 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Consolato Sergi | -- | 2098 | 2023-04-13 11:40:05 | | | |
| 2 | Lindsay Dong | Meta information modification | 2098 | 2023-04-14 02:49:03 | | |
Video Upload Options
Echinococcosis is considered a neglected disease in most European countries. However, migratory flows of populations, long-term stays in endemic areas, uninterrupted tourism (travel to Echinococcus-endemic countries), traveling dogs and dog translocations from endemic areas, and inappropriate hygiene practices are potential factors that alarm public health officials. Identifying a cyst-like mass in the liver or lung of an individual with a travel history of likely exposure to sheepdogs in an area where the parasite Echinococcus (E.) granulosus (sive cysticus) is endemic advocates for a prompt preliminary diagnosis of cystic echinococcosis (CE), no matter the age of the affected individuals.
1. Introduction
2. Echinococcosis
3. Epidemiology
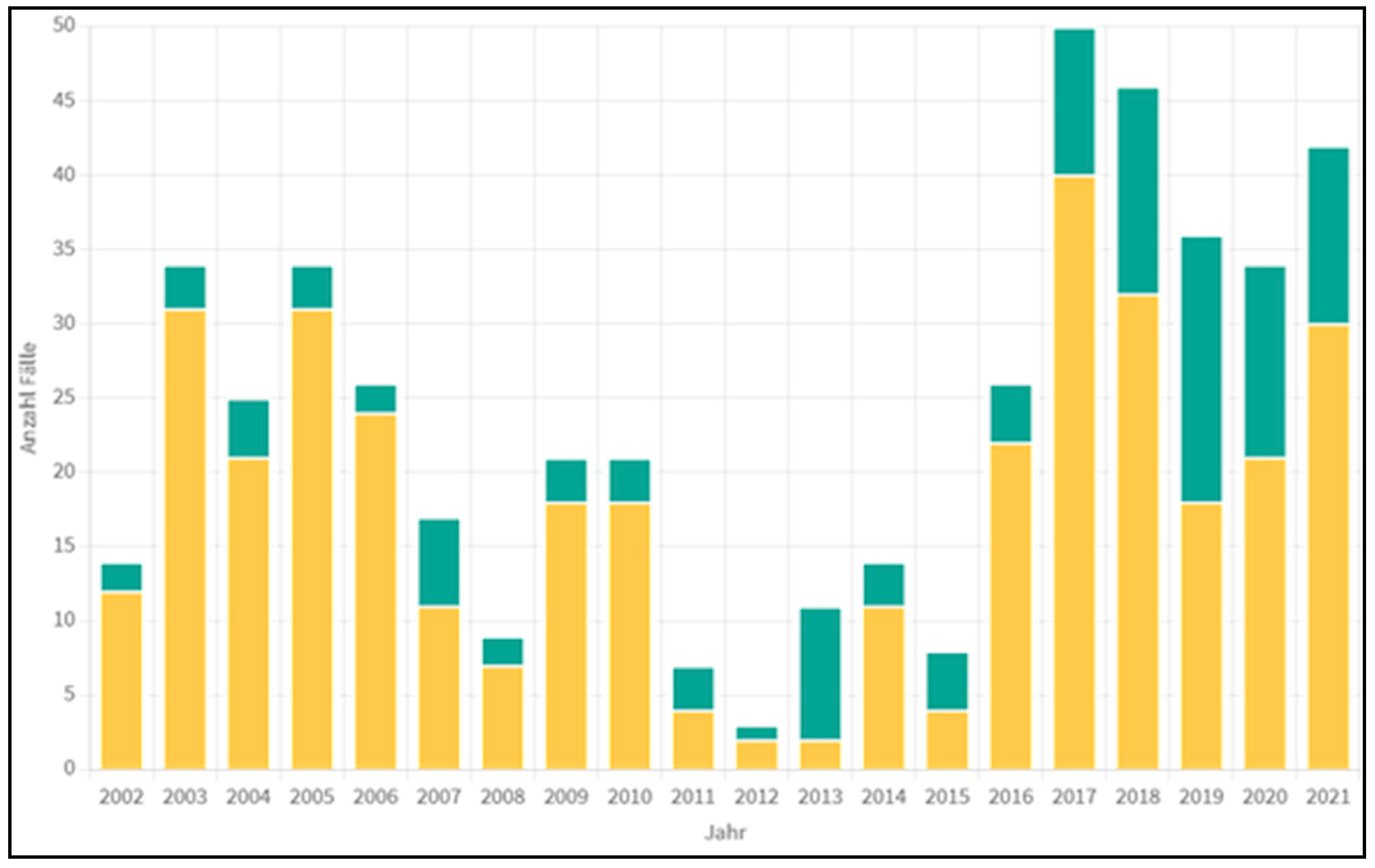
4. Statistical Data from Austria
5. The Parasite Biology
6. Clinical Symptomatology
7. Diagnostics
The diagnostic procedures include sonography (better contrast-enhanced sonography (CEUS)), a CT scan, and, if possible, an MRI of the abdomen [14][17][18]. In addition, a lung X-ray is indicated because lung involvement—usually asymptomatic—is possible [19].
8. Therapy
8.1. Alveolar Echinococcosis
8.2. Cystic Echinococcosis
References
- Albendazole: New indication. Useful adjunct in hydatid disease. Prescrire Int. 2000, 9, 139–142.
- da Silva, A.M. Human echinococcosis: A neglected disease. Gastroenterol. Res. Pract. 2010, 2010, 583297.
- Djuricic, S.M.; Grebeldinger, S.; Kafka, D.I.; Djan, I.; Vukadin, M.; Vasiljevic, Z.V. Cystic echinococcosis in children—The seventeen-year experience of two large medical centers in Serbia. Parasitol. Int. 2010, 59, 257–261.
- Petropoulos, A.S.; Chatzoulis, G.A. Echinococcus Granulosus in Childhood: A Retrospective Study of 187 Cases and Newer Data. Clin. Pediatr. 2019, 58, 864–888.
- Jonaityte, E.; Judickas, M.; Tamuleviciene, E.; Seskute, M. Alveolar Echinococcosis in Children. Case Rep. Pediatr. 2020, 2020, 5101234.
- Tappe, D.; Stich, A.; Frosch, M. Emergence of polycystic neotropical echinococcosis. Emerg. Infect. Dis. 2008, 14, 292–297.
- Xiao, N.; Qiu, J.; Nakao, M.; Li, T.; Yang, W.; Chen, X.; Schantz, P.M.; Craig, P.S.; Ito, A. Echinococcus shiquicus n. sp., a taeniid cestode from Tibetan fox and plateau pika in China. Int. J. Parasitol. 2005, 35, 693–701.
- Gottstein, B. Epidemiology and systematics of cystic and alveolar hydatid disease. Chirurg 2000, 71, 1–8.
- Austrian Agency for Health and Food Safety GmbH: Pathogens from A to Z; Actualised at 20 December 2022. Available online: https://www.ages.at/en/ (accessed on 17 January 2023).
- Pakala, T.; Molina, M.; Wu, G.Y. Hepatic Echinococcal Cysts: A Review. J. Clin. Transl. Hepatol. 2016, 4, 39–46.
- Behera, P.K.; Satpathy, S. Hydatidosis of female genital tract: A case report. Indian J. Pathol. Microbiol. 2003, 46, 78–79.
- Nunnari, G.; Pinzone, M.R.; Gruttadauria, S.; Celesia, B.M.; Madeddu, G.; Malaguarnera, G.; Pavone, P.; Cappellani, A.; Cacopardo, B. Hepatic echinococcosis: Clinical and therapeutic aspects. World J. Gastroenterol. 2012, 18, 1448–1458.
- Yoshida, T.; Kamiyama, T.; Okada, T.; Nakanishi, K.; Yokoo, H.; Kamachi, H.; Matsushita, M.; Sato, N.; Sasaki, F.; Todo, S. Alveolar echinococcosis of the liver in children. J. Hepatobiliary Pancreat. Sci. 2010, 17, 152–157.
- Eckert, J.; Deplazes, P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin. Microbiol. Rev. 2004, 17, 107–135.
- Senyuz, O.F.; Celayir, A.C.; Kilic, N.; Celayir, S.; Sarimurat, N.; Erdogan, E.; Yeker, D. Hydatid disease of the liver in childhood. Pediatr. Surg. Int. 1999, 15, 217–220.
- Foroughi, M.; Bahador, A.; Beizavi, Z. Rapid Growth of Hydatid Cyst: A Pediatric Case Report. Iran J. Parasitol. 2021, 16, 164–167.
- Kratzer, W.; Gruener, B.; Kaltenbach, T.E.; Ansari-Bitzenberger, S.; Kern, P.; Fuchs, M.; Mason, R.A.; Barth, T.F.; Haenle, M.M.; Hillenbrand, A.; et al. Proposal of an ultrasonographic classification for hepatic alveolar echinococcosis: Echinococcosis multilocularis Ulm classification-ultrasound. World J. Gastroenterol. 2015, 21, 12392–12402.
- Stojkovic, M.; Rosenberger, K.; Kauczor, H.U.; Junghanss, T.; Hosch, W. Diagnosing and Staging of Cystic Echinococcosis: How Do CT and MRI Perform in Comparison to Ultrasound? PLoS Negl Trop Dis. 2012, 6, e1880.
- Cevik, M.; Boleken, M.E.; Kurkcuoglu, I.C.; Eser, I.; Dorterler, M.E. Pulmonary hydatid disease is difficult recognized in children. Pediatr. Surg. Int. 2014, 30, 737–741.
- Turgut, A.T.; Akhan, O.; Bhatt, S.; Dogra, V.S. Sonographic spectrum of hydatid disease. Ultrasound Q. 2008, 24, 17–29.
- Calame, P.; Weck, M.; Busse-Cote, A.; Brumpt, E.; Richou, C.; Turco, C.; Doussot, A.; Bresson-Hadni, S.; Delabrousse, E. Role of the radiologist in the diagnosis and management of the two forms of hepatic echinococcosis. Insights Imaging 2022, 13, 68.
- Gharbi, H.A.; Hassine, W.; Brauner, M.W.; Dupuch, K. Ultrasound examination of the hydatic liver. Radiology 1981, 139, 459–463.
- Caoduro, C.; Porot, C.; Vuitton, D.A.; Bresson-Hadni, S.; Grenouillet, F.; Richou, C.; Boulahdour, H.; Blagosklonov, O. The role of delayed 18F-FDG-PET imaging in the follow-up of patients with alveolar echinococcosis. J. Nucl. Med. 2013, 54, 358–363.
- Bulakci, M.; Ilhan, M.; Bademler, S.; Yilmaz, E.; Gulluoglu, M.; Bayraktar, A.; Asik, M.; Guloglu, R. Efficacy of ultrasound-guided core-needle biopsy in the diagnosis of hepatic alveolar echinococcosis: A retrospective analysis. Parasite 2016, 23, 19.
- Sulima, M.; Nahorski, W.; Gorycki, T.; Wolyniec, W.; Waz, P.; Felczak-Korzybska, I.; Szostakowska, B.; Sikorska, K. Ultrasound images in hepatic alveolar echinococcosis and clinical stage of the disease. Adv. Med. Sci. 2019, 64, 324–330.
- Kratzer, W.; Weimer, H.; Schmidberger, J. Echinococcosis: A Challenge for Liver Sonography. Ultraschall Med. 2022, 43, 120–145.
- Graeter, T.; Kratzer, W.; Oeztuerk, S.; Haenle, M.M.; Mason, R.A.; Hillenbrand, A.; Kull, T.; Barth, T.F.; Kern, P.; Gruener, B. Proposal of a computed tomography classification for hepatic alveolar echinococcosis. World J. Gastroenterol. 2016, 22, 3621–3631.
- Brunetti, E.; Kern, P.; Vuitton, D.A. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010, 114, 1–16.
- Faraj, W.; Abi Faraj, C.; Kanso, M.; Nassar, H.; Hoteit, L.; Farsakoury, R.; Zaghal, A.; Yaghi, M.; Jaafar, R.F.; Khalife, M. Hydatid Disease of the Liver in the Middle East: A Single Center Experience. Surg. Infect. 2022, 23, 29–34.
- Calame, P.; Doussot, A.; Turco, C.; Colpart, P.; Heyd, B.; Delabrousse, E. Local invasion of hepatic alveolar echinococcosis should not be underestimated: Lessons learned from imaging-pathologic correlation. Diagn. Interv. Imaging 2021, 102, 189–192.
- Gupta, N.; Javed, A.; Puri, S.; Jain, S.; Singh, S.; Agarwal, A.K. Hepatic hydatid: PAIR, drain or resect? J. Gastrointest. Surg. 2011, 15, 1829–1836.
- Stojkovic, M.; Weber, T.F.; Junghanss, T. Clinical management of cystic echinococcosis: State of the art and perspectives. Curr. Opin. Infect. Dis. 2018, 31, 383–392.
- Demir, S.; Ilikan, G.B.; Erturk, A.; Oztorun, C.I.; Guney, D.; Azili, M.N.; Senel, E.; Tiryaki, H.T. A serious complication of liver hydatid cysts in children: Cystobiliary fistulas. Pediatr. Surg. Int. 2020, 36, 611–620.
- Tersigni, C.; Venturini, E.; Montagnani, C.; Bianchi, L.; Chiappini, E.; de Martino, M.; Galli, L. Should Pediatricians Be Aware of Cystic Echinococcosis? A Literature Review. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 161–168.
- Junghanss, T.; da Silva, A.M.; Horton, J.; Chiodini, P.L.; Brunetti, E. Clinical management of cystic echinococcosis: State of the art, problems, and perspectives. Am. J. Trop. Med. Hyg. 2008, 79, 301–311.

