Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Ianthe Piscaer | -- | 1574 | 2023-05-09 21:59:23 | | | |
| 2 | Rita Xu | -12 word(s) | 1562 | 2023-05-10 03:55:41 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Piscaer, I.; Janssen, R.; Franssen, F.M.E.; Schurgers, L.J.; Wouters, E.F.M. Vitamin K in Chronic Obstructive Pulmonary Disease. Encyclopedia. Available online: https://encyclopedia.pub/entry/44067 (accessed on 08 August 2026).
Piscaer I, Janssen R, Franssen FME, Schurgers LJ, Wouters EFM. Vitamin K in Chronic Obstructive Pulmonary Disease. Encyclopedia. Available at: https://encyclopedia.pub/entry/44067. Accessed August 08, 2026.
Piscaer, Ianthe, Rob Janssen, Frits M. E. Franssen, Leon J. Schurgers, Emiel F. M. Wouters. "Vitamin K in Chronic Obstructive Pulmonary Disease" Encyclopedia, https://encyclopedia.pub/entry/44067 (accessed August 08, 2026).
Piscaer, I., Janssen, R., Franssen, F.M.E., Schurgers, L.J., & Wouters, E.F.M. (2023, May 09). Vitamin K in Chronic Obstructive Pulmonary Disease. In Encyclopedia. https://encyclopedia.pub/entry/44067
Piscaer, Ianthe, et al. "Vitamin K in Chronic Obstructive Pulmonary Disease." Encyclopedia. Web. 09 May, 2023.
Copy Citation
Although defined by the presence of airflow obstruction and respiratory symptoms, patients with chronic obstructive pulmonary disease (COPD) are characterized by multimorbidity. Numerous co-occurring conditions and systemic manifestations contribute to the clinical presentation and progression of COPD. Vitamin A and vitamin D have been related to COPD pathogenesis. Another fat-soluble vitamin, vitamin K, has been put forward to exert protective roles in COPD. Vitamin K is an unequivocal cofactor for the carboxylation of coagulation factors, but also for extra-hepatic proteins including the soft tissue calcification inhibitor matrix Gla-protein and the bone protein osteocalcin.
chronic obstructive pulmonary disease
emphysema
vitamin K
1. Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by chronic respiratory symptoms and persistent airflow limitation [1]. Structural abnormalities in the lungs are part of the disease, including parenchymal destruction and small airways disease, and one of both may predominate relative to the other [1]. In addition, patients with COPD frequently have multiple co-occurring chronic conditions (i.e., multimorbidity) [2]. Many of these are more common and show more overlap in COPD patients compared with controls [3]. Recognition and treatment of these disorders are relevant since they have a negative impact on the quality of life, morbidity, hospitalizations, and mortality in COPD patients [4].
Smoking is the most important risk factor for the development of COPD and is causally related to multiple chronic morbidities including cardiovascular disease [1][4]. Smoking is, however, not solely accountable for the high prevalence of other chronic diseases in COPD patients. Several additional underlying mechanisms have been suggested, including systemic inflammation, oxidative stress, and genetic susceptibility [4][5][6][7]. Recently, the possible mechanistic role of vitamins in COPD has gained increasing attention. Especially fat-soluble vitamins A [8] and vitamin D [9] have been reported to exert positive effects on COPD. Vitamin K is another fat-soluble vitamin and is proposed to have favorable effects on bone and cardiovascular health [10].
Figure 1. Vitamin K in multimorbidity of COPD.
2. Vitamin K
Vitamin K is well-known for its role as a cofactor in the carboxylation of coagulation factors II, VII, IX, and X as well as proteins C and S in the liver [10][11]. Furthermore, numerous extra-hepatic proteins are vitamin K-dependent [11]. Vitamin K is required for γ-carboxylation of glutamate residues of vitamin K-dependent proteins (VKDPs) thereby gaining biological activity, during a process that is catalyzed by the enzyme γ-glutamyl carboxylase (GGCX) [11]. As part of this conversion, vitamin K hydroquinone is oxidized into vitamin K epoxide [12]. The enzyme vitamin K epoxide reductase (VKOR) plays a critical role in the recycling of vitamin K by converting vitamin K epoxide back to reduced vitamin K in a process called the vitamin K cycle (Figure 2) [11].
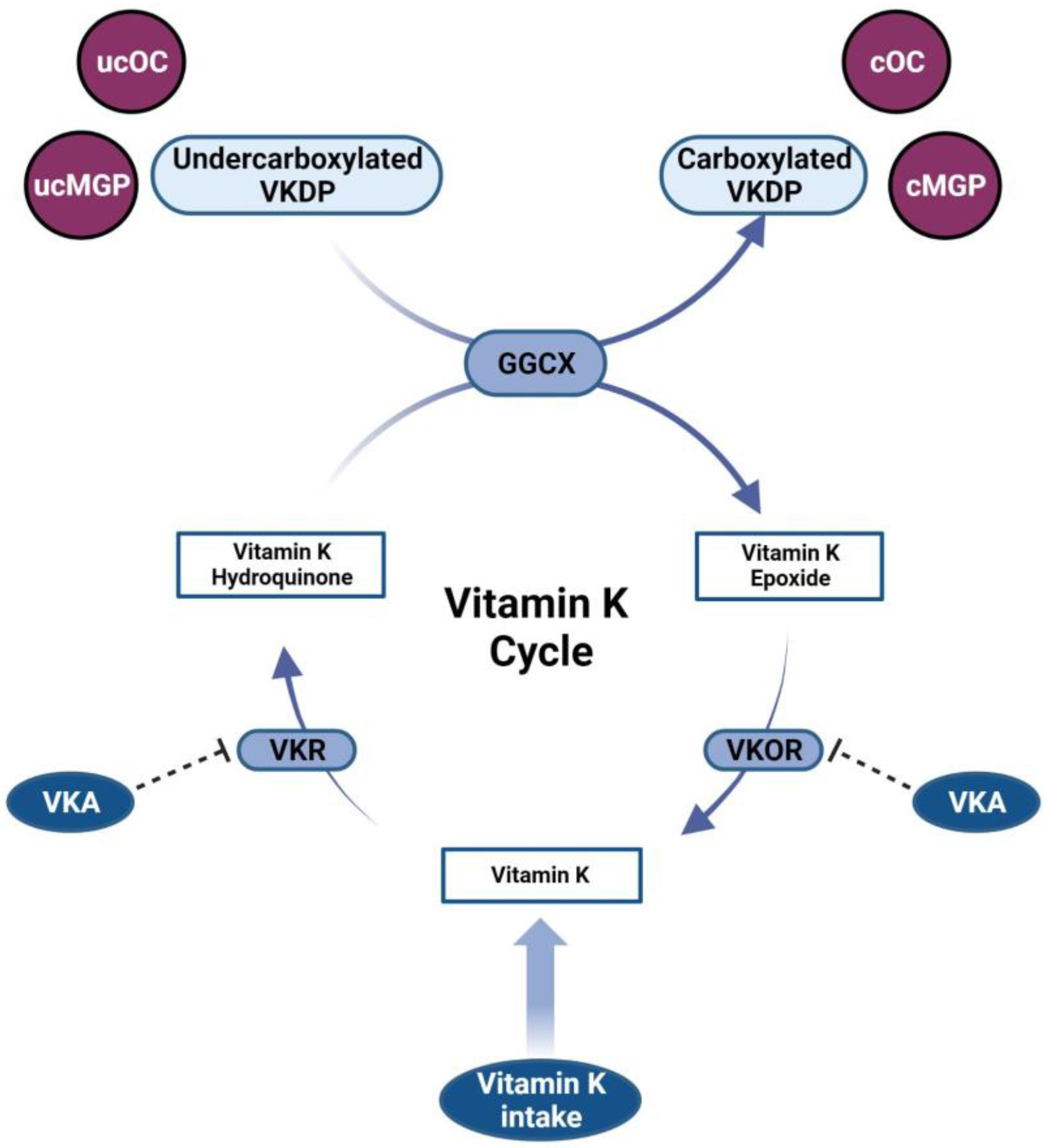
Figure 2. The vitamin K cycle. Vitamin K is reduced into the biologically active vitamin K hydroquinone. During the process of γ-carboxylation of vitamin K-dependent proteins (VKDPs), catalyzed by the enzyme γ-glutamyl carboxylase (GGCX), vitamin K hydroquinone is oxidized into vitamin K epoxide. Subsequently, in a two-step reduction catalyzed by vitamin K epoxide reductase (VKOR) and vitamin K reductase (VKR), vitamin K epoxide is converted back into vitamin K hydroquinone. Vitamin K antagonists (VKA) inhibit VKOR, thereby hampering the recycling of vitamin K. Carboxylated VKDPs including carboxylated osteocalcin (cOC) and carboxylated matrix Gla-protein (cMGP) exert biological activity. ucMGP: undercarboxylated matrix Gla-protein; ucOC: undercarboxylated osteocalcin.
Vitamin K1 (phylloquinone) and vitamin K2 (menaquinones) are the two naturally occurring forms of vitamin K [11]. Green leafy vegetables are an important source of vitamin K1, whereas vitamin K2 is produced by bacteria and mainly found in fermented food products including cheese and the Japanese traditional breakfast “natto” consisting of soybeans fermented by Bacillus subtilis [11][13]. Vitamin K1 is preferentially taken up in the liver, where it is used to activate coagulation factors [11]. Long-chain vitamin K2 is more lipophilic and, due to the long plasma half-life, more efficaciously penetrates extra-hepatic tissues for activation of matrix Gla-protein (MGP) in blood vessels and osteocalcin in bone [11][14]. In the Western diet, the majority of vitamin K intake occurs in the form of vitamin K1 [15]. Vitamin K2, however, has a higher bioavailability than vitamin K1 and may therefore be at least as important for its bioactivity [15][16].
Vitamin K status is influenced by different factors (Figure 3). Dietary intake is the most important of these; however, vitamin K is also synthesized by intestinal bacteria [10]. Poor intake, malabsorption, and reduction of intestinal bacteria by the use of antibiotics are factors that have a negative influence on vitamin K status [10]. In addition, vitamin K status is affected by the efficacy of vitamin K recycling. Various single nucleotide polymorphisms (SNPs) in the VKOR complex subunit 1 (VKORC1) exist, with some haplotypes resulting in lower vitamin K recycling than others [17]. The use of vitamin K antagonists (VKA) interferes with the recycling of vitamin K since these anticoagulants bind to and competitively inhibit the binding of vitamin K to VKORC1 [18]. Finally, vitamin K status can be reduced by increased utilization of vitamin K.
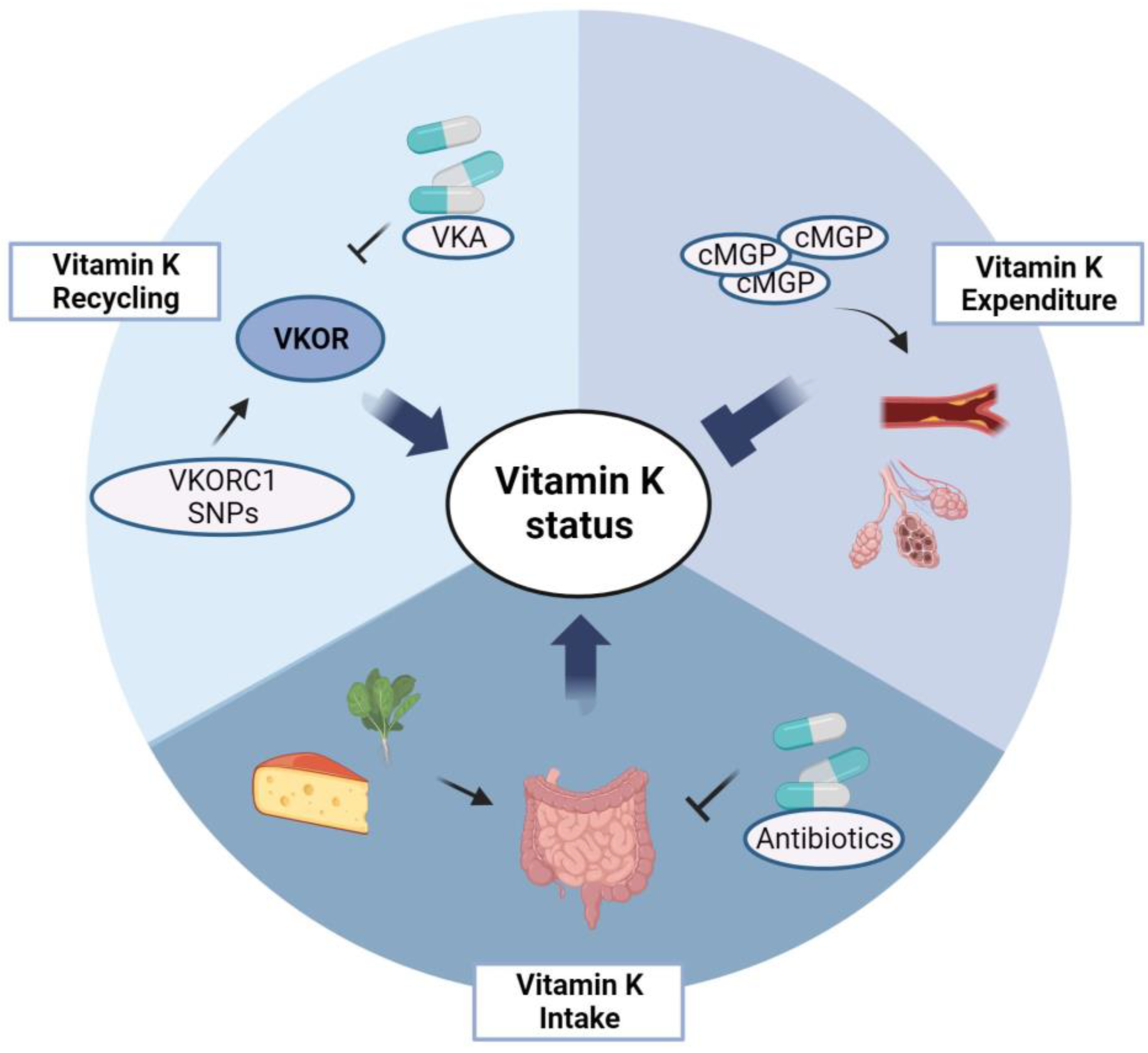
Figure 3. Determinants of vitamin K status. Vitamin K status is influenced by vitamin K intake, recycling, and expenditure. Vitamin K intake is determined by vitamin K consumption, intestinal absorption of vitamin K, and composition of gut microbiota, which can be influenced by use of antibiotics. Vitamin recycling is dependent on VKOR complex subunit 1 (VKORC1) haplotype and inhibition of vitamin K epoxide reductase (VKOR) by use of vitamin K antagonists (VKA). Increased vitamin K expenditure occurs in subjects with extensive vascular calcifications and, potentially, in subjects with pulmonary emphysema. In order to inhibit these pathological processes, the demand for vitamin K to activate VKDPs is increased, thereby exhausting the vitamin K storage. cMGP: carboxylated matrix Gla-protein; SNPs: single nucleotide polymorphisms.
The daily recommended vitamin K intake varies per country and is usually set between 50 μg and 120 μg per day [10][19]. There are currently no cut-off values defining vitamin K deficiency. Although it is technically possible to measure vitamin K directly in circulation, several factors limit the use of serum concentrations as a biomarker for vitamin K status. Vitamin K1 levels in serum highly fluctuate and depend on vitamin K intake as well as triglyceride levels [19]. Vitamin K2 can usually not be detected in the blood when subjects are on an average Western diet unless vitamin K2-containing supplements are used [19]. Vitamin K deficiency in humans results in the secretion of biologically inactive, undercarboxylated forms of VKDPs into plasma [12]. Plasma levels of these proteins are commonly used for assessing functional vitamin K status, with high levels of undercarboxylated VKDPs reflecting low vitamin K status and vice versa. Undercarboxylated coagulation factor II is referred to as protein induced by vitamin K antagonism or absence II (PIVKA-II) and reflects hepatic vitamin K status. The inactive form of the calcification inhibitor MGP, i.e., dephosphorylated undercarboxylated (dp-uc) MGP, is widely used as a biomarker for extra-hepatic vitamin K status [12]. Undercarboxylated osteocalcin can be used for the same purpose [19]. On average, 20% to 30% of MGP and osteocalcin circulate in the undercarboxylated form in subjects not supplemented with vitamin K [16]. This indicates that a certain degree of subclinical vitamin K deficiency is highly prevalent. The triage theory postulates that in a state of shortage, vitamins are primarily directed to the most vital pathways in the body [20]. This implies that when supplies are low, vitamin K is preferentially used for the activation of coagulation factors in the liver at the expense of the activation of extra-hepatic VKDPs [20]. Since only carboxylated VKDPs harbor full activity, suboptimal vitamin K status potentially contributes to pathologies in different organ systems.
3. Vitamin K in COPD
Studies on the role of vitamin K in COPD patients are limited. A cross-sectional study using data from 17,681 subjects from the National Health and Nutrition Examination Survey (NHANES) demonstrated an inverse association between the presence of emphysema and vitamin K consumption [21]. The likelihood of having emphysema was 39% lower in subjects who met the recommended daily intake for vitamin K compared to subjects who did not, and significance was maintained after adjustment for confounders such as smoking, age, and body mass index (BMI) [21].
Another study demonstrated that dp-ucMGP levels (inversely corresponding with vitamin K status) were significantly higher in COPD patients compared to both smoking and never-smoking controls [22]. Dp-ucMGP was inversely associated with the diffusing capacity of the lung for carbon monoxide (DLCO) [22], suggesting an association between vitamin K status and emphysema. However, this correlation was not confirmed in a second independent cohort of COPD patients [22]. Additional research, including studies on the correlation between vitamin K status and emphysema quantification on computed tomography (CT), is necessary to further explore this association. Mortality was higher in COPD patients in the quartile with the highest dp-ucMGP levels compared to patients in the other three quartiles [22]. In line, preliminary retrospective data demonstrated that mortality was higher in COPD patients using VKA compared to those using direct oral anticoagulants (DOAC) [23]. It is tempting to speculate that VKA-induced vitamin K deficiency and, consequentially, insufficient extra-hepatic VKDP carboxylation might be the underlying mechanism contributing to higher mortality. It should be kept in mind that—although analyses were adjusted for possible confounders such as age and comorbidities—confounding by indication might be a source of bias in retrospective studies.
Although aforementioned studies suggest that vitamin K has favorable effects in COPD, specifically in emphysema, a causative relationship cannot be unequivocally proven based on the present limited data. Studies on the effect of vitamin K supplementation in COPD patients are recommended to further explore the beneficial effects of vitamin K on the progression of emphysema and other outcomes in COPD.
References
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582.
- Vanfleteren, L.E.; Spruit, M.A.; Groenen, M.; Gaffron, S.; van Empel, V.P.; Bruijnzeel, P.L.; Rutten, E.P.; Op’t Roodt, J.; Wouters, E.F.; Franssen, F.M. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 728–735.
- Triest, F.J.J.; Franssen, F.M.E.; Reynaert, N.; Gaffron, S.; Spruit, M.A.; Janssen, D.J.A.; Rutten, E.P.A.; Wouters, E.F.M.; Vanfleteren, L.E.G.W. Disease-Specific Comorbidity Clusters in COPD and Accelerated Aging. J. Clin. Med. 2019, 8, 511.
- Cavaillès, A.; Brinchault-Rabin, G.; Dixmier, A.; Goupil, F.; Gut-Gobert, C.; Marchand-Adam, S.; Meurice, J.C.; Morel, H.; Person-Tacnet, C.; Leroyer, C.; et al. Comorbidities of COPD. Eur. Respir. Rev. 2013, 22, 454–475.
- Bernardo, I.; Bozinovski, S.; Vlahos, R. Targeting oxidant-dependent mechanisms for the treatment of COPD and its comorbidities. Pharmacol. Ther. 2015, 155, 60–79.
- Negewo, N.A.; Gibson, P.G.; McDonald, V.M. COPD and its comorbidities: Impact, measurement and mechanisms. Respirology 2015, 20, 1160–1171.
- Macnee, W.; Maclay, J.; McAllister, D. Cardiovascular injury and repair in chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2008, 5, 824–833.
- Caram, L.M.; Amaral, R.A.; Ferrari, R.; Tanni, S.E.; Correa, C.R.; Paiva, S.A.; Godoy, I. Serum Vitamin A and Inflammatory Markers in Individuals with and without Chronic Obstructive Pulmonary Disease. Mediators Inflamm. 2015, 2015, 862086.
- Jolliffe, D.A.; Greenberg, L.; Hooper, R.L.; Mathyssen, C.; Rafiq, R.; de Jongh, R.T.; Camargo, C.A.; Griffiths, C.J.; Janssens, W.; Martineau, A.R. Vitamin D to prevent exacerbations of COPD: Systematic review and meta-analysis of individual participant data from randomised controlled trials. Thorax 2019, 74, 337–345.
- Fairfield, K.M.; Fletcher, R.H. Vitamins for chronic disease prevention in adults: Scientific review. JAMA 2002, 287, 3116–3126, Erratum in JAMA 2002, 288, 1720.
- Stafford, D.W. The vitamin K cycle. J. Thromb. Haemost. 2005, 3, 1873–1878.
- Schurgers, L.J.; Uitto, J.; Reutelingsperger, C.P. Vitamin K-dependent carboxylation of matrix Gla-protein: A crucial switch to control ectopic mineralization. Trends Mol. Med. 2013, 19, 217–226.
- Nagata, C.; Wada, K.; Tamura, T.; Konishi, K.; Goto, Y.; Koda, S.; Kawachi, T.; Tsuji, M.; Nakamura, K. Dietary soy and natto intake and cardiovascular disease mortality in Japanese adults: The Takayama study. Am. J. Clin. Nutr. 2017, 105, 426–431.
- Schurgers, L.J.; Vermeer, C. Differential lipoprotein transport pathways of K-vitamins in healthy subjects. Biochim. Biophys. Acta 2002, 1570, 27–32.
- Beulens, J.W.; Booth, S.L.; van den Heuvel, E.G.; Stoecklin, E.; Baka, A.; Vermeer, C. The role of menaquinones (vitamin K₂) in human health. Br. J. Nutr. 2013, 110, 1357–1368.
- Vermeer, C. Vitamin, K: The effect on health beyond coagulation—An overview. Food Nutr. Res. 2012, 56, 5329.
- Crosier, M.D.; Peter, I.; Booth, S.L.; Bennett, G.; Dawson-Hughes, B.; Ordovas, J.M. Association of sequence variations in vitamin K epoxide reductase and gamma-glutamyl carboxylase genes with biochemical measures of vitamin K status. J. Nutr. Sci. Vitaminol. 2009, 55, 112–119.
- Tie, J.K.; Stafford, D.W. Structure and function of vitamin K epoxide reductase. Vitam. Horm. 2008, 78, 103–130.
- Shea, M.K.; Booth, S.L. Concepts and Controversies in Evaluating Vitamin K Status in Population-Based Studies. Nutrients 2016, 8, 8.
- McCann, J.C.; Ames, B.N. Vitamin K an example of triage theory: Is micronutrient inadequacy linked to diseases of aging? Am. J. Clin. Nutr. 2009, 90, 889–907.
- Shen, T.; Bimali, M.; Faramawi, M.; Orloff, M.S. Consumption of Vitamin K and Vitamin A Are Associated With Reduced Risk of Developing Emphysema: NHANES 2007–2016. Front. Nutr. 2020, 7, 47.
- Piscaer, I.; van den Ouweland, J.M.W.; Vermeersch, K.; Reynaert, N.L.; Franssen, F.M.E.; Keene, S.; Wouters, E.F.M.; Janssens, W.; Vermeer, C.; Janssen, R. Low Vitamin K Status Is Associated with Increased Elastin Degradation in Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2019, 8, 1116.
- Piscaer, I.; Kalkman, G.A.; Fleuren, H.W.; Janssens, W.; Wouters, E.F.; Franssen, F.M.; Janssen, R. Use of Vitamin K Antagonists Is Associated with Increased Mortality in Chronic Obstructive Pulmonary Disease . Am. J. Respir. Crit. Care Med. 2018, 197, A4234.
More
Information
Subjects:
Respiratory System
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.5K
Revisions:
2 times
(View History)
Update Date:
10 May 2023
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No