Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Rita Balsano | -- | 1318 | 2022-09-07 13:21:54 | | | |
| 2 | Rita Xu | Meta information modification | 1318 | 2022-09-08 02:49:51 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Balsano, R.; Kruize, Z.; Lunardi, M.; Comandatore, A.; Barone, M.; Cavazzoni, A.; Cecconi, A.D.R.; Morelli, L.; Wilmink, H.; Tiseo, M.; et al. Transforming Growth Factor-Beta Signaling Activation in Cancer-Induced Cachexia. Encyclopedia. Available online: https://encyclopedia.pub/entry/26962 (accessed on 26 July 2026).
Balsano R, Kruize Z, Lunardi M, Comandatore A, Barone M, Cavazzoni A, et al. Transforming Growth Factor-Beta Signaling Activation in Cancer-Induced Cachexia. Encyclopedia. Available at: https://encyclopedia.pub/entry/26962. Accessed July 26, 2026.
Balsano, Rita, Zita Kruize, Martina Lunardi, Annalisa Comandatore, Mara Barone, Andrea Cavazzoni, Andrea David Re Cecconi, Luca Morelli, Hanneke Wilmink, Marcello Tiseo, et al. "Transforming Growth Factor-Beta Signaling Activation in Cancer-Induced Cachexia" Encyclopedia, https://encyclopedia.pub/entry/26962 (accessed July 26, 2026).
Balsano, R., Kruize, Z., Lunardi, M., Comandatore, A., Barone, M., Cavazzoni, A., Cecconi, A.D.R., Morelli, L., Wilmink, H., Tiseo, M., Garajovà, I., Zuylen, L.V., Giovannetti, E., & Piccirillo, R. (2022, September 07). Transforming Growth Factor-Beta Signaling Activation in Cancer-Induced Cachexia. In Encyclopedia. https://encyclopedia.pub/entry/26962
Balsano, Rita, et al. "Transforming Growth Factor-Beta Signaling Activation in Cancer-Induced Cachexia." Encyclopedia. Web. 07 September, 2022.
Copy Citation
Cachexia is a metabolic syndrome consisting of massive loss of muscle mass and function that has a severe impact on the quality of life and survival of cancer patients. Up to 20% of lung cancer patients and up to 80% of pancreatic cancer patients are diagnosed with cachexia, leading to death in 20% of them. The main drivers of cachexia are cytokines such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), macrophage inhibitory cytokine 1 (MIC-1/GDF15) and transforming growth factor-beta (TGF-β). Besides its double-edged role as a tumor suppressor and activator, TGF-β causes muscle loss through myostatin-based signaling, involved in the reduction in protein synthesis and enhanced protein degradation.
cachexia
TGF-β
cancer-related syndrome
1. Introduction
Cachexia is a multifactorial metabolic and immune system imbalance that represents one of the most detrimental side effects of cancer and anti-tumoral treatment [1]. Cancer-associated cachexia is a paraneoplastic syndrome consisting of ongoing skeletal muscle loss (with or without fat mass loss) during cancer appearance and treatment], which cannot be fully reversed by standard or enriched nutritional support, leading to progressive functional impairment and death [2]. Body emaciation, progressive loss of deambulatory function and body weight as well as an increased sense of fatigue are some of the clinical hallmarks of cancer cachexia. Half of all cancer patients develop cachexia, and this estimate increases to 80% in hospitalized or advanced-stage patients [3].
The incidence and prevalence of cancer cachexia are not homogenous across cancer patients. They rather occur at different rates depending on the type and stage of cancer. For instance, cachexia is observed in 80% of gastric, pancreatic, and esophageal cancer patients, 70% of individuals suffering from head-and-neck tumors and 60% of the combined patients with lung, colorectal, lymphoma, and prostate cancer [4]. However, cachexia is the cause of death in at least 22% of all cancer patients [5]. In addition, it has been established that cachexia can lead to lower responsiveness to anticancer therapies, worsening the quality of life of patients, and is associated with poor prognosis in advanced cancer patients [6]. With respect to the lower responsiveness, it has been reported that treating cachectic patients with conventional chemotherapeutics further enhances muscle hyper-catabolism forcing therapy discontinuation for the undesirable toxicity and could also cause detrimental changes in fat and bone mass. This would exacerbate the pathological condition, thus requiring dosage limitation or early therapy interruption [7].
Cachexia progression is often described as ranging from pre-cachexia to cachexia, and finally to refractory cachexia, where the expected survival is less than 3 months [2]. Even though its pathologic mechanisms are complex, it is often mistakenly regarded as a homogeneous condition, with little understanding that the underlying causes can be heterogeneous. Cachexia involves the loss of skeletal muscle and adipose tissue, depending in part on the grade of systemic inflammation. This muscle loss can greatly reduce the quality of life of cancer patients. Cachectic patients exhibit several other symptoms and clinicopathological alterations, such as anorexia, fatigue, anemia, early satiety, weakness, altered blood biochemistry parameters, and increased levels of inflammatory factors in various organs and tissues. The knowledge of the inflammatory changes is of extreme importance for a better understanding of the clinical picture of this syndrome [5]. Previous research suggests that systemic inflammation has a role both in the progression of cancer and of cachexia [8].
The systemic inflammation is mediated by an imbalance between pro-inflammatory and anti-inflammatory cytokines, which are normally in equilibrium. In cancer patients, this equilibrium is disturbed, which results in a dysfunctional state of both immune stimulation and suppression [9]. Cytokines function by interacting with other body tissues as well as within the tumor micro-environment itself, to generate a systemic response [10]. Hereby, cytokines contribute to mechanisms that determine the initiation, promotion, invasion and metastasis of cancer [11]. Previous work also reported that the production rate of several cytokines is associated with the prevalence of cachexia in some types of cancer [12]. The main cytokines driving cachexia are IL-6, TNF-α, TGF-β and MIC-1/GDF15 [12] MIC-1/GDF15, a member of the TGF-β superfamily, is produced in large amounts by normal and cancer cells. It acts on the feeding centers in the hypothalamus and brainstem, thereby causing anorexia and eventually cachexia [13].
Next to its role as a tumor suppressor as well as tumor activator, TGF-β has an emerging role in metabolism regulation. Acting through the SMAD2/3 pathway, it causes muscle loss through myostatin-related signaling, which is involved in the reduction in protein synthesis and in the increase in protein degradation [14]. Myostatin or GDF8 is a well-known negative regulator of muscle mass [15]. In addition, TGF-β plays a role in the mechanisms behind weight loss, muscle atrophy and fibrosis [16]. Greco and colleagues proved that anti-TGF-β antibodies, inhibiting TGF-β-based signaling, significantly improved overall survival, weight, fat mass, lean body mass, skeletal muscle proteolysis and bone mineral density of mouse models with advanced pancreatic cancer. Overall, they showed that inhibiting TGF-β could decrease the metabolic changes associated with cancer cachexia and improve overall survival [17]. Multiple studies have shown the correlation between cytokine levels and both cancer and cachexia; however, the mechanisms by which these cytokines act on the tumor and body are not completely understood.
Notably, aside from cancer, cachexia is observed in the late stages of almost every major chronic illness (such as diabetes, cardiac failure, renal failure, and chronic obstructive pulmonary disease), which underlines the need for more insights into this syndrome [18]. Despite the prevalence and severity, cachexia remains understudied, while treatment options are limited due to therapy inadequacy and inconsistency [19]. Therefore, it is essential to investigate the molecular mediators involved in the onset of cachexia to find potential therapeutic targets.
2. TGF-β Signaling Activation
Puzzlingly, TGF-β plays a dual regulation in cancer, both as a tumor suppressor and tumor enhancer. On one side, the TGF-β pathway is involved in tumor suppression, inhibiting Natural Killer (NK)-cell activity and stimulating the production of regulatory T cells (Treg) that inactivate both cytotoxic and T helper cells [20]. On the other side, TGF-β activity paradoxically promotes tumor growth by interfering with many cancer-related processes such as cell proliferation, apoptosis and epithelial-to-mesenchymal transition (EMT) [21].
In the canonical pathway, signaling is mediated by three types of receptors: TGF-β receptor I (TFβRI, also known as activin receptor-like kinase ALK5), TGF-β receptor II (TFβRII) and TGF-β receptor III (TFβRIII) [22]. TGF-β ligands bind directly to TFβRII, which phosphorylates TFβRI, which, in turn, activates SMAD proteins (SMADs) (Figure 1). SMAD2 and SMAD3 proteins are activated by ligands of TGF-β in their C-terminal serine residues, while other ligands such as BMP activate SMAD5 and SMAD8. In this process, some auxiliary proteins intervene as regulators: for example, the receptor activator SARA stabilizes both SMAD2 and SMAD3 transcription factors.
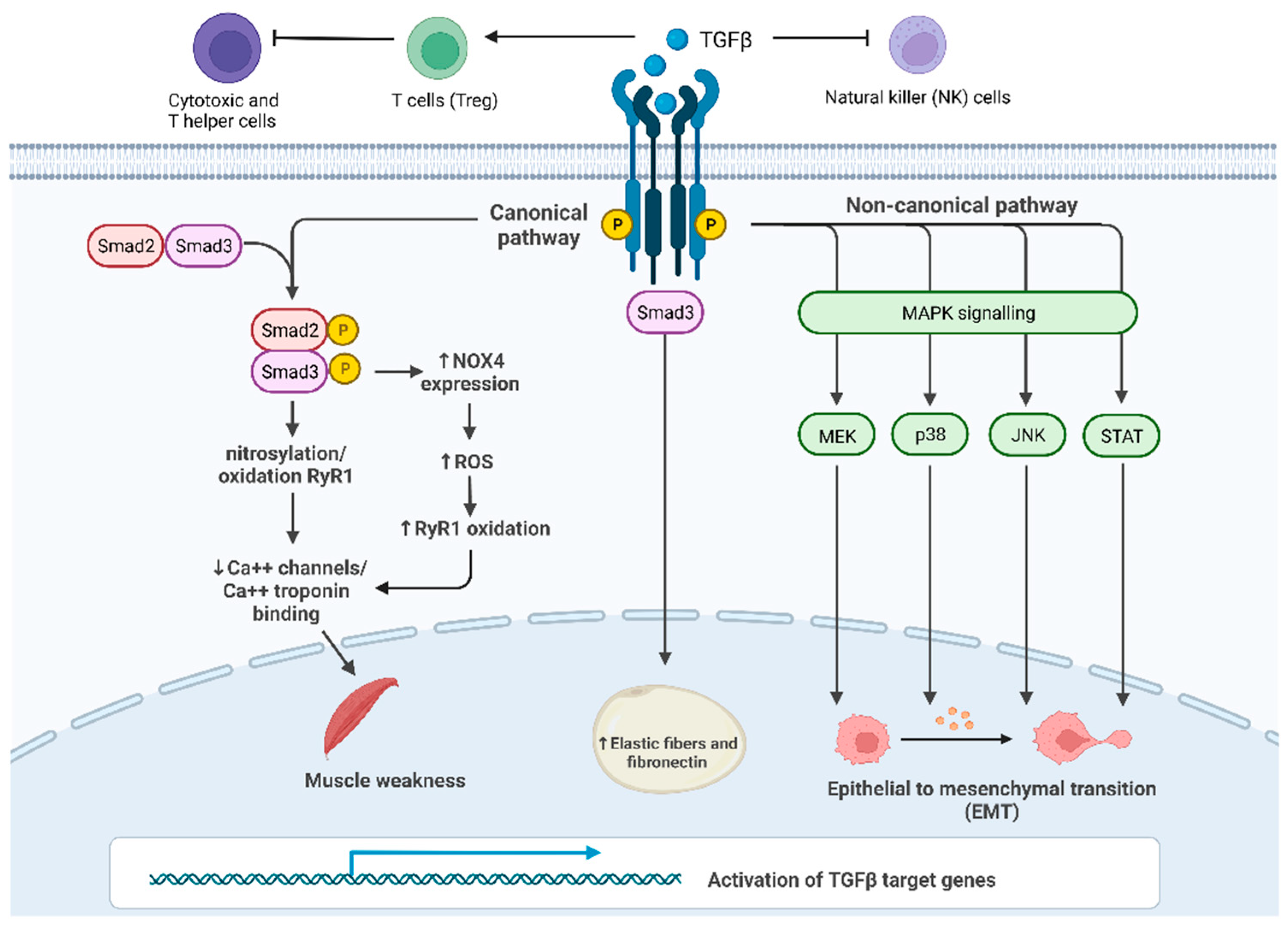
Figure 1. TGF-β signaling and its main roles in cancer progression and in cachexia: Canonical SMAD-dependent pathway: in proximal and distal skeletal muscles, SMAD3 signaling pathway results in the oxidation and nitrosylation of ryanodine receptor 1 (RyR1), which, in turn, reduces Ca2+ channels in the sarcoplasmic reticulum and causes muscle weakness; furthermore, SMAD3 induces the transcription of Nox4 gene increasing the production of ROS that oxidize RyR1. Non-canonical JNK/p38 MAPK signaling pathway affects EMT in many tissues promoting cancer growth; c. TGF-β/SMAD3 pathway leads to an increase in fibrosis in the subcutaneous adipose tissue.
Once activated, SMAD proteins change conformation, thus allowing binding to SMAD4 (co-SMAD), an important mediator of this pathway. The resulting heterodimer translocates into the nucleus, where SMAD Mad-Homology 1 (MH1) domain can bind SMAD binding elements (SBE) [23].
TGF-βRII can also cause endocytosis of parathyroid hormone type I receptor (PTH1R), after stimulation of PTH. The loss of TGF-βRII allows the persistence of PTH1R-based signaling on the cell surface and its continuous activation by the ligand. Thus, TGF-βRII KO mice provide the anabolic effect of PTH/PTHrP on osteoblasts [24].
The above-mentioned mechanisms illustrate the complex and multifactorial interaction between the TGF-β signaling and several factors potentially influencing cancer cachexia (Figure 1). However, further studies are essential to better elucidate the crosstalk of TGF-β signaling with the tissue and cancer microenvironment.
References
- Tisdale, M.J. Molecular Pathways Leading to Cancer Cachexia. Physiology 2005, 20, 340–348.
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and Classification of Cancer Cachexia: An International Consensus. Lancet Oncol. 2011, 12, 489–495.
- Tisdale, M.J. The “Cancer Cachectic Factor. ” Supportive Care Cancer 2003, 11, 73–78.
- Anker, M.S.; Holcomb, R.; Muscaritoli, M.; von Haehling, S.; Haverkamp, W.; Jatoi, A.; Morley, J.E.; Strasser, F.; Landmesser, U.; Coats, A.J.S.; et al. Orphan Disease Status of Cancer Cachexia in the USA and in the European Union: A Systematic Review. J. Cachexia Sarcopenia Muscle 2019, 10, 22–34.
- Argilés, J.M.; Busquets, S.; Stemmler, B.; López-Soriano, F.J. Cancer Cachexia: Understanding the Molecular Basis. Nat. Rev. Cancer 2014, 14, 754–762.
- Prado, C.M.M.; Bekaii-Saab, T.; Doyle, L.A.; Shrestha, S.; Ghosh, S.; Baracos, V.E.; Sawyer, M.B. Skeletal Muscle Anabolism Is a Side Effect of Therapy with the MEK Inhibitor: Selumetinib in Patients with Cholangiocarcinoma. Br. J. Cancer 2012, 106, 1583–1586.
- Pin, F.; Couch, M.E.; Bonetto, A. Preservation of Muscle Mass as a Strategy to Reduce the Toxic Effects of Cancer Chemotherapy on Body Composition. Curr. Opin. Support Palliat Care 2018, 12, 420–426.
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-Associated Cachexia. Nat. Rev. Dis. Primers 2018, 4, 17105.
- Lippitz, B.E.; Harris, R.A. Cytokine Patterns in Cancer Patients: A Review of the Correlation between Interleukin 6 and Prognosis. Oncoimmunology 2016, 5, e1093722.
- Wang, M.; Zhao, J.; Zhang, L.; Wei, F.; Lian, Y.; Wu, Y.; Gong, Z.; Zhang, S.; Zhou, J.; Cao, K.; et al. Role of Tumor Microenvironment in Tumorigenesis. J. Cancer 2017, 8, 761–773.
- Landskron, G.; de La Fuente, M.; Thuwajit, P.; Thuwajit, C.; Hermoso, M.A. Chronic Inflammation and Cytokines in the Tumor Microenvironment. J. Immunol. Res. 2014, 2014, 149185.
- Fearon, K.C.H.; Glass, D.J.; Guttridge, D.C. Cancer Cachexia: Mediators, Signaling, and Metabolic Pathways. Cell Metab. 2012, 16, 153–166.
- Tsai, V.W.W.; Lin, S.; Brown, D.A.; Salis, A.; Breit, S.N. Anorexia-Cachexia and Obesity Treatment May Be Two Sides of the Same Coin: Role of the TGF-b Superfamily Cytokine MIC-1/GDF15. Int. J. Obes 2016, 40, 193–197.
- Chen, J.L.; Walton, K.L.; Hagg, A.; Colgan, T.D.; Johnson, K.; Qian, H.; Gregorevic, P.; Harrison, C.A. Specific Targeting of TGF-β Family Ligands Demonstrates Distinct Roles in the Regulation of Muscle Mass in Health and Disease. Proc. Natl. Acad. Sci. USA 2017, 114, E5266–E5275.
- McPherron, A.C.; Lawler, A.M.; Lee, S.J. Regulation of Skeletal Muscle Mass in Mice by a New TGF-Beta Superfamily Member. Nature 1997, 387, 83–90.
- Mendias, C.L.; Gumucio, J.P.; Davis, M.E.; Bromley, C.W.; Davis, C.S.; Brooks, S.V. Transforming Growth Factor-Beta Induces Skeletal Muscle Atrophy and Fibrosis through the Induction of Atrogin-1 and Scleraxis. Muscle Nerve 2012, 45, 55–59.
- Greco, S.H.; Tomkötter, L.; Vahle, A.K.; Rokosh, R.; Avanzi, A.; Mahmood, S.K.; Deutsch, M.; Alothman, S.; Alqunaibit, D.; Ochi, A.; et al. TGF-β Blockade Reduces Mortality and Metabolic Changes in a Validated Murine Model of Pancreatic Cancer Cachexia. PLoS ONE 2015, 10, e0132786.
- Farkas, J.; von Haehling, S.; Kalantar-Zadeh, K.; Morley, J.E.; Anker, S.D.; Lainscak, M. Cachexia as a Major Public Health Problem: Frequent, Costly, and Deadly. J. Cachexia Sarcopenia Muscle 2013, 4, 173–178.
- Roeland, E.J.; Bohlke, K.; Baracos, V.E.; Bruera, E.; Fabbro, E.D.; Dixon, S.; Fallon, M.; Herrstedt, J.; Lau, H.; Platek, M.; et al. Management of Cancer Cachexia: ASCO Guideline. J. Clin. Oncol. 2020, 38, 2438–2453.
- Chen, W.J.; Wahl, S.M. TGF-Beta: The Missing Link in CD4+CD25+ Regulatory T Cell-Mediated Immunosuppression. Cytokine Growth Factor Rev. 2003, 14, 85–89.
- Colak, S.; ten Dijke, P. Targeting TGF-β Signaling in Cancer. Trends Cancer 2017, 3, 56–71.
- Tian, M.; Neil, J.R.; Schiemann, W.P. Transforming Growth Factor-β and the Hallmarks of Cancer. Cell Signal. 2011, 23, 951–962.
- Dardare, J.; Witz, A.; Merlin, J.L.; Gilson, P.; Harlé, A. SMAD4 and the TGFβ Pathway in Patients with Pancreatic Ductal Adenocarcinoma. Int. J. Mol. Sci. 2020, 21, 3534.
- Qiu, T.; Wu, X.; Zhang, F.; Clemens, T.L.; Wan, M.; Cao, X. TGF-Beta Type II Receptor Phosphorylates PTH Receptor to Integrate Bone Remodelling Signalling. Nat. Cell Biol. 2010, 12, 224–234.
More
Information
Subjects:
Oncology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
937
Revisions:
2 times
(View History)
Update Date:
09 Sep 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No