | ||
| Final Contact | |||||
| Front/20–45° |
|
Wide, Moderate, Narrow | Wide = 2, Moderate = 1, Narrow = 0 | ||
| Front/20–45° |
|
Y/N | Y = 1/N = 0 | ||
| Front/20–45° |
|
Y/N | Y = 1/N = 0 | ||
| All 3 |
|
Y/N | Y = 1/N = 0 | ||
| Front/20–45° |
|
L/TR, U, M | L/TR = 2, U = 1, M = 0 | ||
| Side/20–45° |
|
Y/N | Y = 1/N = 0 | ||
| Side/20–45° |
|
Y/N | Y = 1/N = 0 | ||
| Front/20–45° |
|
Y/N | Y = 1/N = 0 | ||
| Low CMAS ≤ 3 | Moderate CMAS 4–6 | High CMAS ≥ 7 | Score | /11 | |
Key: PFC: Penultimate foot contact; WA: Weight acceptance; L: Lateral; TR: Trunk rotation; U: Upright; M: Medial; Y: Yes; N: No.
In the preliminary validation study by Jones et al. [76], using 3D motion and two 2D cameras (30 Hz) to record video data for qualitative screening, a strong association between CMAS and peak KAM (ρ = 0.633; p < 0.001) was demonstrated during a 60–90° cut. More recently, Dos’Santos [55] expanded on the preliminary study by investigating a greater sample size (41 vs. 8), using an extra camera placed 45° to the cut at a higher sampling rate (100 Hz vs. 30 Hz), and also slightly modified the CMAS (provided extra details) details to the CMAS screening tool. Substantiating the preliminary findings [76], a very large (ρ = 0.796, p < 0.001) relationship was observed between CMAS and peak KAM for participant average data [55]. In addition, athletes were divided into high (~7) and low (~3) CMAS groups (top 33% and bottom 33%), where cutting kinetics and kinematics were compared. Importantly, athletes with higher CMASs demonstrated “higher-risk” postures and knee joint loads connected with ACL injury risk compared to athletes with lower CMASs. These included significantly (moderate to very large effect sizes) greater mean vertical braking forces, greater peak KAAs, greater initial foot progression angles, greater lateral foot plant distances, and greater knee flexion (KFM), knee internal rotation (KIRM), and KAMs [55].
Later analysis in the study by Dos’Santos et al. [55], revealed that when statistical analysis was performed for all pooled trials, female trials, and male trials, large, large, and very large associations were observed between CMAS and peak KAMs (Supplementary Materials), respectively [93]. Additionally, in terms of cutting mechanics, greater peak and mean vertical braking forces, greater peak and initial KAAs, and lower peak knee flexion angle and range of motion, greater initial foot progression angles, greater lateral trunk flexion, greater lateral foot plant distances, and greater multiplanar knee joint moments were displayed during trials with higher CMASs (≥7) compared to lower CMASs (≤3) [93]. To the best of our knowledge, the LESS is the only other qualitative screening tool that has been validated against the gold standard of 3D motion analysis with respect to knee joint moments [74] and subsequent surrogates of ACL injury risk. Thus, the CMAS would appear to have validity and be a rigorous enough method to potentially identify athletes who generate high peak KAMs (and multiplanar knee joint loads) and potential ACL injury risk. This method requires only three high-speed cameras and video analysis software (which in most cases is free), which is a cost- and time-effective alternative to 3D motion analysis, and is a field-based method for practitioners.
4. CMAS Methodological Procedures
The CMAS is applicable to side-step cuts of 30–90° with published literature using the CMAS during 60–90° [76], 70° [94], and 90° cuts [55], and in unpublished observations, we have also used the CMAS during 45° cuts. Ideally, CMAS screening should take place on the same surface that the athlete performs their sport on (e.g., court, synthetic field-turf, grass) and where possible athletes should wear sport-specific footwear to improve ecological validity [95][96][97]. If athletes hold an implement in their sport (e.g., ball or racket), practitioners may consider screening cutting trials where athletes hold the implement to improve ecological validity. Anecdotally, we have had a positive experience screening ball-carrying 45° cutting in rugby union players. Nevertheless, it is advised that athletes tuck-in loose clothing, and ideally wear tight fitting clothing to make it easier to screen and observe movement quality and postures. Although the aim of the CMAS is to profile movement quality, practitioners may consider assessing performance using timing gates positioned at a start and finish line to obtain cutting completion time to monitor and standardise performance.
Figure 3 provides a schematic representation of the CMAS for administering during 45°, 70°, and 90° cuts. As a minimum recommendation, practitioners are encouraged to use 2 high-speed cameras for qualitative screening positioned on tripods placed at approximate hip height at least 3 metres away in the frontal plane and 5 metres away in the sagittal plane away from the cutting zone. However, to accommodate athletes who pre-rotate during the cut, and to reduce parallax error, practitioners are strongly encouraged to position an additional camera 20–45° to the cut to assist in more accurate qualitative screening. Although published research placed the third camera at 45° [55][94], we have recently had better observations of CMAS trials with a camera positioned at 20°. This approach has tended to reduce parallax error because the subjects who pre-rotate are more perpendicular to the 20° camera in contrast to 45° camera observations. As such, this has made subsequent screening of relevant criteria easier and is therefore our preferred method going forward. As previously stated, practitioners should ideally use high-speed cameras for qualitative screening, sampling at a minimum 100 Hz. Access to high-speed cameras for practitioners is becoming increasingly accessible as most smartphone and tablet technology have high-speed cameras as default features. Nonetheless, when using high-speed cameras for the CMAS, practitioners should ensure that there is sufficient lighting to permit accurate qualitative screening.
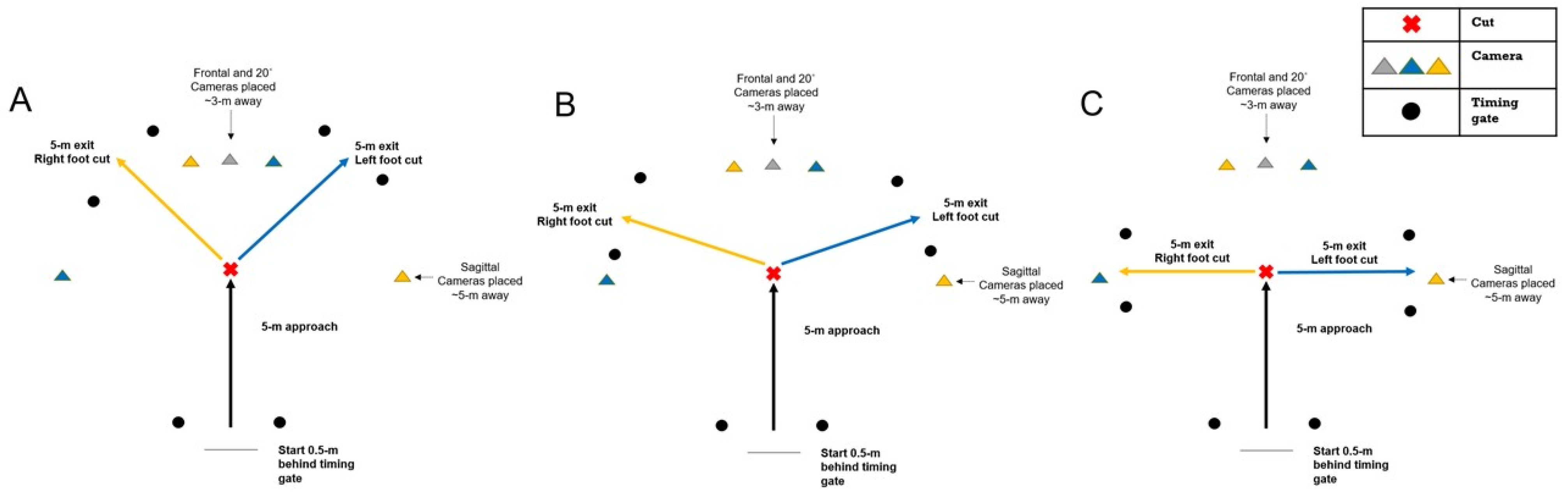
Figure 3. Schematic representation of the CMAS protocol. (A): 45° cut; (B): 70° cut; (C): 90° cut. Yellow cameras indicate camera placement for right foot cuts, blue cameras indicate camera placement for left foot cuts, grey camera used for both left and right cuts.
It is encouraged that practitioners evaluate 2–3 cutting trials per limb for each athlete during the cutting trials, typically during a cut which contains a 5-m entry and exit. However, practitioners are free to adjust entry and exit distances at their own discretion in context of their populations’ sporting demands. From our experience, we have been able to collect CMAS video footage (along with completion times) for 6 trials (3 trials per limb) in groups of athletes as large 12 in less than 15 min, highlighting the simplicity and application for large mass screening in contract to 3D motion analysis.
Once video footage data are collected, video footage should ideally be viewed in a software which enables videos to be played at various speeds, frame-by-frame, while a software which can open multiple video windows, create photo-sequences, and also contains drawing tools is also advantageous. We have used Kinovea software (0.8.15 for Windows, Bordeaux, France), which is free, and we have found this software to be more than adequate for qualitative screening purposes; however, practitioners are free to select an alternative video software at their own discretion. From our experience, qualitative screening of one trial takes ~3 min. However, given the subjective nature of qualitative screening, it is strongly encouraged that practitioners within sports science, sports medicine, and clinical departments are familiar and adequately trained using the CMAS and other qualitative screening tools. This is to ensure that high levels of intra- and inter-rater reliability are obtained, and more importantly so that the athlete obtains accurate, consistent, and reliable evaluations [57][58]. By this, it is strongly encouraged that practitioners within their departments perform their own in-house training and collect pilot video footage where they discuss and agree on “low-risk” and “high-risk” movement patterns. These should be consensually agreed by all coaches, practitioners, and potential raters within the department, team, or institution. Practitioners unfamiliar with the CMAS may consider receiving training and education from practitioners’ experienced in qualitative screening and knowledgeable in COD biomechanics. We have had recent success whereby the lead researcher has facilitated a one hour-training session and created manuals for raters outlining how to grade the cutting trials using the CMAS, and to establish and uniformly agree on “low-risk” and “high-risk” movement patterns. Subsequently we have observed high levels of intra- and inter-rater reliability [55][76][94].
5. CMAS Criteria Rationale and Operational Definitions
The purpose of the following section is to provide the rationale and operational definitions for the 9-items of the CMAS.
5.1. Item (1) Clear PFC Braking Strategy
COD is multistep action with evidence indicating that the PFC is involved in deceleration prior to COD, and is a “preparatory step” [30][98]. A “large anterior placement of the foot relative to centre of mass and backward inclination of the trunk relative to planted foot” is considered to increase horizontal braking forces during the PFC, based on research demonstrating a relationship between average horizontal GRF during PFC and peak KAMs during the FFC [30][93]. Reducing the majority of momentum during the PFC will reduce the braking requirements of the FFC, which may result in lower knee joint loads and protect against non-contact injury [30][42][62]. Maximising braking forces during the PFC is considered a safer strategy, as this braking is typically performed in the sagittal plane whereby the GRF vector is more aligned with the knee joint centre, and importantly the knee goes through substantially greater flexion as opposed to the FFC [99][100]. Figure 4 provides the operational definition and example yes and no “clear PFC braking strategy” images to assist in qualitative screening.
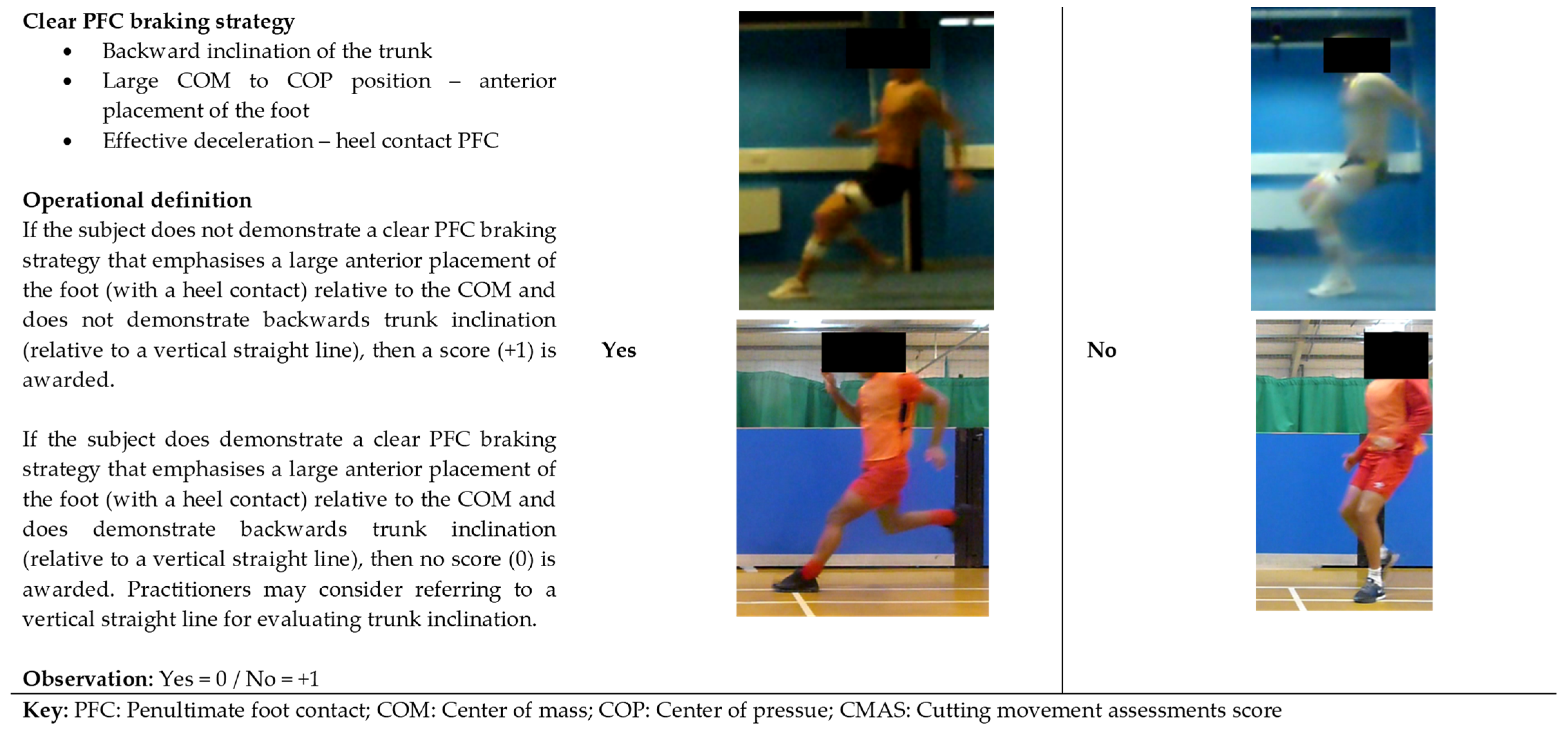
Figure 4. Operational definition and example images for CMAS item: clear PFC braking strategy.
5.2. Item (2) Lateral Leg Plant Distance
A wide lateral leg plant is a major determinant of peak KAM during side-step cutting [31][33][41][42][55][93]. This posture results in a more medial whole-body position with respect to the foot, creating a large GRF acting laterally outside the knee. Subsequently, this position results in a large moment arm between the perpendicular distance of the axis of rotation (knee) to the force (acting outside the knee), creating greater KAMs [41][42][69]. Abducted hip positions are also commonly observed characteristics displayed during visual inspection of non-contact ACL injuries during COD [20][25][26][101], and have also been associated with greater KAMs [68][69]. Wide lateral leg plants are typically performed to generate greater medio-lateral GRF, thus impulse, for acceleration into the new intended direction [42][98][102][103]. Additionally, the lateral leg plant is also considered a “false” step to deceive opponents [104]. Figure 5 provides the operational definition and example wide, moderate, and narrow “lateral leg plant distance” images to assist in qualitative screening.

Figure 5. Operational definition and example images for CMAS item: lateral leg plant.
5.3. Item (3) Hip in an Initially Rotated Position
Internal hip rotation (anatomical rotation) is a contributing factor to dynamic knee valgus which contributes to a more medially positioned knee relative to the GRF vector, thus increase in moment arm distance and subsequent KAM [40][41][63][69]. Figure 6 provides the operational definition and example yes and no “hip in an initially rotated position” images to assist in qualitative screening.
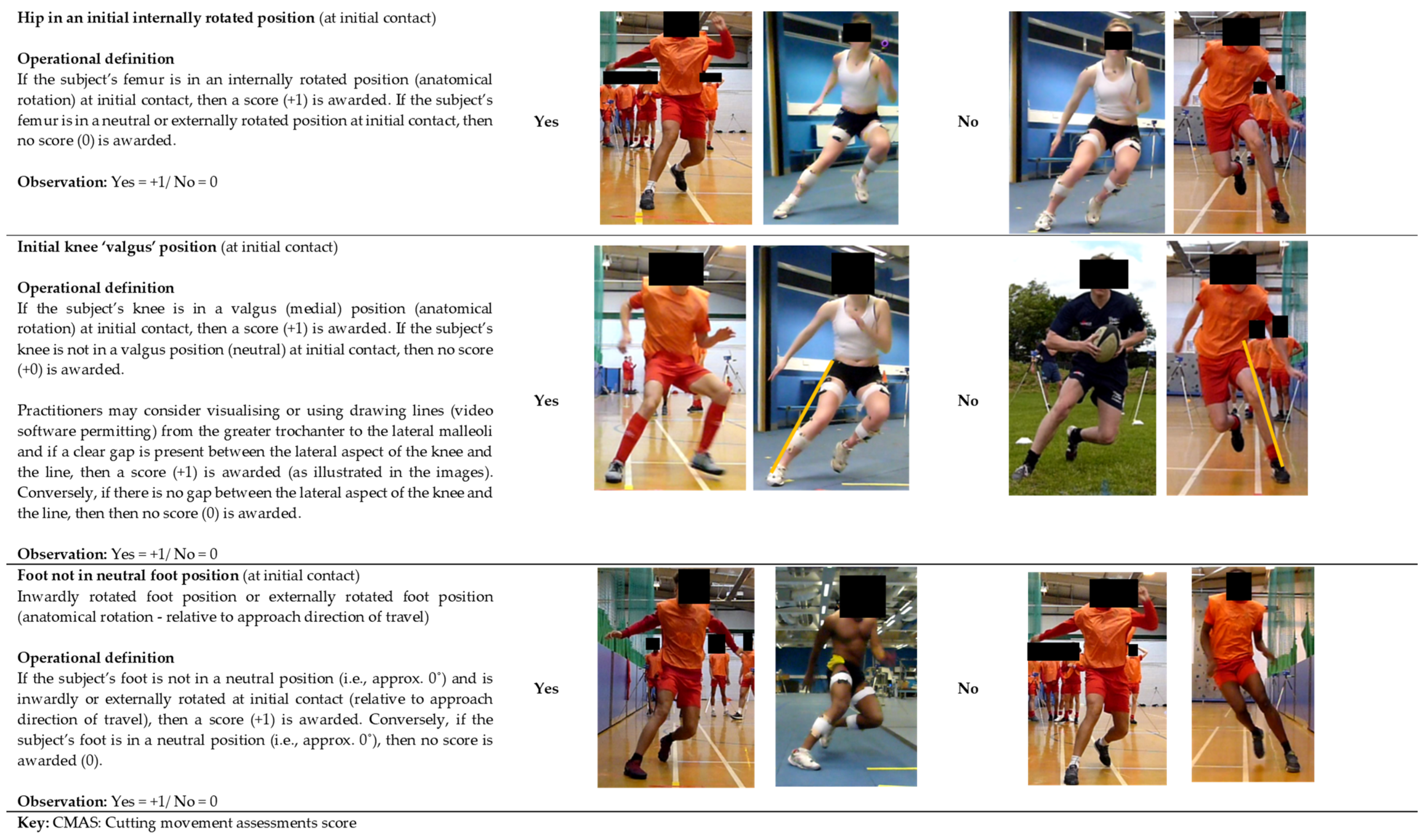
Figure 6. Operational definition and example images for CMAS items hip in an initial internally rotated position, initial knee valgus position, and foot not in neutral position.
5.4. Item (4) Initial Knee ‘Valgus’ Position
Initial knee valgus position (anatomical rotation) is associated with peak KAMs during cutting [33][40][42][62][63][93] and is considered a major determinant. An increased KAA at initial contact has an effect of placing the knee more medial to the resultant GRF vector, increasing the moment arm distance, leading to an increased KAM. Additionally, McLean et al. [105] reported a change in KAA of 2° can cause a 40 Nm increase in KAM (assuming a GRF of 2500 N), while greater KAAs were reported in female athletes who sustained an ACL injury compared to uninjured athletes [39]. Moreover, dynamic knee valgus is a commonly observed posture during non-contact ACL injuries during directional changes and landings [17][19][20][21][24][25][26][27][86][101]. Therefore, improving frontal plane knee control appears to be a worthwhile strategy to reduce ACL injury risk during side-stepping. Figure 6 provides the operational definition and example yes and no “initial knee valgus position” images to assist in qualitative screening.
5.5. Item (5) Foot Not in Neutral Foot Position
Greater initial foot progression angles (anatomical rotation) are associated with greater KAMs [62][69], with a neutral foot position considered the safest strategy [31][62][69]. Internally rotated foot positions during weight acceptance can result in a more medially positioned knee relative to the GRF vector, thus increased moment arm distance and subsequent KAM [62][69]. A neutral foot position would most likely result in forces being attenuated in the sagittal plane utilising the large knee and hip extensor musculature, which is potentially a safer strategy [62]. Equally, excessive foot external rotation increases the susceptibility to eversion and pronation which could lead to knee valgus and tibial internal rotation [106][107][108], thus ACL loading. External rotation of the foot has also been stated as a visual characteristic observed during COD non-contact ACL injuries [26]. Figure 6 provides the operational definition and example yes and no “foot not in neutral foot position” images to assist in qualitative screening.
5.6. Item (6) Frontal/Transverse Plane Trunk Position
The trunk contains approximately half of the body’s mass [109], and during cutting the entire body’s mass must be balanced and supported on one leg, thus trunk control and positioning is a critical factor influencing knee joint loads [87][110][111]. Lateral trunk flexion [31][42][64] or trunk rotation [31][65] towards stance limb are major determinants of peak KAM during COD. Laterally flexing the trunk (deviation of the trunk) or rotating the trunk towards the plant leg shifts weight laterally, creating a more laterally directed GRF vector, thereby increasing its moment arm relative to the knee joint centre, and therefore increasing the resultant KAM [31][32][42][64][65]. Conversely, trunk lean and rotation towards the intended direction of travel shifts the GRF vector more in line with the knee joint centre, thus decreasing the moment arm distance [65][66]. Prospective research has shown deficits in trunk control and proprioception are associated with increased risk of non-contact ACL injury [112][113], while lateral trunk flexion is also an observed visual posture during non-contact ACL injuries during plant-and cut manoeuvres and landings [25][27][87].
Collectively, these findings suggest side-step techniques which encourage trunk lean and rotation towards the intended direction of travel may potentially reduce knee joint loading and subsequent risk of injury [31][32][42][64][65]. Computer simulations of side-stepping have showed a reduction in knee valgus loading through shifting the whole-body centre of mass more medially [66], while COD technique modification interventions which focus on reducing lateral foot plant distances and maintaining an erect (frontal plane) trunk posture was found to reduce KAMs [32]. Furthermore, from a performance perspective, trunk lean and rotation towards the intended direction of travel is also associated with faster COD performance [41][114][115]. Figure 7 provides the operational definition and example lateral, trunk rotation, upright, and medial “frontal/transverse plane trunk position” images to assist in qualitative screening.
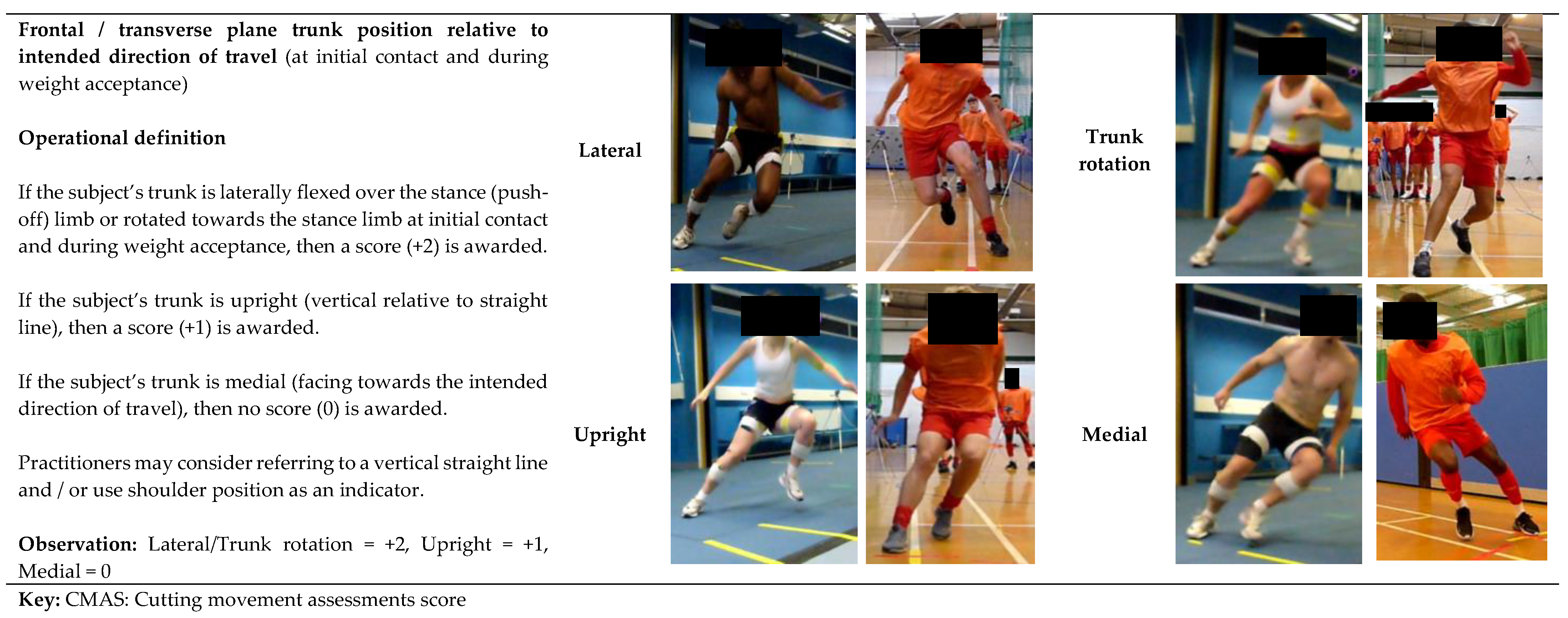
Figure 7. Operational definition and example images for CMAS item: frontal/transverse plane trunk position relative to intended direction of travel.
5.7. Item (7) Trunk Upright or Leaning Back Throughout Contact
Trunk inclination (leaning back or upright) with limited hip flexion and trunk flexion displacement during weight acceptance may increase the overall knee joint load, due an increased lever arm of the trunk relative to the knee and increasing the centre of mass distance from the base of support [116]. Some trunk flexion allows generation of hip moments to help attenuate GRF during weight acceptance and thus, may lower KAMs [62]. Increasing hip flexion and promoting a hip dominant strategy are involved in GRF attenuation [117][118][119], energy dissipation [120][121], reducing loading rates [119] and reducing knee joint loads [119][120][122][123] during high-impact tasks. Increasing hip flexion increases the moment arm distance at the hip which creates a greater hip flexor moment (utilising hip extensor musculature). This can have the effect of unloading the knee by more evenly distributing loading proximally up the lower-limb chain [62][119][120][123], thus reducing the demands for the knee. Figure 8 provides the operational definition and example yes and no “trunk upright or leaning back throughout contact” images to assist in qualitative screening.
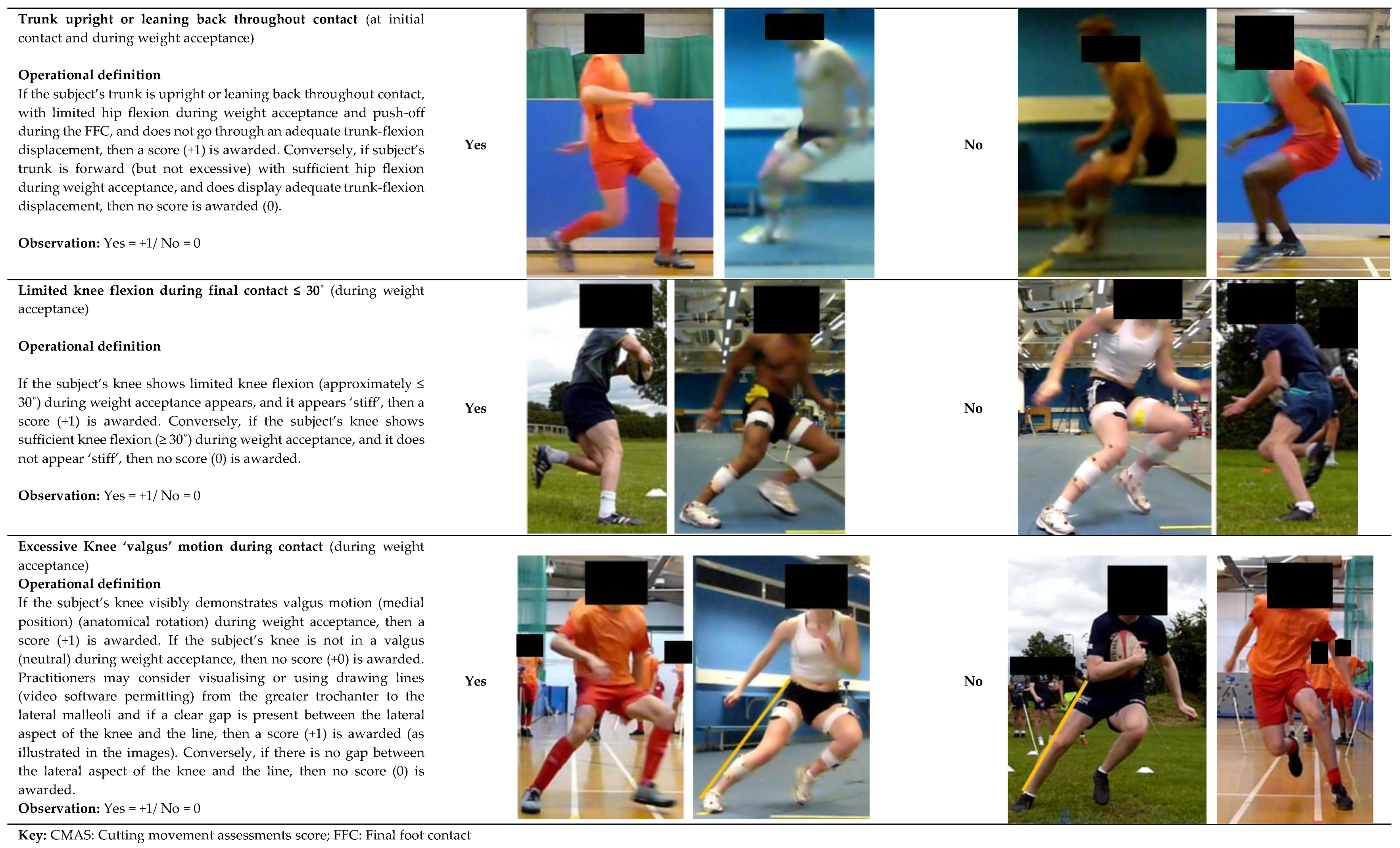
Figure 8. Operational definition and example images for CMAS items trunk upright or leaning back throughout contact, limited knee flexion, and excessive knee valgus motion.
5.8. Item (8) Limited Knee Flexion
Extended knee postures with large anterior tibial shear can increase ACL strain [124][125][126][127] and are also commonly observed visual characteristics of non-contact ACL injury [17][18][19][20][21][23][24][25][26][86][101]. Moreover, stiffer landings and extended knee postures can increase GRFs and are associated with increased risk of ACL injury [128]. Stiffer weight acceptance strategies can increase impact GRFs [67][129][130], and greater GRFs are associated with increased KAMs [63][69]. Lower knee flexion angles are also associated with greater KAMs during COD [33][68]. Figure 8 provides the operational definition and example yes and no “limited knee flexion” images to assist in qualitative screening.
5.9. Item (9) Excessive Knee ‘Valgus’ Motion during Weight Acceptance
The rationale for knee valgus was presented earlier (Item 4). Figure 8 provides the operational definition and example yes and no “excessive knee valgus motion during weight acceptance” images to assist in qualitative screening.
5.10. CMAS Criteria: Considerations for Rearfoot, Midfoot, Forefoot Contact?
Although not a specific criterion on the CMAS qualitative tool, practitioners are encouraged to monitor foot contact position during initial contact. Previous research has reported rearfoot techniques evoke more extended, abducted knee positions, greater GRF, and greater knee joint loads [33][131][132][133][134]. Additionally, heel strikes are commonly observed characteristics of non-contact ACL injuries during COD [18][28], while an ACL case study also reported a heel strike during COD [135]. However, an anterior placement of the foot relative to the centre of mass is required to create posterior braking force, typically characterised with a rearfoot technique to facilitate braking [136]. From our experience, heel strikes during the FFC appear to be consequence of poor and ineffective PFC braking; thus, resulting in a large anterior placement of the foot relative to the centre of mass to subsequently create posterior braking force. Moreover, although greater knee joint loads are present with a rearfoot technique, from an ankle injury perspective, a rearfoot contact results in a greater surface area, thus base of support and stability for changing direction. This is particularly important for generating perpendicular force. Conversely, a forefoot landing results in a reduced surface area and base of support which is most likely suboptimal for perpendicular force application and ankle joint stability. Additionally, it should be highlighted that a forefoot strategy increases (internal) ankle plantar-flexor moment and gastrocnemius activity, which acts as an antagonist to the ACL, and may contribute to ACL strain (tibial shear mechanism) [137][138][139].
6. Practical Applications: Interpreting CMAS Score and the CMAS Training Recommendations Decision Tree
As strong relationships between CMAS and peak KAMs have been observed [55][76][93], a higher total score is generally indicative of suboptimal technique and greater non-contact ACL injury risk. Additionally, “higher-risk” cutting postures connected with ACL injury risk were demonstrated by participants and trials with “high” CMASs (~7) compared to participants and trials with “low” CMASs (~3) [55][93]. As such, practitioners can use scores of ≥7, 4–6, and ≤3 as initial benchmarks to classify athletes with high, moderate, and low CMASs [55][93], respectively. However, practitioners should note that suboptimal and unsafe technique may still be displayed during trials with low CMASs; therefore, it is advised to focus on the CMAS criteria where athletes scored deficits [57][76]. For example, an athlete with a low CMAS may still display “high-risk” cutting deficits, such as knee valgus, lateral trunk flexion, limited knee flexion, or hip internal rotation. Therefore, in this scenario, the athlete would still warrant specific injury risk mitigation training and conditioning. In addition, it is worth noting that some CMAS criteria are associated with faster performance [41][43][67][70]. For instance, a wide lateral leg plant is displayed to generate greater medio-lateral propulsive forces and subsequent exit velocity [41][42], while reduced knee flexion is associated with shorter ground contact time [43][67]. Thus, practitioners must be mindful and acknowledge the trade-off between knee joint loading (injury risk) and performance when screening and modifying cutting mechanics.
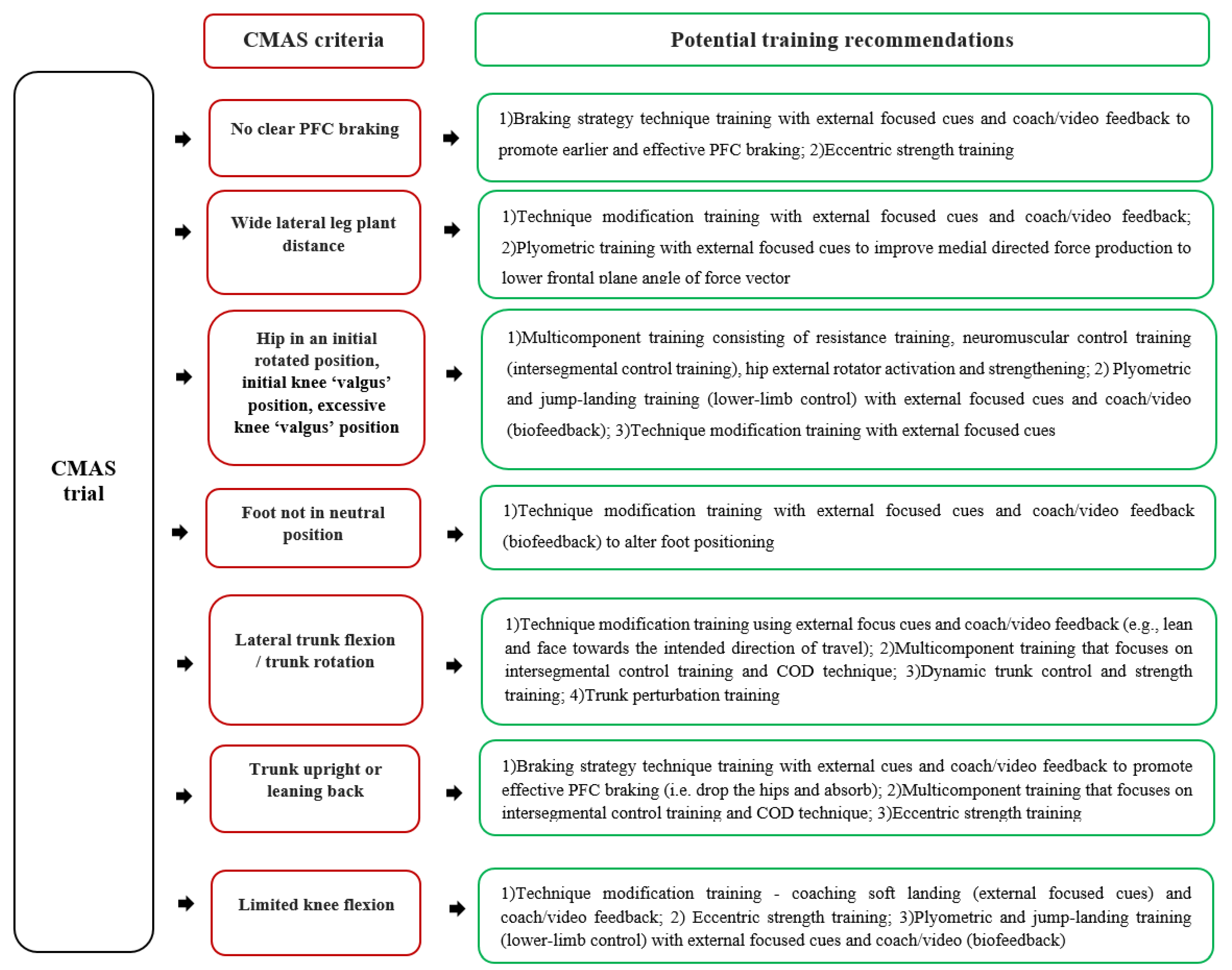
A low CMAS score generally indicates an ability to performance a cutting task well against the prescribed CMAS criteria, in a closed, controlled environment. Further work is needed to assess both scoring during tasks in a sport-specific, open skill environment to determine if performance transitions (scores) to these environments. Additionally, it is worth highlighting that the CMAS is based on postures associated with ACL injury risk, but the CMAS is indicating relative risk of injury and we are by no means are stating that athletes with greater scores will definitely sustain an ACL injury. Nevertheless, practitioners are recommended to use the CMAS as a regular monitoring tool to assist in identifying “high-risk” cutting deficits in their athletes. This can be used to inform and help develop individualised training programmes to modify the specific deficits and mitigate potential ACL injury risk [59][60][140]. Readers are encouraged to read specific reviews regarding training strategies to mitigate non-contact ACL injury [45][46][48][141][142]; thus, a brief overview is presented in the CMAS training recommendations decision tree (Figure 9).
References
- Hewett, T. Preventive biomechanics: A paradigm shift with a translational approach to biomechanics. Am. J. Sports Med. 2017, 45, 2654–2664.
- Cumps, E.; Verhagen, E.; Annemans, L.; Meeusen, R. Injury rate and socioeconomic costs resulting from sports injuries in Flanders: Data derived from sports insurance statistics 2003. Br. J. Sports Med. 2008, 42, 767–772.
- Quatman, C.E.; Hewett, T.E. The anterior cruciate ligament injury controversy: Is “valgus collapse” a sex-specific mechanism? Br. J. Sports Med. 2009, 43, 328–335.
- Langford, J.L.; Webster, K.E.; Feller, J.A. A prospective longitudinal study to assess psychological changes following anterior cruciate ligament reconstruction surgery. Br. J. Sports Med. 2009, 43, 377–378.
- Lohmander, L.S.; Englund, P.M.; Dahl, L.L.; Roos, E.M. The long-term consequence of anterior cruciate ligament and meniscus injuries. Am. J. Sports Med. 2007, 35, 1756–1769.
- Quatman, C.E.; Quatman-Yates, C.C.; Hewett, T.E. A ‘Plane’Explanation of Anterior Cruciate Ligament Injury Mechanisms. Sports Med. 2010, 40, 729–746.
- Meeuwisse, W.H.; Tyreman, H.; Hagel, B.; Emery, C. A dynamic model of etiology in sport injury: The recursive nature of risk and causation. Clin. J. Sport Med. 2007, 17, 215–219.
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition-narrative review and new concept. Br. J. Sports Med. 2016, 50, 1309–1314.
- Lloyd, D.G. Rationale for training programs to reduce anterior cruciate ligament injuries in Australian football. J. Orthop. Sport Phys. 2001, 31, 645–654.
- Lipps, D.B.; Wojtys, E.M.; Ashton-Miller, J.A. Anterior cruciate ligament fatigue failures in knees subjected to repeated simulated pivot landings. Am. J. Sports Med. 2013, 41, 1058–1066.
- Wojtys, E.M.; Beaulieu, M.L.; Ashton-Miller, J.A. New perspectives on ACL injury: On the role of repetitive sub-maximal knee loading in causing ACL fatigue failure. J. Orthop. Res. 2016, 34, 2059–2068.
- Gallagher, S.; Schall, M.C., Jr. Musculoskeletal disorders as a fatigue failure process: Evidence, implications and research needs. Ergonomics 2017, 60, 255–269.
- Beaulieu, M.L.; Wojtys, E.M.; Ashton-Miller, J.A. Risk of anterior cruciate ligament fatigue failure is increased by limited internal femoral rotation during in vitro repeated pivot landings. Am. J. Sports Med. 2015, 43, 2233–2241.
- Chen, J.; Kim, J.; Shao, W.; Schlecht, S.H.; Baek, S.Y.; Jones, A.K.; Ahn, T.; Ashton-Miller, J.A.; Banaszak Holl, M.M.; Wojtys, E.M. An Anterior Cruciate Ligament Failure Mechanism. Am. J. Sports Med. 2019, 47, 2067–2076.
- Bahr, R.; Krosshaug, T. Understanding injury mechanisms: A key component of preventing injuries in sport. Br. J. Sports Med. 2005, 39, 324–329.
- Edwards, W.B. Modeling overuse injuries in sport as a mechanical fatigue phenomenon. Exerc. Sport Sci. Rev. 2018, 46, 224–231.
- Walden, M.; Krosshaug, T.; Bjorneboe, J.; Andersen, T.E.; Faul, O.; Hagglund, M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: A systematic video analysis of 39 cases. Br. J. Sports Med. 2015, 49, 1452–1460.
- Montgomery, C.; Blackburn, J.; Withers, D.; Tierney, G.; Moran, C.; Simms, C. Mechanisms of ACL injury in professional rugby union: A systematic video analysis of 36 cases. Br. J. Sports Med. 2018, 52, 944–1001.
- Olsen, O.-E.; Myklebust, G.; Engebretsen, L.; Bahr, R. Injury mechanisms for anterior cruciate ligament injuries in team handball a systematic video analysis. Am. J. Sports Med. 2004, 32, 1002–1012.
- Brophy, R.H.; Stepan, J.G.; Silvers, H.J.; Mandelbaum, B.R. Defending puts the anterior cruciate ligament at risk during soccer: A gender-based analysis. Sports Health 2015, 7, 244–249.
- Cochrane, J.L.; Lloyd, D.G.; Buttfield, A.; Seward, H.; McGivern, J. Characteristics of anterior cruciate ligament injuries in Australian football. J. Sci. Med. Sport 2007, 10, 96–104.
- Faude, O.; Junge, A.; Kindermann, W.; Dvorak, J. Injuries in female soccer players a prospective study in the german national league. Am. J. Sports Med. 2005, 33, 1694–1700.
- Boden, B.P.; Dean, G.S.; Feagin, J.A.; Garrett, W.E. Mechanisms of anterior cruciate ligament injury. Orthopedics 2000, 23, 573–578.
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebretsen, L.; Bahr, R.; Krosshaug, T. Mechanisms for noncontact anterior cruciate ligament injuries knee joint kinematics in 10 injury situations from female team handball and basketball. Am. J. Sports Med. 2010, 38, 2218–2225.
- Kimura, Y.; Ishibashi, Y.; Tsuda, E.; Yamamoto, Y.; Tsukada, H.; Toh, S. Mechanisms for anterior cruciate ligament injuries in badminton. Br. J. Sports Med. 2010, 44, 1124–1127.
- Johnston, J.T.; Mandelbaum, B.R.; Schub, D.; Rodeo, S.A.; Matava, M.J.; Silvers, H.J.; Cole, B.J.; ElAttrache, N.S.; McAdams, T.R.; Brophy, R.H. Video analysis of anterior cruciate ligament tears in professional American football athletes. Am. J. Sports Med. 2018, 46, 862–868.
- Stuelcken, M.C.; Mellifont, D.B.; Gorman, A.D.; Sayers, M.G. Mechanisms of anterior cruciate ligament injuries in elite women’s netball: A systematic video analysis. J. Sports Sci. 2016, 34, 1516–1522.
- Boden, B.P.; Torg, J.S.; Knowles, S.B.; Hewett, T.E. Video analysis of anterior cruciate ligament injury abnormalities in hip and ankle kinematics. Am. J. Sports Med. 2009, 37, 252–259.
- Besier, T.F.; Lloyd, D.G.; Cochrane, J.L.; Ackland, T.R. External loading of the knee joint during running and cutting maneuvers. Med. Sci. Sports Exerc. 2001, 33, 1168–1175.
- Jones, P.A.; Herrington, L.; Graham-Smith, P. Braking characteristics during cutting and pivoting in female soccer players. J. Electromyogr. Kinesiol. 2016, 30, 46–54.
- Dempsey, A.R.; Lloyd, D.G.; Elliott, B.C.; Steele, J.R.; Munro, B.J.; Russo, K.A. The effect of technique change on knee loads during sidestep cutting. Med. Sci. Sports Exerc. 2007, 39, 1765–1773.
- Dempsey, A.R.; Lloyd, D.G.; Elliott, B.C.; Steele, J.R.; Munro, B.J. Changing sidestep cutting technique reduces knee valgus loading. Am. J. Sports Med. 2009, 37, 2194–2200.
- Kristianslund, E.; Faul, O.; Bahr, R.; Myklebust, G.; Krosshaug, T. Sidestep cutting technique and knee abduction loading: Implications for ACL prevention exercises. Br. J. Sports Med. 2014, 48, 779–783.
- Shin, C.S.; Chaudhari, A.M.; Andriacchi, T.P. Valgus plus internal rotation moments increase anterior cruciate ligament strain more than either alone. Med. Sci. Sports Exerc. 2011, 43, 1484–1491.
- Markolf, K.L.; Burchfield, D.M.; Shapiro, M.M.; Shepard, M.F.; Finerman, G.A.M.; Slauterbeck, J.L. Combined knee loading states that generate high anterior cruciate ligament forces. J. Orthop. Res. 1995, 13, 930–935.
- Kiapour, A.M.; Demetropoulos, C.K.; Kiapour, A.; Quatman, C.E.; Wordeman, S.C.; Goel, V.K.; Hewett, T.E. Strain response of the anterior cruciate ligament to uniplanar and multiplanar loads during simulated landings: Implications for injury mechanism. Am. J. Sports Med. 2016, 44, 2087–2096.
- Oh, Y.K.; Lipps, D.B.; Ashton-Miller, J.A.; Wojtys, E.M. What strains the anterior cruciate ligament during a pivot landing? Am. J. Sports Med. 2012, 40, 574–583.
- Bates, N.A.; Myer, G.D.; Shearn, J.T.; Hewett, T.E. Anterior cruciate ligament biomechanics during robotic and mechanical simulations of physiologic and clinical motion tasks: A systematic review and meta-analysis. Clin. Biomech. 2015, 30, 1–13.
- Hewett, T.; Myer, G.D.; Ford, K.R.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Van den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes a prospective study. Am. J. Sports Med. 2005, 33, 492–501.
- McLean, S.G.; Huang, X.; van den Bogert, A.J. Association between lower extremity posture at contact and peak knee valgus moment during sidestepping: Implications for ACL injury. Clin. Biomech. 2005, 20, 863–870.
- Havens, K.L.; Sigward, S.M. Cutting mechanics: Relation to performance and anterior cruciate ligament injury risk. Med. Sci. Sports Exerc. 2015, 47, 818–824.
- Jones, P.A.; Herrington, L.; Graham-Smith, P. Technique determinants of knee joint loads during cutting in female soccer players. Hum. Mov. Sci. 2015, 42, 203–211.
- Fox, A.S. Change-of-Direction Biomechanics: Is What’s Best for Anterior Cruciate Ligament Injury Prevention Also Best for Performance? Sports Med. 2018, 48, 1799–1807.
- Pappas, E.; Nightingale, E.J.; Simic, M.; Ford, K.R.; Hewett, T.E.; Myer, G.D. Do exercises used in injury prevention programmes modify cutting task biomechanics? A systematic review with meta-analysis. Br. J. Sports Med. 2015, 49, 673–680.
- Padua, D.A.; DiStefano, L.J.; Hewett, T.E.; Garrett, W.E.; Marshall, S.W.; Golden, G.M.; Shultz, S.J.; Sigward, S.M. National Athletic Trainers’ Association Position Statement: Prevention of Anterior Cruciate Ligament Injury. J. Athl. Train. 2018, 53, 5–19.
- Dos’Santos, T.; Thomas, C.; Comfort, P.; Jones, P.A. The Effect of Training Interventions on Change of Direction Biomechanics Associated with Increased Anterior Cruciate Ligament Loading: A Scoping Review. Sports Med. 2019, 49, 1837–1859.
- Lloyd, D.G.; Buchanan, T.S. Strategies of muscular support of varus and valgus isometric loads at the human knee. J. Biomech. 2001, 34, 1257–1267.
- Donnelly, C.; Elliott, B.C.; Ackland, T.R.; Doyle, T.L.; Beiser, T.F.; Finch, C.F.; Cochrane, J.; Dempsey, A.R.; Lloyd, D. An anterior cruciate ligament injury prevention framework: Incorporating the recent evidence. Res. Sports Med. 2012, 20, 239–262.
- Fox, A.S.; Bonacci, J.; McLean, S.G.; Saunders, N. Efficacy of ACL injury risk screening methods in identifying high-risk landing patterns during a sport-specific task. Scand. J. Med. Sci. Sports 2017, 27, 525–534.
- Zahidi, N.N.M.; Ismail, S.I. Notational analysis of evasive agility skills executed by attacking ball carriers among elite rugby players of the 2015 Rugby World Cup. J. Movement Health Exerc. 2018, 7, 99–113.
- Wheeler, K.W.; Askew, C.D.; Sayers, M.G. Effective attacking strategies in rugby union. Eur. J. Sports Sci. 2010, 10, 237–242.
- Karcher, C.; Buchheit, M. On-court demands of elite handball, with special reference to playing positions. Sports Med. 2014, 44, 797–814.
- Taylor, J.B.; Wright, A.A.; Dischiavi, S.L.; Townsend, M.A.; Marmon, A.R. Activity Demands During Multi-Directional Team Sports: A Systematic Review. Sports Med. 2017, 47, 2533–2551.
- Dos’Santos, T.; McBurnie, A.; Thomas, C.; Comfort, P.; Jones, P.A. Biomechanical Comparison of Cutting Techniques: A Review and Practical Applications. Strength Cond. J. 2019, 41, 40–54.
- Dos’Santos, T.; McBurnie, A.; Donelon, T.; Thomas, C.; Comfort, P.; Jones, P.A. A qualitative screening tool to identify athletes with “high-risk” movement mechanics during cutting: The cutting movement assessment score (CMAS). Phys. Ther. Sport 2019, 38, 152–161.
- Bahr, R. Why screening tests to predict injury do not work and probably never will: A critical review. Br. J. Sports Med. 2016, 50, 776–780.
- Fox, A.S.; Bonacci, J.; McLean, S.G.; Spittle, M.; Saunders, N. A systematic evaluation of field-based screening methods for the assessment of anterior cruciate ligament (ACL) injury risk. Sports Med. 2016, 46, 715–735.
- McCunn, R.; Aus der Fünten, K.; Fullagar, H.H.K.; McKeown, I.; Meyer, T. Reliability and association with injury of movement screens: A critical review. Sports Med. 2015, 46, 763–781.
- Herrington, L.C.; Munro, A.G.; Jones, P.A. Assessment of factors associated with injury risk. In Performance Assessment in Strength and Conditioning; Comfort, P., McMahon, J.J., Jones, P.A., Eds.; Routledge: Abingdon, UK, 2018; pp. 53–95.
- Mok, K.-M.; Leow, R.-S. Measurement of movement patterns to enhance ACL injury prevention-A dead end? J. Sports Med. Arthrosc. Rehabil. Technol. 2016, 5, 13–16.
- McCunn, R.; Meyer, T. Screening for risk factors: If you liked it then you should have put a number on it. Br. J. Sports Med. 2016, 50, 1354.
- Jones, P.A.; Herrington, L.; Graham-Smith, P. Technique determinants of knee abduction moments during pivoting in female soccer players. Clin. Biomech. 2016, 31, 107–112.
- Sigward, S.M.; Cesar, G.M.; Havens, K.L. Predictors of frontal plane knee moments during side-step cutting to 45 and 110 degrees in men and women: Implications for anterior cruciate ligament injury. Clin. J. Sport Med. 2015, 25, 529–534.
- Jamison, S.T.; Pan, X.; Chaudhari, A.M.W. Knee moments during run-to-cut maneuvers are associated with lateral trunk positioning. J. Biomech. 2012, 45, 1881–1885.
- Frank, B.; Bell, D.R.; Norcross, M.F.; Blackburn, J.T.; Goerger, B.M.; Padua, D.A. Trunk and hip biomechanics influence anterior cruciate loading mechanisms in physically active participants. Am. J. Sports Med. 2013, 41, 2676–2683.
- Donnelly, C.J.; Lloyd, D.G.; Elliott, B.C.; Reinbolt, J.A. Optimizing whole-body kinematics to minimize valgus knee loading during sidestepping: Implications for ACL injury risk. J. Biomech. 2012, 45, 1491–1497.
- Dai, B.; William, E.G.; Michael, T.G.; Darin, A.P.; Robin, M.Q.; Bing, Y. The Effects of 2 Landing Techniques on Knee Kinematics, Kinetics, and Performance During Stop-Jump and Side-Cutting Tasks. Am. J. Sports Med. 2014, 43, 466–474.
- Weir, G.; Alderson, J.; Smailes, N.; Elliott, B.; Donnelly, C. A Reliable Video-based ACL Injury Screening Tool for Female Team Sport Athletes. Int. J. Sports Med. 2019, 40, 191–199.
- Sigward, S.M.; Powers, C.M. Loading characteristics of females exhibiting excessive valgus moments during cutting. Clin. Biomech. 2007, 22, 827–833.
- Dos’Santos, T.; Thomas, C.; Comfort, P.; Jones, P.A. The effect of angle and velocity on change of direction biomechanics: An angle-velocity trade-off. Sports Med. 2018, 48, 2235–2253.
- McBurnie, A.; Dos’ Santos, T.; Jones, P.A. Biomechanical Associates of Performance and Knee Joint Loads During an 70–90° Cutting Maneuver in Sub-Elite Soccer Players. J. Strength Cond. Res. 2019.
- Kristianslund, E.; Krosshaug, T. Comparison of drop jumps and sport-specific sidestep cutting: Implications for anterior cruciate ligament injury risk screening. Am. J. Sports Med. 2013, 41, 684–688.
- Chinnasee, C.; Weir, G.; Sasimontonkul, S.; Alderson, J.; Donnelly, C. A Biomechanical Comparison of Single-Leg Landing and Unplanned Sidestepping. Int. J. Sports Med. 2018, 39, 636–645.
- Padua, D.A.; Marshall, S.W.; Boling, M.C.; Thigpen, C.A.; Garrett, W.E.; Beutler, A.I. The landing error scoring system (LESS) is a valid and reliable clinical assessment tool of jump-landing biomechanics the JUMP-ACL study. Am. J. Sports Med. 2009, 37, 1996–2002.
- Herrington, L.; Munro, A. A preliminary investigation to establish the criterion validity of a qualitative scoring system of limb alignment during single-leg squat and landing. J. Exerc. Sports Orthop. 2014, 1, 1–6.
- Jones, P.A.; Donelon, T.; Dos’ Santos, T. A preliminary investigation into a qualitative assessment tool to identify athletes with high knee abduction moments during cutting: Cutting Movement Assessment Score (CMAS). Prof. Strength Cond. 2017, 47, 37–42.
- Nilstad, A.; Andersen, T.E.; Kristianslund, E.; Bahr, R.; Myklebust, G.; Steffen, K.; Krosshaug, T. Physiotherapists can identify female football players with high knee valgus angles during vertical drop jumps using real-time observational screening. J. Orthop. Sport Phys. 2014, 44, 358–365.
- Smith, H.C.; Johnson, R.J.; Shultz, S.J.; Tourville, T.; Holterman, L.A.; Slauterbeck, J.; Vacek, P.M.; Beynnon, B.D. A prospective evaluation of the Landing Error Scoring System (LESS) as a screening tool for anterior cruciate ligament injury risk. Am. J. Sports Med. 2012, 40, 521–526.
- Ekegren, C.L.; Miller, W.C.; Celebrini, R.G.; Eng, J.J.; Macintyre, D.L. Reliability and validity of observational risk screening in evaluating dynamic knee valgus. J. Orthop. Sport Phys. 2009, 39, 665–674.
- Padua, D.A.; Boling, M.C.; DiStefano, L.J.; Onate, J.A.; Beutler, A.I.; Marshall, S.W. Reliability of the landing error scoring system-real time, a clinical assessment tool of jump-landing biomechanics. J. Sport Rehabil. 2011, 20, 145–156.
- Myer, G.D.; Brent, J.L.; Ford, K.R.; Hewett, T.E. Real-time assessment and neuromuscular training feedback techniques to prevent ACL injury in female athletes. Strength Cond. J. 2011, 33, 21–35.
- Myer, G.D.; Ford, K.R.; Hewett, T.E. Tuck jump assessment for reducing anterior cruciate ligament injury risk. Athl. Ther. Today J. Sports Health Care Prof. 2008, 13, 39–44.
- Herrington, L.; Myer, G.D.; Munro, A. Intra and inter-tester reliability of the tuck jump assessment. Phys. Ther. Sport 2013, 14, 152–155.
- Almangoush, A.; Herrington, L.; Jones, R. A preliminary reliability study of a qualitative scoring system of limb alignment during single leg squat. Phys. Ther. Rehabil. 2014, 1, 1–7.
- Herrington, L.; Myer, G.; Horsley, I. Task based rehabilitation protocol for elite athletes following anterior cruciate ligament reconstruction: A clinical commentary. Phys. Ther. Sport 2013, 14, 188–198.
- Krosshaug, T.; Nakamae, A.; Boden, B.P.; Engebretsen, L.; Smith, G.; Slauterbeck, J.R.; Hewett, T.E.; Bahr, R. Mechanisms of anterior cruciate ligament injury in basketball video analysis of 39 cases. Am. J. Sports Med. 2007, 35, 359–367.
- Hewett, T.E.; Torg, J.S.; Boden, B.P. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: Lateral trunk and knee abduction motion are combined components of the injury mechanism. Br. J. Sports Med. 2009, 43, 417–422.
- Alenezi, F.; Herrington, L.; Jones, P.; Jones, R. Relationships between lower limb biomechanics during single leg squat with running and cutting tasks: A preliminary investigation. Br. J. Sports Med. 2014, 48, 560–561.
- Tanikawa, H.; Matsumoto, H.; Komiyama, I.; Kiriyama, Y.; Toyama, Y.; Nagura, T. Comparison of knee mechanics among risky athletic motions for noncontact anterior cruciate ligament injury. J. Appl. Biomech. 2013, 29, 749–755.
- O’Connor, K.M.; Monteiro, S.K.; Hoelker, I.A. Comparison of selected lateral cutting activities used to assess ACL injury risk. J. Appl. Biomech. 2009, 25, 9–21.
- Jones, P.A.; Herrington, L.C.; Munro, A.G.; Graham-Smith, P. Is there a relationship between landing, cutting, and pivoting tasks in terms of the characteristics of dynamic valgus? Am. J. Sports Med. 2014, 42, 2095–2102.
- Munro, A.G.; Herrington, L.; Comfort, P. The Relationship Between 2-Dimensional Knee-Valgus Angles During Single-Leg Squat, Single-Leg-Land, and Drop-Jump Screening Tests. J. Sports Rehabil. 2017, 26, 72–77.
- Dos’ Santos, T. Biomechanical Determinants of Injury Risk and Performance during Change of Direction: Implications for Screening and Intervention. Doctoral Dissertation, University of Salford, Salford, UK, 2020.
- Dos’Santos, T.; McBurnie, A.; Comfort, P.; Jones, P.A. The Effects of Six-Weeks Change of Direction Speed and Technique Modification Training on Cutting Performance and Movement Quality in Male Youth Soccer Players. Sports 2019, 7, 205.
- Dowling, A.V.; Corazza, S.; Chaudhari, A.M.; Andriacchi, T.P. Shoe-surface friction influences movement strategies during a sidestep cutting task: Implications for anterior cruciate ligament injury risk. Am. J. Sports Med. 2010, 38, 478–485.
- Dowling, A.V.; Andriacchi, T.P. Role of Shoe–Surface Interaction and Noncontact ACL Injuries. In ACL Injuries in the Female Athlete; Springer: Berlin/Heidelberg, Germany, 2012; pp. 85–108.
- Pedroza, A.; Fernandez, S.; Heidt, J.R.; Kaeding, C. Evaluation of the shoe-surface interaction using an agility maneuver. Med. Sci. Sports Exerc. 2010, 42, 1754–1759.
- Andrews, J.R.; McLeod, W.D.; Ward, T.; Howard, K. The cutting mechanism. Am. J. Sports Med. 1977, 5, 111–121.
- Dos’ Santos, T.; Thomas, C.; Comfort, P.; Jones, P.A. The Role of the Penultimate Foot Contact During Change of Direction: Implications on Performance and Risk of Injury. Strength Cond. J. 2019, 41, 87–104.
- Graham-Smith, P.; Rumpf, M.; Jones, P.A. Assessment of Deceleration Ability and Relationship to Approach Speed and Eccentric Strength. ISBS Proc. Arch. 2018, 36, 8.
- Grassi, A.; Smiley, S.P.; Roberti di Sarsina, T.; Signorelli, C.; Marcheggiani Muccioli, G.M.; Bondi, A.; Romagnoli, M.; Agostini, A.; Zaffagnini, S. Mechanisms and situations of anterior cruciate ligament injuries in professional male soccer players: A YouTube-based video analysis. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 697–981.
- Havens, K.L.; Sigward, S.M. Whole body mechanics differ among running and cutting maneuvers in skilled athletes. Gait Posture 2014, 42, 240–245.
- Inaba, Y.; Yoshioka, S.; Iida, Y.; Hay, D.C.; Fukashiro, S. A biomechanical study of side steps at different distances. J. Appl. Biomech. 2013, 29, 336–345.
- Golden, G.M.; Pavol, M.J.; Hoffman, M.A. Knee joint kinematics and kinetics during a lateral false-step maneuver. J. Athl. Train. 2009, 44, 503–510.
- McLean, S.G.; Lipfert, S.W.; Van den Bogert, A.J. Effect of gender and defensive opponent on the biomechanics of sidestep cutting. Med. Sci. Sports Exerc. 2004, 36, 1008–1016.
- Nyland, J.; Caborn, D.N.M.; Shapiro, R.; Johnson, D.L.; Fang, H. Hamstring extensibility and transverse plane knee control relationship in athletic women. Knee Surg. Sports Traumatol. Arthrosc. 1999, 7, 257–261.
- Loudon, J.K.; Jenkins, W.; Loudon, K.L. The relationship between static posture and ACL injury in female athletes. J. Orthop. Sport Phys. 1996, 24, 91–97.
- Ford, K.R.; Myer, G.D.; Toms, H.E.; Hewett, T.E. Gender differences in the kinematics of unanticipated cutting in young athletes. Med. Sci. Sports Exerc. 2005, 37, 124–129.
- Dempster, W.T. Space Requirements of the Seated Operator: Geometrical, Kinematic, and Mechanical Aspects of the Body, with Special Reference to the Limbs. Michigan State Univ East Lansing. 1955. Available online: (accessed on 6 April 2021).
- Mendiguchia, J.; Ford, K.R.; Quatman, C.E.; Alentorn-Geli, E.; Hewett, T.E. Sex differences in proximal control of the knee joint. Sports Med. 2011, 41, 541–557.
- Hewett, T.E.; Myer, G.D. The mechanistic connection between the trunk, knee, and anterior cruciate ligament injury. Exerc. Sport Sci. Rev. 2011, 39, 161.
- Zazulak, B.T.; Hewett, T.E.; Reeves, N.P.; Goldberg, B.; Cholewicki, J. The effects of core proprioception on knee injury: A prospective biomechanical-epidemiological study. Am. J. Sports Med. 2007, 35, 368–373.
- Zazulak, B.T.; Hewett, T.E.; Reeves, N.P.; Goldberg, B.; Cholewicki, J. Deficits in Neuromuscular Control of the Trunk Predict Knee Injury Risk: Prospective Biomechanical-Epidemiologic Study. Am. J. Sports Med. 2007, 35, 1123–1130.
- Marshall, B.M.; Franklyn-Miller, A.D.; King, E.A.; Moran, K.A.; Strike, S.; Falvey, A. Biomechanical factors associated with time to complete a change of direction cutting maneuver. J. Strength Cond. Res. 2014, 28, 2845–2851.
- David, S.; Mundt, M.; Komnik, I.; Potthast, W. Understanding cutting maneuvers–The mechanical consequence of preparatory strategies and foot strike pattern. Hum. Mov. Sci. 2018, 62, 202–210.
- Sheehan, F.T.; Sipprell Iii, W.H.; Boden, B.P. Dynamic sagittal plane trunk control during anterior cruciate ligament injury. Am. J. Sports Med. 2012, 40, 1068–1074.
- Shimokochi, Y.; Ambegaonkar, J.P.; Meyer, E.G.; Lee, S.Y.; Shultz, S.J. Changing sagittal plane body position during single-leg landings influences the risk of non-contact anterior cruciate ligament injury. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 888–897.
- Yu, B.; Lin, C.-F.; Garrett, W.E. Lower extremity biomechanics during the landing of a stop-jump task. Clin. Biomech. 2006, 21, 297–305.
- Sigward, S.M.; Pollard, C.D. Proximal Risk Factors for ACL Injury: Role of the Hip Joint and Musculature. In ACL Injuries in the Female Athlete; Springer: Berlin/Heidelberg, Germany, 2018; pp. 207–223.
- Pollard, C.D.; Sigward, S.M.; Powers, C.M. Limited hip and knee flexion during landing is associated with increased frontal plane knee motion and moments. Clin. Biomech. 2010, 25, 142–146.
- Yeow, C.H.; Lee, P.V.S.; Goh, J.C.H. Non-linear flexion relationships of the knee with the hip and ankle, and their relative postures during landing. Knee 2011, 18, 323–328.
- Nguyen, A.-D.; Taylor, J.B.; Wimbish, T.G.; Keith, J.L.; Ford, K.R. Preferred Hip Strategy During Landing Reduces Knee Abduction Moment in Collegiate Female Soccer Players. J. Sport Rehabil. 2018, 27, 213–217.
- Powers, C.M. The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J. Orthop. Sport Phys. 2010, 40, 42–51.
- Markolf, K.L.; Gorek, J.F.; Kabo, J.M.; Shapiro, M.S. Direct measurement of resultant forces in the anterior cruciate ligament. An in vitro study performed with a new experimental technique. J. Bone Jt. Surg. Am. 1990, 72, 557–567.
- Withrow, T.J.; Huston, L.J.; Wojtys, E.M.; Ashton-Miller, J.A. The relationship between quadriceps muscle force, knee flexion, and anterior cruciate ligament strain in an in vitro simulated jump landing. Am. J. Sports Med. 2006, 34, 269–274.
- Beynnon, B.D.; Fleming, B.C.; Johnson, R.J.; Nichols, C.E.; Renström, P.A.; Pope, M.H. Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am. J. Sports Med. 1995, 23, 24–34.
- Beynnon, B.; Howe, J.; Pope, M.H.; Johnson, R.J.; Fleming, B. The measurement of anterior cruciate ligament strain in vivo. Int. Orthop. 1992, 16, 1–12.
- Leppänen, M.; Pasanen, K.; Kujala, U.M.; Vasankari, T.; Kannus, P.; Äyrämö, S.; Krosshaug, T.; Bahr, R.; Avela, J.; Perttunen, J. Stiff landings are associated with increased ACL injury risk in young female basketball and floorball players. Am. J. Sports Med. 2017, 45, 386–393.
- Devita, P.; Skelly, W.A. Effect of landing stiffness on joint kinetics and energetics in the lower extremity. Med. Sci. Sports Exerc. 1992, 24, 108–115.
- Zhang, S.-N.; Bates, B.T.; Dufek, J.S. Contributions of lower extremity joints to energy dissipation during landings. Med. Sci. Sports Exerc. 2000, 32, 812–819.
- Donnelly, C.J.; Chinnasee, C.; Weir, G.; Sasimontonkul, S.; Alderson, J. Joint dynamics of rear-and fore-foot unplanned sidestepping. J. Sci. Med. Sport 2017, 20, 32–37.
- Cortes, N.; Morrison, S.; Van Lunen, B.L.; Onate, J.A. Landing technique affects knee loading and position during athletic tasks. J. Sci. Med. Sport 2012, 15, 175–181.
- David, S.; Komnik, I.; Peters, M.; Funken, J.; Potthast, W. Identification and risk estimation of movement strategies during cutting maneuvers. J. Sci. Med. Sport 2017, 20, 1075–1080.
- Yoshida, N.; Kunugi, S.; Mashimo, S.; Okuma, Y.; Masunari, A.; Miyazaki, S.; Hisajima, T.; Miyakawa, S. Effect of forefoot strike on lower extremity muscle activity and knee joint angle during cutting in female team handball players. Sports Med. Open 2016, 2, 32.
- Burkhart, B.; Ford, K.R.; Myer, G.D.; Heidt, R.S., Jr.; Hewett, T.E. Anterior cruciate ligament tear in an athlete: Does increased heel loading contribute to ACL rupture? N. Am. J. Sports Phys. Ther. NAJSPT 2008, 3, 141–144.
- Hewit, J.; Cronin, J.; Button, C.; Hume, P. Understanding deceleration in sport. Strength Cond. J. 2011, 33, 47–52.
- O’Connor, J.J. Can muscle co-contraction protect knee ligaments after injury or repair? J. Bone Jt. Surg. Am. 1993, 75, 41–48.
- Fleming, B.C.; Renstrom, P.A.; Ohlen, G.; Johnson, R.J.; Peura, G.D.; Beynnon, B.D.; Badger, G.J. The gastrocnemius muscle is an antagonist of the anterior cruciate ligament. J. Orthop. Res. 2001, 19, 1178–1184.
- Adouni, M.; Shirazi-Adl, A.; Marouane, H. Role of gastrocnemius activation in knee joint biomechanics: Gastrocnemius acts as an ACL antagonist. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 376–385.
- Hewett, T.E. Response to: ‘Why screening tests to predict injury do not work -and probably never will…: A critical review’. Br. J. Sports Med. 2016, 50, 1353.
- Benjaminse, A.; Gokeler, A.; Dowling, A.V.; Faigenbaum, A.; Ford, K.R.; Hewett, T.E.; Onate, J.A.; Otten, B.; Myer, G.D. Optimization of the anterior cruciate ligament injury prevention paradigm: Novel feedback techniques to enhance motor learning and reduce injury risk. J. Orthop. Sport Phys. 2015, 45, 170–182.
- Herrington, L.C.; Comfort, P. Training for prevention of ACL injury: Incorporation of progressive landing skill challenges into a program. Strength Cond. J. 2013, 35, 59–65.


