Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Jean-François Lesgards | -- | 1864 | 2023-03-27 20:25:01 | | | |
| 2 | Dean Liu | Meta information modification | 1864 | 2023-03-28 04:13:31 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Lesgards, J. Whey Proteins for Type 2 Diabetes Mellitus. Encyclopedia. Available online: https://encyclopedia.pub/entry/42568 (accessed on 11 August 2026).
Lesgards J. Whey Proteins for Type 2 Diabetes Mellitus. Encyclopedia. Available at: https://encyclopedia.pub/entry/42568. Accessed August 11, 2026.
Lesgards, Jean-François. "Whey Proteins for Type 2 Diabetes Mellitus" Encyclopedia, https://encyclopedia.pub/entry/42568 (accessed August 11, 2026).
Lesgards, J. (2023, March 27). Whey Proteins for Type 2 Diabetes Mellitus. In Encyclopedia. https://encyclopedia.pub/entry/42568
Lesgards, Jean-François. "Whey Proteins for Type 2 Diabetes Mellitus." Encyclopedia. Web. 27 March, 2023.
Copy Citation
Type 2 diabetes mellitus (T2DM) is a major cause of morbidity and mortality, and it is a major risk factor for the early onset of cardiovascular diseases (CVDs). More than genetics, food, physical activity, walkability, and air pollution are lifestyle factors, which have the greatest impact on T2DM. Certain diets have been shown to be associated with lower T2DM and cardiovascular risk. Diminishing added sugar and processed fats and increasing antioxidant-rich vegetable and fruit intake has often been highlighted, as in the Mediterranean diet. However, less is known about the interest of proteins in low-fat dairy and whey in particular, which have great potential to improve T2DM and could be used safely as a part of a multi-target strategy.
whey proteins
type 2 diabetes mellitus
postprandial hyperglycemia
gut hormones
satiety
antioxidant
1. Whey Intake Improved Insulin Secretion and Postprandial Glycemia
Milk-derived whey as well as casein proteins can produce insulin secretion in obese, pre-diabetic, and also type 2 diabetes individuals [1][2][3][4][5][6]. Studies in humans have shown that whey protein decreases postprandial glycemia and could be used in medical/nutritional therapy to regulate blood sugar [7][8]. In diabetic subjects, whey intake has been associated with a reduction of postprandial hyperglycemia [9][10]. Even a small 15 g dose of whey protein consumed shortly before mixed-macronutrient meals stimulates insulin release, improves postprandial glycemia (−13%), and increases satiety in T2DM subjects (p < 0.05) [11].
Various studies have similarly reported positive effects of whey protein on insulin secretion [12]. The intake of 50 g WPI associated with maltodextrin increased insulin production by 96% versus maltodextrin alone in pre-diabetic adults (p < 0.05) and a 21% decrease in postprandial blood glucose after protein meals (p < 0.0001) [13]. Interestingly, for practical nutrition, the addition of whey (27.6 g) to high-glycemic-index meals (such as bread and mashed potatoes and meatballs) increases insulin release (31% for breakfast and 57% for lunch, both p < 0.05) and diminishes postprandial blood glucose (−21%, p < 0.05) excursion in type 2 diabetic subjects [14].
In lean and healthy subjects, whey consumption has also been shown to decrease blood sugar [13][15]. Between whey, tuna, turkey, and egg albumin, the measure of postprandial glucose and insulin concentrations in 22 lean, healthy men provided the best results for whey [1]. Blood glucose was significantly lower for whey meal than for turkey (p < 0.023) and eggs (p < 0.001), indicating a faster glucose uptake in cells, but not with the tuna meal. Blood insulin was also significantly higher for whey compared to tuna, turkey, and eggs (all p < 0.001).
Moreover, whey protein may have beneficial effects on some symptoms of metabolic syndrome and improve cardiovascular risk factors [12][16][17]. Metabolic syndrome is a combination of hyperglycemia, hypertension, excess body fat around the waist, and abnormal cholesterol or triglyceride levels, increasing the risk of diabetes, heart disease, and stroke [18]. Moreover, a meta-analysis of 22 randomized controlled trials (RCTs), using the Cochrane method for the elimination of bias, showed that whey intake decreased insulin significantly in patients with metabolic syndrome (weighted mean difference (WMD): −0.94; 95% CI: −1.68, −0.21) but did not have an effect on fasting plasma glucose levels [19]. Meanwhile subgroup analyses showed a significant reduction in fasting plasma glucose levels and other meta-analyses including in obese participants who had also shown improvement in fasting plasma glucose levels after whey protein intake [20][21].
2. Effects on Insulin Resistance and Glycated Hemoglobin
A meta-analysis of 22 randomized controlled trials (RCTs) highlighted a significant decrease in glycated hemoglobin (HbA1c) with whey intake in patients with metabolic syndrome (WMD: −0.15; 95% CI: −0.29, −0.01) and in the Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) (WMD: −0.20; 95% CI: −0.36, −0.05) [19]. Another meta-analysis of 30 RCTs suggested that dairy intake, in particular, low-fat dairy products, has a positive action on HOMA-IR (mean difference (MD) of −1.21; 95% CI −1.74 to −0.67; p < 0.00001; I2 = 92%) [22].
Dairy protein consumption before a meal decreases food intake and, in association with carbohydrates, decreases glycemia by insulin-dependent as well as insulin-independent mechanisms [23][24].
Interestingly, whey can also be effective for controlling blood sugar parameters and inflammation before surgery. Fasting before surgery, which can be prolonged from 10 up to 16 h, can induce hyperglycemia due to a limitation of insulin action by the effect of counter-regulatory hormone action. Whey protein in a drink associated with carbohydrates has been shown to minimize the postoperative insulin resistance (HOMA-IR) and associated acute inflammation vs. carbohydrates alone (2.75 ± 0.72 vs. 5.74 ± 1.16; p < 0.05) [25].
3. Mechanisms of Whey and Dairy Proteins Associated with Decrease in Postprandial Glycemia
3.1. Activity of Amino Acids on Insulin Secretion
It has been confirmed that the insulinotropic effect of dairy proteins is associated with certain amino acids, in particular the branched-chain amino acids (BCAAs) who seem to be of vital importance, especially leucine, isoleucine, valine, lysine, and threonine, inducing insulin secretion with leucine, reportedly having the greatest effect acutely [26][27][28]. Leucine activates glutamate dehydrogenase activity in β-cells, which leads to an increase in Krebs cycle activity, oxygen consumption by these cells, and then to increased insulin production [26]. Leucine and high protein intake also seem to modulate AMP-activated protein kinase (AMPK) and mTOR and influence hypothalamic neuropeptides, reducing the expression of orexigenic neuropeptides (NPY) and AgRP (Agouti-related peptide) and increasing anorexigenic neuropeptide pro-opiomelanocortin (POMC) [28].
Whey protein is an exceptional source of BCAAs, which are easily and quickly digested, leading to a rapid increase in BCAA leads in the circulation and insulin release, which may improve postprandial hyperglycemia (Figure 1) [19]. Glutamate and alanine can also participate in insulin secretion coupling, not alone but by amplifying the stimulation by glucose [27]. Cysteine could also be implicated in this process [29].
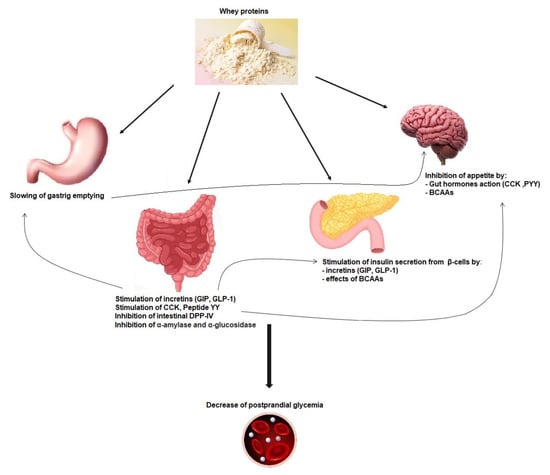
Figure 1. Mechanisms implicated in whey protein activity on postprandial glycemia reduction. GIP: glucose-dependent insulinotropic polypeptide; GLP-1: glucagon-like-peptide-1; CCK: cholecystokinin; PYY: peptide YY; DPP-IV: dipeptidyl peptidase-IV; BCAAs: branched-chain amino acids.
3.2. Incretin Secretion and Insulin Secretion
Dairy-protein-derived peptides can also increase the insulin secretion effect through dipeptidyl peptidase-4 (DPP-4) inhibitory activity in the proximal gut, preventing the incretin glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like-peptide-1 (GLP-1) degradation [17] (Figure 1) [30]. Indeed a major part of secreted insulin is a result of the action of both GIP and GLP-1. However, because of the cleaving activity of DPP-4, GIP and GLP-1 have a half-life of only 1–2 min [31]. Thus, inhibiting DPP-IV activity is considered as a way of treatment in T2DM [32]. Incretins also increase the sensitivity of β-cells to glucose, stimulate β-cell proliferation, and protect these cells against apoptosis [33].
When provided shortly prior to a meal, whey dose-dependently reduces (using from 9 to 18 g) the postprandial glycemia (p < 0.0001) and increases GLP-1 levels (p < 0.0001) [34]. Bioactive substances in whey, among which are IGs, Lf, α-La, and glutamine, have been shown to increase incretin hormones and to inhibit dipeptidyl peptidase-IV [8][19][35][36]. Other studies have shown a strong increase in GLP-1 concentrations after a whey drink when compared to a glucose or fructose drink (from 25 to 50 g of whey, p < 0.05) taken before a meal (30 min to 4 h) [37][38].
Some bioactive peptides should be responsible for influencing postprandial incretin responses [39]. Indeed, whey and milk proteins are degraded during low-pH digestion in the stomach and by gastric pepsin and other peptidases. The resulting hydrolyzed proteins pass into the small intestine and are further split by pancreatic proteases into single amino acids and oligopeptides and finally by other enzymes from the brush-border enzymes into dipeptides, tripeptides, and amino acids. Bioactive peptides can contain from two to twenty amino acid residues or more. Some of these peptides have been identified in the gastrointestinal tract as well as in bloodstream after milk intake, but more studies are needed to fully characterize these peptides and their precise role in glycemia management [39].
However, in present hypertriglyceridemia, obesity and high-baseline GLP-1 levels tend to have poorer response to whey proteins [40], and even positive results have been also observed [2]. It could be linked to glucagon-induced increase with whey protein intake [37]. Furthermore, hypertriglyceridemia augments the hyperglycemic effects of glucagon [41].
3.3. Gastric Emptying Effect on Postprandial Glycemia
The actions of whey proteins on gastric emptying, on postprandial glycemia, and on secretion of incretin hormones are linked together. In addition to its impact on insulinotropic effects, GLP-1 induced by whey intake is also able to slow down gastric emptying by relaxing the proximal stomach, reducing antral and duodenal motility, and increasing pyloric tone. This restrains energy intake and can inhibit glucagon secretion, which all together improve postprandial glycaemia (Figure 1) [44]. The function of the gastrointestinal tract is key for glucose homeostasis, especially during the postprandial phase, and slowing gastric emptying can diminish postprandial glycemic excursions in healthy and diabetic subjects (Figure 1) [35][45][46][47]. Other gut hormones, namely, cholecystokinin (CCK) and peptide YY (PYY), can decrease gastric emptying and appetite [48].
The importance of slowing gastric emptying is key in the decrease in postprandial glycemia observed when proteins are added to glucose intake [49]. Likewise, a whey “preload” is able to slow gastric emptying of a following meal in both healthy [50] and T2DM subjects [51]. In diabetic subjects, GLP-1 was higher when whey was ingested (55 g) between −15 min and 90 min before the meal versus during the mean (p < 0.001), even if the incremental area under the curve (iAUC) was not significantly different [51], and both decrease postprandial glucose (363.7 ± 64.5 mmol · min−1 · L−1) and (406.3 ± 85.9 mmol · min−1 · L−1) compared with no whey (734.9 ± 98.9 mmol · min−1 · L−1; p < 0.005).
3.4. Gut Hormones, Amino Acids, and Satiety
Satiety induced by proteins has been demonstrated, in an acute manner, with meals containing from 25 to 90% proteins, leading to a significant decrease in energy intake. It has also been shown with high protein content in ad libitum diets, lasting from a few days up to 6 months [52]. Among the three macronutrients, protein has the greatest satiating action. After protein-containing nutrient intake, signals can be sent to the central nervous system (CNS) via gastric and gut peptide action and via the bloodstream after digestion. Indeed, satiety is induced by various mechanisms, which are both visceral (during digestion) and metabolic (inter-prandial phase) and directed towards the CNS directly at the level of the hypothalamus and indirectly mainly through the vagus nerve [53]. Regarding meal size, the negative feedback control from gastrointestinal signals and bloodstream takes place in the dorsal vagal complex (brainstem) and in the hypothalamus.
The gut peptide hormones upregulated by whey consumption include CCK, PYY, GLP-1, and GPI (Figure 1) [33][35][50]. It has been proposed that high protein meals could induce the greatest production of PYY and the highest satiety feeling in obese as well as normal-weight human subjects [51]. Ghrelin, an orexigenic peptide decreased after consumption of proteins; leptin; and insulin levels are also known to influence satiety [35][37][51].
Although GLP-1 can have an action on peripheral organs through the circulation, it is of note also that GLP-1 can be produced by the pancreas and brain as well [33].
Studies demonstrate that dairy and whey proteins decrease appetite better than other protein sources such as eggs, casein, or soy [50][54][55][56]. In the study from Hall et al., plasma CCK was increased by 60% (iAUC, p < 0.005), GLP-1 by 65% (iAUC, p < 0.05), and GIP by 36% (iAUC, p < 0.01) following a 48 g whey preload when compared with casein, showing the particular potential of whey in this field [50]. Whey, tuna, turkey, and egg albumin meals were compared in terms of appetite measures and energy intake in 22 lean healthy men. The best results were obtained for whey, with a significant reduction of mean energy intake at the ad libitum meal 4 h after (p < 0.001) [1]. Appetite rated by the subjects, postprandial insulin, and energy intake during the meal were strongly related.
References
- Pal, S.; Ellis, V. The acute effects of four protein meals on insulin, glucose, appetite and energy intake in lean men. Br. J. Nutr. 2010, 104, 1241–1248.
- Pal, S.; Ellis, V. The chronic effects of whey proteins on blood pressure, vascular function, and inflammatory markers in overweight individuals. Obesity 2010, 18, 1354–1359.
- Jonker, J.T.; Wijngaarden, M.A.; Kloek, J.; Groeneveld, Y.; Gerhardt, C.; Brand, R.; Kies, A.K.; Romijn, J.A.; Smit, J.W. Effects of low doses of casein hydrolysate on post-challenge glucose and insulin levels. Eur. J. Intern. Med. 2011, 22, 245–248.
- Gunnerud, U.J.; Ostman, E.M.; Björck, I.M. Effects of whey proteins on glycaemia and insulinaemia to an oral glucose load in healthy adults; a dose-response study. Eur. J. Clin. Nutr. 2013, 67, 749–753.
- Manders, R.J.; Hansen, D.; Zorenc, A.H.; Dendale, P.; Kloek, J.; Saris, W.H.; van Loon, L.J. Protein co-ingestion strongly increases postprandial insulin secretion in type 2 diabetes patients. J. Med. Food 2014, 17, 758–763.
- Mortensen, L.S.; Holmer-Jensen, J.; Hartvigsen, M.L.; Jensen, V.K.; Astrup, A.; de Vrese, M.; Holst, J.J.; Thomsen, C.; Hermansen, K. Effects of different fractions of whey protein on postprandial lipid and hormone responses in type 2 diabetes. Eur. J. Clin. Nutr. 2012, 66, 799–805.
- Petersen, B.L.; Ward, L.S.; Bastian, E.D.; Jenkins, A.L.; Campbell, J.; Vuksan, V. A whey protein supplement decreases post-prandial glycemia. Nutr. J. 2009, 8, 47.
- Adams, R.L.; Broughton, K.S. Insulinotropic Effects of Whey: Mechanisms of Action, Recent Clinical Trials, and Clinical Applications. Ann. Nutr. Metab. 2016, 69, 56–63.
- Smith, K.; Taylor, G.S.; Brunsgaard, L.H.; Walker, M.; Bowden Davies, K.A.; Stevenson, E.J.; West, D.J. Thrice daily consumption of a novel, premeal shot containing a low dose of whey protein increases time in euglycemia during 7 days of free-living in individuals with type 2 diabetes. BMJ Open Diabetes Res. Care 2022, 10, e002820.
- Comerford, K.B.; Pasin, G. Emerging Evidence for the Importance of Dietary Protein Source on Glucoregulatory Markers and Type 2 Diabetes: Different Effects of Dairy, Meat, Fish, Egg, and Plant Protein Foods. Nutrients 2016, 8, 446.
- King, D.G.; Walker, M.; Campbell, M.D.; Breen, L.; Stevenson, E.J.; West, D.J. A small dose of whey protein co-ingested with mixed-macronutrient breakfast and lunch meals improves postprandial glycemia and suppresses appetite in men with type 2 diabetes: A randomized controlled trial. Am. J. Clin. Nutr. 2018, 107, 550–557.
- Pal, S.; Radavelli-Bagatini, S. The effects of whey protein on cardiometabolic risk factors. Obes. Rev. 2013, 14, 324–343.
- Hoefle, A.S.; Bangert, A.M.; Stamfort, A.; Gedrich, K.; Rist, M.J.; Lee, Y.M.; Skurk, T.; Daniel, H. Metabolic responses of healthy or prediabetic adults to bovine whey protein and sodium caseinate do not differ. J. Nutr. 2015, 145, 467–475.
- Frid, A.H.; Nilsson, M.; Holst, J.J.; Björck, I.M. Effect of whey on blood glucose and insulin responses to composite breakfast and lunch meals in type 2 diabetic subjects. Am. J. Clin. Nutr. 2005, 82, 69–75.
- Power, O.; Hallihan, A.; Jakeman, P. Human insulinotropic response to oral ingestion of native and hydrolysed whey protein. Amino Acids 2009, 37, 333–339.
- Sousa, G.T.; Lira, F.S.; Rosa, J.C.; de Oliveira, E.P.; Oyama, L.M.; Santos, R.V.; Pimentel, G.D. Dietary whey protein lessens several risk factors for metabolic diseases: A review. Lipids Health Dis. 2012, 11, 67.
- Bjørnshave, A.; Hermansen, K. Effects of dairy protein and fat on the metabolic syndrome and type 2 diabetes. Rev. Diabet Stud. 2014, 11, 153–166.
- Grundy, S.M.; Brewer, H.B.; Cleeman, J.I.; Smith, S.C.; Lenfant, C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438.
- Amirani, E.; Milajerdi, A.; Reiner, Ž.; Mirzaei, H.; Mansournia, M.A.; Asemi, Z. Effects of whey protein on glycemic control and serum lipoproteins in patients with metabolic syndrome and related conditions: A systematic review and meta-analysis of randomized controlled clinical trials. Lipids Health Dis. 2020, 19, 209.
- Wirunsawanya, K.; Upala, S.; Jaruvongvanich, V.; Sanguankeo, A. Whey Protein Supplementation Improves Body Composition and Cardiovascular Risk Factors in Overweight and Obese Patients: A Systematic Review and Meta-Analysis. J. Am. Coll. Nutr. 2018, 37, 60–70.
- Badely, M.; Sepandi, M.; Samadi, M.; Parastouei, K.; Taghdir, M. The effect of whey protein on the components of metabolic syndrome in overweight and obese individuals; a systematic review and meta-analysis. Diabetes Metab. Syndr. 2019, 13, 3121–3131.
- Sochol, K.M.; Johns, T.S.; Buttar, R.S.; Randhawa, L.; Sanchez, E.; Gal, M.; Lestrade, K.; Merzkani, M.; Abramowitz, M.K.; Mossavar-Rahmani, Y.; et al. The Effects of Dairy Intake on Insulin Resistance: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrients 2019, 11, 2237.
- Akhavan, T.; Luhovyy, B.L.; Brown, P.H.; Cho, C.E.; Anderson, G.H. Effect of premeal consumption of whey protein and its hydrolysate on food intake and postmeal glycemia and insulin responses in young adults. Am. J. Clin. Nutr. 2010, 91, 966–975.
- Pereira, M.A.; Jacobs, D.R.; Van Horn, L.; Slattery, M.L.; Kartashov, A.I.; Ludwig, D.S. Dairy consumption, obesity, and the insulin resistance syndrome in young adults: The CARDIA Study. JAMA 2002, 287, 2081–2089.
- Perrone, F.; da-Silva-Filho, A.C.; Adôrno, I.F.; Anabuki, N.T.; Leal, F.S.; Colombo, T.; da Silva, B.D.; Dock-Nascimento, D.B.; Damião, A.; de Aguilar-Nascimento, J.E. Effects of preoperative feeding with a whey protein plus carbohydrate drink on the acute phase response and insulin resistance. A randomized trial. Nutr. J. 2011, 10, 66.
- van Loon, L.J.; Saris, W.H.; Verhagen, H.; Wagenmakers, A.J. Plasma insulin responses after ingestion of different amino acid or protein mixtures with carbohydrate. Am. J. Clin. Nutr. 2000, 72, 96–105.
- Newsholme, P.; Bender, K.; Kiely, A.; Brennan, L. Amino acid metabolism, insulin secretion and diabetes. Biochem. Soc. Trans. 2007, 35, 1180–1186.
- Potier, M.; Darcel, N.; Tomé, D. Protein, amino acids and the control of food intake. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 54–58.
- Jain, S.K. L-cysteine supplementation as an adjuvant therapy for type-2 diabetes. Can. J. Physiol. Pharmacol. 2012, 90, 1061–1064.
- Lacroix, I.M.; Li-Chan, E.C. Inhibition of dipeptidyl peptidase (DPP)-IV and α-glucosidase activities by pepsin-treated whey proteins. J. Agric. Food Chem. 2013, 61, 7500–7506.
- Psallas, M.; Manes, C. Incretins in type 2 diabetes mellitus: Cardiovascular and anti-atherogenic effects beyond glucose lowering. Hippokratia 2012, 16, 100–105.
- Deacon, C.F. Dipeptidyl peptidase-4 inhibitors in the treatment of type 2 diabetes: A comparative review. Diabetes Obes. Metab. 2011, 13, 7–18.
- Campbell, J.E.; Drucker, D.J. Pharmacology, physiology, and mechanisms of incretin hormone action. Cell Metab. 2013, 17, 819–837.
- Gunnerud, U.J.; Heinzle, C.; Holst, J.J.; Östman, E.M.; Björck, I.M. Effects of pre-meal drinks with protein and amino acids on glycemic and metabolic responses at a subsequent composite meal. PLoS ONE 2012, 7, e44731.
- Mignone, L.E.; Wu, T.; Horowitz, M.; Rayner, C.K. Whey protein: The “whey” forward for treatment of type 2 diabetes. World J. Diabetes 2015, 6, 1274–1284.
- Jakubowicz, D.; Froy, O. Biochemical and metabolic mechanisms by which dietary whey protein may combat obesity and Type 2 diabetes. J. Nutr. Biochem. 2013, 24, 1–5.
- Bowen, J.; Noakes, M.; Clifton, P.M. Appetite hormones and energy intake in obese men after consumption of fructose, glucose and whey protein beverages. Int. J. Obes. 2007, 31, 1696–1703.
- Wu, T.; Little, T.J.; Bound, M.J.; Borg, M.; Zhang, X.; Deacon, C.F.; Horowitz, M.; Jones, K.L.; Rayner, C.K. A Protein Preload Enhances the Glucose-Lowering Efficacy of Vildagliptin in Type 2 Diabetes. Diabetes Care 2016, 39, 511–517.
- Horner, K.; Drummond, E.; Brennan, L. Bioavailability of milk protein-derived bioactive peptides: A glycaemic management perspective. Nutr. Res. Rev. 2016, 29, 91–101.
- Almario, R.U.; Buchan, W.M.; Rocke, D.M.; Karakas, S.E. Glucose-lowering effect of whey protein depends upon clinical characteristics of patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2017, 5, e000420.
- Steiner, G.; Morita, S.; Vranic, M. Resistance to insulin but not to glucagon in lean human hypertriglyceridemics. Diabetes 1980, 29, 899–905.
- Baba, W.N.; Mudgil, P.; Kamal, H.; Kilari, B.P.; Gan, C.Y.; Maqsood, S. Identification and characterization of novel α-amylase and α-glucosidase inhibitory peptides from camel whey proteins. J. Dairy Sci. 2021, 104, 1364–1377.
- Konrad, B.; Anna, D.; Marek, S.; Marta, P.; Aleksandra, Z.; Józefa, C. The Evaluation of Dipeptidyl Peptidase (DPP)-IV, α-Glucosidase and Angiotensin Converting Enzyme (ACE) Inhibitory Activities of Whey Proteins Hydrolyzed with Serine Protease Isolated from Asian Pumpkin (Cucurbita ficifolia). Int. J. Pept. Res. Ther. 2014, 20, 483–491.
- Marathe, C.S.; Rayner, C.K.; Jones, K.L.; Horowitz, M. Relationships between gastric emptying, postprandial glycemia, and incretin hormones. Diabetes Care 2013, 36, 1396–1405.
- Horowitz, M.; Edelbroek, M.A.; Wishart, J.M.; Straathof, J.W. Relationship between oral glucose tolerance and gastric emptying in normal healthy subjects. Diabetologia 1993, 36, 857–862.
- Rayner, C.K.; Samsom, M.; Jones, K.L.; Horowitz, M. Relationships of upper gastrointestinal motor and sensory function with glycemic control. Diabetes Care 2001, 24, 371–381.
- Kojecky, V.; Bernatek, J.; Horowitz, M.; Zemek, S.; Bakala, J.; Hep, A. Prevalence and determinants of delayed gastric emptying in hospitalised Type 2 diabetic patients. World J. Gastroenterol. 2008, 14, 1564–1569.
- Nguyen, N.Q.; Fraser, R.J.; Bryant, L.K.; Chapman, M.J.; Wishart, J.; Holloway, R.H.; Butler, R.; Horowitz, M. The relationship between gastric emptying, plasma cholecystokinin, and peptide YY in critically ill patients. Crit. Care 2007, 11, R132.
- Karamanlis, A.; Chaikomin, R.; Doran, S.; Bellon, M.; Bartholomeusz, F.D.; Wishart, J.M.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Effects of protein on glycemic and incretin responses and gastric emptying after oral glucose in healthy subjects. Am. J. Clin. Nutr. 2007, 86, 1364–1368.
- Hall, W.L.; Millward, D.J.; Long, S.J.; Morgan, L.M. Casein and whey exert different effects on plasma amino acid profiles, gastrointestinal hormone secretion and appetite. Br. J. Nutr. 2003, 89, 239–248.
- Ma, J.; Stevens, J.E.; Cukier, K.; Maddox, A.F.; Wishart, J.M.; Jones, K.L.; Clifton, P.M.; Horowitz, M.; Rayner, C.K. Effects of a protein preload on gastric emptying, glycemia, and gut hormones after a carbohydrate meal in diet-controlled type 2 diabetes. Diabetes Care 2009, 32, 1600–1602.
- Veldhorst, M.; Smeets, A.; Soenen, S.; Hochstenbach-Waelen, A.; Hursel, R.; Diepvens, K.; Lejeune, M.; Luscombe-Marsh, N.; Westerterp-Plantenga, M. Protein-induced satiety: Effects and mechanisms of different proteins. Physiol. Behav. 2008, 94, 300–307.
- Fromentin, G.; Darcel, N.; Chaumontet, C.; Marsset-Baglieri, A.; Nadkarni, N.; Tomé, D. Peripheral and central mechanisms involved in the control of food intake by dietary amino acids and proteins. Nutr. Res. Rev. 2012, 25, 29–39.
- Anderson, G.H.; Tecimer, S.N.; Shah, D.; Zafar, T.A. Protein source, quantity, and time of consumption determine the effect of proteins on short-term food intake in young men. J. Nutr. 2004, 134, 3011–3015.
- Uhe, A.M.; Collier, G.R.; O’Dea, K. A comparison of the effects of beef, chicken and fish protein on satiety and amino acid profiles in lean male subjects. J. Nutr. 1992, 122, 467–472.
- Tahavorgar, A.; Vafa, M.; Shidfar, F.; Gohari, M.; Heydari, I. Whey protein preloads are more beneficial than soy protein preloads in regulating appetite, calorie intake, anthropometry, and body composition of overweight and obese men. Nutr. Res. 2014, 34, 856–861.
More
Information
Subjects:
Food Science & Technology
Contributor
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.2K
Entry Collection:
Peptides for Health Benefits
Revisions:
2 times
(View History)
Update Date:
28 Mar 2023
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No