Photodynamic therapy (PDT) is a two-stage treatment that combines light energy with a photosensitizer designed to destroy cancerous and precancerous cells after light activation. Photosensitizers are activated by a specific wavelength of light energy, usually from a laser. The photosensitizer is nontoxic until it is activated by light. However, after light activation, the photosensitizer becomes toxic to the targeted tissue. Among sensitizers, the topical use of 5-aminolevulinic acid (ALA), a natural precursor of protoporphyrin IX, a precursor of the heme group, and a powerful photosensitizing agent, represents a turning point for PDT in the dermatological field, as it easily absorbable by the skin. Wound healing requires a complex interaction and coordination of different cells and molecules. Any alteration in these highly coordinated events can lead to either delayed or excessive healing.
1. The Photodynamic Therapy
In medicine, the use of photodynamic therapy (PDT) is now widely documented and well-codified for the treatment of oncological and non-oncological diseases. In dermatology, the use varies from oncological pathologies such as basal cell carcinoma, squamous cell carcinoma, actinic and non-oncologic keratoses, bacterial, fungal, viral, immunological or inflammatory infections, to the treatment of chronic wounds, and finally, cosmetology for photorejuvenation
[1][2][3]. PDT is based on the cytotoxic action of some hyperactive oxygen species (i.e., a type of unstable oxygen molecule that easily reacts with other molecules in a cell; a build-up of reactive oxygen species in cells may cause damage to DNA, RNA, and proteins, and potentially induce cell death
[6], especially singlet oxygen, but also superoxide anions and hydroxyl radicals, generated by the transfer of energy and/or electrons from the photoexcited oxygen sensitizer. Three important mechanisms are responsible for the efficacy of PDT: (1) direct death, or inflammation, of tumor cells, (2) damage to tumor vessels, (3) immunological response associated with the stimulation of leukocytes and release of interleukins and other cytokines, growth factors, complement components, acute phase proteins, and other immunoregulators
[1][2][3][4]. In wound healing, recent studies show the efficacy of PDT for its antibacterial activity, in attacking the biofilm, and in remodeling the extracellular matrix by activating MMPs, thus inducing changes in the collagen of the extracellular matrix for the tissue healing process. In addition, PDT induces cellular changes, which is the phenomenon observed during the course of tissue repair
[1][2][3][4].
2. Photosensitizers
PDT is a treatment that uses a photosensitizer (administered topically or systemically), light (which interacts with the substance in question), and oxygen to cause selective cell death by necrosis or apoptosis of the cells “atypically” sensitized, in which the photosensitizer or its precursor—administered topically or intravenously—accumulate selectively.
In summary, the photodynamic effect (through photophysical, photochemical, and photobiological mechanisms) is mediated by the generation of ROS, a process that depends on the intracellular interactions of the photosensitizer with light and oxygen
[1][2][3][4].
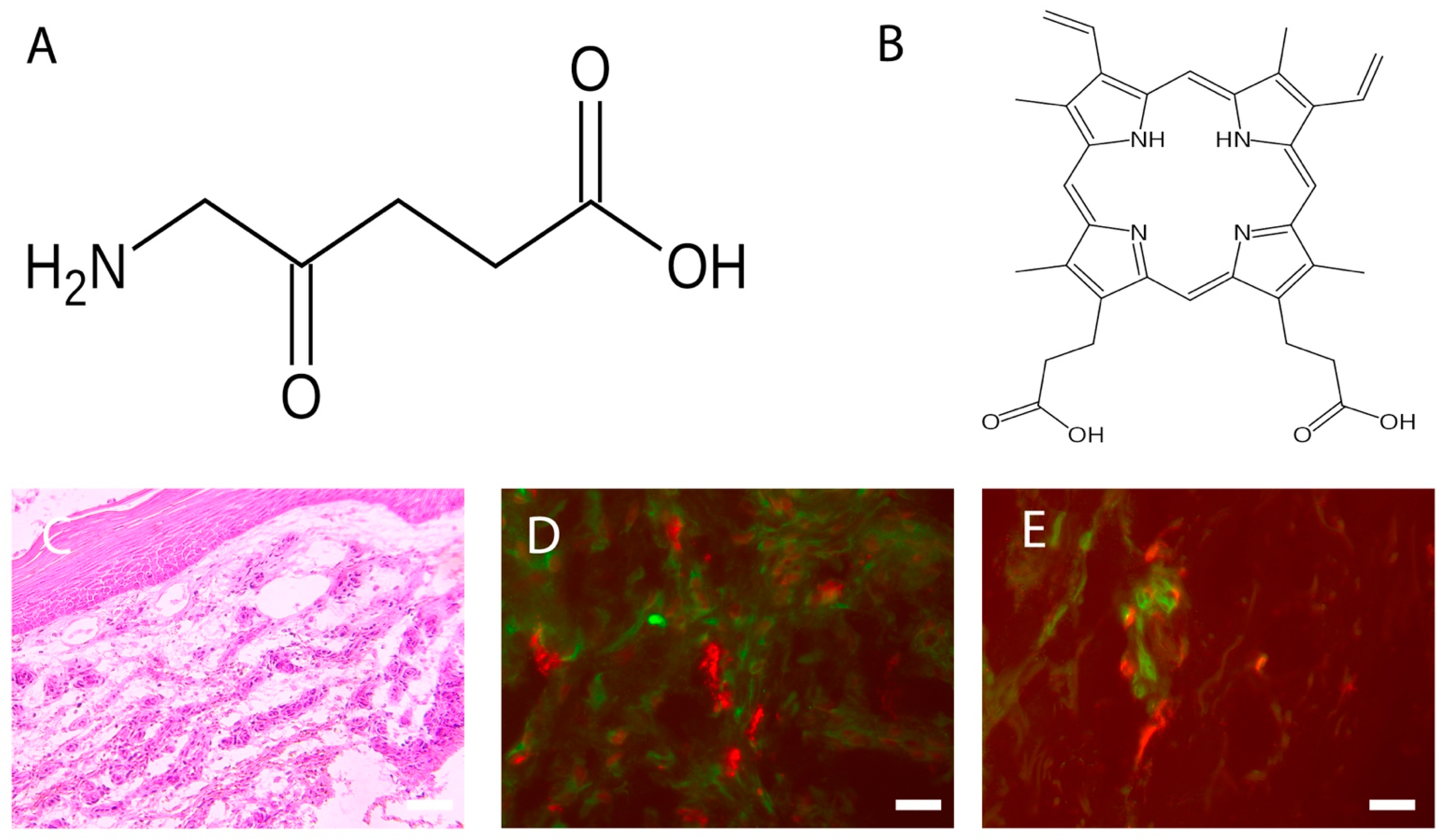
The topical use of ALA (
Figure 1A), a natural precursor of protoporphyrin IX (
Figure 1B) and, in turn, a precursor of the heme group and a powerful photosensitizing agent, represents an important turning point in the dermatological field, as it is easily absorbable by the skin
[2][3][5][6][7][8]. At the cellular level, the pro-drug, once transformed into protoporphyrin IX, causes the production of reactive oxygen species, which induce cell death in target cells. The presence of ROS in the immediate vicinity of cellular and subcellular membranes (in particular the mitochondrial ridges) allows the release of cytochrome C, with consequent activation of the caspase cascade, which ultimately leads to the intrinsic apoptotic phenomenon. The effect is enhanced by the degeneration of small vessels via a photodynamic mechanism, and by the triggering of an inflammatory reaction
[3][5][6][7][9]. The concentration of 5-ALA usually depends on the mode of treatment, but the range is between 2–40% systematically, and 30–50 mg/cm2 topically. It is usually applied for less than 4 h, and it reaches peak accumulation between 3 and 8 h
[2][3][5][6][7][8].
Figure 1. (A) Fvasconcellos: Structural diagram of aminolevulinic acid. Created using ACD/ChemSketch 10.0 and Inkscape. This image of a simple structural formula is ineligible for copyright and, therefore, is in the public domain, because it contains no original authorship. (B) Fvasconcellos: Skeletal formula of protoporphyrin IX. Created using ACD/ChemSketch 10.0 and Inkscape. The copyright holder of this work has released it into the public domain. This standard applies worldwide. In some countries this may not be legally possible. I grant anyone the right to use this work for any purpose, without any conditions, unless such conditions are required by law. (C) Chronic wound: Increased thickness of the epidermis and richness of cellular infiltrate. Hematoxylin Eosin, Light microscopy, scale bar = 10 microns. (D) Colocalization between MCs (stained with avidin, in red) and fibroblasts (stained with HSP47, in green) in PDT-treated chronic wounds. Fluorescence microscopy, scale bar =10 microns (see Table 1 for others information). (E) Colocalization between MCs (stained with avidin, in red) and DCs (stained with MHC class II, in green) in PDT-treated chronic wounds. Fluorescence microscopy, scale bar =10 microns (see Table 1 for others information).
Table 1. Reagents used to stain inflammatory cells.
| Substances |
Target |
References |
| HSP 47 (Antibody) |
Fibroblasts |
[10] |
| Avidin (Egg white protein linking biotin) |
MCs |
[11] |
| MHC class II (Antibody) |
Dendritic cells |
[12] |
3. Wound Healing
Wound healing makes organisms resilient to injuries, allowing survival
[13]. This process involves the interaction of various elements, such as soluble mediators (such as cytokines and factors growth), the extracellular matrix, vessels, and various other cell types. The physiological process underlying tissue repair is traditionally divided into four phases: coagulation, inflammatory, proliferative, and maturation
[14][15][16][17][18][19][20][21].
Coagulation phase: An initial process occurs during the inflammatory phase of hemostasis, with temporary vasoconstriction caused by release of vasoactive substances by damaged cells, followed by hemorrhage and subsequent platelet aggregation. The platelets, as well as being involved in clot formation, are also important producers of cytokines used in the activation of leukocytes and macrophages. With the aggregation process of the platelets, a biochemical cascade is then activated, in which dozens of factors are involved that lead to formation of an insoluble fibrin network
[14][15][16][17][18][19][20][21].
Inflammatory phase: The initial vasoconstriction process is followed by vasodilation mediated by substances such as histamine and serotonin secreted by MCs
[22][23][24]. This leads to increased blood flow in the area of the wound that determines an initial process of migration (diapedesis) of elements of blood corpuscles, such as neutrophil granulocytes, initially, and macrophages, subsequently.
Proliferative phase: The proliferative phase leads to the formation granulation tissue. During this stage, the fibroblasts play a central role, as they are responsible for the production of precursors of collagen, elastin, and other molecules fundamental to the constitution of the extracellular matrix, and are also implicated in the regulation of migration and proliferation of the cellular protagonists involved in the re-epithelialization process and neo-angiogenesis
[14][15][16][17][18][19][20][21].
Maturation phase: The remodeling of a wound can take up to 1 year. In humans, this phenomenon is characterized by two single processes, wound contraction and collagen restoration, where myofibroblasts allow contraction of the wound, with the formation of a scar both in children and adults
[14][15][16][17][18][19][20][21]. During this process, the tensile strength increases, reaching approximately 80% that of unwounded skin, and is in relation to collagen crosslinking by lysyl oxidase
[14][15][16][17][18][19][20][21].
4. PDT and Wound Healing
The mechanisms that lead to wound healing upon PDT treatment are not fully understood; however, one of the main reasons is represented by apoptosis, caused by damage to the cellular and mitochondrial membranes, enzymatic inactivation and arrest of cellular respiration processes, and the release of cytochrome C, leading to the activation of the caspase cascade. It has also been observed that PDT modulates the production of MMPs, cytokines, and growth factors by fibroblasts and keratinocytes, substances that can accelerate wound healing
[25][26][27]. In particular, when the process of remodeling is required, MMPs are expressed and activated, and their contribution is related to collagen degradation and extracellular matrix remodeling
[25][26][27].
Regarding the inflammatory process that develops
[15][21], the occurrence of the following have been observed: the degranulation of MCs and neutrophil granulocytes
[22][23][24][28][29], the formation of oxygen radicals, and the release of lysosomal enzymes and chemotactic agents. The release of antigens of dead cells, in the presence of inflammatory cytokines, determines the activation of skin DCs, which, after the presentation of these antigens to T lymphocytes in the district lymph nodes, stimulates a specific immune response
[30].
Occurring simultaneously with the described cellular events, after PDT treatment, lipids are produced, as well as pro-inflammatory cytokines, such as IL-1β and IL-8, demonstrating that therapy has a significant effect on the immune system
[25][26][27]. Moreover, since a balance between the synthesis and degradation of extracellular matrix is required, it is evident that PDT modulates the production of TGF-β
[30], the isoforms of which are involved in the deposition of collagen fibers
[25][26][27].
5. PDT and Chronic Wounds
Wounds that do not heal within 6/8 weeks are considered chronic
[31][32][33][34][35]. Numerous factors prevent wound healing. Among local factors, it is necessary to acknowledge the presence of foreign bodies, tissue maceration, ischemia, infection, and tissue hypoxia. Among the systemic factors, advanced age, malnutrition, diabetes, and renal disease are, without doubt, factors of primary importance. In addition, reduction in the secretion of tissue growth factors, the decompensation between the proteolytic enzymes and their inhibitors, and the presence of senescent cells in the microenvironment seem to be particularly important in the pathogenesis of chronic wounds
[31][32][33][34][35].
Chronic venous ulcers are associated with an extremely high psychosocial burden in terms of morbidity, loss of productivity, functional disability, and emotional distress, causing depression and social isolation. The difficulty, or even the impossibility, of treating these types of wounds leads to high costs, in terms of care, for the various communities
[31][32][33][34][35].
5.1. The Response of Cellular Infiltrate
Among the multiple properties of PDT, there is evidence of a strong cellular infiltrate response in the treated chronic wound (Figure 1C).
Moreover, in recent studies, it was found that, after PDT therapy in chronic wounds, there is a significant increase in certain inflammatory cells, such as TNF alfa+ MCs, T regs, plasmacytoid dendritic cells, MHCII positive dermal DCs
[30], and macrophages
[36], as well as an overall expression of TGF beta, which directly correlates with wound’s volume reduction
[30]. TGF beta seems to exert activities in early phases of wound healing, where it possibly promotes an epithelial–mesenchymal transition, allowing the migration of keratinocytes from the borders towards the wound’s bed
[37]. Finally, intercellular correlations between plasmacytoid dendritic cells and T reg have been found, confirming the fact that certain DC subsets are highly specialized in inducing regulatory T cell differentiation and, in some tissues, the local microenvironment plays a role in driving DCs towards a tolerogenic response
[38][39].
5.2. Neuroimmunomodulation
In healing wounds, the activity of immune system is certainly modulated by the nervous system
[40][41][42], and delayed wound healing is observed in animal models after surgical resection of cutaneous nerves
[41][42]. Sensory neurons possess several means of detecting the presence of noxious or harmful stimuli: (1) cytokine receptors, such as IL-1β and TNFα, recognize the factors secreted by immune cells (e.g., IL-1β, TNFα, nerve growth factor), which activates MAP kinases and other signaling mechanisms to increase membrane excitability; (2) distress signal receptors, including TRP channels, P2X channels, and DAMPs, recognize exogenous signals from the environment (e.g., heat, acidity, chemicals) and signals endogenous hazards released during trauma or tissue injury (for example, ATP or uric acid)
[43]. Studies have demonstrated that the stimulation of dorsal roots induces cutaneous vasodilation and enhancement of inflammatory processes
[43], consisting of (a) chemotaxis and subsequent activation of neutrophils, macrophages, and lymphocytes at the site of injury; (b) degranulation of MCs; (c) an increase in blood flow, which also allows easier recruitment of inflammatory leukocytes; and (d) dendritic cell activation and subsequent T helper cell differentiation
[30][44][45]. An example of this relationship is demonstrated by a recent study
[46], where it was investigated, in PDT-treated chronic wounds, MC interaction with neurons containing neurotransmitters involved in wound healing processes. The results demonstrate that, in chronic wounds treated with PDT, there is an increase in neuronal populations containing mediators involved in wound healing, as well as that relating to the percentage of MCs containing NGF and VIP. This mean that the effects of PDT chronic wounds is probably due to neuronal activation; consequently nervous fibers can activate other cells involved in wound healing including MCs.
 +1 credit
+1 credit