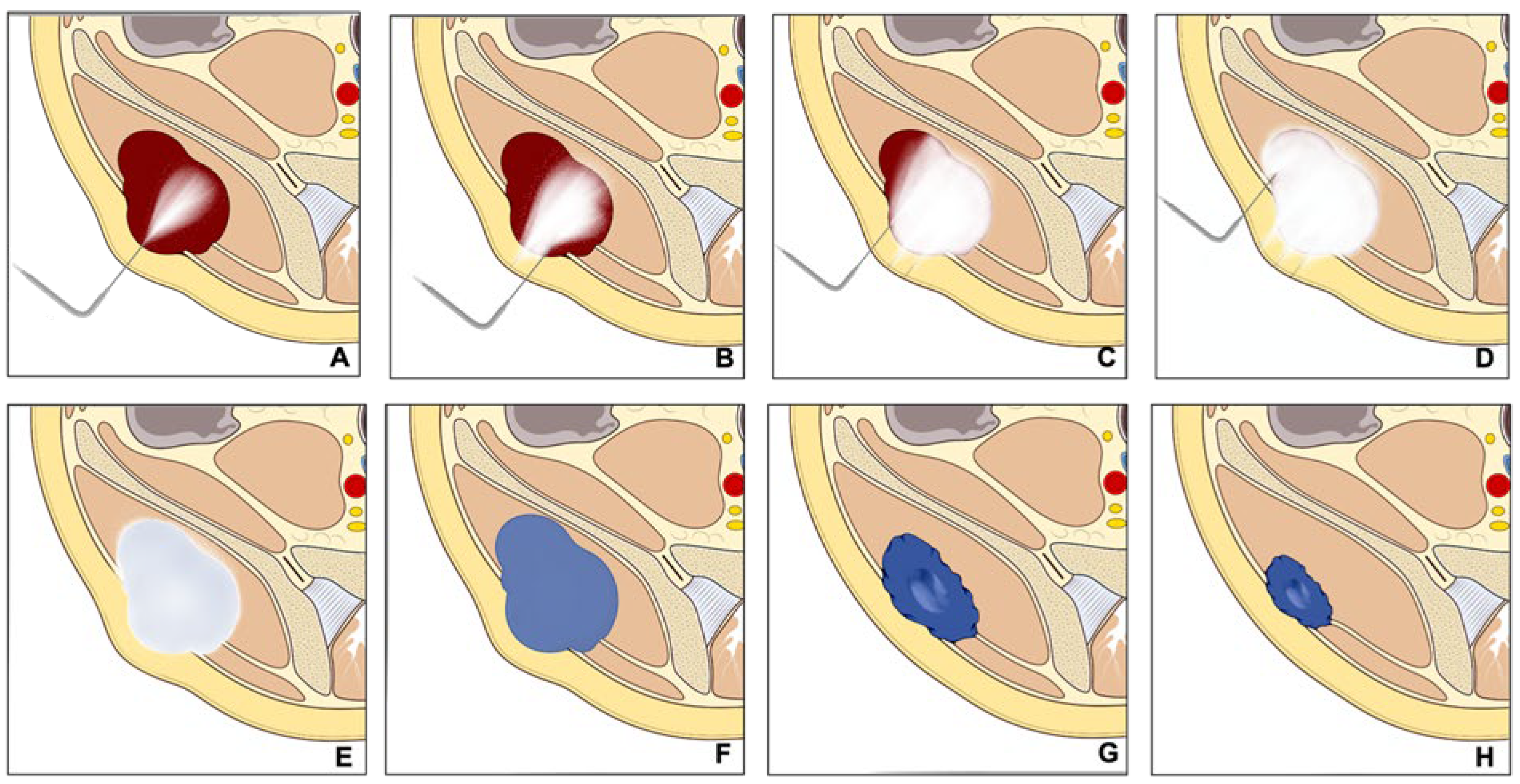
In the rapidly evolving field of interventional oncology, minimally invasive methods, including CT-guided cryoablation, play an increasingly important role in tumor treatment, notably in bone and soft tissue cancers. Cryoablation works using compressed gas-filled probes to freeze tumor cells to temperatures below −20 °C, exploiting the Joule–Thompson effect. This cooling causes cell destruction by forming intracellular ice crystals and disrupting blood flow through endothelial cell damage, leading to local ischemia and devascularization. Coupling this with CT technology enables precise tumor targeting, preserving healthy surrounding tissues and decreasing postoperative complications.
- interventional radiology
- metastatic neoplasms
- orthopedic surgery
- palliative medicine
- cryoablation
1. Introduction
2. Malignant Bone and Soft Tissue Tumors
Percutaneous cryoablation is becoming an increasingly accepted option within the multidisciplinary sarcoma board for the treatment of primary bone and soft tissue tumors, applicable for selected cases. Despite surgical intervention being the mainstay for treating primary, non-metastatic bone, and soft tissue tumors, the local control of recurring bone and soft tissue sarcoma (STS) continues to be a challenging task. It mainly hinges on the disease prognosis as per the guidelines of the European Society for Medical Oncology (ESMO) [10,11][10][11]. Surgical resection is the common protocol for localized conditions, while chemotherapy or radiation therapy may be employed for more extensive diseases or recurrences [10,11,12][10][11][12]. Lately, minimally invasive techniques such as radiofrequency ablation, microwave ablation, or cryoablation have been proposed as potential surgical alternatives for some selected recurrent bone and soft tissue tumors [13,14,15,16,17][13][14][15][16][17].
Some initial studies evaluated the therapeutic effect of Cryoablation for the treatment of a variety of primary bone and soft tissue malignancies with promising results; however, the scientific evidence is still limited. Moreover, there is a recognized need for the standardization of selection criteria for percutaneous cryoablation. Lippa et al. [12] aimed to identify these criteria, finding high agreement for all proposed criteria between two readers. Eligibility for cryoablation was significantly associated with tumors located deeply, with great axes ≤ 5 cm, high local tumor aggressiveness, and a diagnosis of differentiated myxoid liposarcoma or myxofibrosarcoma.
2.1. Recurrent Retroperitoneal Soft Tissue Tumors
2.2. Sacrococcygeal Tumors and Chordoma
3. Bone Metastases
3.1. Pain Palliation and Disease Control
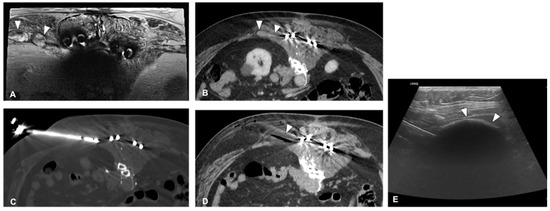
The clinical effect in pain reduction and safety of cryoablation for metastatic bone disease has been investigated by several studies in recent years [40,43,44,46,48][34][35][36][37][38] (Figure 3). A recent multicenter prospective study by Jennings et al. [38][39] assessed the clinical efficacy of cryoablation as a pain palliating method for patients with metastatic bone disease. The main goal was the pain score change from pre-treatment to the eighth-week follow-up, with participants monitored for 24 weeks post-treatment. A cohort of 66 participants (average age 60.8 years, 53% male) was recruited and underwent percutaneous cryoablation; 65 completed the follow-up. The average change in pain score from baseline to the eighth week decreased by 2.61 points. Average pain scores improved by 2 points at the first week and attained clinically significant levels (a decrease of more than 2 points) post the eighth week, with scores continuing to improve throughout the follow-up period. Quality of life was enhanced, opioid doses were steady, and functional status remained unchanged over six months. Severe adverse events were reported in three participants.
3.2. Application to Spinal Metastases
The treatment of spinal metastases is notoriously difficult due to the sensitive nature of the spine, with both watchful waiting and active treatment carrying significant risks of local complications [56,57][42][43]. Cryoablation for spinal metastases is often conducted alone or frequently in combination with vertebral augmentation techniques such as cementoplasty [51][44]. In a study by Autrusseau et al. [51][44], 31 patients (including 36 spinal metastases in 32 sessions) received cryoablation for pain relief, and 10 patients (10 metastases in 10 sessions) for local control. The procedure successfully alleviated pain in 93.8% of palliative sessions, with the average pain scores notably decreasing at 24 h, 1 month, and at the final follow-up (approximately 16.5 months). For those patients needing local tumor control, primary clinical success was achieved in 60% of cases with about 25 months of median follow-up. The overall complication rate was 8%, with no reported secondary fractures or thermal nerve injuries.3.3. Application to Sternal Metastases
Due to its high success rate and the safety provided by real-time visualization of the ice formation, cryoablation can be employed to treat highly sensitive body areas. A study by Hegg et al. [42][45] sought to evaluate the safety and efficacy of cryoablation for sternal metastases. The retrospective review included 12 patients with 12 sternal metastases. The results indicated that cryoablation provided pain relief, as shown by a drop in average pain score from 7.0 to 1.8. Local tumor control was achieved in 80% of the patients treated for this purpose. The study concluded that cryoablation is a safe and potentially effective treatment for painful sternal metastases.3.4. Evaluation of Post-Ablation Area
Evaluating the treated area after cryoablation is crucial in determining the success of the procedure and detecting any local tumor recurrence. In this regard, Gravel et al. [53][46] conducted a study to assess the effectiveness of post-ablation MRI in identifying cases of incomplete treatment of spinal osseous metastases following cryoablation. The study involved 54 spinal bone metastases in 39 patients. The classification of MRI images into four categories resulted in a sensitivity of 77.3% and specificity of 85.9% in identifying residual tumors.3.5. Technical Consideration for Neuroprotection
Preserving neural structures is paramount when treating lesions close to the spine or major peripheral nerves. Kurup et al. [59][47] explored the use of motor evoked potential (MEP) monitoring during the cryoablation procedure of musculoskeletal tumors to reduce the likelihood of nerve damage. This study included 59 procedures on 64 tumors in 52 patients, with tumors located in various sites such as the spine, sacrum, retroperitoneum, pelvis, and extremities. During these procedures, MEP monitoring identified significant decreases in MEPs in 32% of the cases, with transient decreases in 25% and persistent decreases in 7%. Out of the four patients with persistent decreases in MEPs, two experienced motor deficits post-ablation3.6. Technical Consideration for Bone Reinforcement
When conducting ablation on large bone sections or bones that bear weight [47][48], bone reinforcement might be required to avoid post-procedural pathologic fractures. Combining cryoablation with cement stabilization has been reported as highly effective by several studies. Masala et al. [60][49] studied the efficacy of combining cryoablation and vertebroplasty (CVT) vs. vertebroplasty alone in 46 patients with a single vertebral metastasis. They used the Visual Analog Scale (VAS) and the Oswestry Disability Index (ODI) to measure pain levels and quality of life. Although both treatment groups showed a significant reduction in VAS and ODI scores, more notable improvements were observed in the CVT group at various follow-up stages, suggesting CVT as a safe, effective option for pain relief and disability improvement.3.7. Combination Treatment
Sundararajan et al. [63][50] proposed a sequential interventional therapy involving embolization, cryoablation, and osteoplasty for patients with osseous neoplasms, who were unresponsive to conventional treatment3.8. Complications
Despite cryoablation being a minimally invasive procedure guided by CT, it carries a small risk of complications. Auloge et al. [64][51] evaluated the complications and related risk factors in bone tumor cryoablation. The study involved 239 patients who underwent cryoablation for 320 primary or metastatic bone tumors from 2008 to 2017. The overall complication rate was 9.1%, with serious complications making up 2.5% of this total. The most common major complication was secondary fractures, which represented 1.2% of the cases.4. Benign Bone Tumors
4.1. Osteoid Osteoma
Osteoid osteoma (OO) is a small, benign tumor primarily found in the bones of young people and children. Even though it only accounts for approximately 10% to 12% of all benign bone tumors, it can significantly affect the quality of life, causing pain and bone deformity, especially in children [65,66,67][52][53][54]. The treatment for OO has seen a considerable evolution over the years. Traditional surgical removal was once the main treatment approach, but technological advancements have facilitated a shift toward less invasive methods like radiofrequency ablation (RFA) [68,69,70,71][55][56][57][58]. Meng et al. [72][59] conducted a study comparing the safety and effectiveness of percutaneous CT-guided cryoablation of OO to surgical curettage. Both treatment approaches reported a 100% technical success rate. However, patients treated with cryoablation spent significantly less time in the hospital than those undergoing surgery, and both groups showed notable improvement in postoperative Visual Analog Scale (VAS) pain scores.4.2. Osteoblastoma
Cryoablation was also found to be a viable treatment for osteoblastoma in the study by Cazzato et al. [78][60] Technical success was achieved in all cases, and primary clinical success was 100% and 78% at 1 and 12 months of follow-up, respectively. Notably, this study emphasized the need for comprehensive protective measures due to the frequent close proximity of critical structures.4.3. Bone Cyst and Aneurysmal Bone Cyst
Bone cysts are fluid-filled holes that develop within bones. They are commonly found in children and adolescents, and most often occur in the long bones of the body such as the femur or the humerus. Most bone cysts do not cause symptoms and are often discovered incidentally during an X-ray performed for other reasons. However, in some cases, they can cause pain or lead to fractures [79][61]. Aneurysmal bone cysts (ABCs), on the other hand, are an uncommon type of bone cyst that is blood-filled rather than fluid-filled. They can occur at any age but are most commonly diagnosed in individuals under the age of 20. ABCs are expansile and can cause pain, swelling, and deformities in the affected bone. They can also lead to fractures due to the weakening of the bone structure.5. Desmoid Tumors
Desmoid tumors are rare benign tumors originating from musculoaponeurotic structures [85][62]. Despite their benign nature, they can display local aggressiveness, causing disability and sometimes pain. The ESMO advises initial observation and subsequent medical treatment for progressing tumors. Cryoablation, an interventional radiology technique, is recommended for desmoid tumor patients due to its ability to induce cell death through multiple cycles of freezing [86,87,88][63][64][65] (Figure 54).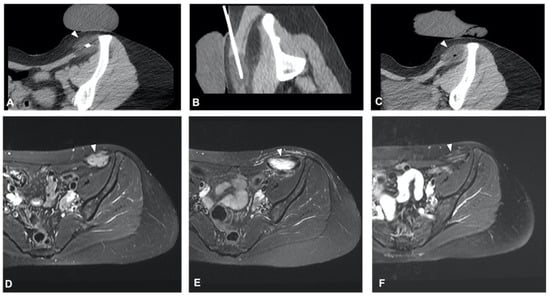
5.1. Cryoablation for Disease Control
5.2. Ablation Margin
Although technically benign tumors, desmoid tumors have a high potential for local recurrence and local invasion. For this reason, they should be treated as malignant lesions, and to obtain a curative effect, all the lesions should be covered by the ice ball, leaving some margins if possible.5.3. Pain Reduction
One of the main symptoms of a desmoid tumor is local pain and discomfort. Bouhamama et al. [99][71] focused on cryoablation’s analgesic efficacy. This study emphasizes the analgesic effect of cryoablation in the treatment of desmoid tumors, reporting a significant reduction in pain post-procedure. It also reports a disease-free survival rate of 42.2% at 3 years, providing a more complete picture of the long-term efficacy of cryoablation.5.4. Patient Selection
In contrast, Testa et al. [97][72] highlighted the trend toward active monitoring as the first line of treatment for desmoid tumors (DTs), reserving systemic and local ablative therapies for cases where the disease is advancing or causing symptoms. This study suggested that determining which patients are better suited for a primary non-interventionist approach as opposed to a direct interventional treatment like cryoablation remains uncertain.6. Technical Consideration
6.1. Planning and Approach
Cryoablation planning requires pre-procedural imaging, ideally within a month prior to the procedure. Thin-section CT is recommended for bone lesions, while MRI with dynamic contrast enhancement and high spatial resolution techniques offer higher sensitivity and specificity for soft tissue lesions [100][73].6.2. Needle Placement and Hydro Dissection
When the lesion is not deeply located and is outside the bone, as in soft tissue tumors, the ultrasound-guided placement of the needles may expedite the process and reduce patient exposure to ionizing radiation [100,101,102][73][74][75]. Hydrodissection is a valuable technique, used to create a safe margin between the tumor and adjacent critical structures. To enhance visibility during control CT scans, it is recommended to use iodinated water for hydro dissection. This allows the operator to clearly delineate the dissected area [58][76].6.3. Ablation and Monitoring
During the ablation phase, real-time visualization of the ice ball using ultrasound can assist in limiting the number of CT scans. However, the complete ice ball cannot be fully visualized due to shadowing; therefore, visualization through CT is essential [103][77]. When performing cryoablation near neural structures, such as the spine or peripheral nerves, continuous monitoring of evoked potentials is necessary.7. Conclusions
Percutaneous cryoablation is a reliable and successful method for treating a range of bone and soft tissue tumors, being increasingly incorporated into the multidisciplinary decision-making process of tumor boards. The procedure’s benefits encompass prompt alleviation of pain, enhancement of life quality, and limited unwanted side effects. Precision in needle placement and ice ball visualization, facilitated by imaging guidance, further enhances the safety and accuracy of the procedure, making it a viable option even for lesions located near critical structures. Despite these benefits, the decision to perform cryoablation should consider tumor location, size, and aggressiveness. Cryoablation has demonstrated substantial potential in handling a variety of musculoskeletal tumors, from retroperitoneal soft tissue sarcomas to sacral chordomas, bone metastases, and benign bone and soft tissue tumors, underlining its adaptability. However, more research is required to fully understand the extent of cryoablation’s capabilities.References
- Foster, R.C.; Stavas, J.M. Bone and Soft Tissue Ablation. Semin. Interv. Radiol. 2014, 31, 167–179.
- Kurup, A.N.; Callstrom, M.R. Ablation of Musculoskeletal Metastases: Pain Palliation, Fracture Risk Reduction, and Oligometastatic Disease. Tech. Vasc. Interv. Radiol. 2013, 16, 253–261.
- Garnon, J.; Koch, G.; Caudrelier, J.; Tsoumakidou, G.; Cazzato, R.; Gangi, A. Expanding the borders: Image-guided procedures for the treatment of musculoskeletal tumors. Diagn. Interv. Imaging 2017, 98, 635–644.
- Mahnken, A.H.; König, A.M.; Figiel, J.H. Current Technique and Application of Percutaneous Cryotherapy. In RöFo-Fortschritte auf dem Gebiet der Röntgenstrahlen und der bildgebenden Verfahren; Georg Thieme Verlag KG: Stuttgart, Germany, 2018; Volume 190, pp. 836–846.
- Cazzato, R.L.; Gantzer, J.; de Marini, P.; Garnon, J.; Koch, G.; Buy, X.; Autrusseau, P.-A.; Auloge, P.; Dalili, D.; Kurtz, J.-E.; et al. Sporadic Desmoid Tumours: Systematic Review with Reflection on the Role of Cryoablation. Cardiovasc. Interv. Radiol. 2022, 45, 613–621.
- Cazzato, R.L.; Garnon, J.; Koch, G.; Dalili, D.; Rao, P.P.; Weiss, J.; Bauones, S.; Auloge, P.; De Marini, P.; Gangi, A. Musculoskeletal interventional oncology: Current and future practices. Br. J. Radiol. 2020, 93, 20200465.
- Baust, J.M.; Santucci, K.L.; Van Buskirk, R.G.; Raijman, I.; Fisher, W.E.; Baust, J.G.; Snyder, K.K. An In Vitro Investigation into Cryoablation and Adjunctive Cryoablation/Chemotherapy Combination Therapy for the Treatment of Pancreatic Cancer Using the PANC-1 Cell Line. Biomedicines 2022, 10, 450.
- Hayek, G.; Kastler, B. Interventional radiology for treatment of bone metastases. Cancer Radiother. 2020, 24, 374–378.
- Chu, K.F.; Dupuy, D.E. Thermal ablation of tumours: Biological mechanisms and advances in therapy. Nat. Rev. Cancer 2014, 14, 199–208.
- The ESMO/European Sarcoma Network Working Group. Soft tissue and visceral sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii102–iii112.
- Casali, P.G.; Blay, J.-Y.; ESMO/CONTICANET/EUROBONET Consensus Panel of Experts. Soft tissue sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v198–v203.
- Lippa, N.; Sargos, P.; Italiano, A.; Kind, M.; Dallaudière, B.; Hauger, O.; Cornelis, F. Standardization of selection criteria for percutaneous image-guided cryoablation of recurrent soft-tissue sarcomas. Diagn. Interv. Imaging 2014, 95, 1071–1077.
- Dalili, D.; Isaac, A.; Cazzato, R.L.; Åström, G.; Bergh, J.; Mansour, R.; Weber, M.-A.; Garnon, J.; Gangi, A. Interventional Techniques for Bone and Musculoskeletal Soft Tissue Tumors: Current Practices and Future Directions—Part II. Stabilization. Semin. Musculoskelet. Radiol. 2020, 24, 710–725.
- Gronchi, A.; Guadagnolo, B.A.; Erinjeri, J.P. Local Ablative Therapies to Metastatic Soft Tissue Sarcoma. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e566–e575.
- de Baere, T.; Tselikas, L.; Gravel, G.; Hakime, A.; Deschamps, F.; Honoré, C.; Mir, O.; Lecesne, A. Interventional radiology: Role in the treatment of sarcomas. Eur. J. Cancer 2018, 94, 148–155.
- Lim, C.T.; Tan, L.B.K.; Nathan, S.S. Prospective evaluation of argon gas probe delivery for cryotherapy of bone tumours. Ann. Acad. Med. Singap. 2012, 41, 347–353.
- Ahlmann, E.R.; Falkinstein, Y.; Fedenko, A.N.; Menendez, L.R. Cryoablation and resection influences patient survival for soft tissue sarcomas: Impact on survivorship and local recurrence. Clin. Orthop. Relat. Res. 2007, 459, 174–181.
- Fan, W.; Niu, L.; Wang, Y.; Zhang, Y.; Yao, X.; Tan, G.; Yang, J.; Li, J. Percutaneous computed tomography-guided cryoablation for recurrent retroperitoneal soft tissue sarcoma: A study of safety and efficacy. Oncotarget 2016, 7, 42639–42649.
- Mendenhall, W.M.; Zlotecki, R.A.; Hochwald, S.N.; Hemming, A.W.; Grobmyer, S.R.; Cance, W.G. Retroperitoneal soft tissue sarcoma. Cancer 2005, 104, 669–675.
- Kurup, A.N.; Woodrum, D.A.; Morris, J.M.; Atwell, T.D.; Schmit, G.D.; Welch, T.J.; Yaszemski, M.J.; Callstrom, M.R. Cryoablation of Recurrent Sacrococcygeal Tumors. J. Vasc. Interv. Radiol. 2012, 23, 1070–1075.
- Susa, M.; Kikuta, K.; Nakayama, R.; Nishimoto, K.; Horiuchi, K.; Oguro, S.; Inoue, M.; Yashiro, H.; Nakatsuka, S.; Nakamura, M.; et al. CT guided cryoablation for locally recurrent or metastatic bone and soft tissue tumor: Initial experience. BMC Cancer 2016, 16, 798.
- Errani, C.; Bazzocchi, A.; Spinnato, P.; Facchini, G.; Campanacci, L.; Rossi, G.; Mavrogenis, A.F. What’s new in management of bone metastases? Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1367–1375.
- Papalexis, N.; Parmeggiani, A.; Peta, G.; Spinnato, P.; Miceli, M.; Facchini, G. Minimally Invasive Interventional Procedures for Metastatic Bone Disease: A Comprehensive Review. Curr. Oncol. 2022, 29, 4155–4177.
- Hong, S.; Youk, T.; Lee, S.J.; Kim, K.M.; Vajdic, C.M. Bone metastasis and skeletal-related events in patients with solid cancer: A Korean nationwide health insurance database study. PLoS ONE 2020, 15, e0234927.
- Cazzato, R.L.; Auloge, P.; De Marini, P.; Boatta, E.; Koch, G.; Dalili, D.; Rao, P.P.; Garnon, J.; Gangi, A. Spinal Tumor Ablation: Indications, Techniques, and Clinical Management. Tech. Vasc. Interv. Radiol. 2020, 23, 100677.
- Gallusser, N.; Goetti, P.; Becce, F.; Vauclair, F.; Rüdiger, H.A.; Bize, P.E.; Cherix, S. Percutaneous image-guided cryoablation of painful bone metastases: A single institution experience. Orthop. Traumatol. Surg. Res. 2019, 105, 369–374.
- Gardner, C.S.; Ensor, J.E.; Ahrar, K.; Huang, S.Y.; Sabir, S.H.; Tannir, N.M.; Lewis, V.O.; Tam, A.L. Cryoablation of Bone Metastases from Renal Cell Carcinoma for Local Tumor Control. J. Bone Jt. Surg. 2017, 99, 1916–1926.
- McArthur, T.A.; Narducci, C.A.; Lander, P.H.; Lopez-Ben, R. Percutane Image-Guided Cryoablation of Painful Osseous Metastases: A Retrospective Single-Center Review. Curr. Probl. Diagn. Radiol. 2017, 46, 282–287.
- Di Staso, M.; Gravina, G.L.; Zugaro, L.; Bonfili, P.; Gregori, L.; Franzese, P.; Marampon, F.; Vittorini, F.; Moro, R.; Tombolini, V.; et al. Treatment of Solitary Painful Osseous Metastases with Radiotherapy, Cryoablation or Combined Therapy: Propensity Matching Analysis in 175 Patients. PLoS ONE 2015, 10, e0129021.
- Thacker, P.G.; Callstrom, M.R.; Curry, T.B.; Mandrekar, J.N.; Atwell, T.D.; Goetz, M.P.; Rubin, J. Palliation of Painful Metastatic Disease Involving Bone with Imaging-Guided Treatment: Comparison of Patients’ Immediate Response to Radiofrequency Ablation and Cryoablation. Am. J. Roentgenol. 2011, 197, 510–515.
- Munk, P.L.; Murphy, K.J.; Gangi, A.; Liu, D.M. Fire and Ice: Percutaneous Ablative Therapies and Cement Injection in Management of Metastatic Disease of the Spine. Semin. Musculoskelet. Radiol. 2011, 15, 125–134.
- Mercadante, S.; Klepstad, P.; Kurita, G.P.; Sjøgren, P.; Pigni, A.; Caraceni, A. Minimally invasive procedures for the management of vertebral bone pain due to cancer: The EAPC recommendations. Acta Oncol. 2015, 55, 129–133.
- Liu, H.; Song, C.; Zhang, B.; Luo, R.; Yang, J. Research trends and areas of focus on cryoablation and oncology: A bibliometric analysis from 2001 to 2020. Medicine 2022, 101, e32513.
- Wallace, A.N.; McWilliams, S.R.; Connolly, S.E.; Symanski, J.S.; Vaswani, D.; Tomasian, A.; Vyhmeister, R.; Lee, A.M.; Madaelil, T.P.; Hillen, T.J. Percutaneous Image-Guided Cryoablation of Musculoskeletal Metastases: Pain Palliation and Local Tumor Control. J. Vasc. Interv. Radiol. 2016, 27, 1788–1796.
- McMenomy, B.P.; Kurup, A.N.; Johnson, G.B.; Carter, R.E.; McWilliams, R.R.; Markovic, S.N.; Atwell, T.D.; Schmit, G.D.; Morris, J.M.; Woodrum, D.A.; et al. Percutaneous Cryoablation of Musculoskeletal Oligometastatic Disease for Complete Remission. J. Vasc. Interv. Radiol. 2013, 24, 207–213.
- Ma, Y.; Wallace, A.N.; Waqar, S.N.; Morgensztern, D.; Madaelil, T.P.; Tomasian, A.; Jennings, J.W. Percutaneous Image-Guided Ablation in the Treatment of Osseous Metastases from Non-small Cell Lung Cancer. Cardiovasc. Interv. Radiol. 2017, 41, 726–733.
- Yang, Y.; Li, Y.; Wu, Y.; Qiu, S.; Liu, C.; Wang, Q.; Hong, Y.; Lyu, J.; Zhang, Y.; Du, D. Retrospective analysis of CT-guided percutaneous cryoablation for treatment of painful osteolytic bone metastasis. Cryobiology 2020, 92, 203–207.
- Prologo, J.D.; Passalacqua, M.; Patel, I.; Bohnert, N.; Corn, D. Image-guided cryoablation for the treatment of painful musculoskeletal metastatic disease: A single-center experience. Skelet. Radiol. 2014, 43, 1551–1559.
- Jennings, J.W.; Prologo, J.D.; Garnon, J.; Gangi, A.; Buy, X.; Palussière, J.; Kurup, A.N.; Callstrom, M.; Genshaft, S.; Abtin, F. Cryoablation for Palliation of Painful Bone Metastases: The MOTION Multicenter Study. Radiol. Imaging Cancer 2021, 3, e200101.
- Callstrom, M.R.; Atwell, T.D.; Charboneau, J.W.; Farrell, M.A.; Goetz, M.P.; Rubin, J.; Sloan, J.A.; Novotny, P.J.; Welch, T.J.; Maus, T.P.; et al. Painful Metastases Involving Bone: Percutaneous Image-guided Cryoablation—Prospective Trial Interim Analysis. Radiology 2006, 241, 572–580.
- De Marini, P.; Cazzato, R.L.; Auloge, P.; Koch, G.; Dalili, D.; Garnon, J.; Gangi, A. Percutaneous image-guided thermal ablation of bone metastases: A retrospective propensity study comparing the safety profile of radio-frequency ablation and cryo-ablation. Int. J. Hyperth. 2020, 37, 1386–1394.
- Grönemeyer, D.H.W.; Schirp, S.; Gevargez, A. Image-guided radiofrequency ablation of spinal tumors: Preliminary experience with an expandable array electrode. Cancer J. 2002, 8, 33–39.
- Levy, J.; Hopkins, T.; Morris, J.; Tran, N.D.; David, E.; Massari, F.; Farid, H.; Vogel, A.; O’connell, W.G.; Sunenshine, P.; et al. Radiofrequency Ablation for the Palliative Treatment of Bone Metastases: Outcomes from the Multicenter OsteoCool Tumor Ablation Post-Market Study (OPuS One Study) in 100 Patients. J. Vasc. Interv. Radiol. 2020, 31, 1745–1752.
- Autrusseau, P.-A.; Cazzato, R.; De Marini, P.; Auloge, P.; Koch, G.; Dalili, D.; Weiss, J.; Mayer, T.; Garnon, J.; Gangi, A. Pain relief and local tumour control following percutaneous image-guided cryoablation for spine metastasis: A 12-year single-centre experience. Clin. Radiol. 2021, 76, 674–680.
- Hegg, R.M.; Kurup, A.N.; Schmit, G.D.; Weisbrod, A.J.; Atwell, T.D.; Olivier, K.R.; Moynihan, T.J.; Callstrom, M.R. Cryoablation of Sternal Metastases for Pain Palliation and Local Tumor Control. J. Vasc. Interv. Radiol. 2014, 25, 1665–1670.
- Gravel, G.; Tselikas, L.; Moulin, B.; Yevich, S.; Baudin, E.; Hakime, A.; Moalla, S.; Mihoubi, F.; Balleyguier, C.; de Baere, T.; et al. Early detection with MRI of incomplete treatment of spine metastases after percutaneous cryoablation. Eur. Radiol. 2019, 29, 5655–5663.
- Kurup, A.N.; Morris, J.M.; Boon, A.J.; Strommen, J.A.; Schmit, G.D.; Atwell, T.D.; Carter, R.E.; Brown, M.J.; Wass, C.T.; Rose, P.S.; et al. Motor Evoked Potential Monitoring during Cryoablation of Musculoskeletal Tumors. J. Vasc. Interv. Radiol. 2014, 25, 1657–1664.
- Prologo, J.D.; Patel, I.; Buethe, J.; Bohnert, N. Ablation Zones and Weight-Bearing Bones: Points of Caution for the Palliative Interventionalist. J. Vasc. Interv. Radiol. 2014, 25, 769–775.e2.
- Masala, S.; Chiocchi, M.; Taglieri, A.; Bindi, A.; Nezzo, M.; De Vivo, D.; Simonetti, G. Combined use of percutaneous cryoablation and vertebroplasty with 3D rotational angiograph in treatment of single vertebral metastasis: Comparison with vertebroplasty. Neuroradiology 2012, 55, 193–200.
- Sundararajan, S.H.; Calamita, S.; Girgis, P.; Ngo, G.; Ranganathan, S.; Giglio, M.; Gendel, V.; Goyal, S.; Nosher, J.; Roychowdhury, S. Sequential Interventional Management of Osseous Neoplasms via Embolization, Cryoablation, and Osteoplasty. J. Oncol. 2019, 2019, 5247837.
- Auloge, P.; Cazzato, R.L.; Rousseau, C.; Caudrelier, J.; Koch, G.; Rao, P.; Chiang, J.B.; Garnon, J.; Gangi, A. Complications of Percutaneous Bone Tumor Cryoablation: A 10-year Experience. Radiology 2019, 291, 521–528.
- Bazzocchi, A.; Gómez, M.P.A.; Tomassoni, M.T.; Napoli, A.; Filippiadis, D.; Guglielmi, G. Musculoskeletal oncology and thermal ablation: The current and emerging role of interventional radiology. Skelet. Radiol. 2022, 52, 447–459.
- Tepelenis, K.; Skandalakis, G.P.; Papathanakos, G.; Kefala, M.A.; Kitsouli, A.; Barbouti, A.; Tepelenis, N.; Varvarousis, D.; Vlachos, K.; Kanavaros, P.; et al. Osteoid Osteoma: An Updated Review of Epidemiology, Pathogenesis, Clinical Presentation, Radiological Features, and Treatment Option. In Vivo 2021, 35, 1929–1938.
- Wu, B.; Xiao, Y.-Y.; Zhang, X.; Zhao, L.; Carrino, J.A. CT-guided percutaneous cryoablation of osteoid osteoma in children: An initial study. Skelet. Radiol. 2011, 40, 1303–1310.
- Shanmugasundaram, S.; Nadkarni, S.; Kumar, A.; Shukla, P.A. Percutaneous Ablative Therapies for the Management of Osteoid Osteomas: A Systematic Review and Meta-Analysis. Cardiovasc. Interv. Radiol. 2021, 44, 739–749.
- Parmeggiani, A.; Martella, C.; Ceccarelli, L.; Miceli, M.; Spinnato, P.; Facchini, G. Osteoid osteoma: Which is the best mininvasive treatment option? Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1611–1624.
- Parvinian, A.; Welch, B.T.; Callstrom, M.R.; Kurup, A.N. Trends in Musculoskeletal Ablation: Emerging Indications and Techniques. Tech. Vasc. Interv. Radiol. 2020, 23, 100678.
- Izzo, A.; Zugaro, L.; Fascetti, E.; Bruno, F.; Zoccali, C.; Arrigoni, F. Management of Osteoblastoma and Giant Osteoid Osteoma with Percutaneous Thermoablation Techniques. J. Clin. Med. 2021, 10, 5717.
- Meng, L.; Zhang, X.; Xu, R.; Wu, B.; Wei, Y.; Li, J.; Shan, H.; Xiao, Y. A preliminary comparative study of percutaneous CT-guided cryoablation with surgical resection for osteoid osteoma. PeerJ 2021, 9, e10724.
- Cazzato, R.L.; Auloge, P.; Dalili, D.; DE Marini, P.; Di Marco, A.; Garnon, J.; Gangi, A. Percutaneous Image-Guided Cryoablation of Osteoblastoma. Am. J. Roentgenol. 2019, 213, 1157–1162.
- Lokiec, F.; Wientroub, S. Simple bone cyst: Etiology, classification, pathology, and treatment modalities. J. Pediatr. Orthop. B 1998, 7, 262–273.
- Walczak, B.E.; Rose, P.S. Desmoid: The Role of Local Therapy in an Era of Systemic Options. Curr. Treat. Options Oncol. 2013, 14, 465–473.
- Kurtz, J.-E.; Buy, X.; Deschamps, F.; Sauleau, E.; Bouhamama, A.; Toulmonde, M.; Honoré, C.; Bertucci, F.; Brahmi, M.; Chevreau, C.; et al. CRYODESMO-O1: A prospective, open phase II study of cryoablation in desmoid tumour patients progressing after medical treatment. Eur. J. Cancer 2020, 143, 78–87.
- Kasper, B.; Baumgarten, C.; Garcia, J.; Bonvalot, S.; Haas, R.; Haller, F.; Hohenberger, P.; Penel, N.; Messiou, C.; van Der Graaf, W.T.; et al. An update on the management of sporadic desmoid-type fibromatosis: A European Consensus Initiative between Sarcoma PAtients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann. Oncol. 2017, 28, 2399–2408.
- Yan, Y.Y.; Walsh, J.P.; Munk, P.L.; Mallinson, P.I.; Simmons, C.; Clarkson, P.W.; Jayaram, P.R.; Heran, M.K.; Ouellette, H.A. A Single-Center 10-Year Retrospective Analysis of Cryoablation for the Management of Desmoid Tumors. J. Vasc. Interv. Radiol. 2021, 32, 1277–1287.
- Errani, C.; Mavrogenis, A.F.; Tsukamoto, S. What’s new in musculoskeletal oncology. BMC Musculoskelet. Disord. 2021, 22, 704.
- Zhou, M.Y.; Bui, N.Q.; Charville, G.W.; Ghanouni, P.; Ganjoo, K.N. Current management and recent progress in desmoid tumors. Cancer Treat. Res. Commun. 2022, 31, 100562.
- Havez, M.; Lippa, N.; Al-Ammari, S.; Kind, M.; Stoeckle, E.; Italiano, A.; Gangi, A.; Hauger, O.; Cornelis, F. Percutaneous Image-Guided Cryoablation in Inoperable Extra-abdominal Desmoid Tumors: A Study of Tolerability and Efficacy. Cardiovasc. Interv. Radiol. 2014, 37, 1500–1506.
- Saltiel, S.; Bize, P.E.; Goetti, P.; Gallusser, N.; Cherix, S.; Denys, A.; Becce, F.; Tsoumakidou, G. Cryoablation of Extra-Abdominal Desmoid Tumors: A Single-Center Experience with Literature Review. Diagnostics 2020, 10, 556.
- Mandel, J.E.; Kim, D.; Yarmohammadi, H.; Ziv, E.; Keohan, M.L.; D’angelo, S.P.; Gounder, M.M.; Whiting, K.; Qin, L.-X.; Singer, S.; et al. Percutaneous Cryoablation Provides Disease Control for Extra-Abdominal Desmoid-Type Fibromatosis Comparable with Surgical Resection. Ann. Surg. Oncol. 2021, 29, 640–648.
- Bouhamama, A.; Lame, F.; Mastier, C.; Cuinet, M.; Thibaut, A.; Beji, H.; Ricoeur, A.; Blay, J.-Y.; Pilleul, F. Local Control and Analgesic Efficacy of Percutaneous Cryoablation for Desmoid Tumors. Cardiovasc. Interv. Radiol. 2019, 43, 110–119.
- Testa, S.; Bui, N.Q.; Charville, G.W.; Avedian, R.S.; Steffner, R.; Ghanouni, P.; Mohler, D.G.; Ganjoo, K.N. Management of Patients with Newly Diagnosed Desmoid Tumors in a First-Line Setting. Cancers 2022, 14, 3907.
- Ryan, A.; Byrne, C.; Pusceddu, C.; Buy, X.; Tsoumakidou, G.; Filippiadis, D. CIRSE Standards of Practice on Thermal Ablation of Bone Tumours. Cardiovasc. Interv. Radiol. 2022, 45, 591–605.
- Cornelis, F.; Havez, M.; Lippa, N.; Al-Ammari, S.; Verdier, D.; Carteret, T.; Amoretti, N.; Gangi, A.; Palussiere, J.; Hauger, O.; et al. Radiologically guided percutaneous cryotherapy for soft tissue tumours: A promising treatment. Diagn. Interv. Imaging 2013, 94, 364–370.
- Tacke, J.; Speetzen, R.; Heschel, I.; Hunter, D.W.; Rau, G.; Günther, R.W. Imaging of interstitial cryotherapy—An in vitro comparison of ultrasound, computed tomography, and magnetic resonance imaging. Cryobiology 1999, 38, 250–259.
- Autrusseau, P.-A.; Garnon, J.; Auloge, P.; Weiss, J.; Dalili, D.; Caudrelier, J.; Cazzato, R.L.; Koch, G.; Gangi, A. Hydrodissection of the Retro-Sternal Space to Protect the Pericardium During Sternal Cryoablation. Cardiovasc. Interv. Radiol. 2020, 43, 1371–1377.
- Castañeda Rodriguez, W.R.; Callstrom, M.R. Effective pain palliation and prevention of fracture for axial-loading skeletal metastases using combined cryoablation and cementoplasty. Tech. Vasc. Interv. Radiol. 2011, 14, 160–169.