 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Natalia Ivanovna Ivanovna Agalakova | -- | 4785 | 2023-02-01 18:16:48 | | | |
| 2 | Camila Xu | -26 word(s) | 4759 | 2023-02-02 02:01:12 | | |
Video Upload Options
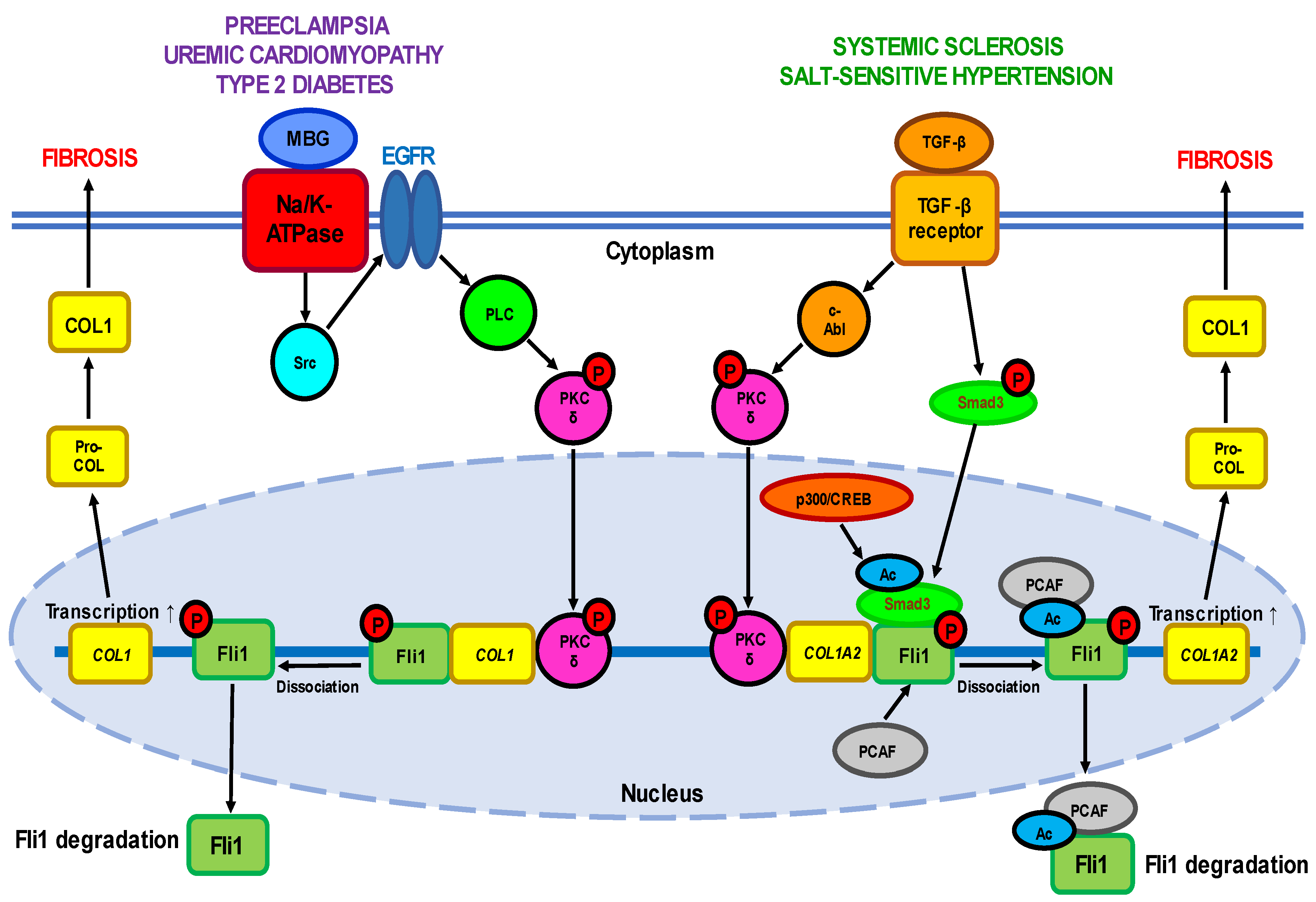
Being initially described as a factor of virally induced leukemias, Fli1 (Friend leukemia integration 1) lately has attracted considerable interest due to its role in both healthy physiology and a variety of pathological conditions. Over the past years Fli1 was found to be one of the crucial regulators of normal hematopoiesis, vasculogenesis and immune responses. However, abnormal expression of Fli1 due to genetic predisposition, epigenetic reprogramming (modifications) or environmental factors is associated with a few diseases of different etiology. Fli1 hyperexpression leads to malignant transformation of cells and progression of cancers such as Ewing’s sarcoma. The deficiency of Fli1 implicates in development of systemic sclerosis and hypertensive disorders, which are often accompanied by pronounced fibrosis in different organs.
1. Introduction
2. Diseases Associated with Fli1 Deficiency
2.1. Fli1 in Systemic Sclerosis
2.2. Fli1 in Uremic Cardiomyopathy
2.3. Fli1 in Preeclampsia
2.4. Fli1 as a Common Causative Factor of Hypertension
| Expression | Effect | Experimental System | References | |
|---|---|---|---|---|
| Fli1 repressors | ||||
| TGF-β | ↑ | Activation of TGF-β receptors |
Human dermal fibroblasts; rat diabetes model; rat hypertension model |
[25][29][32][38][39][79][80][81] |
| c-Abl | ↑ | PKC-δ phosphorylation | Human normal and SSc dermal fibroblasts | [40][41][47][51] |
| PKC-δ | ↑ | Fli1 phosphorylation | Human normal and SSc dermal fibroblasts; FLI1-transfected HEK293T cells; FLI1 silencing in human UA |
[37][39][42][47][77] |
| Endothelin-1 | ↑ | Fli1 activation | Human normal and SSc dermal fibroblasts; BLM-treated mice |
[42] |
| PCAF | ↑ | Fli1 acetylation | Human dermal fibroblasts; FLI1-transfected HEK293T cells |
[38] |
| CXCL4 | ↑ | Vasculopathy | HUVECs | [51] |
| MBG | ↑ | PKC-δ activation; Fli1 suppression | Wild-type and FLI1-knockdown mice; rat CKD model; rat cardiac fibroblasts; human cardiac fibroblasts; human renal fibroblasts; FLI1-transfected renal fibroblasts; rat diabetes model; rat hypertension model; rat PE model |
[16][66][67][68][73][74][75][76][77][79][80][81] |
| Fli1-deficiency targets | ||||
| COL1 | ↑ | Collagen synthesis | FLI1-transfected human dermal fibroblasts; human normal and SSc dermal fibroblasts; murine Fli11−/−, Fli1+/− and Fli1+/+ fibroblasts; wild-type and FLI1-knockdown mice; rat CKD model; rat cardiac fibroblasts; human cardiac fibroblasts; human renal fibroblasts; FLI1-transfected renal fibroblasts; rat diabetes model; rat hypertension model; rat PE model; human PE UA; FLI1 silencing in human UA; human MBG-treated UA |
[8][16][25][29][32][38][66][67][68][73][74][75][76][77][79][80][81] |
| CTGF(CCN2) | ↑ | COL1A1 and COL1A2 upregulation; MMP-1 downregulation | FLI1-transfected human dermal fibroblasts; human SSc fibroblasts |
[32][33] |
| MMP-1 | ↓ | Increased production of EMC components | FLI1-transfected human dermal fibroblasts; human SSc fibroblasts |
[32][33] |
| Fibronectin | ↑ | Fibrosis | Human CD14+ monocytes and CD14+ macrophages | [23] |
| Chemerin | ↑ | Impaired angiogenesis | Human SSc dermal vessels and HDMECs; murine Fli1+/− dermal blood vessels; |
[35] |
| S100A12 | ↑ | Skin sclerosis | Human SSc skin; | [36] |
| RALDH1 | ↓ | Fibrosis | Human dermal dendritic cells; BLM-treated Fli1+/− mice |
[30] |
| Cathepsin B | ↑ ↓ |
Vasculopathy Increased production of EMC components |
FLI1 silencing in HDMECs; Fli1+/− mice; human dcSSc dermal fibroblasts, early dcSSc dermal fibroblasts |
[43] |
| Cathepsin L | ↑ ↓ |
Vasculopathy Increased production of EMC components |
FLI1 silencing in HDMECs; human SS dermal vessels and skin; FLI1-knockout mice; skin of BLM-treated mice |
[45] |
| Cathepsin V | ↓ | Increased production of EMC components | FLI1 silencing in HDMECs; human dcSSc dermal fibroblasts, microvascular ECs, dcSSc and lcSSc skin keratinocytes |
[44] |
| PGRN | ↑ | Inflammation; skin sclerosis; fibrosis |
Human SSc dermal fibroblasts; Fli-1+/− mice; BLM-treated mice; human LSc skin lesions |
[46][47] |
| TNF-α | ↑ | Inflammation; fibrosis |
Human LSc skin lesions; | [47] |
| CXCL5 | ↓ | Vasculopathy | Human dcSSc dermal blood vessels; FLI1 silencing in HDMECs; dermal vessels of Fli1 knockout mice |
[48] |
| CXCL6 | ↑ | Tissues fibrosis; vasculopathy |
Human SSc dermal fibroblasts; FLI1 silencing in HDMECs |
[49] |
| CCL20 | ↑ | Fibrosis | Human early dcSSc | [52] |
| CCL6 | ↑ | Vasculopathy | Human SSc dermal vessels; FLI1 silencing in HDMECs |
[52] |
| EPCR | ↓ | Impaired vascular homeostasis | Human SSc dermal vessels; Fli1+/− mice; FLI1 silencing in HDMECs |
[53] |
| VE-cadherin | ↓ | Impaired vascular homeostasis | MDMECs of Fli1 CKO mice; MDMECs of Fli1+/− mice; FLI1 silencing in HDMECs |
[34] |
| PECAM-1 | ↓ | Impaired vascular homeostasis | MDMECs of Fli1 CKO mice; MDMECs of Fli1+/− mice; FLI1 silencing in HDMECs |
[34] |
| MMP-9 | ↓ | Impaired vascular homeostasis | MDMECs of Fli1 CKO mice; MDMECs of Fli1+/− mice; FLI1 silencing in HDMECs |
[34] |
| PDGF-B | ↓ | Impaired vascular homeostasis | MDMECs of Fli1 CKO mice; MDMECs of Fli1+/− mice; FLI1 silencing in HDMECs |
[34] |
| S1P1 | ↓ | Impaired vascular homeostasis | MDMECs of Fli1 CKO mice; MDMECs of Fli1+/− mice; FLI1 silencing in HDMECs |
[34] |
| Adipsin | ↑ | Vascular hypertension | Human SSc dermal vessels; FLI1 silencing in HDMECs |
[54] |
| Genetic and epigenetic factors | ||||
| (GA)n alleles | ↑ | Increased susceptibility to SSc | Human SSc peripheral blood | [56] |
| Acetylation of histones H3 and H4 in the FLI1 gene promoter | ↓ | FLI1 suppression; increased collagen synthesis | Human skin, normal and dcSSc fibroblasts | [57] |
| HDAC-1 and 6 | ↑ | FLI1 suppression | Human skin, normal and dcSSc fibroblasts | [57] |
| MBD-1 and 2, MeCP2 | ↑ | DNA methylation | Human skin, normal and dcSSc fibroblasts | [57] |
| Methylation of CpG islands in the FLI1 promoter | ↑ | FLI1 suppression; increased Collagen synthesis | Human skin, normal and dcSSc fibroblasts | [57] |
| DNMT1 | ↑ | FLI1 suppression | Human skin, normal and dcSSc fibroblasts | [33][57] |
| COL23A1, COL4A2 methylation | ↓ | Increased collagen synthesis | Human dcSSc and lcSSc dermal fibroblasts | [58] |
| ITGA9 methylation | ↓ | TGF-β upregulation | Human dcSSc and lcSSc dermal fibroblasts | [58] |
| ADAM12 methylation | ↓ | TGF-β upregulation | Human dcSSc and lcSSc dermal fibroblasts | [58] |
| miRNA-26a | ↑ | FLI1 suppression | Primary SSc skin fibroblasts | [31] |
| miRNA-21 | ↑ | TGF-β upregulation; collagen synthesis |
Human dcSSc and TGF-β treated normal fibroblasts | [59] |
| miRNA-29a | ↓ | TGF-β upregulation; collagen synthesis |
Human dcSSc and TGF-β treated normal fibroblasts | [59] |
References
- Ben-David, Y.; Giddens, E.B.; Bernstein, A. Identification and mapping of a common proviral integration site Fli-1 in erythroleukemia cells induced by Friend murine leukemia virus. Proc. Natl. Acad. Sci. USA 1990, 87, 1332–1336.
- Ben-David, Y.; Giddens, E.B.; Letwin, K.; Bernstein, A. Erythroleukemia induction by Friend murine leukemia virus: Insertional activation of a new member of the ets gene family, Fli-1, closely linked to c-ets-1. Genes Dev. 1991, 5, 908–918.
- He, Y.S.; Yang, X.K.; Hu, Y.Q.; Xiang, K.; Pan, H.F. Emerging role of Fli1 in autoimmune diseases. Int. Immunopharmacol. 2021, 90, 107127.
- Ben-David, Y.; Babu Gajendran, B.; Klarke, M.; Sample, K.M.; Zacksenhaus, E. Current insights into the role of Fli-1 in hematopoiesis and malignant transformation. Cell. Mol. Life Sci. 2022, 79, 163.
- Sato, Y. Role of ETS family transcription factors in vascular development and angiogenesis. Cell Struct. Funct. 2001, 26, 19–24.
- Ferdous, A.; Singh, S.; Luo, Y.; Abedin, M.J.; Jiang, N.; Perry, C.E.; Evers, B.M.; Gillette, T.G.; Kyba, M.; Trojanowska, M.; et al. Fli1 Promotes Vascular Morphogenesis by Regulating Endothelial Potential of Multipotent Myogenic Progenitors. Circ. Res. 2021, 129, 949–964.
- Spyropoulos, D.D.; Pharr, P.N.; Lavenburg, K.R.; Jackers, P.; Papas, T.S.; Ogawa, M.; Watson, D.K. Hemorrhage, impaired hematopoiesis, and lethality in mouse embryos carrying a targeted disruption of the Fli1 transcription factor. Mol. Cell. Biol. 2000, 20, 5643–5652.
- Asano, Y.J. What can we learn from Fli1-deficient mice, new animal models of systemic sclerosis? Scleroderma Relat. Disord. 2018, 3, 6–13.
- Pimanda, J.E.; Chan, W.Y.; Donaldson, I.J.; Bowen, M.; Green, A.R.; Göttgens, B. Endoglin expression in the endothelium is regulated by Fli-1, Erg, and Elf-1 acting on the promoter and a −8-kb enhancer. Blood 2006, 107, 4737–4745.
- Le Bras, A.; Samson, C.; Trentini, M.; Caetano, B.; Lelievre, E.; Mattot, V.; Beermann, F.; Soncin, F. VE-statin/egfl7 expression in endothelial cells is regulated by a distal enhancer and a proximal promoter under the direct control of Erg and GATA-2. PLoS ONE 2010, 5, e12156.
- Soncin, F.; Mattot, V.; Lionneton, F.; Spruyt, N.; Lepretre, F.; Begue, A.; Stehelin, D. VE-statin, an endothelial repressor of smooth muscle cell migration. EMBO J. 2003, 22, 5700–5711.
- Lelièvre, E.; Lionneton, F.; Mattot, V.; Spruyt, N.; Soncin, F. Ets-1 regulates fli-1 expression in endothelial cells. Identification of ETS binding sites in the fli-1 gene promoter. J. Biol. Chem. 2002, 277, 25143–25151.
- Li, L.; Yu, J.; Cheng, S.; Peng, Z.; Luo, H. Transcription factor Fli-1 as a new target for antitumor drug development. Int. J. Biol. Macromol. 2022, 209 Pt A, 1155–1168.
- Gargallo, P.; Yáñez, Y.; Juan, A.; Segura, V.; Balaguer, J.; Torres, B.; Oltra, S.; Castel, V.; Cañete, A. Review: Ewing Sarcoma Predisposition. Pathol. Oncol. Res. 2020, 26, 2057–2066.
- Qian, C.; Li, D.; Chen, Y. ETS factors in prostate cancer. Cancer Lett. 2022, 530, 181–189.
- Elkareh, J.; Periyasamy, S.M.; Shidyak, A.; Vetteth, S.; Schroeder, J.; Raju, V.; Hariri, I.M.; El-Okdi, N.; Gupta, S.; Fedorova, L.; et al. Marinobufagenin induces increases in procollagen expression in a process involving protein kinase C and Fli-1: Implications for uremic cardiomyopathy. Am. J. Physiol. Renal Physiol. 2009, 296, F1219–F1226.
- Agalakova, N.I.; Kolodkin, N.I.; Adair, C.D.; Trashkov, A.P.; Bagrov, A.Y. Preeclampsia: Cardiotonic Steroids, Fibrosis, Fli1 and Hint to Carcinogenesis. Int. J. Mol. Sci. 2021, 22, 1941.
- Toyama, T.; Asano, Y.; Miyagawa, T.; Nakamura, K.; Hirabayashi, M.; Yamashita, T.; Saigusa, R.; Miura, S.; Ichimura, Y.; Takahashi, T.; et al. The impact of transcription factor Fli1 deficiency on the regulation of angiogenesis. Exp. Dermatol. 2017, 26, 912–918.
- Asano, Y. Epigenetic suppression of Fli1, a potential predisposing factor in the pathogenesis of systemic sclerosis. Int. J. Biochem. Cell Biol. 2015, 67, 86–91.
- Fioretto, B.S.; Rosa, I.; Romano, E.; Wang, Y.; Guiducci, S.; Zhang, G.; Manetti, M.; Matucci-Cerinic, M. The contribution of epigenetics to the pathogenesis and gender dimorphism of systemic sclerosis: A comprehensive overview. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X20918456.
- Yu, J.; Tang, R.; Ding, K. Epigenetic Modifications in the Pathogenesis of Systemic Sclerosis. Int. J. Gen. Med. 2022, 15, 3155–3166.
- Kowalska-Kępczyńska, A.J. Systemic Scleroderma-Definition, Clinical Picture and Laboratory Diagnostics. Clin. Med. 2022, 11, 2299.
- Rudnik, M.; Hukara, A.; Kocherova, I.; Jordan, S.; Schniering, J.; Milleret, V.; Ehrbar, M.; Klingel, K.; Feghali-Bostwick, C.; Distler, O.; et al. Elevated Fibronectin Levels in Profibrotic CD14+ Monocytes and CD14+ Macrophages in Systemic Sclerosis. Front. Immunol. 2021, 12, 642891.
- Bhattacharyya, S.; Midwood, K.S.; Varga, J. Tenascin-C in fibrosis in multiple organs: Translational implications. Semin. Cell Dev. Biol. 2022, 128, 130–136.
- Czuwara-Ladykowska, J.; Shirasaki, F.; Jackers, P.; Watson, D.K.; Trojanowska, M.J. Fli-1 inhibits collagen type I production in dermal fibroblasts via an Sp1-dependent pathway. Biol. Chem. 2001, 276, 20839–20848.
- Manetti, M. Fli1 deficiency and beyond: A unique pathway linking peripheral vasculopathy and dermal fibrosis in systemic sclerosis. Exp. Dermatol. 2015, 24, 256–257.
- Takahashi, T.; Asano, Y.; Sugawara, K.; Yamashita, T.; Nakamura, K.; Saigusa, R.; Ichimura, Y.; Toyama, T.; Taniguchi, T.; Akamata, K.; et al. Epithelial Fli1 deficiency drives systemic autoimmunity and fibrosis: Possible roles in scleroderma. J. Exp. Med. 2017, 214, 1129–1151.
- Asano, Y.J. The Pathogenesis of Systemic Sclerosis: An Understanding Based on a Common Pathologic Cascade across Multiple Organs and Additional Organ-Specific Pathologies. Clin. Med. 2020, 9, 2687.
- Kubo, M.; Czuwara-Ladykowska, J.; Moussa, O.; Markiewicz, M.; Smith, E.; Silver, R.M.; Jablonska, S.; Blaszczyk, M.; Watson, D.K.; Trojanowska, M. Persistent down-regulation of Fli1, a suppressor of collagen transcription, in fibrotic scleroderma skin. Am. J. Pathol. 2003, 163, 571–581.
- Miura, S.; Watanabe, Y.; Saigusa, R.; Yamashita, T.; Nakamura, K.; Hirabayashi, M.; Miyagawa, T.; Yoshizaki, A.; Trojanowska, M.; Sato, S.; et al. Fli1 deficiency suppresses RALDH1 activity of dermal dendritic cells and related induction of regulatory T cells: A possible role in scleroderma. Arthritis Res. Ther. 2021, 23, 137.
- Cheng, Z.; Zhang, J.; Deng, W.; Lin, S.; Li, D.; Zhu, K.; Qi, Q. Bushen Yijing Decoction (BSYJ) exerts an anti-systemic sclerosis effect via regulating MicroRNA-26a/FLI1 axis. Bioengineered 2021, 12, 1212–1225.
- Nakerakanti, S.S.; Kapanadze, B.; Yamasaki, M.; Markiewicz, M.; Trojanowska, M. Fli1 and Ets1 have distinct roles in connective tissue growth factor/CCN2 gene regulation and induction of the profibrotic gene program. J. Biol. Chem. 2006, 281, 25259–25269.
- Bujor, A.M.; Haines, P.; Padilla, C.; Christmann, R.B.; Junie, M.; Sampaio-Barros, P.D.; Lafyatis, R.; Trojanowska, M. Ciprofloxacin has antifibrotic effects in scleroderma fibroblasts via downregulation of Dnmt1 and upregulation of Fli1. Int. J. Mol. Med. 2012, 30, 1473–1480.
- Asano, Y.; Stawski, L.; Hant, F.; Highland, K.; Silver, R.; Szalai, G.; Watson, D.K.; Trojanowska, M. Endothelial Fli1 deficiency impairs vascular homeostasis: A role in scleroderma vasculopathy. Am. J. Pathol. 2010, 176, 1983–1998.
- Akamata, K.; Asano, Y.; Taniguchi, T.; Yamashita, T.; Saigusa, R.; Nakamura, K.; Noda, S.; Aozasa, N.; Toyama, T.; Takahashi, T.; et al. Increased expression of chemerin in endothelial cells due to Fli1 deficiency may contribute to the development of digital ulcers in systemic sclerosis. Rheumatology 2015, 54, 1308–1316.
- Omatsu, J.; Saigusa, R.; Miyagawa, T.; Fukui, Y.; Toyama, S.; Awaji, K.; Ikawa, T.; Norimatsu, Y.; Yoshizaki, A.; Sato, S.; et al. Serum S100A12 levels: Possible association with skin sclerosis and interstitial lung disease in systemic sclerosis. Exp. Dermatol. 2021, 30, 409–415.
- Jinnin, M.; Ihn, H.; Yamane, K.; Mimura, Y.; Asano, Y.; Tamaki, K. Alpha2(I) collagen gene regulation by protein kinase C signaling in human dermal fibroblasts. Nucleic Acids Res. 2005, 33, 1337–1351.
- Asano, Y.; Czuwara, J.; Trojanowska, M. Transforming growth factor-beta regulates DNA binding activity of transcription factor Fli1 by p300/CREB-binding protein-associated factor-dependent acetylation. J. Biol. Chem. 2007, 282, 34672–34683.
- Asano, Y.; Trojanowska, M. Phosphorylation of Fli1 at threonine 312 by protein kinase C delta promotes its interaction with p300⁄CREB-binding protein-associated factor and subsequent acetylation in response to transforming growth factor beta. Mol. Cell. Biol. 2009, 29, 1882–1894.
- Bujor, A.M.; Asano, Y.; Haines, P.; Lafyatis, R.; Trojanowska, M. The c-Abl tyrosine kinase controls protein kinase Cδ-induced Fli-1 phosphorylation in human dermal fibroblasts. Arthritis Rheum. 2011, 63, 1729–1737.
- Noda, S.; Asano, Y.; Akamata, K.; Aozasa, N.; Taniguchi, T.; Takahashi, T.; Ichimura, Y.; Toyama, T.; Sumida, H.; Yanaba, K.; et al. Constitutive activation of c-Abl/protein kinase C-δ/Fli1 pathway in dermal fibroblasts derived from patients with localized scleroderma. Br. J. Dermatol. 2012, 167, 1098–1105.
- Akamata, K.; Asano, Y.; Aozasa, N.; Noda, S.; Taniguchi, T.; Takahashi, T.; Ichimura, Y.; Toyama, T.; Sato, S. Bosentan reverses the pro-fibrotic phenotype of systemic sclerosis dermal fibroblasts via increasing DNA binding ability of transcription factor Fli1. Arthritis Res. Ther. 2014, 16, R86.
- Noda, S.; Asano, Y.; Akamata, K.; Aozasa, N.; Taniguchi, T.; Takahashi, T.; Ichimura, Y.; Toyama, T.; Sumida, H.; Yanaba, K.; et al. A possible contribution of altered cathepsin B expression to the development of skin sclerosis and vasculopathy in systemic sclerosis. PLoS ONE 2012, 7, e32272.
- Noda, S.; Asano, Y.; Takahashi, T.; Akamata, K.; Aozasa, N.; Taniguchi, T.; Ichimura, Y.; Toyama, T.; Sumida, H.; Kuwano, Y.; et al. Decreased cathepsin V expression due to Fli1 deficiency contributes to the development of dermal fibrosis and proliferative vasculopathy in systemic sclerosis. Rheumatology 2013, 52, 790–799.
- Yamashita, T.; Asano, Y.; Taniguchi, T.; Nakamura, K.; Saigusa, R.; Takahashi, T.; Ichimura, Y.; Toyama, T.; Yoshizaki, A.; Miyagaki, T.; et al. A potential contribution of altered cathepsin L expression to the development of dermal fibrosis and vasculopathy in systemic sclerosis. Exp. Dermatol. 2016, 25, 287–292.
- Ichimura, Y.; Asano, Y.; Akamata, K.; Noda, S.; Taniguchi, T.; Takahashi, T.; Toyama, T.; Tada, Y.; Sugaya, M.; Sato, S.; et al. Progranulin Overproduction Due to Fli-1 Deficiency Contributes to the Resistance of Dermal Fibroblasts to Tumor Necrosis Factor in Systemic Sclerosis. Arthritis Rheumatol. 2015, 67, 3245–3255.
- Miyagawa, T.; Ichimura, Y.; Nakamura, K.; Hirabayashi, M.; Yamashita, T.; Saigusa, R.; Miura, S.; Takahashi, T.; Toyama, T.; Taniguchi, T.; et al. Progranulin overproduction due to constitutively activated c-Abl/PKC-δ/Fli1 pathway contributes to the resistance of dermal fibroblasts to the anti-fibrotic effect of tumor necrosis factor-α in localized scleroderma. Dermatol. Sci. 2018, 92, 207–214.
- Ichimura, Y.; Asano, Y.; Akamata, K.; Takahashi, T.; Noda, S.; Taniguchi, T.; Toyama, T.; Aozasa, N.; Sumida, H.; Kuwano, Y.; et al. Fli1 deficiency contributes to the suppression of endothelial CXCL5 expression in systemic sclerosis. Arch. Dermatol. Res. 2014, 306, 331–338.
- Taniguchi, T.; Asano, Y.; Nakamura, K.; Yamashita, T.; Saigusa, R.; Ichimura, Y.; Takahashi, T.; Toyama, T.; Yoshizaki, A.; Sato, S. Fli1 Deficiency Induces CXCL6 Expression in Dermal Fibroblasts and Endothelial Cells, Contributing to the Development of Fibrosis and Vasculopathy in Systemic Sclerosis. J. Rheumatol. 2017, 44, 1198–1205.
- Taniguchi, T.; Miyagawa, T.; Toyama, S.; Yamashita, T.; Nakamura, K.; Saigusa, R.; Ichimura, Y.; Takahashi, T.; Toyama, T.; Yoshizaki, A.; et al. CXCL13 produced by macrophages due to Fli1 deficiency may contribute to the development of tissue fibrosis, vasculopathy and immune activation in systemic sclerosis. Exp. Dermatol. 2018, 27, 1030–1037.
- Jiang, Z.; Chen, C.; Yang, S.; He, H.; Zhu, X.; Liang, M. Contribution to the peripheral vasculopathy and endothelial cell dysfunction by CXCL4 in Systemic Sclerosis. J. Dermatol. Sci. 2021, 104, 63–73.
- Ikawa, T.; Miyagawa, T.; Fukui, Y.; Toyama, S.; Omatsu, J.; Awaji, K.; Norimatsu, Y.; Watanabe, Y.; Yoshizaki, A.; Sato, S.; et al. Endothelial CCR6 expression due to FLI1 deficiency contributes to vasculopathy associated with systemic sclerosis. Arthritis Res. Ther. 2021, 23, 283.
- Saigusa, R.; Asano, Y.; Yamashita, T.; Taniguchi, T.; Takahashi, T.; Ichimura, Y.; Toyama, T.; Yoshizaki, A.; Miyagaki, T.; Sugaya, M.; et al. Fli1 deficiency contributes to the downregulation of endothelial protein C receptor in systemic sclerosis: A possible role in prothrombotic conditions. Br. J. Dermatol. 2016, 174, 338–347.
- Miyagawa, T.; Taniguchi, T.; Saigusa, R.; Fukayama, M.; Takahashi, T.; Yamashita, T.; Hirabayashi, M.; Miura, S.; Nakamura, K.; Yoshizaki, A.; et al. Fli1 deficiency induces endothelial adipsin expression, contributing to the onset of pulmonary arterial hypertension in systemic sclerosis. Rheumatology 2020, 59, 2005–2015.
- Mayes, M.D.; Trojanowska, M. Genetic factors in systemic sclerosis. Arthritis Res. Ther. 2007, 9, S5.
- Yamashita, K.; Kawasaki, A.; Matsushita, T.; Furukawa, H.; Kondo, Y.; Okiyama, N.; Nagaoka, S.; Shimada, K.; Sugii, S.; Katayama, M.; et al. Association of functional (GA)n microsatellite polymorphism in the FLI1 gene with susceptibility to human systemic sclerosis. Rheumatology 2020, 59, 3553–3562.
- Wang, Y.; Fan, P.S.; Kahaleh, B. Association between enhanced type I collagen expression and epigenetic repression of the FLI1 gene in scleroderma fibroblasts. Arthritis Rheum. 2006, 54, 2271–2279.
- Altorok, N.; Tsou, P.S.; Coit, P.; Khanna, D.; Sawalha, A.H. Genome-wide DNA methylation analysis in dermal fibroblasts from patients with diffuse and limited systemic sclerosis reveals common and subset-specific DNA methylation aberrancies. Ann. Rheum. Dis. 2015, 74, 1612–1620.
- Jafarinejad-Farsangi, S.; Gharibdoost, F.; Farazmand, A.; Kavosi, H.; Jamshidi, A.; Karimizadeh, E.; Noorbakhsh, F.; Mahmoudi, M. MicroRNA-21 and microRNA-29a modulate the expression of collagen in dermal fibroblasts of patients with systemic sclerosis. Autoimmunity 2019, 52, 108–116.
- Maurer, B.; Stanczyk, J.; Jüngel, A.; Akhmetshina, A.; Trenkmann, M.; Brock, M.; Kowal-Bielecka, O.; Gay, R.E.; Michel, B.A.; Distler, J.H.; et al. MicroRNA-29, a key regulator of collagen expression in systemic sclerosis. Arthritis Rheum. 2010, 62, 1733–1743.
- Makino, K.; Jinnin, M.; Hirano, A.; Yamane, K.; Eto, M.; Kusano, T.; Honda, N.; Kajihara, I.; Makino, T.; Sakai, K.; et al. The downregulation of miR-let-7a contributes to the excessive expression of type I collagen in systemic and localized scleroderma. J. Immunol. 2013, 190, 3905–3915.
- Makino, T.; Jinnin, M.; Etoh, M.; Yamane, K.; Kajihara, I.; IMakino, H.; Ichihara, A.; Igata, T.; Sakai, K.; Fukushima, S.; et al. Downregulation of microRNA-196a in the sera and involved skin of localized scleroderma patients. Eur. J. Dermatol. 2014, 24, 470–476.
- O’Reilly, S.; Ciechomska, M.; Fullard, N.; Przyborski, S.; van Laar, J.M. IL-13 mediates collagen deposition via STAT6 and microRNA-135b: A role for epigenetics. Sci. Rep. 2016, 6, 25066.
- Garikapati, K.; Goh, D.; Khanna, S.; Echampati, K. Uraemic Cardiomyopathy: A Review of Current Literature. Clin. Med. Insights Cardiol. 2021, 15, 1179546821998347.
- Zhang, L.; Eddy, A.; Teng, Y.T.; Fritzler, M.; Kluppel, M.; Melet, F.; Bernstein, A. An immunological renal disease in transgenic mice that overexpress Fli-1, a member of the ets family of transcription factor genes. Mol. Cell. Biol. 1995, 15, 6961–6970.
- Kennedy, D.J.; Vetteth, S.; Periyasamy, S.M.; Kanj, M.; Fedorova, L.; Khouri, S.; Kahaleh, M.B.; Xie, Z.; Malhotra, D.; Kolodkin, N.I.; et al. Central role for the cardiotonic steroid marinobufagenin in the pathogenesis of experimental uremic cardiomyopathy. Hypertension 2006, 47, 488–495.
- Elkareh, J.; Kennedy, D.J.; Yashaswi, B.; Vetteth, S.; Shidyak, A.; Kim, E.G.; Smaili, S.; Periyasamy, S.M.; Hariri, I.M.; Fedorova, L.; et al. Marinobufagenin stimulates fibroblast collagen production and causes fibrosis in experimental uremic cardiomyopathy. Hypertension 2007, 49, 215–224.
- Haller, S.T.; Kennedy, D.J.; Shidyak, A.; Budny, G.V.; Malhotra, D.; Fedorova, O.V.; Shapiro, J.I.; Bagrov, A.Y. Monoclonal antibody against marinobufagenin reverses cardiac fibrosis in rats with chronic renal failure. Am. J. Hypertens. 2012, 25, 690–696.
- Reznik, V.A.; Kashkin, V.A.; Agalakova, N.I.; Adair, C.D.; Bagrov, A.Y. Endogenous Bufadienolides, Fibrosis and Preeclampsia. Cardiol. Res. Pract. 2019, 2019, 5019287.
- Dennehy, N.; Lees, C. Preeclampsia: Maternal cardiovascular function and optimising outcomes. Early Hum. Dev. 2022, 174, 105669.
- Tossetta, G.; Fantone, S.; Muti, N.D.; Balercia, G.; Ciavattini, A.; Giannubilo, S.R.; Marzioni, D. Preeclampsia and severe acute respiratory syndrome coronavirus 2 infection: A systematic review. J. Hypertens. 2022, 40, 629–1638.
- Opichka, M.A.; Rappelt, M.W.; Gutterman, D.D.; Grobe, J.L.; McIntosh, J.J. Vascular Dysfunction in Preeclampsia. Cells 2021, 10, 3055.
- Nikitina, E.R.; Mikhailov, A.V.; Nikandrova, E.S.; Frolova, E.V.; Fadeev, A.V.; Shman, V.V.; Shilova, V.Y.; Tapilskaya, N.I.; Shapiro, J.I.; Fedorova, O.V.; et al. In preeclampsia endogenous cardiotonic steroids induce vascular fibrosis and impair relaxation of umbilical arteries. J. Hypertens. 2011, 29, 769–776.
- Fedorova, O.V.; Ishkaraeva, V.V.; Grigorova, Y.N.; Reznik, V.A.; Kolodkin, N.I.; Zazerskaya, I.E.; Zernetkina, V.; Agalakova, N.I.; Tapilskaya, N.I.; Adair, C.D.; et al. Antibody to Marinobufagenin Reverses Placenta-Induced Fibrosis of Umbilical Arteries in Preeclampsia. Int. J. Mol. Sci. 2018, 19, 2377.
- Agalakova, N.I.; Grigorova, Y.N.; Ershov, I.A.; Reznik, V.A.; Mikhailova, E.V.; Nadei, O.V.; Samuilovskaya, L.; Romanova, L.A.; Adair, C.D.; Romanova, I.V.; et al. Canrenone Restores Vasorelaxation Impaired by Marinobufagenin in Human Preeclampsia. Int. J. Mol. Sci. 2022, 23, 3336.
- Agalakova, N.I.; Reznik, V.A.; Nadei, O.V.; Ershov, I.A.; Rassokha, O.S.; Vasyutina, M.L.; Ivanov, D.O.; Adair, C.D.; Galagudza, M.M.; Bagrov, A.Y. Antibody against Na/K-ATPase Inhibitor Lowers Blood Pressure and Increases Vascular Fli1 in Experimental Preeclampsia. Am. J. Hypertens. 2020, 33, 514–519.
- Agalakova, N.I.; Reznik, V.A.; Ershov, I.A.; Lupanova, E.A.; Nadei, O.V.; Ivanov, D.O.; Adair, C.D.; Bagrov, A.Y. Silencing of Fli1 Gene Mimics Effects of Preeclampsia and Induces Collagen Synthesis in Human Umbilical Arteries. Am. J. Hypertens. 2022, 35, 828–832.
- Kolmakova, E.V.; Haller, S.T.; Kennedy, D.J.; Isachkina, A.N.; Budny, G.V.; Frolova, E.V.; Nikitina, E.R.; Piecha, G.; Malhotra, D.; Fedorova, O.V.; et al. Endogenous cardiotonic steroids in chronic renal failure. Nephrol. Dial. Transplant. 2011, 26, 2912–2919.
- Fedorova, O.V.; Fadeev, A.V.; Grigorova, Y.N.; Agalakova, N.I.; Konradi, A.O.; Bagrov, A.Y. Marinobufagenin induces vascular fibrosis via a pressure-independent mechanism in NaCl-loaded diabetic rats. J. Cardiovasc. Pharmacol. 2019, 74, 436–442.
- Zhang, Y.; Wei, W.; Shilova, V.; Petrashevskaya, N.N.; Zernetkina, V.I.; Grigorova, Y.N.; Marshall, C.A.; Fenner, R.C.; Lehrmann, E.; Wood, W.H., III; et al. Monoclonal Antibody to Marinobufagenin Downregulates TGFβ Profibrotic Signaling in Left Ventricle and Kidney and Reduces Tissue Remodeling in Salt-Sensitive Hypertension. J. Am. Heart Assoc. 2019, 8, e012138.
- Grigorova, Y.N.; Juhasz, O.; Zernetkina, V.; Fishbein, K.W.; Fedorova, O.V.; Bagrov, A.Y. Monoclonal antibody to an endogenous sodium pump inhibitor marinobufagenin reverses aortic remodeling and stiffness in normotensive rats on a high salt intake. Am. J. Hypertens. 2016, 29, 641–646.


