Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Elisabetta Di Profio | -- | 2800 | 2022-09-27 15:59:05 | | | |
| 2 | Lindsay Dong | Meta information modification | 2800 | 2022-09-28 03:38:34 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Profio, E.D.; Magenes, V.C.; Fiore, G.; Agostinelli, M.; Mendola, A.L.; Acunzo, M.; Francavilla, R.; Indrio, F.; Bosetti, A.; D’auria, E.; et al. Impact of Special Diets on Infants Gut Microbiome. Encyclopedia. Available online: https://encyclopedia.pub/entry/27721 (accessed on 27 June 2026).
Profio ED, Magenes VC, Fiore G, Agostinelli M, Mendola AL, Acunzo M, et al. Impact of Special Diets on Infants Gut Microbiome. Encyclopedia. Available at: https://encyclopedia.pub/entry/27721. Accessed June 27, 2026.
Profio, Elisabetta Di, Vittoria Carlotta Magenes, Giulia Fiore, Marta Agostinelli, Alice La Mendola, Miriam Acunzo, Ruggiero Francavilla, Flavia Indrio, Alessandra Bosetti, Enza D’auria, et al. "Impact of Special Diets on Infants Gut Microbiome" Encyclopedia, https://encyclopedia.pub/entry/27721 (accessed June 27, 2026).
Profio, E.D., Magenes, V.C., Fiore, G., Agostinelli, M., Mendola, A.L., Acunzo, M., Francavilla, R., Indrio, F., Bosetti, A., D’auria, E., Borghi, E., Zuccotti, G., & Verduci, E. (2022, September 27). Impact of Special Diets on Infants Gut Microbiome. In Encyclopedia. https://encyclopedia.pub/entry/27721
Profio, Elisabetta Di, et al. "Impact of Special Diets on Infants Gut Microbiome." Encyclopedia. Web. 27 September, 2022.
Copy Citation
Gut microbiota is a complex system that starts to take shape early in life. Several factors influence the rise of microbial gut colonization, such as term and mode of delivery, exposure to antibiotics, maternal diet, presence of siblings and family members, pets, genetics, local environment, and geographical location. Breastfeeding, complementary feeding, and later dietary patterns during infancy and toddlerhood are major players in the proper development of microbial communities. Nonetheless, if dysbiosis occurs, gut microbiota may remain impaired throughout life, leading to deleterious consequences, such as greater predisposition to non-communicable diseases, more susceptible immune system and altered gut–brain axis.
gut microbiota
infants
standard diets
special diets
1. Introduction
Gut microbiota is a complex community of microorganisms that live in the gastrointestinal (GI) tract of humans and animals [1][2]. Gut microbiota consists of more than 1500 species, distributed in more than 50 different phyla [3]. The most abundant phyla were reported to be Bacteroidetes and Firmicutes, followed by Proteobacteria, Fusobacteria, Tenericutes, Actinobacteria, and Verrucomicrobia, which make up to 90% of the total microbial population in humans [2][4]. Concerning diversity, the developing infant microbiota progressively undergoes an increase in within-individual diversity (the so-called alpha diversity) and a decrease in between-individual diversity (beta diversity) [5][6][7]. Several factors influence the rise of microbial gut colonization, such as term and mode of birth, exposure to antibiotics, presence of pets, siblings and family members, genetics, local environment, geographical location, and maternal and infant/toddler diet, with diet being a major player [5][8][9]. Nevertheless, the pivotal colonization event occurs at birth. The newborn external body surfaces and GI tract are then rapidly colonized by several microorganisms, reaching up to 108 microorganisms per gram of feces in hours to days [10]. Over weeks to months, this number increases, reaching 1011–1012 [5][11], values that are comparable to the adult microbial densities [12].
As the infant gets older, their exposure to new microbes increases, but the influence of these exposures to the microbial gut composition decreases [5]. Extensive research has focused on dietetic influence on microbiota, specifically on breast milk versus formulas, whereas much less is known about the effects of complementary feeding on microbiota composition [13]. Around 4–6 months of age, infants pass from exclusive milk-feeding to eating family foods, usually referred to as the complementary feeding (CF) period [14].
Dietary fibers and incompletely digested proteins are the main sources of energy for microbes that reside in the gut, and tare he most involved in shaping the microbial composition [13]. The main end products of dietary fiber fermentation are the short chain fatty acids (SCFAs) (i.e., acetate, propionate, and butyrate) [15]. SCFAs influence intestinal barrier function, metabolism, immune and nervous systems [8][16].
2. Gut Microbiota in Infants and Toddlers under Standard Diets
2.1. Breast Milk vs. Formula Milk and Gut Microbiota
Breast milk, composed of lactose, lipids, proteins, and more than 200 different human milk oligosaccharides (HMOs) [17], is recommended as the first nutrition during infancy, providing all the necessary nutrients to support growth and development [18][19][20]. HMOs are not hydrolyzed by gastrointestinal saccharolytic enzymes; thus, they reach the colon intact, where they serve as metabolic substrates for gut bifidobacteria [8]. Some bifidobacterial species (e.g., B. bifidum, B. breve and subsp. infantis) possess specific membrane transporters and saccharolytic enzymes that are capable of cleaving and internalizing HMOs, producing lactate, acetate, formate, and 1,2-propanediol [21]. The end products of HMOs’ metabolism have potential beneficial host-health effects. Indeed, acetate and lactate have been reported to suppress the growth of opportunistic pathogens belonging to Clostridiaceae, Enterobacteriaceae, and Staphylococcaceae [8][22]. The lack of Bifidobacterium spp. has been instead associated with immune dysregulation [23], asthma [24], and autoimmune diseases [25]. Interestingly, Alcon-Giner et al. conducted a longitudinal study to evaluate the gut microbiota composition in two groups of preterm infants (101 orally supplemented with Bifidobacterium and Lactobacillus -Bif/Lacto- species and 133 non-supplemented). They observed enrichment in Bifidobacterium and a lower abundance of opportunistic pathogens in the Bif/Lacto group [26]. Moreover, fecal acetate positively correlated with Bifidobacterium relative abundance [26].
Overall, HMO and lactose promote the GI microbiota development and stimulated the infant immune system through growth factors, cytokines and immunoglobulins, with a positive impact on growth, neurodevelopment and metabolism [27].
Exclusively formula-fed (FF) infants possess different microbiota, characterized by a lower abundance of HMO-utilizing Bifidobacterium species and increased Clostridium species (e.g., C. difficile and C. perfringens) and Enterobacteriaceae (e.g., Escherichia coli) [28][29]. These observations seem to correlate with the lack of HMOs and the higher protein content in milk formulas [8]. Recently, Berger et al., in a double-blinded randomized controlled trial, evaluated whether supplementation of infant formula with HMOs, (specifically 2′-fucosyl-lactose-2′FL- and lacto-N-neotetraose-LNnT) could influence the gut microbiota [30]. Notably, recent studies have evaluated the effect of infant formula supplemented with synthetic HMOs (e.g., 2′FL and LNnT) in order to mimic a BF-like gut metabolism and microbial colonization [31]. Moreover, the researchers compared HMO-supplemented and un-supplemented formula groups with BF infants [30][32]. The intervention group led to a microbiota pattern that was more similar to that of the breast-fed (BF) infants, with higher levels of Bifidobacterium spp. and a lower relative abundance of Clostridiaceae and Enterobacteriaceae, compared with infants fed with un-supplemented formula [30].
Many infant formulas are, nowadays, supplemented with fructo-oligo-saccharides (FOS) and/or galacto-oligosaccharides (GOS), although these are not selected as maternal HMOs as they can be utilized by most Bifidobacterium species (e.g., B. adolescentis and B. catenulatum, typical of adulthood) [28][29]. Studies comparing the fecal metabolome in exclusively BF and exclusively FF infants (even when the formula contains galacto-oligosaccharides) show that proteolytic rather than saccharolytic metabolism dominates in the FF gut [33][34]. Indeed, in BF infants, remnants of HMO metabolism are mainly present, while in FF infants, the main observed products are derived from protein fermentation [33][34]. Thus, the authors evaluated the intestinal fermentation capability, which might be influenced by early diet [33]. The different fecal microbiota were also related to the differences in the fecal water % and in the concentration of microbial by-products in the stool [33]. In FF infants, limited oligosaccharides and high protein levels were present [33]. The difference in terms of fecal microbial taxonomic profiles of the milk fat globule membrane (MFGM) supplemented with experimental formula (EF) and standard formula (SF) was moderate, with respect to the difference between BF and FF infants [33]. However, to confirm these results, further studies are needed.
In conclusion, breastfeeding, mainly due to the presence of HMOs, promotes the colonization of beneficial bifidobacteria and is able to support immune system development and to prevent infections, as depicted in Figure 1 [8][22][35][36][37]. On the contrary, milk formulas have been correlated to the growth of opportunistic pathogens and to proteolytic gut metabolism, potentially causing adverse health effects [38][39][40][41].
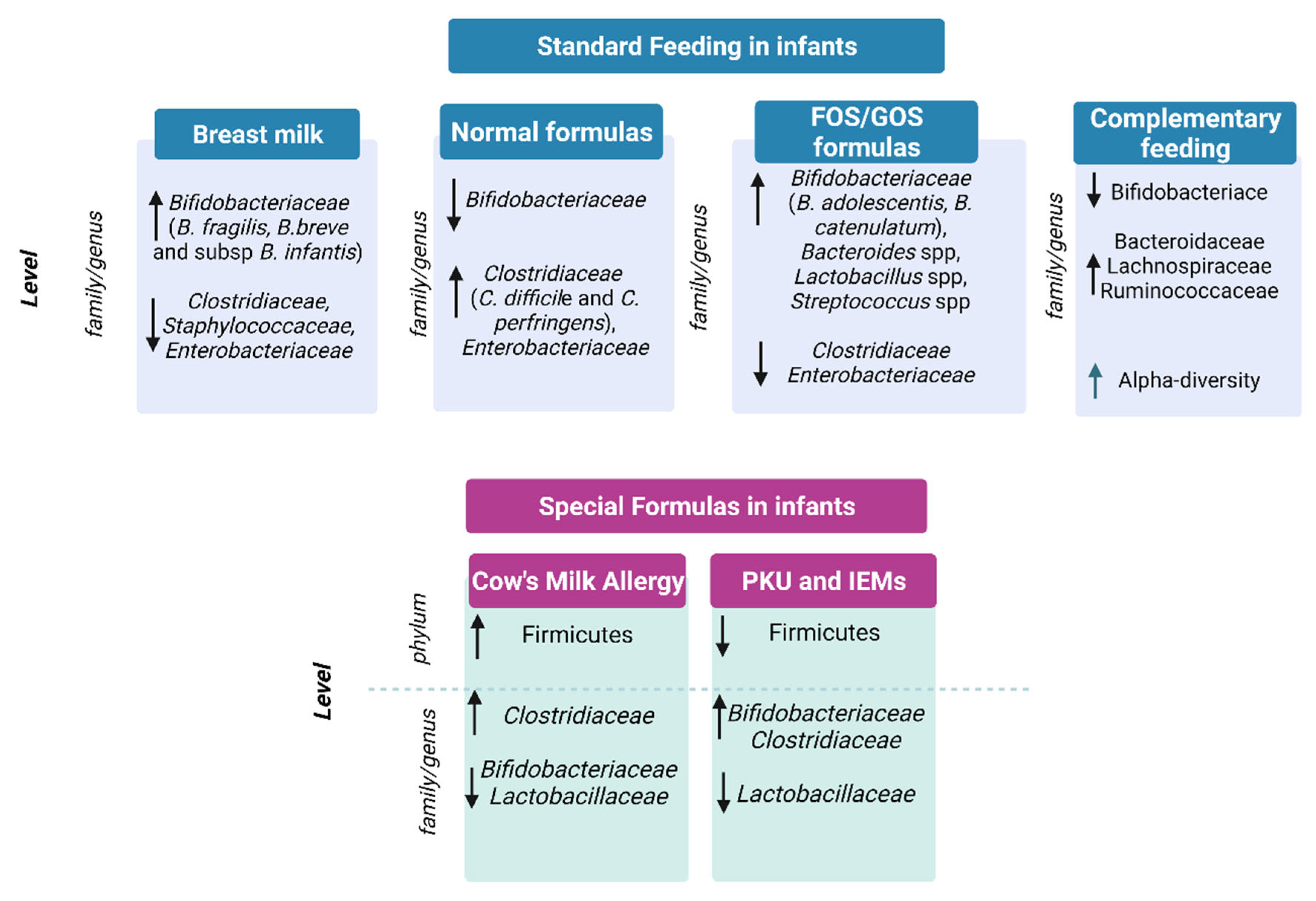
Figure 1. Gut microbiota in standard feeding vs. special formula-fed infants. ↓= decrease in family/genus or phylum; ↑ = increase in genus/family or phylum.
2.2. Gut Microbiota and Complementary Feeding
Complementary feeding is a period characterized by a shift from an exclusive milk diet to a mixed diet, including food consumption and it goes along with a phase of remarkable changes in the gut microbiota, of which the most relevant is the rapid decline in HMO-degrading Bifidobacterium species [42]. Moreover, alpha diversity increases and higher levels of Bacteroidaceae, Lachnospiraceae, and Ruminococcaceae species are present. This mirrors the higher diversity and complexity of the diet, due to the introduction of fibers (from fruits, vegetables and cereals) and new protein sources (as meats, dairy products, and legumes) [8][13].
Coherently, Differding et al. associated Bilophila wadsworthia and Roseburia spp. with early complementary feeding practice (e.g., consumption of solids or non-water/formula liquids at or before 3 months) [43]. Leong et al., in a randomized controlled trial, compared the gut microbiota composition of children weaned with a “baby-led” approach of complementary feeding with traditional spoon-fed infants [44]. The baby-led weaning approach was associated with lower alpha diversity and lower levels of Lachnospiraceae (Roseburia facies and Eubacterium rectale) and Ruminococcaceae (Faecalibacterium prausnitzii) [44]. The multinational European INFABIO study (n = 605 infants) found that early introduction of complementary foods was associated with a decrease in bifidobacteria (sp. unknown) [45]. Specifically, the study confirmed that the initial feeding method influenced the relative abundance of the Clostridium leptum group, Clostridioides difficile and C perfringens, and bifidobacteria dominated the feces of initially breast-fed infants [45].
Some complementary foods, such as rye bread, cheese, and meat products, have been specifically correlated to this increase in diversification of the infant gut microbiota [46]. Importantly, complementary feeding progression has also been correlated to higher levels of several Lachnospiraceae and Ruminococcaceae, and to a lower abundance in Bifidobacterium spp. [13]. This underlines the transition from a bifidobacteria-rich gut community toward a more diverse gut microbial community, rich in butyrate-, propionate-, and BCFA-producing bacteria [13].
Concerning the different food introduced, meat causes significantly increased levels of genera that belong to Lachnospiraceae, which are potential short-chain fatty acid producers with respect to dairy [47]. Recently, a comparison between refined grain cereal products and whole grain cereal products as the first complementary food showed a significant increase in Bacteroides and Lachnoclostridium (Lachnospiraceae family) and a decrease in Escherichia (Enterobacteriaceae family) in the whole grain cereal group [46].
3. Gut Microbiota in Infants under Special Diets
3.1. Special Formulas for the Treatment of Cow’s Milk Allergy
Cow’s milk protein allergy (CMA) is the most common food allergy in the pediatric population [48]. The use of extensively hydrolyzed formulas (eHF) is recommended as the first choice for the treatment of infants and children with confirmed CMA [49]. Amino acid-based formulas (AAFs) are also available and are considered the safest dietary strategy for infants with severe CMA [50][51]. Hydrolyzed formulas minimize antigen contact compared to whole-protein formulas, but due to the presence of sparse small peptide fragments, it also may favor immune tolerance by different mechanisms, acting on barrier reinforcement, neuro-immune pathways, and on the resident microbial community [52]. Indeed, the peptides derived from protein hydrolysates can act locally in the gut, modulating the microbiota. Dysbiosis induces functional alterations that result in aberrant Th2 responses toward an allergic, rather than a tolerogenic, response [53]. Conversely, recent data suggest that the use of AAF, the only totally non-allergenic formulas, exclusively providing nitrogen equivalent proteins as free amino acids, may delay the acquisition of immune tolerance [54], since they are completely devoid of allergenic antigenic epitopes [49][55]. Paparo et al. showed the absence of AAF-related effects on the intestinal barrier, Th1/Th2 cytokine response, and regulatory T cells (Treg) activation in vitro [56]. The onset of oral tolerance occurs during the critical early stages of immune development and it depends not only on genetic factors, but also on environmental factors, including appropriate intestinal bacterial colonization [57]. Research on the development of oral tolerance has recently focused on the influence of host–microbe interactions on immune function, in particular on the ability of specific gut microbes to promote tolerance to food antigens [58][59][60]. In this respect, it has been reported that supplementation with Lactobacilllus rhamnosus GG (in an extensively hydrolyzed casein formula, eHCF) in infants with CMA stimulates immune tolerance [54][61][62], and some eHFs were supplemented with specific probiotic strains, which in turn may act on immunomodulation, in addition to the small peptides. Berni Canani et al. found that dietary management with an eHCF formula supplemented with the probiotic Lactobacillus rhamnosus GG (LGG) results in a higher rate of tolerance acquisition in children with IgE-mediated CMA, compared with non-supplemented eHCF or non-casein-based formulas [54]. In addition, in a well-characterized population of children with IgE-mediated CMA, it was shown that eHCF + LGG is superior to eHCF alone in preventing other allergic manifestations over a 36-month period [63]. The gut microbiota produces metabolites, such as SCFAs, beneficial for the colonic environment, which participate in improving barrier function, increasing Treg cells, and protecting against pathogenic bacteria colonization [64][65]. Another of the hypothesized mechanisms for an increased immune tolerance is the enrichment of butyrate-producing bacteria, as butyrate stimulates the development of Treg. Treg cells play a pivotal role in the development of oral tolerance [66][67][68] and their reduction has been associated with an allergic phenotype [69][70]. Ruohtula and colleagues found that an increase in highly activated Treg cells is associated with colonization of butyrate-producing bacilli and suggested a narrow window of opportunity (from birth to 3 months of age) for primary prevention of atopic diseases [71]. eHFs favour butyrate production, as highlighted by Car RennKok et al., who compared healthy term breastfed infants vs. infants fed with eHF or AAF. The authors found significant differences between the groups in beta-diversity at day 60, and a similar gut microbiota composition in the formula groups compared to the breastfed group. The relative abundance of Bifidobacterium spp. increased over time and was significantly enriched at day 60 in the human milk group. In contrast, a significant increase in Firmicutes members was found at day 60 in the formula groups, as well as butyrate-producing species in the eHF group. Butyrate increased significantly from baseline to day 60 in the eHF group and it was significantly higher in the study formula groups than in the human milk at day 60 [72]. Berni Canani et al. performed gut microbiota and oligotyping analysis on stool samples collected from healthy infants and infants with CMA before and after treatment with eHCF with or without LGG supplementation. They found that the infants who became tolerant early showed a significant increase in fecal butyrate levels and that eHCF + LGG promotes tolerance in infants with CMA, in part, by influencing the structure of the gut bacterial community at the strain level [62]. The same authors showed that children with non-IgE-mediated CMA had significantly lower fecal butyrate concentrations than healthy controls at the baseline, and dietary regimes (eHCF or eHCF + LGG) were associated with a significant increase in butyrate concentrations, especially in children treated with eHCF + LGG. In particular, the treatment with eHCF + LGG appears to restore the composition and structure of the subgenus Bacteroides, which shows similar diversity to that of healthy controls. Treatment with eHCF + LGG significantly increased butyrate production, and this change correlated with the enrichment of potential SCFA producers and selected Bacteroides oligotypes [73].
Besides probiotics, hydrolyzed formulas were also supplemented with oligosaccharides [74]. The effects of a formula supplemented with 2 HMOs-2′fucosyllactose (2′FL) and 0.5 g/L lacto-N-neotetraose (LNnT) on infant growth, tolerance and morbidity have been evaluated vs. non-supplemented formula milk [74]. The authors observed a similar weight gain in the two groups at 4 months, and similar digestive symptoms and behavioral patterns between the groups [75]. The safety and hypoallergenicity of an eHF supplemented with 2′FL and LNnT compared with a standard eHF were successfully assessed by Nowak-Wegrzyn and coworkers [76].
The possible influence of eHF formulas in promoting butyrate-producing species, and consequently butyrate production itself, is of great interest in the development of oral tolerance in infants with CMA. In addition, the role of probiotic-supplemented formulas, particularly LGGs, in the acquisition of immune tolerance is emerging. Future studies are required to elucidate the role of both synbiotics and HMOs in the pediatric population with CMA.
3.2. Special Formula for Functional Gastrointestinal Symptoms
Gastrointestinal symptoms, including frequent regurgitation, vomiting, and colicky, are very common in infants, and represent the most frequent cause of formula change in the first six months of age.
These symptoms can overlap non-IgE CMA ones, making it difficult to distinguish between them in clinical practice. However, it is very important to differentiate between these conditions as CMA is confirmed by oral food challenge only in a small percentage of infants [77] and it requires the use of an eHF, according to the guidelines [49]. A clinical score known as CoMiSS (cow’s milk related symptoms score) has been developed as a clinical tool aimed at increasing the awareness of health care professionals in identifying clinical manifestations possibly related to cow’s milk (CM) intake [78]. In a study comparing the effects of two eHF supplemented with probiotics in infants with suspected CMA, an improvement in all the items was observed after dietary intervention [79]. The observed effects on intestinal microbes were, as expected, an increase in bifidobacteria in the group with eHF supplemented with bifidobacteria, and enrichment in lactobacilli in the group with eHF supplemented with lactobacilli. Both formulas were equally effective and safe.
The effective response to hydrolyzed formulas in both functional gastrointestinal disorders and non-IgE CMA may be due to immunological mechanisms, as well as to improved gastric emptying [53][80]. Furthermore, a CM-free diet reduces mast cell infiltration and normalizes immune–nerve interactions and motor function [53].
Comparing a thickened eHF vs. a standard eHF on 77 infants with suspected CMA and bothersome regurgitation or vomiting (more than five episodes per day), a reduction in regurgitation was observed, both upon eHF use (after one month of intervention) and, to a greater extent, upon thickened formula intake [81].
In a French group of 30 infants with proven CMA by a double-blind dietary test (70% with positive IgE tests), the administration of a casein-based thickened eHF significantly decreased both regurgitation and clinical crying scores after only 14 days [82].
3.3. Phenylketonuria and Inborn Errors of Metabolism Formulas
Studies on the microbiome and its influence in patients with inborn errors of metabolism formulas (IEMs) mostly focused on phenylketonuria (PKU). To date, only one open-label, single-arm intervention pilot study in 2011 has evaluated the tolerance and efficacy of adding a prebiotic oligosaccharide mixture (scGOS/lcFOS) to a protein replacement suitable for children with PKU in 9 infants with PKU diagnosis. At the end of the observation period (8-weeks), all children had microbiota dominated by bifidobacteria, unchanged from the baseline. No child showed abnormally high levels of Clostridium histolyticum/lituseburense or potentially pathogenic Enterobacteriaceae at any time during the study. A significant reduction in median stool pH from the baseline was observed at week 4 (pH from 6.79 to 5.83), but this observation was not confirmed at week 8 [83].
References
- Passos, M.D.C.F.; Moraes-Filho, J.P. Intestinal Microbiota in Digestive Diseases. Arq. Gastroenterol. 2017, 54, 255–262.
- Gomaa, E.Z. Human Gut Microbiota/Microbiome in Health and Diseases: A Review. Antonie Van Leeuwenhoek 2020, 113, 2019–2040.
- Alonso, V.R.; Guarner, F. Linking the Gut Microbiota to Human Health. Br. J. Nutr. 2013, 109, S21–S26.
- Jethwani, P.; Grover, K. Gut Microbiota in Health and Diseases—A Review. Int. J. Curr. Microbiol. Appl. Sci. 2019, 8, 1586–1599.
- Laursen, M.F.; Bahl, M.I.; Licht, T.R. Settlers of Our Inner Surface—Factors Shaping the Gut Microbiota from Birth to Toddlerhood. FEMS Microbiol. Rev. 2021, 45, fuab001.
- Arrieta, M.-C.; Stiemsma, L.T.; Amenyogbe, N.; Brown, E.M.; Finlay, B. The Intestinal Microbiome in Early Life: Health and Disease. Front. Immunol. 2014, 5, 427.
- Bergström, A.; Skov, T.H.; Bahl, M.I.; Roager, H.M.; Christensen, L.B.; Ejlerskov, K.T.; Mølgaard, C.; Michaelsen, K.F.; Licht, T.R. Establishment of Intestinal Microbiota during Early Life: A Longitudinal, Explorative Study of a Large Cohort of Danish Infants. Appl. Environ. Microbiol. 2014, 80, 2889–2900.
- Laursen, M.F. Gut Microbiota Development: Influence of Diet from Infancy to Toddlerhood. Ann. Nutr. Metab. 2021, 77, 1–14.
- Chong, C.; Bloomfield, F.; O’Sullivan, J. Factors Affecting Gastrointestinal Microbiome Development in Neonates. Nutrients 2018, 10, 274.
- Bittinger, K.; Zhao, C.; Li, Y.; Ford, E.; Friedman, E.S.; Ni, J.; Kulkarni, C.V.; Cai, J.; Tian, Y.; Liu, Q.; et al. Bacterial Colonization Reprograms the Neonatal Gut Metabolome. Nat. Microbiol. 2020, 5, 838–847.
- Obermajer, T.; Grabnar, I.; Benedik, E.; Tušar, T.; Pikel, T.R.; Mis, N.F.; Matijašić, B.B.; Rogelj, I. Microbes in Infant Gut Development: Placing Abundance Within Environmental, Clinical and Growth Parameters. Sci. Rep. 2017, 7, 11230.
- Jian, C.; Luukkonen, P.; Yki-Järvinen, H.; Salonen, A.; Korpela, K. Quantitative PCR Provides a Simple and Accessible Method for Quantitative Microbiota Profiling. PLoS ONE 2020, 15, e0227285.
- Laursen, M.F.; Bahl, M.I.; Michaelsen, K.F.; Licht, T.R. First Foods and Gut Microbes. Front. Microbiol. 2017, 8, 356.
- World Health Organization, WHO. Available online: https://www.who.int/health-topics/com-plementary-feeding#tab=tab_2 (accessed on 1 May 2022).
- Simpson, H.L.; Campbell, B.J. Review Article: Dietary Fibre-Microbiota Interactions. Aliment. Pharmacol. Ther. 2015, 42, 158–179.
- Koh, A.; De Vadder, F.; Kovatcheva-Datchary, P.; Bäckhed, F. From Dietary Fiber to Host Physiology: Short-Chain Fatty Acids as Key Bacterial Metabolites. Cell 2016, 165, 1332–1345.
- Davis, J.C.C.; Totten, S.M.; Huang, J.O.; Nagshbandi, S.; Kirmiz, N.; Garrido, D.A.; Lewis, Z.T.; Wu, L.D.; Smilowitz, J.T.; German, J.B.; et al. Identification of Oligosaccharides in Feces of Breast-Fed Infants and Their Correlation with the Gut Microbial Community. Mol. Cell. Proteom. 2016, 15, 2987–3002.
- WHO. Protecting, Promoting, and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services: The Revised Baby-Friendly Hospital Initiative 2018; WHO: Geneva, Switzerland, 2018.
- Section on Breastfeeding; Eidelman, A.I.; Schanler, R.J.; Johnston, M.; Landers, S.; Noble, L.; Szucs, K.; Viehmann, L. Breastfeeding and the Use of Human Milk. Pediatrics 2012, 129, e827–e841.
- Agostoni, C.; Braegger, C.; Decsi, T.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Mihatsch, W.; Moreno, L.A.; Puntis, J.; Shamir, R.; et al. Breast-Feeding: A Commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 112–125.
- Sakanaka, M.; Gotoh, A.; Yoshida, K.; Odamaki, T.; Koguchi, H.; Xiao, J.; Kitaoka, M.; Katayama, T. Varied Pathways of Infant Gut-Associated Bifidobacterium to Assimilate Human Milk Oligosaccharides: Prevalence of the Gene Set and Its Correlation with Bifidobacteria-Rich Microbiota Formation. Nutrients 2019, 12, 71.
- Fukuda, S.; Toh, H.; Hase, K.; Oshima, K.; Nakanishi, Y.; Yoshimura, K.; Tobe, T.; Clarke, J.M.; Topping, D.L.; Suzuki, T.; et al. Bifidobacteria Can Protect from Enteropathogenic Infection through Production of Acetate. Nature 2011, 469, 543–547.
- Henrick, B.M.; Rodriguez, L.; Lakshmikanth, T.; Pou, C.; Henckel, E.; Arzoomand, A.; Olin, A.; Wang, J.; Mikes, J.; Tan, Z.; et al. Bifidobacteria-Mediated Immune System Imprinting Early in Life. Cell 2021, 184, 3884–3898.e11.
- Stokholm, J.; Blaser, M.J.; Thorsen, J.; Rasmussen, M.A.; Waage, J.; Vinding, R.K.; Schoos, A.-M.M.; Kunøe, A.; Fink, N.R.; Chawes, B.L.; et al. Maturation of the Gut Microbiome and Risk of Asthma in Childhood. Nat. Commun. 2018, 9, 141.
- Vatanen, T.; Kostic, A.D.; d’Hennezel, E.; Siljander, H.; Franzosa, E.A.; Yassour, M.; Kolde, R.; Vlamakis, H.; Arthur, T.D.; Hämäläinen, A.-M.; et al. Variation in Microbiome LPS Immunogenicity Contributes to Autoimmunity in Humans. Cell 2016, 165, 842–853.
- Alcon-Giner, C.; Dalby, M.J.; Caim, S.; Ketskemety, J.; Shaw, A.; Sim, K.; Lawson, M.A.E.; Kiu, R.; Leclaire, C.; Chalklen, L.; et al. Microbiota Supplementation with Bifidobacterium and Lactobacillus Modifies the Preterm Infant Gut Microbiota and Metabolome: An Observational Study. Cell Rep. Med. 2020, 1, 100077.
- Cerdó, T.; Ruíz, A.; Suárez, A.; Campoy, C. Probiotic, Prebiotic, and Brain Development. Nutrients 2017, 9, 1247.
- Ma, J.; Li, Z.; Zhang, W. Comparison of the Gut Microbiota in Healthy Infants With Different Delivery Modes and Feeding Types: A Cohort Study. Front. Microbiol. 2022, 13, 868227.
- Bäckhed, F.; Roswall, J.; Peng, Y.; Feng, Q.; Jia, H.; Kovatcheva-Datchary, P.; Li, Y.; Xia, Y.; Xie, H.; Zhong, H.; et al. Dynamics and Stabilization of the Human Gut Microbiome during the First Year of Life. Cell Host Microbe 2015, 17, 690–703.
- Berger, B.; Porta, N.; Foata, F.; Grathwohl, D.; Delley, M.; Moine, D.; Charpagne, A.; Siegwald, L.; Descombes, P.; Alliet, P.; et al. Linking Human Milk Oligosaccharides, Infant Fecal Community Types, and Later Risk to Require Antibiotics. mBio 2020, 11, e03196-19.
- Salminen, S.; Stahl, B.; Vinderola, G.; Szajewska, H. Infant Formula Supplemented with Biotics: Current Knowledge and Future Perspectives. Nutrients 2020, 12, 1952.
- Pärnänen, K.; Hultman, J.; Satokari, R.; Rautava, S.; Lamendella, R.; Wright, J.; McLimans, C.J.; Kelleher, S.L.; Virta, M. Formula alters preterm infant gut microbiota and increases its antibiotic resistance load. bioRxiv 2019, 782441.
- He, X.; Parenti, M.; Grip, T.; Lönnerdal, B.; Timby, N.; Domellöf, M.; Hernell, O.; Slupsky, C.M. Fecal Microbiome and Metabolome of Infants Fed Bovine MFGM Supplemented Formula or Standard Formula with Breast-Fed Infants as Reference: A Randomized Controlled Trial. Sci. Rep. 2019, 9, 11589.
- Chow, J.; Panasevich, M.R.; Alexander, D.; Vester Boler, B.M.; Rossoni Serao, M.C.; Faber, T.A.; Bauer, L.L.; Fahey, G.C. Fecal Metabolomics of Healthy Breast-Fed versus Formula-Fed Infants before and during In Vitro Batch Culture Fermentation. J. Proteome Res. 2014, 13, 2534–2542.
- Ehrlich, A.M.; Pacheco, A.R.; Henrick, B.M.; Taft, D.; Xu, G.; Huda, M.N.; Mishchuk, D.; Goodson, M.L.; Slupsky, C.; Barile, D.; et al. Indole-3-Lactic Acid Associated with Bifidobacterium-Dominated Microbiota Significantly Decreases Inflammation in Intestinal Epithelial Cells. BMC Microbiol. 2020, 20, 357.
- Meng, D.; Sommella, E.; Salviati, E.; Campiglia, P.; Ganguli, K.; Djebali, K.; Zhu, W.; Walker, W.A. Indole-3-Lactic Acid, a Metabolite of Tryptophan, Secreted by Bifidobacterium longum Subspecies Infantis Is Anti-Inflammatory in the Immature Intestine. Pediatr. Res. 2020, 88, 209–217.
- Henrick, B.M.; Chew, S.; Casaburi, G.; Brown, H.K.; Frese, S.A.; Zhou, Y.; Underwood, M.A.; Smilowitz, J.T. Colonization by B. infantis EVC001 Modulates Enteric Inflammation in Exclusively Breastfed Infants. Pediatr. Res. 2019, 86, 749–757.
- Shaw, A.G.; Cornwell, E.; Sim, K.; Thrower, H.; Scott, H.; Brown, J.C.S.; Dixon, R.A.; Kroll, J.S. Dynamics of Toxigenic Clostridium perfringens Colonisation in a Cohort of Prematurely Born Neonatal Infants. BMC Pediatr. 2020, 20, 75.
- Kuiper, G.-A.; van Prehn, J.; Ang, W.; Kneepkens, F.; van der Schoor, S.; de Meij, T. Clostridium difficile Infections in Young Infants: Case Presentations and Literature Review. IDCases 2017, 10, 7–11.
- Saraf, M.K.; Piccolo, B.D.; Bowlin, A.K.; Mercer, K.E.; LeRoith, T.; Chintapalli, S.V.; Shankar, K.; Badger, T.M.; Yeruva, L. Formula Diet Driven Microbiota Shifts Tryptophan Metabolism from Serotonin to Tryptamine in Neonatal Porcine Colon. Microbiome 2017, 5, 77.
- Fernández-Reina, A.; Urdiales, J.; Sánchez-Jiménez, F. What We Know and What We Need to Know about Aromatic and Cationic Biogenic Amines in the Gastrointestinal Tract. Foods 2018, 7, 145.
- Isolauri, E.; Rautava, S.; Salminen, S.; Collado, M.C. Early-Life Nutrition and Microbiome Development. In Nestlé Nutrition Institute Workshop Series; Donovan, S.M., German, J.B., Lönnerdal, B., Lucas, A., Eds.; S. Karger AG: Berlin, Germany, 2019; Volume 90, pp. 151–162. ISBN 978-3-318-06340-0.
- Differding, M.K.; Benjamin-Neelon, S.E.; Hoyo, C.; Østbye, T.; Mueller, N.T. Timing of Complementary Feeding Is Associated with Gut Microbiota Diversity and Composition and Short Chain Fatty Acid Concentrations over the First Year of Life. BMC Microbiol. 2020, 20, 56.
- Leong, C.; Haszard, J.J.; Lawley, B.; Otal, A.; Taylor, R.W.; Szymlek-Gay, E.A.; Fleming, E.A.; Daniels, L.; Fangupo, L.J.; Tannock, G.W.; et al. Mediation Analysis as a Means of Identifying Dietary Components That Differentially Affect the Fecal Microbiota of Infants Weaned by Modified Baby-Led and Traditional Approaches. Appl. Environ. Microbiol. 2018, 84, e00914-18.
- Fallani, M.; Amarri, S.; Uusijarvi, A.; Adam, R.; Khanna, S.; Aguilera, M.; Gil, A.; Vieites, J.M.; Norin, E.; Young, D.; et al. Determinants of the Human Infant Intestinal Microbiota after the Introduction of First Complementary Foods in Infant Samples from Five European Centres. Microbiology 2011, 157, 1385–1392.
- Laursen, M.F.; Andersen, L.B.B.; Michaelsen, K.F.; Mølgaard, C.; Trolle, E.; Bahl, M.I.; Licht, T.R. Infant Gut Microbiota Development Is Driven by Transition to Family Foods Independent of Maternal Obesity. mSphere 2016, 1, e00069-15.
- Tang, M.; Frank, D.; Hendricks, A.; Ir, D.; Krebs, N. Protein Intake During Early Complementary Feeding Affects the Gut Microbiota in U.S. Formula-Fed Infants (FS04-03-19). Curr. Dev. Nutr. 2019, 3, nzz048.FS04-03-19.
- Sicherer, S.H. Epidemiology of Food Allergy. J. Allergy Clin. Immunol. 2011, 127, 594–602.
- Muraro, A.; Werfel, T.; Hoffmann-Sommergruber, K.; Roberts, G.; Beyer, K.; Bindslev-Jensen, C.; Cardona, V.; Dubois, A.; duToit, G.; Eigenmann, P.; et al. EAACI Food Allergy and Anaphylaxis Guidelines: Diagnosis and Management of Food Allergy. Allergy 2014, 69, 1008–1025.
- D’Auria, E.; Salvatore, S.; Acunzo, M.; Peroni, D.; Pendezza, E.; Di Profio, E.; Fiore, G.; Zuccotti, G.V.; Verduci, E. Hydrolysed Formulas in the Management of Cow’s Milk Allergy: New Insights, Pitfalls and Tips. Nutrients 2021, 13, 2762.
- Koletzko, S.; Niggemann, B.; Arato, A.; Dias, J.A.; Heuschkel, R.; Husby, S.; Mearin, M.L.; Papadopoulou, A.; Ruemmele, F.M.; Staiano, A.; et al. Diagnostic Approach and Management of Cow’s-Milk Protein Allergy in Infants and Children: ESPGHAN GI Committee Practical Guidelines. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 221–229.
- von Berg, A. The Role of Hydrolysates for Allergy Prevention—Pro. Pediatr. Allergy Immunol. 2013, 24, 720–723.
- D’Auria, E.; Salvatore, S.; Pozzi, E.; Mantegazza, C.; Sartorio, M.U.A.; Pensabene, L.; Baldassarre, M.E.; Agosti, M.; Vandenplas, Y.; Zuccotti, G. Cow’s Milk Allergy: Immunomodulation by Dietary Intervention. Nutrients 2019, 11, 1399.
- Canani, R.B.; Nocerino, R.; Terrin, G.; Frediani, T.; Lucarelli, S.; Cosenza, L.; Passariello, A.; Leone, L.; Granata, V.; Di Costanzo, M.; et al. Formula Selection for Management of Children with Cow’s Milk Allergy Influences the Rate of Acquisition of Tolerance: A Prospective Multicenter Study. J. Pediatr. 2013, 163, 771–777.e1.
- Katz, Y.; Rajuan, N.; Goldberg, M.R.; Eisenberg, E.; Heyman, E.; Cohen, A.; Leshno, M. Early Exposure to Cow’s Milk Protein Is Protective against IgE-Mediated Cow’s Milk Protein Allergy. J. Allergy Clin. Immunol. 2010, 126, 77–82.e1.
- Paparo, L.; Picariello, G.; Bruno, C.; Pisapia, L.; Canale, V.; Sarracino, A.; Nocerino, R.; Carucci, L.; Cosenza, L.; Cozzolino, T.; et al. Tolerogenic Effect Elicited by Protein Fraction Derived From Different Formulas for Dietary Treatment of Cow’s Milk Allergy in Human Cells. Front. Immunol. 2020, 11, 604075.
- Tordesillas, L.; Berin, M.C. Mechanisms of Oral Tolerance. Clin. Rev. Allergy Immunol. 2018, 55, 107–117.
- Stefka, A.T.; Feehley, T.; Tripathi, P.; Qiu, J.; McCoy, K.; Mazmanian, S.K.; Tjota, M.Y.; Seo, G.-Y.; Cao, S.; Theriault, B.R.; et al. Commensal Bacteria Protect against Food Allergen Sensitization. Proc. Natl. Acad. Sci. USA 2014, 111, 13145–13150.
- Canani, R.B.; Gilbert, J.A.; Nagler, C.R. The Role of the Commensal Microbiota in the Regulation of Tolerance to Dietary Allergens. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 243–249.
- Arpaia, N.; Campbell, C.; Fan, X.; Dikiy, S.; van der Veeken, J.; deRoos, P.; Liu, H.; Cross, J.R.; Pfeffer, K.; Coffer, P.J.; et al. Metabolites Produced by Commensal Bacteria Promote Peripheral Regulatory T-Cell Generation. Nature 2013, 504, 451–455.
- Paparo, L.; Nocerino, R.; Di Scala, C.; Della Gatta, G.; Di Costanzo, M.; Buono, A.; Bruno, C.; Canani, R.B. Targeting Food Allergy with Probiotics. Probiotics Child Gastrointest. Health 2019, 1125, 57–68.
- Canani, R.B.; Sangwan, N.; Stefka, A.T.; Nocerino, R.; Paparo, L.; Aitoro, R.; Calignano, A.; Khan, A.A.; Gilbert, J.A.; Nagler, C.R. Lactobacillus rhamnosus GG-Supplemented Formula Expands Butyrate-Producing Bacterial Strains in Food Allergic Infants. ISME J. 2016, 10, 742–750.
- Nocerino, R.; Bedogni, G.; Carucci, L.; Cosenza, L.; Cozzolino, T.; Paparo, L.; Palazzo, S.; Riva, L.; Verduci, E.; Canani, R.B. The Impact of Formula Choice for the Management of Pediatric Cow’s Milk Allergy on the Occurrence of Other Allergic Manifestations: The Atopic March Cohort Study. J. Pediatr. 2021, 232, 183–191.e3.
- Tan, J.; McKenzie, C.; Potamitis, M.; Thorburn, A.N.; Mackay, C.R.; Macia, L. The Role of Short-Chain Fatty Acids in Health and Disease. Adv. Immunol. 2014, 121, 91–119.
- Rivera-Chávez, F.; Zhang, L.F.; Faber, F.; Lopez, C.A.; Byndloss, M.X.; Olsan, E.E.; Xu, G.; Velazquez, E.M.; Lebrilla, C.B.; Winter, S.E.; et al. Depletion of Butyrate-Producing Clostridia from the Gut Microbiota Drives an Aerobic Luminal Expansion of Salmonella. Cell Host Microbe 2016, 19, 443–454.
- Tan, J.; McKenzie, C.; Vuillermin, P.J.; Goverse, G.; Vinuesa, C.G.; Mebius, R.E.; Macia, L.; Mackay, C.R. Dietary Fiber and Bacterial SCFA Enhance Oral Tolerance and Protect against Food Allergy through Diverse Cellular Pathways. Cell Rep. 2016, 15, 2809–2824.
- Furusawa, Y.; Obata, Y.; Fukuda, S.; Endo, T.A.; Nakato, G.; Takahashi, D.; Nakanishi, Y.; Uetake, C.; Kato, K.; Kato, T.; et al. Commensal Microbe-Derived Butyrate Induces the Differentiation of Colonic Regulatory T Cells. Nature 2013, 504, 446–450.
- Fujimura, K.E.; Lynch, S.V. Microbiota in Allergy and Asthma and the Emerging Relationship with the Gut Microbiome. Cell Host Microbe 2015, 17, 592–602.
- Perezabad, L.; López-Abente, J.; Alonso-Lebrero, E.; Seoane, E.; Pion, M.; Correa-Rocha, R. The Establishment of Cow’s Milk Protein Allergy in Infants Is Related with a Deficit of Regulatory T Cells (Treg) and Vitamin D. Pediatr. Res. 2017, 81, 722–730.
- Shreffler, W.G.; Wanich, N.; Moloney, M.; Nowak-Wegrzyn, A.; Sampson, H.A. Association of Allergen-Specific Regulatory T Cells with the Onset of Clinical Tolerance to Milk Protein. J. Allergy Clin. Immunol. 2009, 123, 43–52.e7.
- Ruohtula, T.; de Goffau, M.C.; Nieminen, J.K.; Honkanen, J.; Siljander, H.; Hämäläinen, A.-M.; Peet, A.; Tillmann, V.; Ilonen, J.; Niemelä, O.; et al. Maturation of Gut Microbiota and Circulating Regulatory T Cells and Development of IgE Sensitization in Early Life. Front. Immunol. 2019, 10, 2494.
- Kok, C.R.; Brabec, B.; Chichlowski, M.; Harris, C.L.; Moore, N.; Wampler, J.L.; Vanderhoof, J.; Rose, D.; Hutkins, R. Stool Microbiome, PH and Short/Branched Chain Fatty Acids in Infants Receiving Extensively Hydrolyzed Formula, Amino Acid Formula, or Human Milk through Two Months of Age. BMC Microbiol. 2020, 20, 337.
- Berni Canani, R.; De Filippis, F.; Nocerino, R.; Paparo, L.; Di Scala, C.; Cosenza, L.; Della Gatta, G.; Calignano, A.; De Caro, C.; Laiola, M.; et al. Gut Microbiota Composition and Butyrate Production in Children Affected by Non-IgE-Mediated Cow’s Milk Allergy. Sci. Rep. 2018, 8, 12500.
- Smilowitz, J.T.; Lebrilla, C.B.; Mills, D.A.; German, J.B.; Freeman, S.L. Breast Milk Oligosaccharides: Structure-Function Relationships in the Neonate. Annu. Rev. Nutr. 2014, 34, 143–169.
- Puccio, G.; Alliet, P.; Cajozzo, C.; Janssens, E.; Corsello, G.; Sprenger, N.; Wernimont, S.; Egli, D.; Gosoniu, L.; Steenhout, P. Effects of Infant Formula with Human Milk Oligosaccharides on Growth and Morbidity: A Randomized Multicenter Trial. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 624–631.
- Nowak-Wegrzyn, A.; Czerkies, L.; Reyes, K.; Collins, B.; Heine, R.G. Confirmed Hypoallergenicity of a Novel Whey-Based Extensively Hydrolyzed Infant Formula Containing Two Human Milk Oligosaccharides. Nutrients 2019, 11, 1447.
- Hilvo, M. Maternal Elimination Diet and Symptoms of Cow’s Milk Allergy in Breastfed Infants. JAMA Pediatr. 2021, 175, 425–426.
- Vandenplas, Y.; Dupont, C.; Eigenmann, P.; Host, A.; Kuitunen, M.; Ribes-Koninckx, C.; Shah, N.; Shamir, R.; Staiano, A.; Szajewska, H.; et al. A Workshop Report on the Development of the Cow’s Milk-Related Symptom Score Awareness Tool for Young Children. Acta Paediatr. 2015, 104, 334–339.
- Vandenplas, Y.; Steenhout, P.; Planoudis, Y.; Grathwohl, D. Althera Study Group Treating Cow’s Milk Protein Allergy: A Double-Blind Randomized Trial Comparing Two Extensively Hydrolysed Formulas with Probiotics. Acta Paediatr. 2013, 102, 990–998.
- Salvatore, S.; Agosti, M.; Baldassarre, M.E.; D’Auria, E.; Pensabene, L.; Nosetti, L.; Vandenplas, Y. Cow’s Milk Allergy or Gastroesophageal Reflux Disease-Can We Solve the Dilemma in Infants? Nutrients 2021, 13, 297.
- Vandenplas, Y.; Salvatore, S. Infant Formula with Partially Hydrolyzed Proteins in Functional Gastrointestinal Disorders. Nestle Nutr. Inst. Workshop Ser. 2016, 86, 29–37.
- Dupont, C.; Bradatan, E.; Soulaines, P.; Nocerino, R.; Berni-Canani, R. Tolerance and Growth in Children with Cow’s Milk Allergy Fed a Thickened Extensively Hydrolyzed Casein-Based Formula. BMC Pediatr. 2016, 16, 96.
- MacDonald, A.; Cochrane, B.; Wopereis, H.; Loveridge, N. Specific Prebiotics in a Formula for Infants with Phenylketonuria. Mol. Genet. Metab. 2011, 104, S55–S59.
More
Information
Subjects:
Biology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
759
Revisions:
2 times
(View History)
Update Date:
28 Sep 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No