Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Zhaniya Khaibullina | -- | 2528 | 2022-04-13 10:35:33 | | | |
| 2 | Vivi Li | -175 word(s) | 2353 | 2022-04-13 11:56:55 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Khaibullina, Z.; Anchita, A.; , .; Persson, K.M.; Tussupova, K. Health Impact of Drying Aral Sea: One Health. Encyclopedia. Available online: https://encyclopedia.pub/entry/21700 (accessed on 08 August 2026).
Khaibullina Z, Anchita A, , Persson KM, Tussupova K. Health Impact of Drying Aral Sea: One Health. Encyclopedia. Available at: https://encyclopedia.pub/entry/21700. Accessed August 08, 2026.
Khaibullina, Zhaniya, Anchita Anchita, , Kenneth M. Persson, Kamshat Tussupova. "Health Impact of Drying Aral Sea: One Health" Encyclopedia, https://encyclopedia.pub/entry/21700 (accessed August 08, 2026).
Khaibullina, Z., Anchita, A., , ., Persson, K.M., & Tussupova, K. (2022, April 13). Health Impact of Drying Aral Sea: One Health. In Encyclopedia. https://encyclopedia.pub/entry/21700
Khaibullina, Zhaniya, et al. "Health Impact of Drying Aral Sea: One Health." Encyclopedia. Web. 13 April, 2022.
Copy Citation
Once one of the largest saline lakes, the Aral Sea, was recognized as a significant environmental disaster as the water level decreased dramatically. Water level decrease increases water salinity, affecting biodiversity. Exposed lake beds become the source for fine dust picked up by the dust storms and spread across a long distance, affecting people’s health in surrounding areas.
Aral Sea desiccation
water pollution
One Health approach
socio-economic aspects
Kazakhstan
1. Introduction
Environmental factors are significant contributors to the health of people [1]. About 23% of global deaths and 22% of global disability-adjusted life years (DALYs) were due to environmental risks in 2012, which could have been prevented [2]. As it is a concern for many countries, the “One Health” approach has been adopted by collaborating and coordinating the joint efforts of responsible authorities [3][4]. The idea represents the concept of “One Health for the entire ecosystem” as interventions and interconnections among living species. Thus, the main goal is to achieve the best health outcomes for people, animals, plants, and the environment through the cooperation of experts in human health (doctors, nurses, public health practitioners, epidemiologists), animal health (veterinarians, paraprofessionals, agricultural workers), environment (ecologists, wildlife experts), and other related areas of expertise.
While Sustainable Development Goal 3 (SDG 3) considers the importance of decreasing the risks for health caused by air and water pollution, SDG 6 ensures the health of water resources and the sustainable and universal access of everyone to safe water and sanitation [5][6]. According to The Global Burden of Diseases, Injuries, and Risk Factors Study [7], water pollution caused 1.8 million deaths in 2015 compared to 0.84 million in 2012. Consequently, effective handling of domestic, industrial, and agricultural pollution emissions provides benefits for the environment and public health [8].
Once one of the largest saline lakes, the Aral Sea, has been recognized as one of the significant environmental disasters as the water level decreased dramatically in recent years [9] and is one of the examples of a clearly unsustainable case [10]. Water withdrawal for irrigation was a primary reason for the desiccation of the lake. The decrease in water level causes an increase in water salinity and consequently affects biodiversity. In many related cases, the shrinking of saline lakes speeds up the anthropogenic impact rather than the long-term effect of climate change [11][12]. The salt crusts, formed on the dry bottom of the former lake, are rich in various minerals like sodium, chloride, magnesium, calcium, sulfates, borate, lithium and potassium [13]. Minerals from Lake Munclin (Sahara desert) and the Dead Sea are used as fertilizer, salt from Lake Minchin, at present called Salar de Uyuni salt pan in Bolivia, is extracted for table salt and lithium and Bristol Lake in California is extracted for industry and food products [14] and salts from the shrunk bottom of Lake Zuni are used for pharmaceutical purposes [15]. Therefore, several economic benefits due to desiccation, such as mineral extraction, might contradict direct economic losses of affected fisheries, collapsed infrastructure, deteriorated ecosystems, and subsequent environmental costs, like in the Aral Sea case [16].
2. The Aral Sea and Its Related Health Issues
The exposed bottom of the Aral Sea had a dry salt crust and numerous pollutants. The dust storms carried these contaminated salts and deposited them on land surfaces, reportedly causing several health issues like disability, reproductive and tumors to the people living in the Aral Sea region. Numerous studies conducted by scientists show that the population’s state of health in the Aral Sea region has continued to deteriorate in recent decades [17]. The following sections detail the health conditions of the population in the Aral Sea region.
2.1. Respiratory Disorder
The spread of atmospheric air pollution caused by dust storms has led to respiratory diseases such as chronic bronchitis, bronchial asthma, and tuberculosis. Instead, there is a belief that dust storms cause respiratory diseases, several researchers just describe the issue generally, without detail investigations for the case of Kazakhstan [17][18][19][20]. Gazizova [21] analyzed retrospective data about respiratory diseases among the adult population of the Aral Sea zone between 1991 and 2016. A growth of respiratory diseases was detected in the catastrophe zone from 9467 diagnosed people (per 100 thousand population) in 1991 to 10,744 (per 100 thousand) in 2016. The number of people with respiratory diseases in the catastrophe zone in 2016 slightly varied with the number of people diseased in the crisis (9247) and pre-crisis (9079) zones. The number of people in the control zone differed significantly—5879 people per 100,000 population. The respiratory and pulmonary functions were studied by researchers [22] among the children at the Catastrophe zone. 8.1% of the surveyed kids in the study area found chronic cough in the study area, compared with 4.6% in the reference area. The study considered subjects from 200 km and 500 km from the Aral Sea. Some investigations have been carried out in neighborhood countries. An annual analysis of asthmatic status in Central Asia found that about 113 per 100,000 people suffered from asthma in the Khorezm region (Uzbekistan), which is more than three times higher than the national average (38 incidences per year 100,000 of the population). In Karakalpakstan, it was 67 per 100,000 people which is twice the national average [23]. Researchers Kunii et al. and Bennion et al. conducted studies in Uzbekistan during 2000 to find the connection between the dust storms and respiratory disorders among the children residing near the Aral Sea [22][24].
The results of these studies show no strong connection between dust storms and respiratory disorders. However, this does not mean that the sandstorms are harmless. Even though no direct connection to respiratory diseases was found, the dust storms could indirectly affect the Aral Sea region’s demographics.
2.2. Disabilities
The analysis of the results [25] for the study period 2004–2013 revealed the prevalence of 6 classes of pathology: cardiovascular diseases were perhaps highest, respiratory diseases on the second highest, vision pathologies on the third, and mental disorders were in the fourth most prevalent. The malignant neoplasms followed the rank, with injuries being the last. The disability rate in three zones as compared to the control region is shown in Figure 1 [26]. It can be seen that the incidence rates of respiratory disabilities were highest in the catastrophe zone; cardiovascular and psychological disabilities were peaking in the crisis zone.
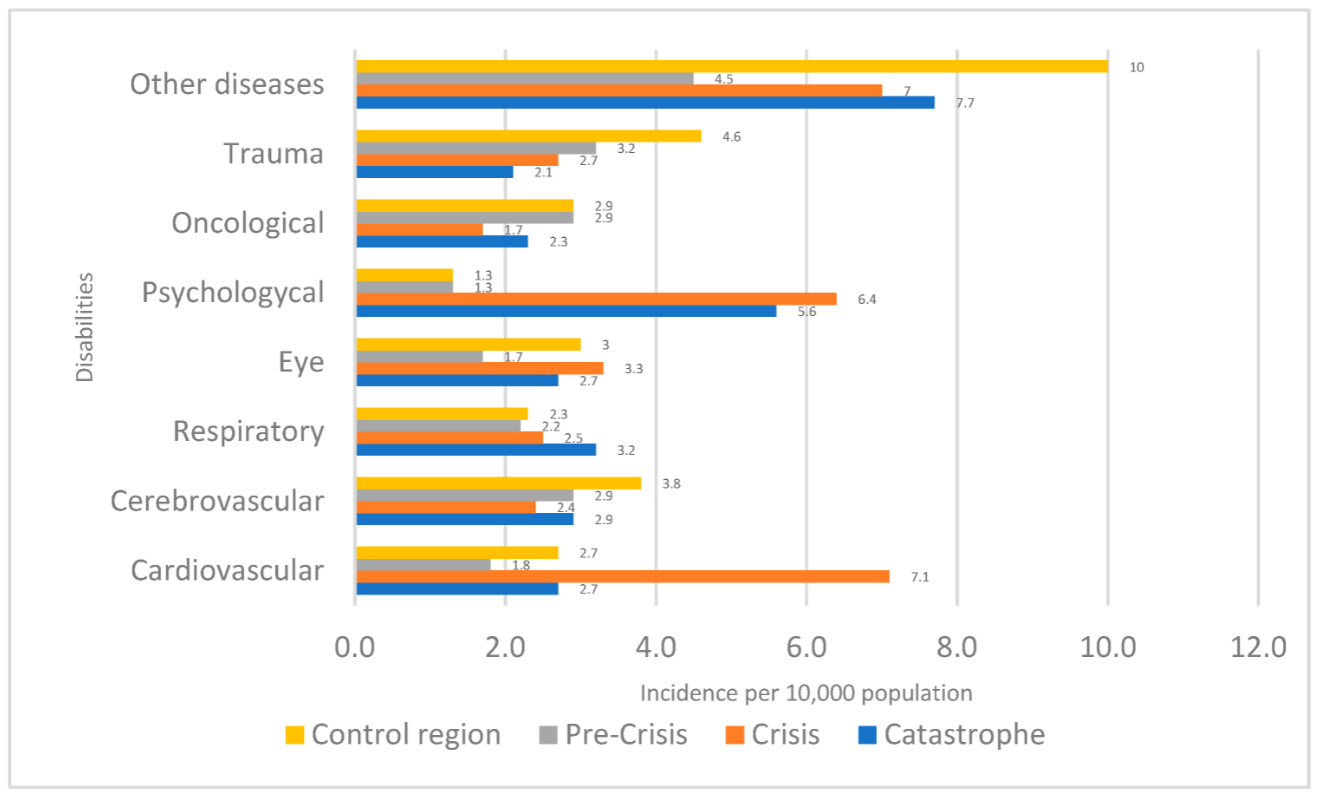
Figure 1. The structure of the primary disability of adults per 10,000 of the population in the Aral Sea region for the years 2004–2013.
The study also calculated the prediction of disability occurrence until 2023 based on the disabilities observed from 2004 to 2013. The predicted incidence of disability for the year 2023 shows a 28.1% increase in the Aral Sea region, 28.4% increase in the Kazalinsk, 7.9% increase in the Shalkar, 46.4% increase in the Karmakshy, 30.9% increase in Zhalagash, 43.7% increase in Arys, 23.1% in Irgyz, and 39.1% increase in Ulytau region. However, this is too rough of an estimation, which does not account for risk factors, the demographic structure of the population, and the curve of the disability distribution. That is why this prediction should be interpreted accordingly.
2.3. Incidence of Cancer
Malignant neoplasm (cancerous tumor) [27] is another health disaster to be considered while analyzing the health effects in the Aral Sea region. To analyze malignant neoplasm incidence, the data of a 10-year (2004–2013) timeframe were considered. The data were reported to be taken from local oncology dispensaries. Figure 2 shows the ten-year average malignant neoplasm incidence in the three disaster zones (catastrophe, crisis and pre-crisis as described in Figure 3), Zhanaarka district, and the whole of the Republic of Kazakhstan for comparison purposes. The incidence rates are calculated for 100,000 populations residing in the regions mentioned above.
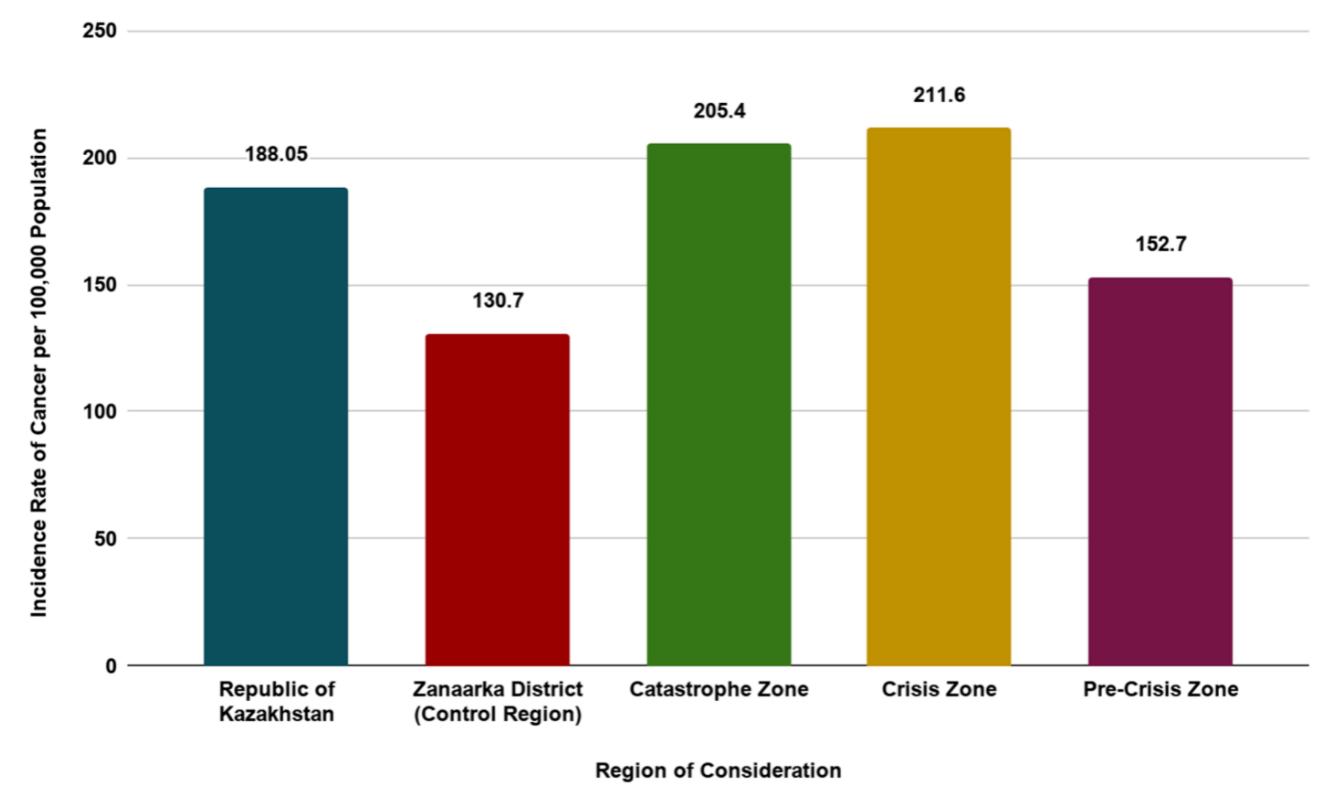
Figure 2. Ten-year annual average of cancer incidence rates 100,000 people for the period 2003–2014 [25].

Figure 3. The study area of the Aral region in Kazakhstan, Kyzylorda region.
The catastrophe and the crisis zones have 61.9% (211.6) and 57.2% (205.4) per 100,000 population increased incidence rate of malignant neoplasm, respectively, when compared to the control region (130.7). The incidence rate in the pre-crisis region is 152.7 for 100,000 population, which is 16.8% higher when compared to the control region but is 18.8% lower than the Republic of Kazakhstan. The detailed observations from individual locations showed the controversial picture.
As discussed previously, the incidence of cancer in the catastrophe zone was notably higher than in the control region. The three districts belonging to the catastrophe zone are Aral, Kazalinsk, and Shalkar. The malignant neoplasm incidents observed in the Aral region were 225.8 per 100,000 population, in Kazalinsk was 200.2 per 100,000 population and in Shalkar, it was 179.9 per 100,000 population. These observations are 1.7, 1.5 and 1.4 times greater, respectively, compared to the control region, Zhanaarka (130.7 per 100,000 population), while the value in Kazakhstan was 188 per 100,000 population.
Similarly, the observations made at the crisis zone are higher than the control region and the Republic of Kazakhstan. The incidence observed in the Zhalagash, Karmakshy, and Shieli regions was 1.65, 1.69 and 1.53 times greater than the control region.
For the pre-crisis zone, which comprises Arys, Irgiz, and Ulytau, the observed cancer incidence was 153.3, 202.2, and 102.6, respectively. Only the Ulytau region has cancer incidence less than the control region. Arys and Irgiz have 1.17 and 1.54 times more than the incidence rates observed in the Zhanaarka region. As for the Ulytau region, the incidence rates observed for the period 2003–2014 were 1.27 times less than the control region and 1.84 times less than the Republic of Kazakhstan.
Another research study [28][29] has collected data on multiple types of cancer that affected the population of the Aral Sea region. These data were collected for 11 years starting from 1999 and lasting until the end of 2009. Figure 2 shows the distribution of types of cancer observed during this time period. A total of 10,382 cancer incidents was recorded. Among these, esophagus cancer is the most prominent with a 17.8% occurrence rate, at second and third positions, lung cancer and cancer of the stomach have a close 12.7% and 12.6% occurrence rates. These forms of cancer were prominent during the 1999 to 2009 period.
2.4. Reproductive System
In the Aral Sea region, it was found that there was a decrease in life expectancy among the demographic indicators along with a high perinatal and infant mortality [30]. Out of the 19,561 mortality cases between 1999–2008 in the Kyzylorda region, 16.1% (3155) were women of reproductive age (15–49 years) [31]. The average annual mortality rate for women in the Kyzylorda region at the fertile age was 1.98 ± 0.05 per 1000 population, decreasing the dynamics for 1999–2008 by 2.15%. High mortality rates of 4.51 ± 0.17 per 1000 population were established in 45–49 years [32]. According to the survey performed on women’s reproductive stage in Kazakhstan, the women in the Aral region, compared to other parts of the Soviet region, faced later menarche, menstrual disorders, and spontaneous miscarriages. At the same time, a positive trend in reproductive behavior was observed. The optimal reproductive age was between 20 to 34 years of age, among 88.2% of the laboring population of women. The usage of contraceptives was relatively high for the region (intrauterine device in 32.1%) and the frequency of abortions was low (5.5%) [33].
The onset of pregnancy in most women occurs against a background of irregularities in the hematopoietic, pituitary-thyroid, and immune systems. During pregnancy time, women got affected due to improper intake of nutrition. Meanwhile, babies’ immune systems are threatened by lack of breastfeeding because of long-term exposure to pesticides in the Aral Sea region [34][35][36]. Such compounds accumulate in fetuses through the placenta and breastfeeding in the postnatal period. Hence, researchers can say that adverse environmental factors and toxicants significantly impact women’s reproductive health [37][38].
However, the studies conducted in this discipline are limited, thus making it challenging to draw well-grounded conclusions.
2.5. Psychological Disorder
A psychological disorder is a wide range of conditions that affect an individual’s mood, thinking, and behavior. A number of cognitive disorders were revealed in the population of the Aral Sea region, for instance, a decrease in short-term memory, long-term memory and attention span, different psycho-emotional disorders and depression.
During May 1999, a study [39] was conducted to determine the connection between the drying of the Aral Sea and the mental health of the population surrounding it. It was an interview survey involving 118 randomly selected individuals in Karakalpakstan. The survey included a general health questionnaire, Somatic Symptom CheckList-90 (SCL-90, which is a psychometric self-report designed to evaluate a broad range of psychological problems) and questions about the perception of the environmental disaster and social support. 41% of participants reported concerns regarding environmental issues, and 48% reported stages of somatic symptoms connected with mental distress, which was above the standardized cut point; cut-point refers to a mean score above the population norm, signifying a probable case of emotional distress manifested in somatic symptoms [40].
Another research study [41] compared the available clinical records of the Aral zone and Kyzyl-Orda zone in Kazakhstan to understand the mental and behavioral conditions of the population inhabiting the regions mentioned above. It was reported that the Aral zone had about 1.4 times more occurrence of psychological disorders (642.9 cases per 1000 population) than in the Kyzyl-Orda zone in Kazakhstan (451.5 cases per 1000 population).
Psychological disorders observed around the Aral Sea region could be an example of the indirect effects of dust storms. The dust storms deposit harmful chemicals on the fertile soil bringing about a decline in agricultural production. The inhabitants of the region who were dependent on agriculture were now unemployed. Poor economic conditions, unemployment and deteriorating health conditions take a toll. These factors could lead to increased stress and depression. However, these survey-based studies are heavily reliant on the self-assessment of the patient. There is no solid standard to weigh the opinion of a patient. Moreover, these studies are cross-sectional with randomly selected participants; thus, the selection of patients for the study, the socio-economic conditions of the selected population and several other factors act as uncontrollable variables, thus making the result of the study less reliable.
2.6. Nervous System
The role of environmental factors in developing neurodegenerative diseases of the nervous system has been repeatedly emphasized. Recent literature finds the association between the environmental factors and multiple sclerosis [42][43][44] among the population and Parkinson’s disease [45].
The adverse effect of environmental factors is indicated by an increase in central nervous system disorders like mental disorders and decreased intelligence [46]. Highly toxic substances such as lead, nickel and chromium cause asthenia and psychogenic disorders [47]. The prevalence of depressive personality disorders in the Catastrophe zone exceeds that of the Control zone by almost three times, the prevalence of anxiety disorders by 2.5 times and depressive disorders by more than two times.
References
- Brulle, R.J.; Pellow, D.N. Environmental justice: Human health and environmental inequalities. Annu. Rev. Public Health 2006, 27, 103–124.
- Pruss-Ustun, A.; Wolf, J.; Corvalan, C.; Neville, T.; Bos, R.; Neira, M. Diseases due to unhealthy environments: An updated estimate of the global burden of disease attributable to environmental determinants of health. J. Public Health UK 2017, 39, 464–475.
- CDC. One Health Basics. Available online: https://www.cdc.gov/onehealth/basics/index.html (accessed on 11 October 2021).
- WHO. One Health. Available online: https://www.who.int/news-room/q-a-detail/one-health (accessed on 11 October 2021).
- SDG 3: Ensure Healthy Lives and Promote Wellbeing for All at All Ages. Available online: https://www.who.int/health-topics/sustainable-development-goals#tab=tab_1 (accessed on 11 October 2021).
- SDG 6: Ensure Availability and Sustainable Management of Water and Sanitation for All. Available online: https://sdgs.un.org/goals/goal6 (accessed on 11 October 2021).
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724.
- Larsen, T.A.; Hoffmann, S.; Luthi, C.; Truffer, B.; Maurer, M. Emerging solutions to the water challenges of an urbanizing world. Science 2016, 352, 928–933.
- Micklin, P. The Aral Sea disaster. Annu. Rev. Earth Planet Sci. 2007, 35, 47–72.
- Kundzewicz, Z.W. Water resources for sustainable development. Hydrol. Sci. J. 1997, 42, 467–480.
- Tussupova, K.; Anchita; Hjorth, P.; Moravej, M. Drying lakes: A review on the applied restoration strategies and health conditions in contiguous areas. Water 2020, 12, 749.
- Wurtsbaugh, W.A.; Miller, C.; Null, S.E.; DeRose, R.J.; Wilcock, P.; Hahnenberger, M.; Howe, F.; Moore, J. Decline of the world′s saline lakes. Nat. Geosci. 2017, 10, 816–821.
- Jellison, R.; Williams, W.D.; Timms, B.; Durand, J.A.; Aladin, N.V. Salt lakes: Values, threats and future. In Aquatic Ecosystems: Trends and Global Prospects; Cambridge University Press: Cambrigde, UK, 2008; pp. 94–110.
- Jones, B.; Deocampo, D. Geochemistry of saline lakes. Treatise Geochem. 2003, 5, 605.
- Scurlock, D. From the Rio to the Sierra: An Environmental History of the Middle Rio Grande Basin; US Department of Agriculture, Forest Service, Rocky Mountain Research Station: Fort Collins, CO, USA, 1998.
- Gross, M. Feature the world′s vanishing lakes. Curr. Biol. 2017, 27, R43–R46.
- Trasande, L.; Thurston, G.D. The role of air pollution in asthma and other pediatric morbidities. J. Allergy Clin. Immunol. 2005, 115, 689–699.
- Micklin, P. The Aral Sea Crisis; Springer: Dordrect, The Netherlands, 2004; pp. 99–123.
- Micklin, P. The Aral Sea crisis and its future: An assessment in 2006. Eurasian Geogr. Econ. 2006, 47, 546–567.
- Whish-Wilson, P. The Aral Sea environmental health crisis. J. Rural Remote Environ. Health 2002, 1, 29–34. Available online: https://www.cabdirect.org/cabdirect/abstract/20083221094 (accessed on 11 October 2021).
- Gazizova, A.O. Effect of Salt-Dust Aerosol of the Aral Sea on Respiratory Organs (Experimental Study). Ph.D. Dissertation, Karaganda Medical University, Karagandy, Kazakhstan, 2018.
- Kunii, O.; Hashizume, M.; Chiba, M.; Sasaki, S.; Shimoda, T.; Caypil, W.; Dauletbaev, D. Respiratory symptoms and pulmonary function among school-age children in the Aral Sea region. Arch. Environ. Health 2003, 58, 676–682.
- Cerny, A. The Tragedy of the Aral: Counting on Cotton, a Region Loses its People. In Disaster by Design: The Aral Sea and its Lessons for Sustainability. Research in Social Problems and Public Policy; Edelstein, M.R., Cerny, A., Gadaev, A., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2012; Volume 20, pp. 223–250.
- Bennion, P.; Hubbard, R.; O′Hara, S.; Wiggs, G.; Wegerdt, J.; Lewis, S.; Small, I.; van der Meer, J.; Upshur, R.; on behalf of the Médecins san Frontières/Aral Sea Respiratory Dust and Disease project team. The impact of airborne dust on respiratory health in children living in the Aral Sea region. Int. J. Epidemiol. 2007, 36, 1103–1110.
- Karaganda State Medical University (KSMU). Comprehensive Approaches to the Management of the Health Condition of Population of the Aral Sea Region; Scientific technical project report; Karaganda State Medical University (KSMU): Karaganda, Kazakhstan, 2015 October. (In Russian)
- Sakiev, K.Z.; Otarbayeva, M.B.; Grebeneva, O.V.; Zhanbasinova, N.M.; Amanbekov, U.A.; Tatkeev, T.A.; Namazbayeva, Z.I. Managing health state of Aral region population. Russ. J. Occup. Health Ind. Ecol. 2015, 7, 19–23.
- Mamyrbayev, A.; Djarkenov, T.; Dosbayev, A.; Dusembayeva, N.; Shpakov, A.; Umarova, G.; Drobchenko, Y.; Kunurkulzhayev, T.; Zhaylybaev, M.; Isayeva, G. The incidence of malignant tumors in environmentally disadvantaged regions of Kazakhstan. Asian Pac. J. Cancer Prev. 2016, 17, 5203.
- Igissinov, S.; Igissinov, N.; Moore, M.A.; Kalieva, Z.; Kozhakhmetov, S. Epidemiology of esophageal cancer in Kazakhstan. Asian Pac. J. Cancer Prev. 2012, 13, 833–836.
- Igissinov, N.; Igissinov, S.; Moore, M.A.; Shaidarov, M.; Tereshkevich, D.; Bilyalova, Z.; Igissinova, G.; Nuralina, I.; Kozhakhmetov, S. Trends of prevalent cancer incidences in the Aral-Syr Darya ecological area of Kazakhstan. Asian Pac. J. Cancer Prev. 2011, 12, 2299–2303. Available online: https://pubmed.ncbi.nlm.nih.gov/22296374/ (accessed on 11 October 2021).
- Crighton, E.J.; Barwin, L.; Small, I. What have we learned? A review of the literature on children’s health and the environment in the Aral Sea area. Int. J. Public Health 2011, 56, 125–138.
- Turdybekova, Y.G.; Dosmagambetova, R.S.; Zhanabayeva, S.U.; Bublik, G.V.; Kubayev, A.B.; Ibraibekov, Z.G.; Kopobayeva, I.L.; Kultanov, B.Z. The Health Status of the Reproductive System in Women Living In the Aral Sea Region. Open Access Maced. J. Med Sci. 2015, 3, 474–477.
- Safarova, G.L. Demography of aging: Current state and priority-driven research directions. Adv. Gerontol. 2011.
- Damalas, C.A.; Eleftherohorinos, I.G. Pesticide Exposure, Safety Issues, and Risk Assessment Indicators. Int. J. Environ. Res. Public Health 2011, 8, 1402–1419.
- Johnson, K.M.; Lichter, D.T. Rural depopulation: Growth and decline processes over the past century. Rural. Sociol. 2019, 84, 3–27.
- Bochkov, N.P. Ecological human genetics: Current problems and ways to solve them. Ecol. Genet. 2003, 5, 82.
- Singer, D.; Hunter, M. Premature Menopause: A Multi-Disciplinary Approach; Wiley: Hoboken, NJ, USA, 2000.
- Reimov, P.; Fayzieva, D. The Present State of the South Aral Sea Area. In The Aral Sea. Springer Earth System Sciences; Micklin, P., Aladin, N., Plotnikov, I., Eds.; Springer Earth System Sciences: Berlin/Heidelberg, Germany, 2014; Volume 10178.
- Turdybekova, Y.G.; Kopobayeva, I.L.; Kultanov, B.Z. Comparative Assessment of Women′s Reproductive Health in the Areas Bordering with the Aral Sea Region. Maced. J. Med. Sci. 2017, 5, 261.
- Crighton, E.J.; Elliott, S.J.; van der Meer, J.; Small, I.; Upshur, R. Impacts of an environmental disaster on psychosocial health and wellbeing in Karakalpakstan. Soc. Sci. Med. 2003, 56, 551–567.
- Derogatis, L.R.; Lipman, R.S.; Covi, L. SCL-90: An outpatient psychiatric rating scale–Preliminary report. Psychopharmacol. Bull. 1973, 9, 13–28.
- Mamyrbayev, A.; Dyussembayeva, N.; Ibrayeva, L.; Satenova, Z.; Tulyayeva, A.; Kireyeva, N.; Zholmukhamedova, D.; Rybalkina, D.; Yeleuov, G.; Yeleuov, A. Features of Malignancy Prevalence among Children in the Aral Sea Region. Asian Pac. J. Cancer Prev. APJCP 2016, 17, 5217–5221.
- Ghaisas, S.; Maher, J.; Kanthasamy, A. Gut microbiome in health and disease: Linking the microbiome-gut-brain axis and environmental factors in the pathogenesis of systemic and neurodegenerative diseases. Pharmacol. Therapeut. 2016, 158, 52–62.
- Chin-Chan, M.; Navarro-Yepes, J.; Quintanilla-Vega, B. Environmental pollutants as risk factors for neurodegenerative disorders: Alzheimer and Parkinson diseases. Front. Cell. Neurosci. 2015, 9, 124.
- Cannon, J.R.; Greenamyre, J.T. The role of environmental exposures in neurodegeneration and neurodegenerative diseases. Toxicol. Sci. 2011, 124, 225–250.
- Klingelhoefer, L.; Reichmann, H. Pathogenesis of Parkinson disease-the gut-brain axis and environmental factors. Nat. Rev. Neurol. 2015, 11, 625–636.
- Gordeev, S.A.; Posokhov, S.I.; Kovrov, G.V.; Katenko, S.V. Psychophysiological characteristics of panic disorder and generalized anxiety disorder. Neurol. Psychatr. 2013, 113, 11–14. Available online: https://pubmed.ncbi.nlm.nih.gov/23739496/ (accessed on 11 October 2021).
- Boxer, P.A. Occupational mass psychogenic illness. History, prevention, and management. J. Occup. Med. Off. Publ. Ind. Med Assoc. 1985, 27, 867–872.
- Alimbaev, T.; Omarova, B.; Tuleubayeva, S.; Kamzayev, B.; Aipov, N.; Mazhitova, Z. Ecological problems of water resources in Kazakhstan. E3S Web Conf. 2021, 244, 01004.
- Kamchatnov, P. Cognitive reserve, cognitive impairment and possibilities of their pharmacological correction. Zhurnal Nevrologii i Psikhiatrii Imeni SS Korsakova 2014, 114, 87–91. Available online: https://medi.ru/info/11548/ (accessed on 11 October 2021).
- Anarbekov, O.; Giska, S.; Dörre, A.; Cassara, M.; Beekma, J.; de Strasser, L.; Murzaeva, M. The Aral Sea Basin: Local and National Institutions and Policies Governing Water Resources Management; Routledge: Oxfordshire, UK, 2019; pp. 136–154.
- Rozanski, A.; Blumenthal, A.J.; Kaplan, J. Impact of Psychological Factors on the Pathogenesis of Cardiovascular Disease and Implications for Therapy. Circulation 1999, 99, 2192–2197.
- Iznak, A.F.; Iznak, E.V.; Sorokin, S.A. Dynamics and communication of parameters of cognitive evoked potentials and sensorimotor reactions in the treatment of apathetic depression. Neurol. Psychiatry 2011, 9, 52–57. Available online: https://www.mediasphera.ru/issues/zhurnal-nevrologii-i-psikhiatrii-im-s-s-korsakova/2011/9/031997-72982011910 (accessed on 11 October 2021).
More
Information
Subjects:
Water Resources
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
3.9K
Entry Collection:
Environmental Sciences
Revisions:
2 times
(View History)
Update Date:
13 Apr 2022
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No