 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Nicolas Papalexis | -- | 3128 | 2023-07-31 17:53:05 | | | |
| 2 | Lindsay Dong | Meta information modification | 3128 | 2023-08-01 02:54:22 | | |
Video Upload Options
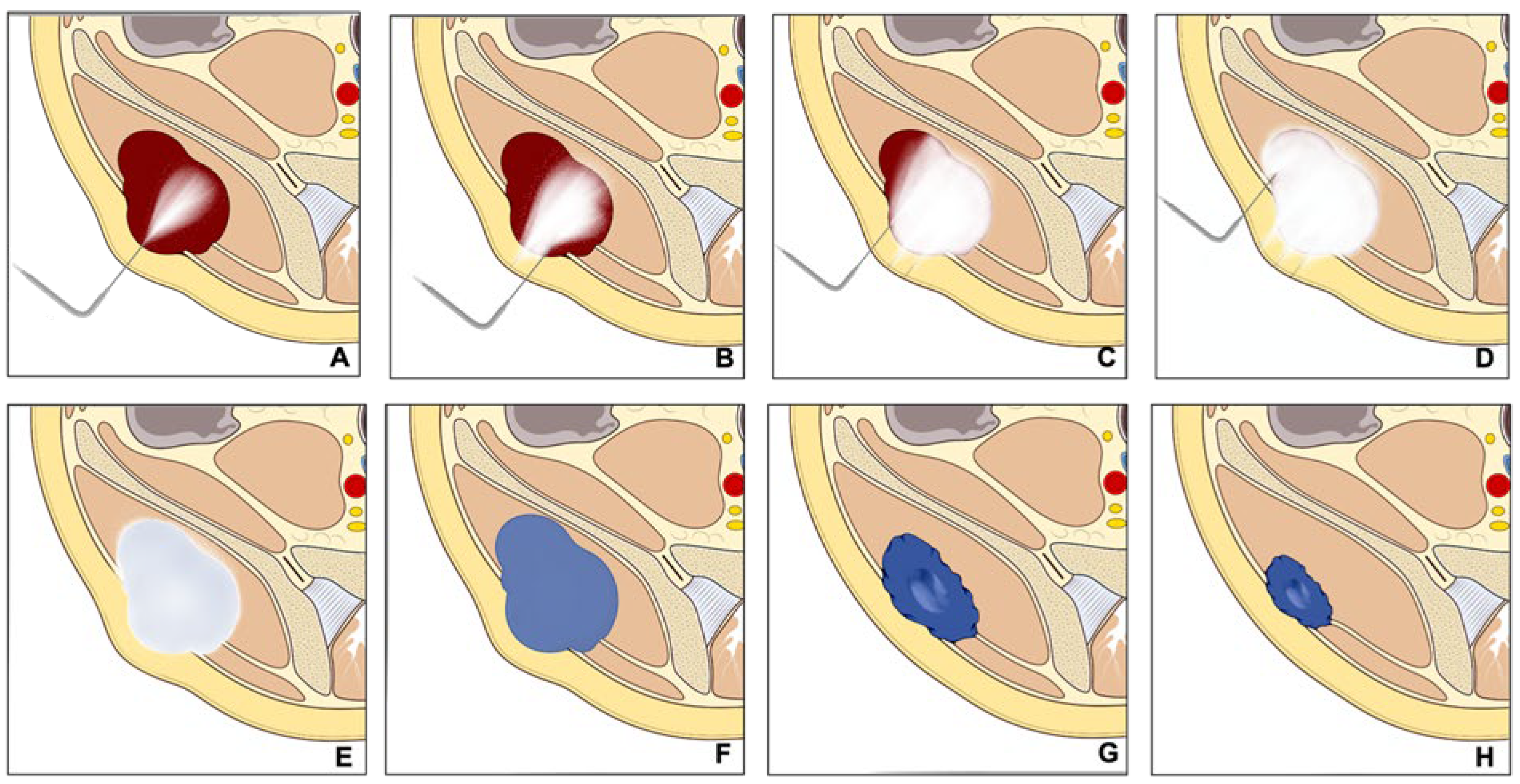
In the rapidly evolving field of interventional oncology, minimally invasive methods, including CT-guided cryoablation, play an increasingly important role in tumor treatment, notably in bone and soft tissue cancers. Cryoablation works using compressed gas-filled probes to freeze tumor cells to temperatures below −20 °C, exploiting the Joule–Thompson effect. This cooling causes cell destruction by forming intracellular ice crystals and disrupting blood flow through endothelial cell damage, leading to local ischemia and devascularization. Coupling this with CT technology enables precise tumor targeting, preserving healthy surrounding tissues and decreasing postoperative complications.
1. Introduction
2. Malignant Bone and Soft Tissue Tumors
Percutaneous cryoablation is becoming an increasingly accepted option within the multidisciplinary sarcoma board for the treatment of primary bone and soft tissue tumors, applicable for selected cases. Despite surgical intervention being the mainstay for treating primary, non-metastatic bone, and soft tissue tumors, the local control of recurring bone and soft tissue sarcoma (STS) continues to be a challenging task. It mainly hinges on the disease prognosis as per the guidelines of the European Society for Medical Oncology (ESMO) [10][11]. Surgical resection is the common protocol for localized conditions, while chemotherapy or radiation therapy may be employed for more extensive diseases or recurrences [10][11][12]. Lately, minimally invasive techniques such as radiofrequency ablation, microwave ablation, or cryoablation have been proposed as potential surgical alternatives for some selected recurrent bone and soft tissue tumors [13][14][15][16][17].
Some initial studies evaluated the therapeutic effect of Cryoablation for the treatment of a variety of primary bone and soft tissue malignancies with promising results; however, the scientific evidence is still limited. Moreover, there is a recognized need for the standardization of selection criteria for percutaneous cryoablation. Lippa et al. [12] aimed to identify these criteria, finding high agreement for all proposed criteria between two readers. Eligibility for cryoablation was significantly associated with tumors located deeply, with great axes ≤ 5 cm, high local tumor aggressiveness, and a diagnosis of differentiated myxoid liposarcoma or myxofibrosarcoma.
2.1. Recurrent Retroperitoneal Soft Tissue Tumors
2.2. Sacrococcygeal Tumors and Chordoma
3. Bone Metastases
3.1. Pain Palliation and Disease Control
3.2. Application to Spinal Metastases
3.3. Application to Sternal Metastases
3.4. Evaluation of Post-Ablation Area
3.5. Technical Consideration for Neuroprotection
3.6. Technical Consideration for Bone Reinforcement
3.7. Combination Treatment
3.8. Complications
4. Benign Bone Tumors
4.1. Osteoid Osteoma
4.2. Osteoblastoma
4.3. Bone Cyst and Aneurysmal Bone Cyst
5. Desmoid Tumors
5.1. Cryoablation for Disease Control
5.2. Ablation Margin
5.3. Pain Reduction
5.4. Patient Selection
6. Technical Consideration
6.1. Planning and Approach
6.2. Needle Placement and Hydro Dissection
6.3. Ablation and Monitoring
7. Conclusions
References
- Foster, R.C.; Stavas, J.M. Bone and Soft Tissue Ablation. Semin. Interv. Radiol. 2014, 31, 167–179.
- Kurup, A.N.; Callstrom, M.R. Ablation of Musculoskeletal Metastases: Pain Palliation, Fracture Risk Reduction, and Oligometastatic Disease. Tech. Vasc. Interv. Radiol. 2013, 16, 253–261.
- Garnon, J.; Koch, G.; Caudrelier, J.; Tsoumakidou, G.; Cazzato, R.; Gangi, A. Expanding the borders: Image-guided procedures for the treatment of musculoskeletal tumors. Diagn. Interv. Imaging 2017, 98, 635–644.
- Mahnken, A.H.; König, A.M.; Figiel, J.H. Current Technique and Application of Percutaneous Cryotherapy. In RöFo-Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgebenden Verfahren; Georg Thieme Verlag KG: Stuttgart, Germany, 2018; Volume 190, pp. 836–846.
- Cazzato, R.L.; Gantzer, J.; de Marini, P.; Garnon, J.; Koch, G.; Buy, X.; Autrusseau, P.-A.; Auloge, P.; Dalili, D.; Kurtz, J.-E.; et al. Sporadic Desmoid Tumours: Systematic Review with Reflection on the Role of Cryoablation. Cardiovasc. Interv. Radiol. 2022, 45, 613–621.
- Cazzato, R.L.; Garnon, J.; Koch, G.; Dalili, D.; Rao, P.P.; Weiss, J.; Bauones, S.; Auloge, P.; De Marini, P.; Gangi, A. Musculoskeletal interventional oncology: Current and future practices. Br. J. Radiol. 2020, 93, 20200465.
- Baust, J.M.; Santucci, K.L.; Van Buskirk, R.G.; Raijman, I.; Fisher, W.E.; Baust, J.G.; Snyder, K.K. An In Vitro Investigation into Cryoablation and Adjunctive Cryoablation/Chemotherapy Combination Therapy for the Treatment of Pancreatic Cancer Using the PANC-1 Cell Line. Biomedicines 2022, 10, 450.
- Hayek, G.; Kastler, B. Interventional radiology for treatment of bone metastases. Cancer Radiother. 2020, 24, 374–378.
- Chu, K.F.; Dupuy, D.E. Thermal ablation of tumours: Biological mechanisms and advances in therapy. Nat. Rev. Cancer 2014, 14, 199–208.
- The ESMO/European Sarcoma Network Working Group. Soft tissue and visceral sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii102–iii112.
- Casali, P.G.; Blay, J.-Y.; ESMO/CONTICANET/EUROBONET Consensus Panel of Experts. Soft tissue sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v198–v203.
- Lippa, N.; Sargos, P.; Italiano, A.; Kind, M.; Dallaudière, B.; Hauger, O.; Cornelis, F. Standardization of selection criteria for percutaneous image-guided cryoablation of recurrent soft-tissue sarcomas. Diagn. Interv. Imaging 2014, 95, 1071–1077.
- Dalili, D.; Isaac, A.; Cazzato, R.L.; Åström, G.; Bergh, J.; Mansour, R.; Weber, M.-A.; Garnon, J.; Gangi, A. Interventional Techniques for Bone and Musculoskeletal Soft Tissue Tumors: Current Practices and Future Directions—Part II. Stabilization. Semin. Musculoskelet. Radiol. 2020, 24, 710–725.
- Gronchi, A.; Guadagnolo, B.A.; Erinjeri, J.P. Local Ablative Therapies to Metastatic Soft Tissue Sarcoma. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e566–e575.
- de Baere, T.; Tselikas, L.; Gravel, G.; Hakime, A.; Deschamps, F.; Honoré, C.; Mir, O.; Lecesne, A. Interventional radiology: Role in the treatment of sarcomas. Eur. J. Cancer 2018, 94, 148–155.
- Lim, C.T.; Tan, L.B.K.; Nathan, S.S. Prospective evaluation of argon gas probe delivery for cryotherapy of bone tumours. Ann. Acad. Med. Singap. 2012, 41, 347–353.
- Ahlmann, E.R.; Falkinstein, Y.; Fedenko, A.N.; Menendez, L.R. Cryoablation and resection influences patient survival for soft tissue sarcomas: Impact on survivorship and local recurrence. Clin. Orthop. Relat. Res. 2007, 459, 174–181.
- Fan, W.; Niu, L.; Wang, Y.; Zhang, Y.; Yao, X.; Tan, G.; Yang, J.; Li, J. Percutaneous computed tomography-guided cryoablation for recurrent retroperitoneal soft tissue sarcoma: A study of safety and efficacy. Oncotarget 2016, 7, 42639–42649.
- Mendenhall, W.M.; Zlotecki, R.A.; Hochwald, S.N.; Hemming, A.W.; Grobmyer, S.R.; Cance, W.G. Retroperitoneal soft tissue sarcoma. Cancer 2005, 104, 669–675.
- Kurup, A.N.; Woodrum, D.A.; Morris, J.M.; Atwell, T.D.; Schmit, G.D.; Welch, T.J.; Yaszemski, M.J.; Callstrom, M.R. Cryoablation of Recurrent Sacrococcygeal Tumors. J. Vasc. Interv. Radiol. 2012, 23, 1070–1075.
- Susa, M.; Kikuta, K.; Nakayama, R.; Nishimoto, K.; Horiuchi, K.; Oguro, S.; Inoue, M.; Yashiro, H.; Nakatsuka, S.; Nakamura, M.; et al. CT guided cryoablation for locally recurrent or metastatic bone and soft tissue tumor: Initial experience. BMC Cancer 2016, 16, 798.
- Errani, C.; Bazzocchi, A.; Spinnato, P.; Facchini, G.; Campanacci, L.; Rossi, G.; Mavrogenis, A.F. What’s new in management of bone metastases? Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1367–1375.
- Papalexis, N.; Parmeggiani, A.; Peta, G.; Spinnato, P.; Miceli, M.; Facchini, G. Minimally Invasive Interventional Procedures for Metastatic Bone Disease: A Comprehensive Review. Curr. Oncol. 2022, 29, 4155–4177.
- Hong, S.; Youk, T.; Lee, S.J.; Kim, K.M.; Vajdic, C.M. Bone metastasis and skeletal-related events in patients with solid cancer: A Korean nationwide health insurance database study. PLoS ONE 2020, 15, e0234927.
- Cazzato, R.L.; Auloge, P.; De Marini, P.; Boatta, E.; Koch, G.; Dalili, D.; Rao, P.P.; Garnon, J.; Gangi, A. Spinal Tumor Ablation: Indications, Techniques, and Clinical Management. Tech. Vasc. Interv. Radiol. 2020, 23, 100677.
- Gallusser, N.; Goetti, P.; Becce, F.; Vauclair, F.; Rüdiger, H.A.; Bize, P.E.; Cherix, S. Percutaneous image-guided cryoablation of painful bone metastases: A single institution experience. Orthop. Traumatol. Surg. Res. 2019, 105, 369–374.
- Gardner, C.S.; Ensor, J.E.; Ahrar, K.; Huang, S.Y.; Sabir, S.H.; Tannir, N.M.; Lewis, V.O.; Tam, A.L. Cryoablation of Bone Metastases from Renal Cell Carcinoma for Local Tumor Control. J. Bone Jt. Surg. 2017, 99, 1916–1926.
- McArthur, T.A.; Narducci, C.A.; Lander, P.H.; Lopez-Ben, R. Percutane Image-Guided Cryoablation of Painful Osseous Metastases: A Retrospective Single-Center Review. Curr. Probl. Diagn. Radiol. 2017, 46, 282–287.
- Di Staso, M.; Gravina, G.L.; Zugaro, L.; Bonfili, P.; Gregori, L.; Franzese, P.; Marampon, F.; Vittorini, F.; Moro, R.; Tombolini, V.; et al. Treatment of Solitary Painful Osseous Metastases with Radiotherapy, Cryoablation or Combined Therapy: Propensity Matching Analysis in 175 Patients. PLoS ONE 2015, 10, e0129021.
- Thacker, P.G.; Callstrom, M.R.; Curry, T.B.; Mandrekar, J.N.; Atwell, T.D.; Goetz, M.P.; Rubin, J. Palliation of Painful Metastatic Disease Involving Bone with Imaging-Guided Treatment: Comparison of Patients’ Immediate Response to Radiofrequency Ablation and Cryoablation. Am. J. Roentgenol. 2011, 197, 510–515.
- Munk, P.L.; Murphy, K.J.; Gangi, A.; Liu, D.M. Fire and Ice: Percutaneous Ablative Therapies and Cement Injection in Management of Metastatic Disease of the Spine. Semin. Musculoskelet. Radiol. 2011, 15, 125–134.
- Mercadante, S.; Klepstad, P.; Kurita, G.P.; Sjøgren, P.; Pigni, A.; Caraceni, A. Minimally invasive procedures for the management of vertebral bone pain due to cancer: The EAPC recommendations. Acta Oncol. 2015, 55, 129–133.
- Liu, H.; Song, C.; Zhang, B.; Luo, R.; Yang, J. Research trends and areas of focus on cryoablation and oncology: A bibliometric analysis from 2001 to 2020. Medicine 2022, 101, e32513.
- Wallace, A.N.; McWilliams, S.R.; Connolly, S.E.; Symanski, J.S.; Vaswani, D.; Tomasian, A.; Vyhmeister, R.; Lee, A.M.; Madaelil, T.P.; Hillen, T.J. Percutaneous Image-Guided Cryoablation of Musculoskeletal Metastases: Pain Palliation and Local Tumor Control. J. Vasc. Interv. Radiol. 2016, 27, 1788–1796.
- McMenomy, B.P.; Kurup, A.N.; Johnson, G.B.; Carter, R.E.; McWilliams, R.R.; Markovic, S.N.; Atwell, T.D.; Schmit, G.D.; Morris, J.M.; Woodrum, D.A.; et al. Percutaneous Cryoablation of Musculoskeletal Oligometastatic Disease for Complete Remission. J. Vasc. Interv. Radiol. 2013, 24, 207–213.
- Ma, Y.; Wallace, A.N.; Waqar, S.N.; Morgensztern, D.; Madaelil, T.P.; Tomasian, A.; Jennings, J.W. Percutaneous Image-Guided Ablation in the Treatment of Osseous Metastases from Non-small Cell Lung Cancer. Cardiovasc. Interv. Radiol. 2017, 41, 726–733.
- Yang, Y.; Li, Y.; Wu, Y.; Qiu, S.; Liu, C.; Wang, Q.; Hong, Y.; Lyu, J.; Zhang, Y.; Du, D. Retrospective analysis of CT-guided percutaneous cryoablation for treatment of painful osteolytic bone metastasis. Cryobiology 2020, 92, 203–207.
- Prologo, J.D.; Passalacqua, M.; Patel, I.; Bohnert, N.; Corn, D. Image-guided cryoablation for the treatment of painful musculoskeletal metastatic disease: A single-center experience. Skelet. Radiol. 2014, 43, 1551–1559.
- Jennings, J.W.; Prologo, J.D.; Garnon, J.; Gangi, A.; Buy, X.; Palussière, J.; Kurup, A.N.; Callstrom, M.; Genshaft, S.; Abtin, F. Cryoablation for Palliation of Painful Bone Metastases: The MOTION Multicenter Study. Radiol. Imaging Cancer 2021, 3, e200101.
- Callstrom, M.R.; Atwell, T.D.; Charboneau, J.W.; Farrell, M.A.; Goetz, M.P.; Rubin, J.; Sloan, J.A.; Novotny, P.J.; Welch, T.J.; Maus, T.P.; et al. Painful Metastases Involving Bone: Percutaneous Image-guided Cryoablation—Prospective Trial Interim Analysis. Radiology 2006, 241, 572–580.
- De Marini, P.; Cazzato, R.L.; Auloge, P.; Koch, G.; Dalili, D.; Garnon, J.; Gangi, A. Percutaneous image-guided thermal ablation of bone metastases: A retrospective propensity study comparing the safety profile of radio-frequency ablation and cryo-ablation. Int. J. Hyperth. 2020, 37, 1386–1394.
- Grönemeyer, D.H.W.; Schirp, S.; Gevargez, A. Image-guided radiofrequency ablation of spinal tumors: Preliminary experience with an expandable array electrode. Cancer J. 2002, 8, 33–39.
- Levy, J.; Hopkins, T.; Morris, J.; Tran, N.D.; David, E.; Massari, F.; Farid, H.; Vogel, A.; O’connell, W.G.; Sunenshine, P.; et al. Radiofrequency Ablation for the Palliative Treatment of Bone Metastases: Outcomes from the Multicenter OsteoCool Tumor Ablation Post-Market Study (OPuS One Study) in 100 Patients. J. Vasc. Interv. Radiol. 2020, 31, 1745–1752.
- Autrusseau, P.-A.; Cazzato, R.; De Marini, P.; Auloge, P.; Koch, G.; Dalili, D.; Weiss, J.; Mayer, T.; Garnon, J.; Gangi, A. Pain relief and local tumour control following percutaneous image-guided cryoablation for spine metastasis: A 12-year single-centre experience. Clin. Radiol. 2021, 76, 674–680.
- Hegg, R.M.; Kurup, A.N.; Schmit, G.D.; Weisbrod, A.J.; Atwell, T.D.; Olivier, K.R.; Moynihan, T.J.; Callstrom, M.R. Cryoablation of Sternal Metastases for Pain Palliation and Local Tumor Control. J. Vasc. Interv. Radiol. 2014, 25, 1665–1670.
- Gravel, G.; Tselikas, L.; Moulin, B.; Yevich, S.; Baudin, E.; Hakime, A.; Moalla, S.; Mihoubi, F.; Balleyguier, C.; de Baere, T.; et al. Early detection with MRI of incomplete treatment of spine metastases after percutaneous cryoablation. Eur. Radiol. 2019, 29, 5655–5663.
- Kurup, A.N.; Morris, J.M.; Boon, A.J.; Strommen, J.A.; Schmit, G.D.; Atwell, T.D.; Carter, R.E.; Brown, M.J.; Wass, C.T.; Rose, P.S.; et al. Motor Evoked Potential Monitoring during Cryoablation of Musculoskeletal Tumors. J. Vasc. Interv. Radiol. 2014, 25, 1657–1664.
- Prologo, J.D.; Patel, I.; Buethe, J.; Bohnert, N. Ablation Zones and Weight-Bearing Bones: Points of Caution for the Palliative Interventionalist. J. Vasc. Interv. Radiol. 2014, 25, 769–775.e2.
- Masala, S.; Chiocchi, M.; Taglieri, A.; Bindi, A.; Nezzo, M.; De Vivo, D.; Simonetti, G. Combined use of percutaneous cryoablation and vertebroplasty with 3D rotational angiograph in treatment of single vertebral metastasis: Comparison with vertebroplasty. Neuroradiology 2012, 55, 193–200.
- Sundararajan, S.H.; Calamita, S.; Girgis, P.; Ngo, G.; Ranganathan, S.; Giglio, M.; Gendel, V.; Goyal, S.; Nosher, J.; Roychowdhury, S. Sequential Interventional Management of Osseous Neoplasms via Embolization, Cryoablation, and Osteoplasty. J. Oncol. 2019, 2019, 5247837.
- Auloge, P.; Cazzato, R.L.; Rousseau, C.; Caudrelier, J.; Koch, G.; Rao, P.; Chiang, J.B.; Garnon, J.; Gangi, A. Complications of Percutaneous Bone Tumor Cryoablation: A 10-year Experience. Radiology 2019, 291, 521–528.
- Bazzocchi, A.; Gómez, M.P.A.; Tomassoni, M.T.; Napoli, A.; Filippiadis, D.; Guglielmi, G. Musculoskeletal oncology and thermal ablation: The current and emerging role of interventional radiology. Skelet. Radiol. 2022, 52, 447–459.
- Tepelenis, K.; Skandalakis, G.P.; Papathanakos, G.; Kefala, M.A.; Kitsouli, A.; Barbouti, A.; Tepelenis, N.; Varvarousis, D.; Vlachos, K.; Kanavaros, P.; et al. Osteoid Osteoma: An Updated Review of Epidemiology, Pathogenesis, Clinical Presentation, Radiological Features, and Treatment Option. In Vivo 2021, 35, 1929–1938.
- Wu, B.; Xiao, Y.-Y.; Zhang, X.; Zhao, L.; Carrino, J.A. CT-guided percutaneous cryoablation of osteoid osteoma in children: An initial study. Skelet. Radiol. 2011, 40, 1303–1310.
- Shanmugasundaram, S.; Nadkarni, S.; Kumar, A.; Shukla, P.A. Percutaneous Ablative Therapies for the Management of Osteoid Osteomas: A Systematic Review and Meta-Analysis. Cardiovasc. Interv. Radiol. 2021, 44, 739–749.
- Parmeggiani, A.; Martella, C.; Ceccarelli, L.; Miceli, M.; Spinnato, P.; Facchini, G. Osteoid osteoma: Which is the best mininvasive treatment option? Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1611–1624.
- Parvinian, A.; Welch, B.T.; Callstrom, M.R.; Kurup, A.N. Trends in Musculoskeletal Ablation: Emerging Indications and Techniques. Tech. Vasc. Interv. Radiol. 2020, 23, 100678.
- Izzo, A.; Zugaro, L.; Fascetti, E.; Bruno, F.; Zoccali, C.; Arrigoni, F. Management of Osteoblastoma and Giant Osteoid Osteoma with Percutaneous Thermoablation Techniques. J. Clin. Med. 2021, 10, 5717.
- Meng, L.; Zhang, X.; Xu, R.; Wu, B.; Wei, Y.; Li, J.; Shan, H.; Xiao, Y. A preliminary comparative study of percutaneous CT-guided cryoablation with surgical resection for osteoid osteoma. PeerJ 2021, 9, e10724.
- Cazzato, R.L.; Auloge, P.; Dalili, D.; DE Marini, P.; Di Marco, A.; Garnon, J.; Gangi, A. Percutaneous Image-Guided Cryoablation of Osteoblastoma. Am. J. Roentgenol. 2019, 213, 1157–1162.
- Lokiec, F.; Wientroub, S. Simple bone cyst: Etiology, classification, pathology, and treatment modalities. J. Pediatr. Orthop. B 1998, 7, 262–273.
- Walczak, B.E.; Rose, P.S. Desmoid: The Role of Local Therapy in an Era of Systemic Options. Curr. Treat. Options Oncol. 2013, 14, 465–473.
- Kurtz, J.-E.; Buy, X.; Deschamps, F.; Sauleau, E.; Bouhamama, A.; Toulmonde, M.; Honoré, C.; Bertucci, F.; Brahmi, M.; Chevreau, C.; et al. CRYODESMO-O1: A prospective, open phase II study of cryoablation in desmoid tumour patients progressing after medical treatment. Eur. J. Cancer 2020, 143, 78–87.
- Kasper, B.; Baumgarten, C.; Garcia, J.; Bonvalot, S.; Haas, R.; Haller, F.; Hohenberger, P.; Penel, N.; Messiou, C.; van Der Graaf, W.T.; et al. An update on the management of sporadic desmoid-type fibromatosis: A European Consensus Initiative between Sarcoma PAtients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann. Oncol. 2017, 28, 2399–2408.
- Yan, Y.Y.; Walsh, J.P.; Munk, P.L.; Mallinson, P.I.; Simmons, C.; Clarkson, P.W.; Jayaram, P.R.; Heran, M.K.; Ouellette, H.A. A Single-Center 10-Year Retrospective Analysis of Cryoablation for the Management of Desmoid Tumors. J. Vasc. Interv. Radiol. 2021, 32, 1277–1287.
- Errani, C.; Mavrogenis, A.F.; Tsukamoto, S. What’s new in musculoskeletal oncology. BMC Musculoskelet. Disord. 2021, 22, 704.
- Zhou, M.Y.; Bui, N.Q.; Charville, G.W.; Ghanouni, P.; Ganjoo, K.N. Current management and recent progress in desmoid tumors. Cancer Treat. Res. Commun. 2022, 31, 100562.
- Havez, M.; Lippa, N.; Al-Ammari, S.; Kind, M.; Stoeckle, E.; Italiano, A.; Gangi, A.; Hauger, O.; Cornelis, F. Percutaneous Image-Guided Cryoablation in Inoperable Extra-abdominal Desmoid Tumors: A Study of Tolerability and Efficacy. Cardiovasc. Interv. Radiol. 2014, 37, 1500–1506.
- Saltiel, S.; Bize, P.E.; Goetti, P.; Gallusser, N.; Cherix, S.; Denys, A.; Becce, F.; Tsoumakidou, G. Cryoablation of Extra-Abdominal Desmoid Tumors: A Single-Center Experience with Literature Review. Diagnostics 2020, 10, 556.
- Mandel, J.E.; Kim, D.; Yarmohammadi, H.; Ziv, E.; Keohan, M.L.; D’angelo, S.P.; Gounder, M.M.; Whiting, K.; Qin, L.-X.; Singer, S.; et al. Percutaneous Cryoablation Provides Disease Control for Extra-Abdominal Desmoid-Type Fibromatosis Comparable with Surgical Resection. Ann. Surg. Oncol. 2021, 29, 640–648.
- Bouhamama, A.; Lame, F.; Mastier, C.; Cuinet, M.; Thibaut, A.; Beji, H.; Ricoeur, A.; Blay, J.-Y.; Pilleul, F. Local Control and Analgesic Efficacy of Percutaneous Cryoablation for Desmoid Tumors. Cardiovasc. Interv. Radiol. 2019, 43, 110–119.
- Testa, S.; Bui, N.Q.; Charville, G.W.; Avedian, R.S.; Steffner, R.; Ghanouni, P.; Mohler, D.G.; Ganjoo, K.N. Management of Patients with Newly Diagnosed Desmoid Tumors in a First-Line Setting. Cancers 2022, 14, 3907.
- Ryan, A.; Byrne, C.; Pusceddu, C.; Buy, X.; Tsoumakidou, G.; Filippiadis, D. CIRSE Standards of Practice on Thermal Ablation of Bone Tumours. Cardiovasc. Interv. Radiol. 2022, 45, 591–605.
- Cornelis, F.; Havez, M.; Lippa, N.; Al-Ammari, S.; Verdier, D.; Carteret, T.; Amoretti, N.; Gangi, A.; Palussiere, J.; Hauger, O.; et al. Radiologically guided percutaneous cryotherapy for soft tissue tumours: A promising treatment. Diagn. Interv. Imaging 2013, 94, 364–370.
- Tacke, J.; Speetzen, R.; Heschel, I.; Hunter, D.W.; Rau, G.; Günther, R.W. Imaging of interstitial cryotherapy—An in vitro comparison of ultrasound, computed tomography, and magnetic resonance imaging. Cryobiology 1999, 38, 250–259.
- Autrusseau, P.-A.; Garnon, J.; Auloge, P.; Weiss, J.; Dalili, D.; Caudrelier, J.; Cazzato, R.L.; Koch, G.; Gangi, A. Hydrodissection of the Retro-Sternal Space to Protect the Pericardium During Sternal Cryoablation. Cardiovasc. Interv. Radiol. 2020, 43, 1371–1377.
- Castañeda Rodriguez, W.R.; Callstrom, M.R. Effective pain palliation and prevention of fracture for axial-loading skeletal metastases using combined cryoablation and cementoplasty. Tech. Vasc. Interv. Radiol. 2011, 14, 160–169.

