 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Thomas Zellers | -- | 1471 | 2022-04-07 22:21:09 | | | |
| 2 | Lindsay Dong | + 5 word(s) | 1476 | 2022-04-08 08:51:25 | | |
Video Upload Options
Computed tomography (CT) and Cardiac magnetic resonance (CMR) continue to advance the field of congenital cardiology by allowing for new and unique procedures not previously imagined. Enabling the interventionalist to enter the catheterization lab with a plan of attack expedites the procedure and has been shown to reduce procedural times and improve outcomes. Substantial advances in cross-sectional image resolution with a significant decrease in radiation exposure for cardiac CTs have led to more mainstream utilization. CMR has a unique ability to deliver real-time functional imaging in several views without exposing the patient to the detrimental effects of ionizing radiation. This can reduce procedural times in the interventional fluoroscopic suite to allow for more directed procedures.
1. Background
2. Cross-Sectional Imaging in Pediatric Interventional Cardiac Catheterization
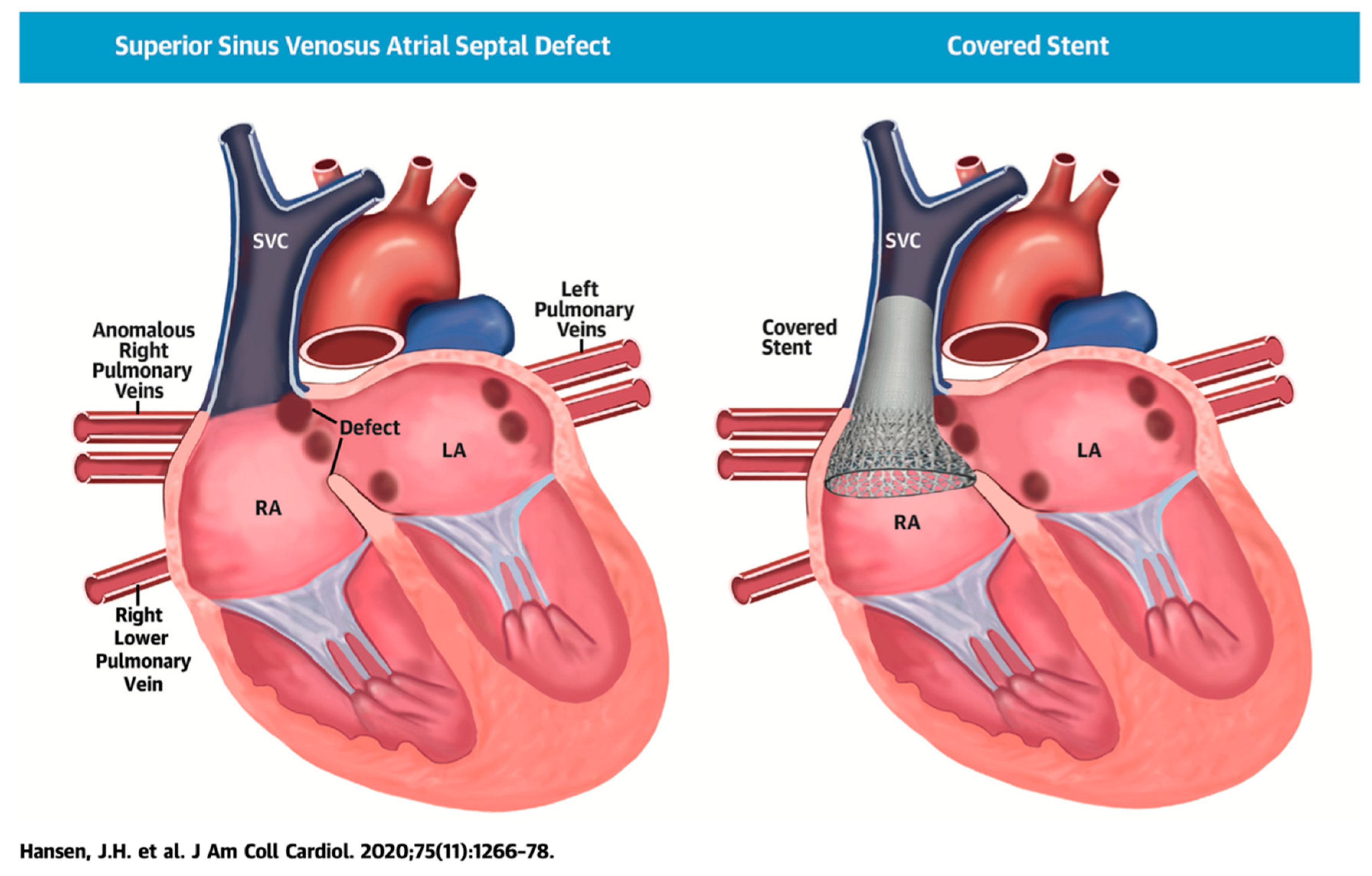
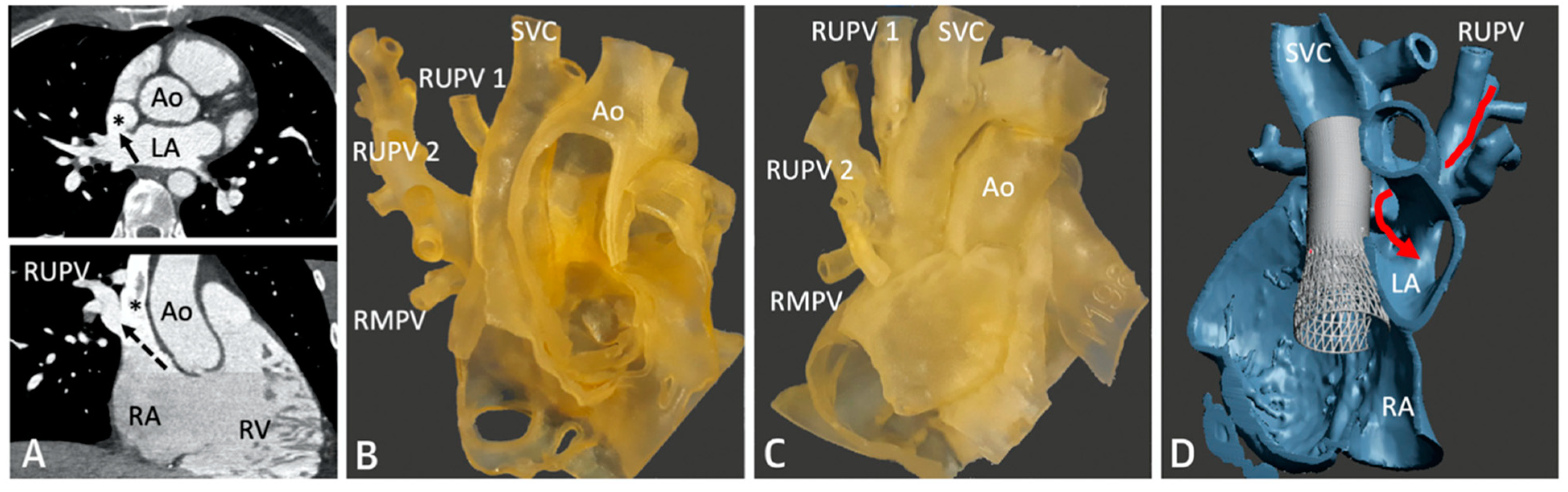
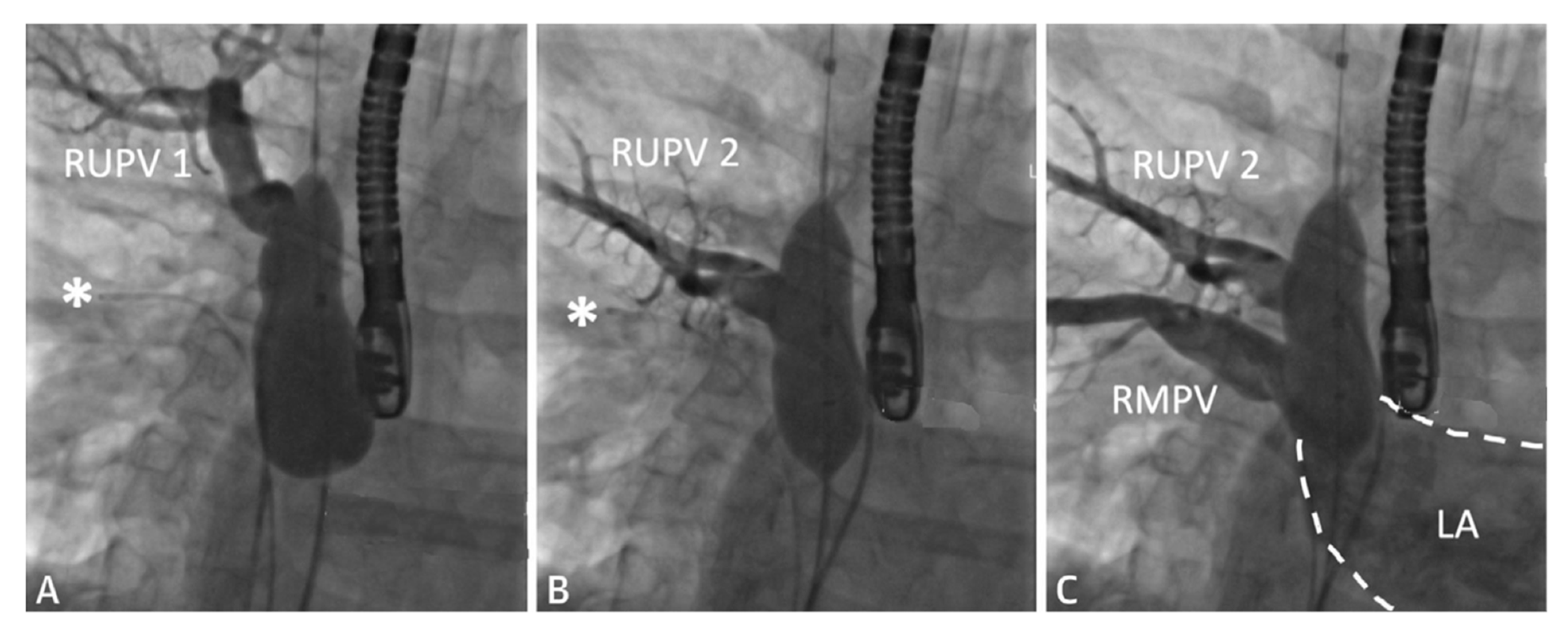
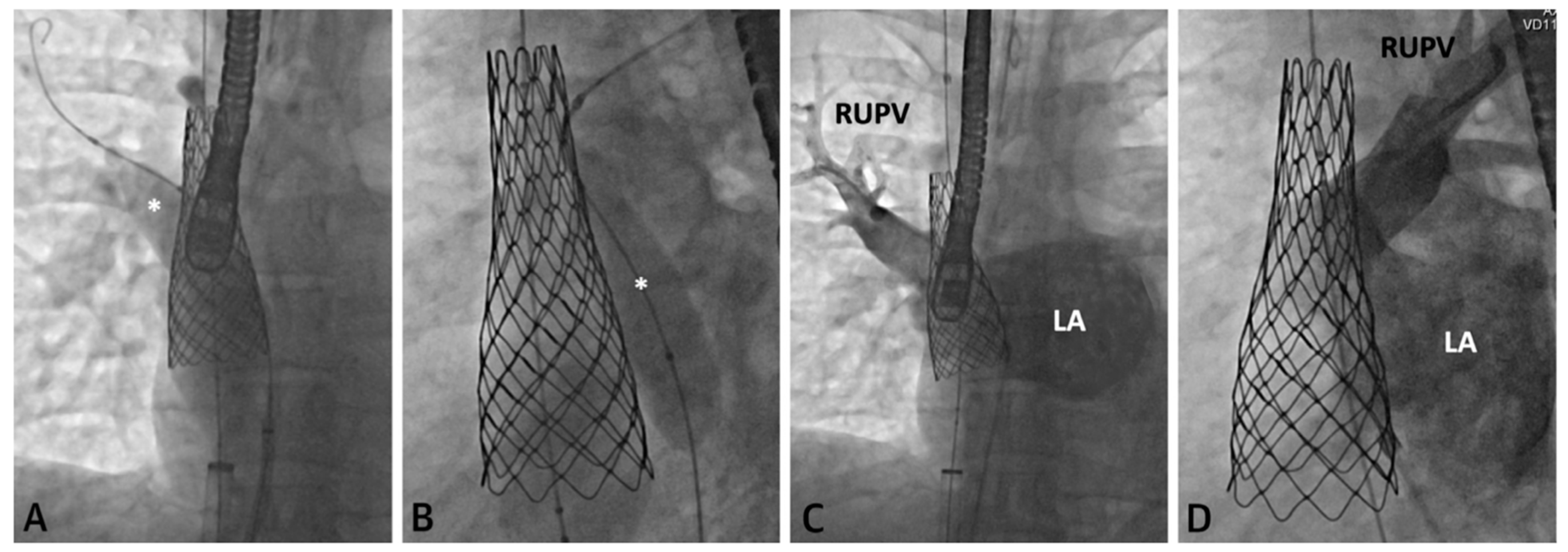
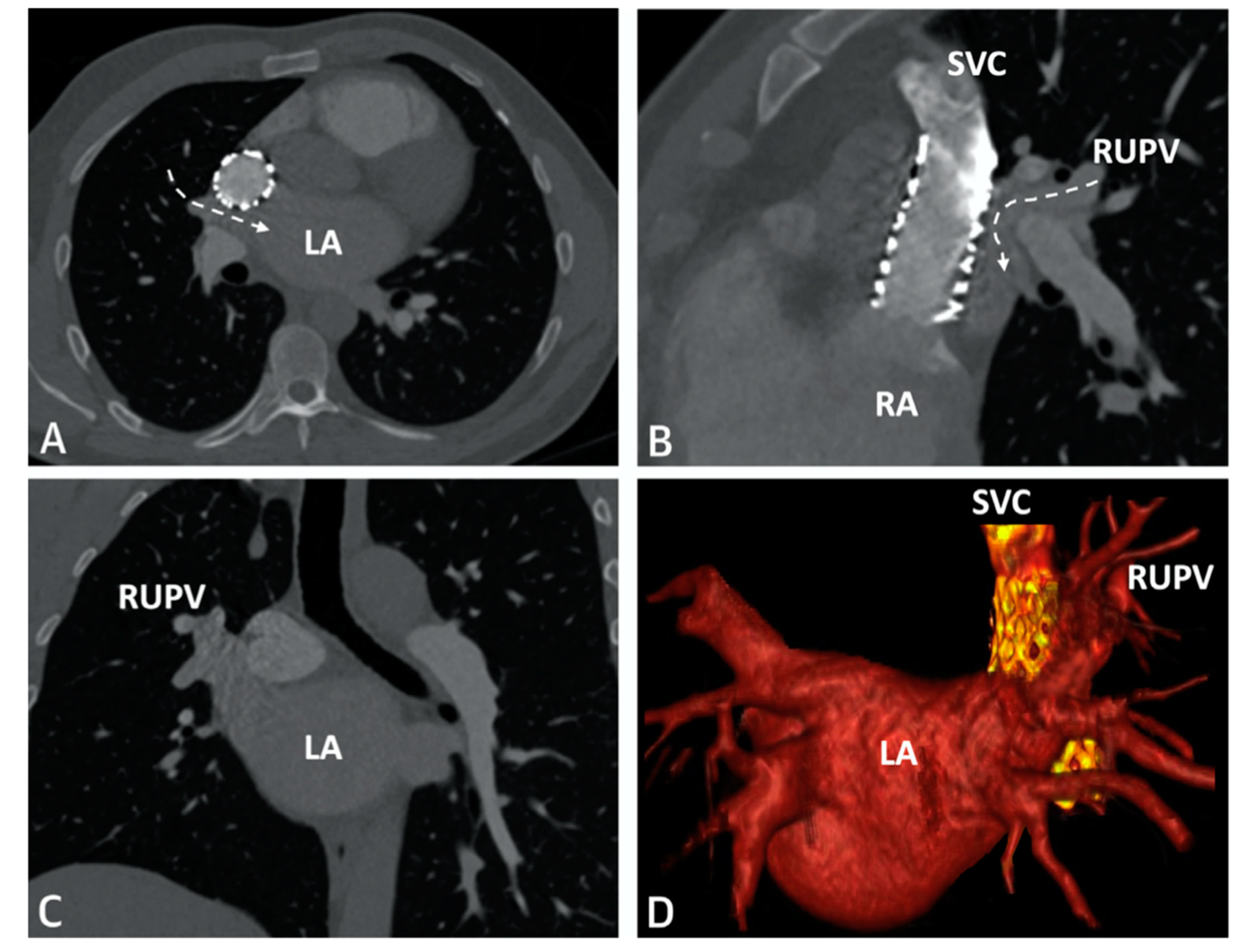
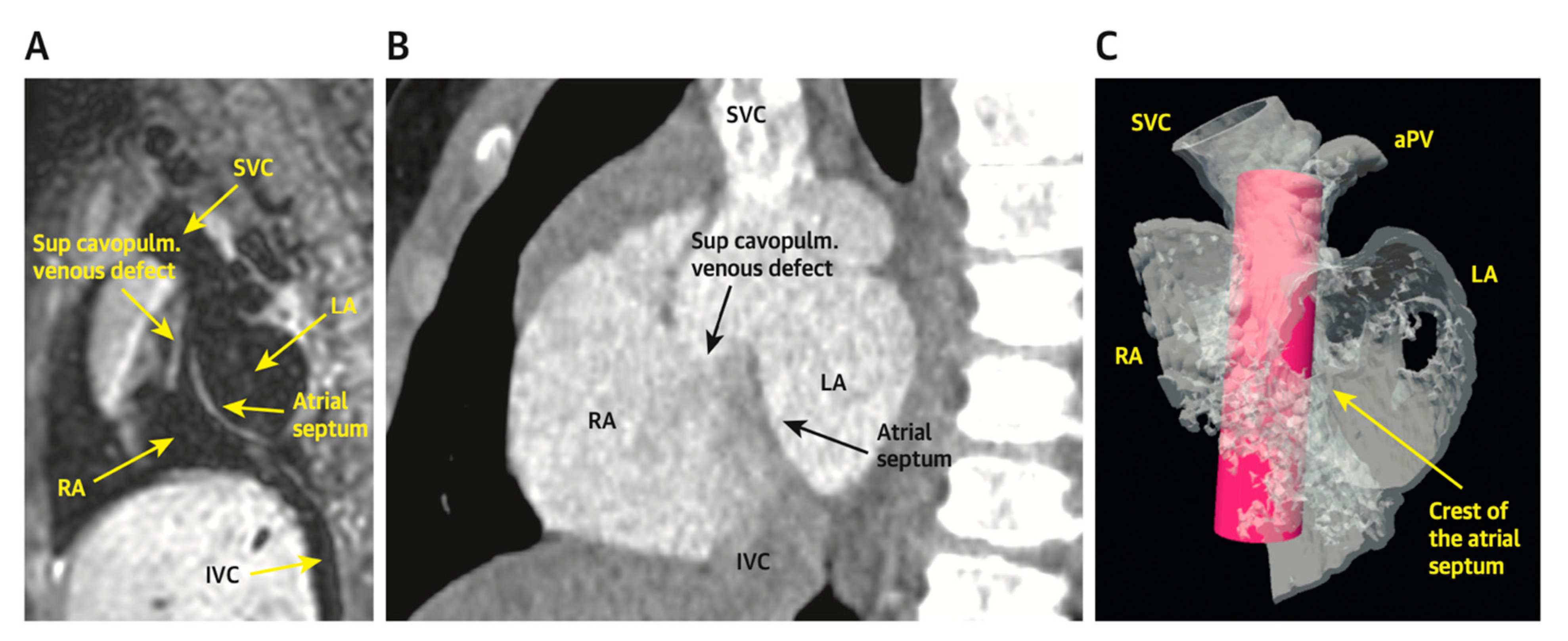
2.1. Sinus Venosus Atrial Septal Defect (SVASD)
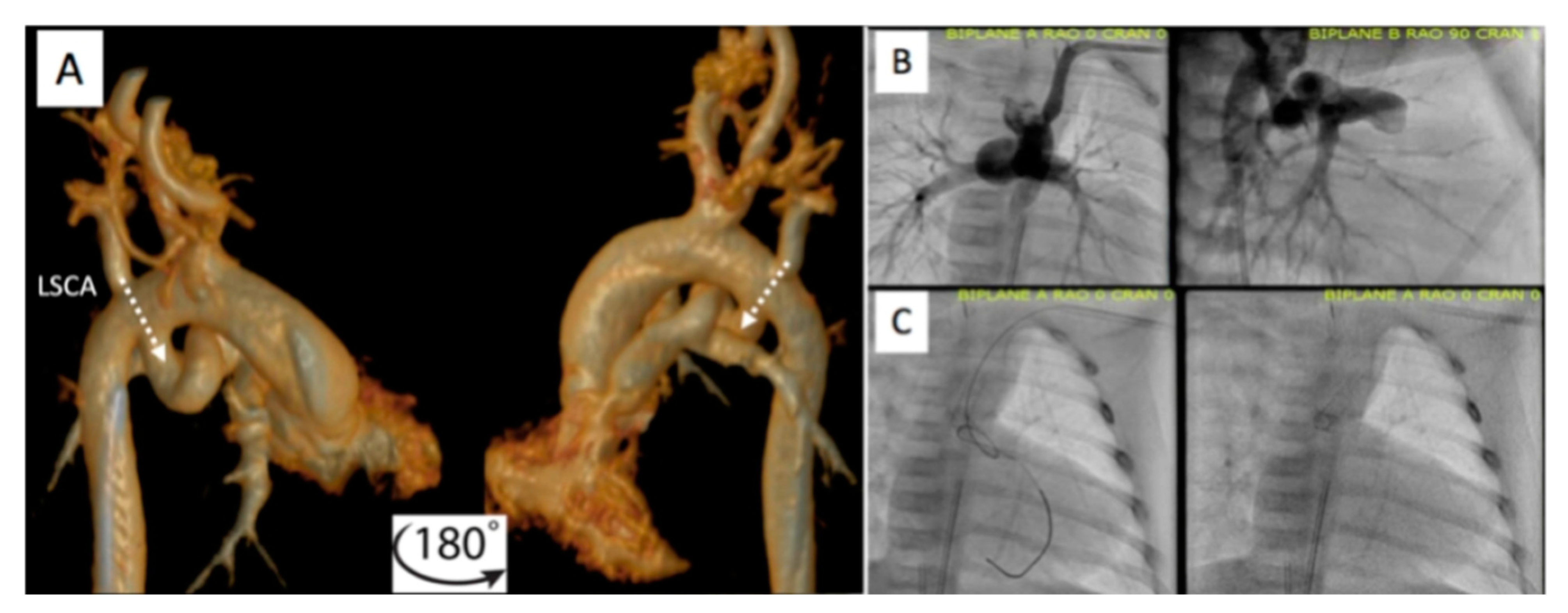
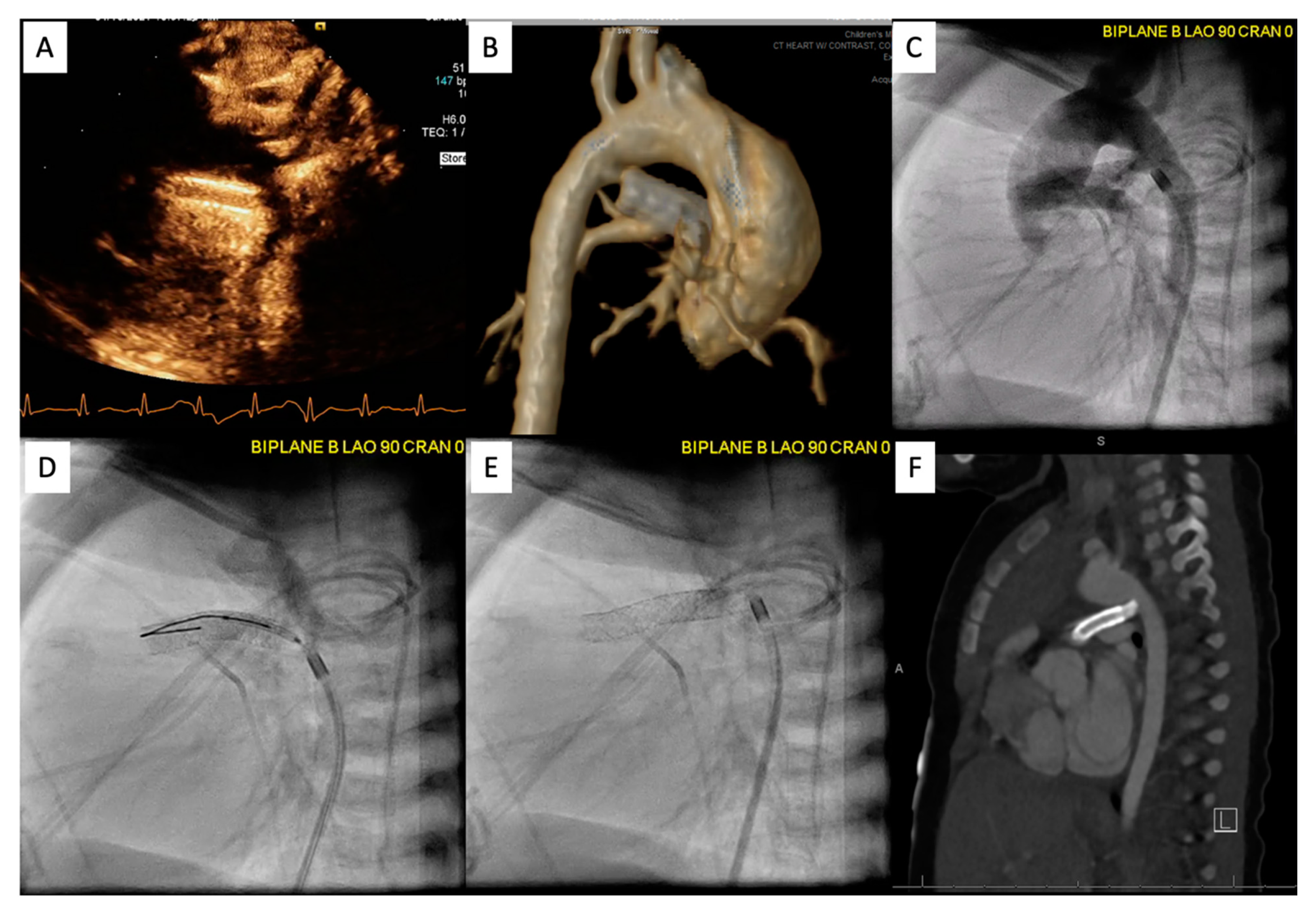
2.2. Patent Ductus Arteriosus (PDA) Stenting for Ductal-Dependent Pulmonary Blood Flow
2.2.1. Pre-Procedural
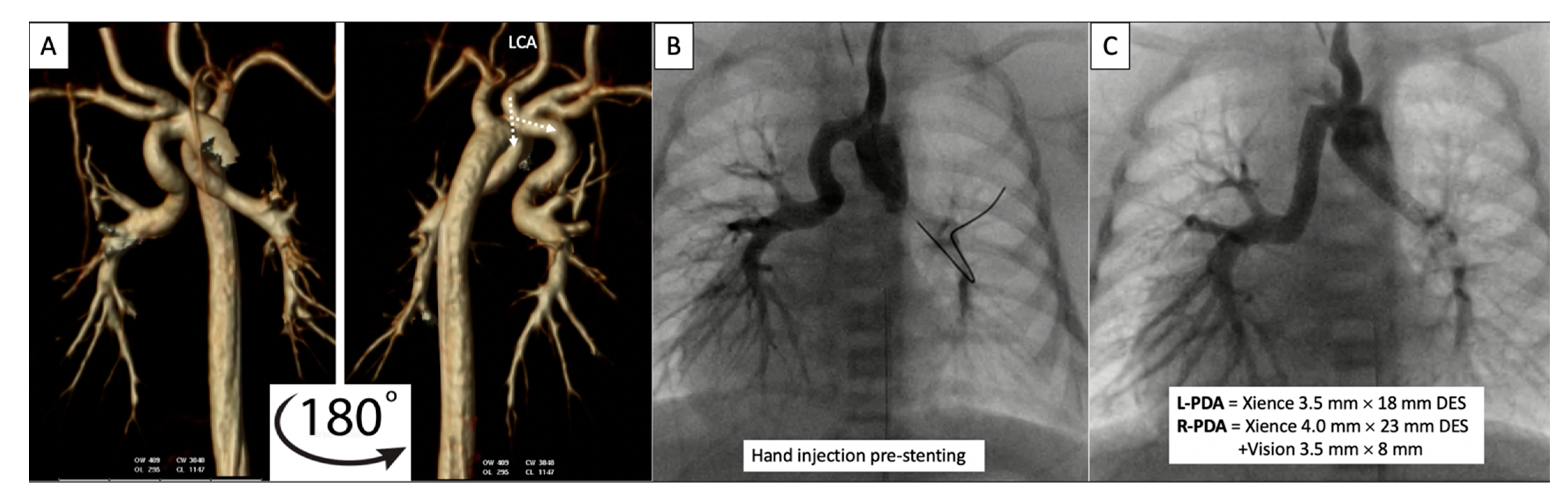
2.2.2. Post-Procedural
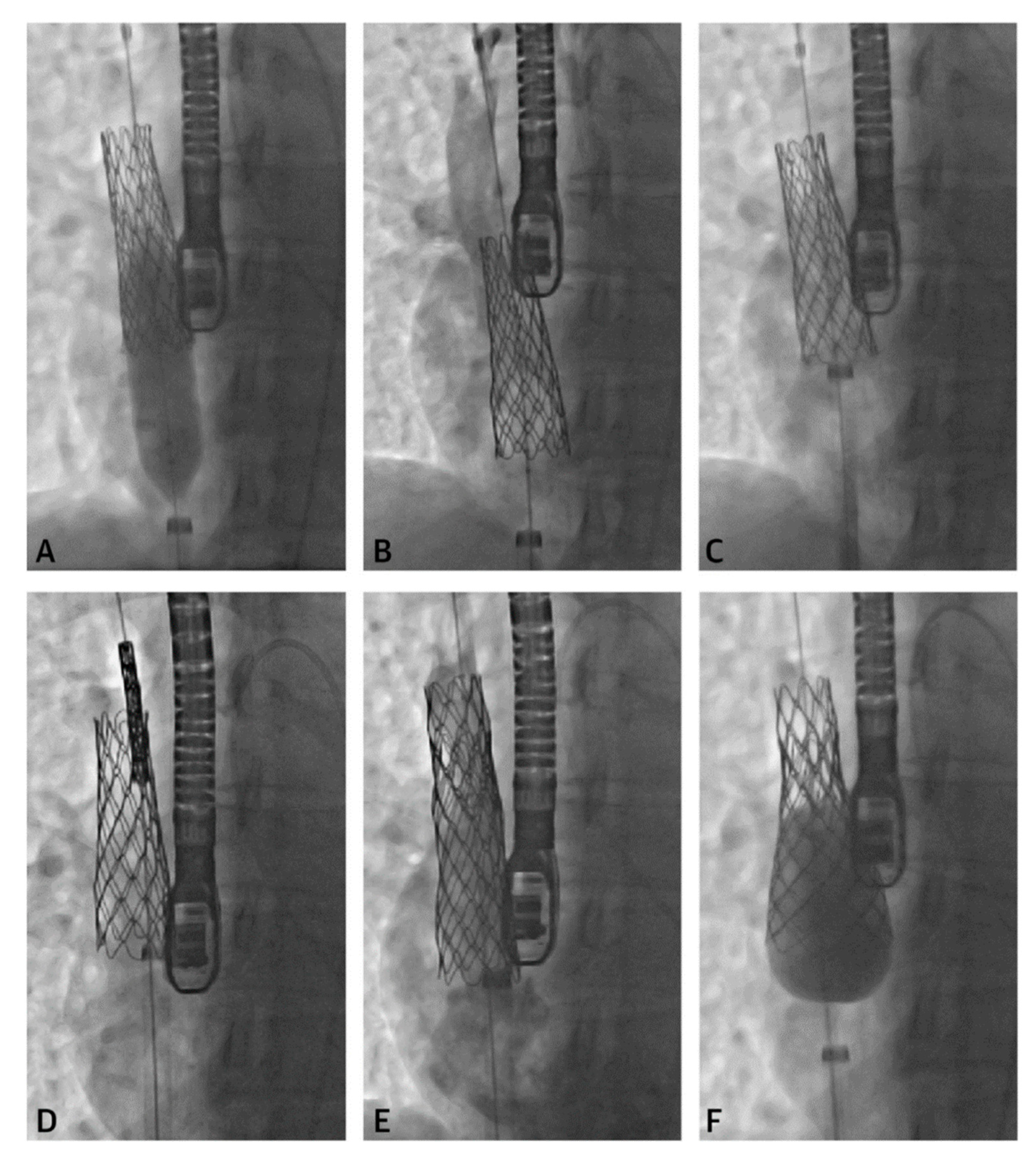
2.3. Percutaneous Pulmonary Valve Placement
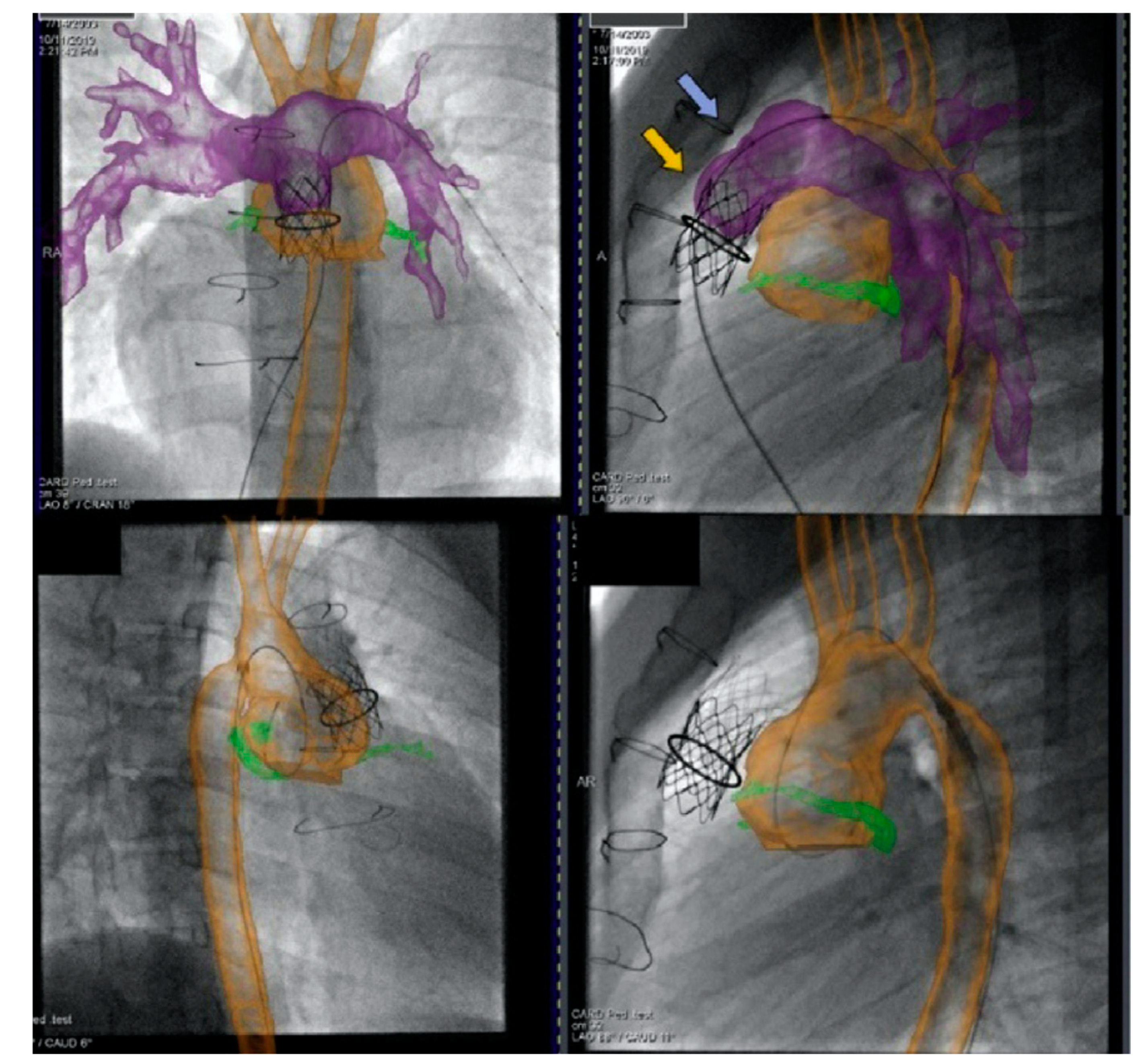
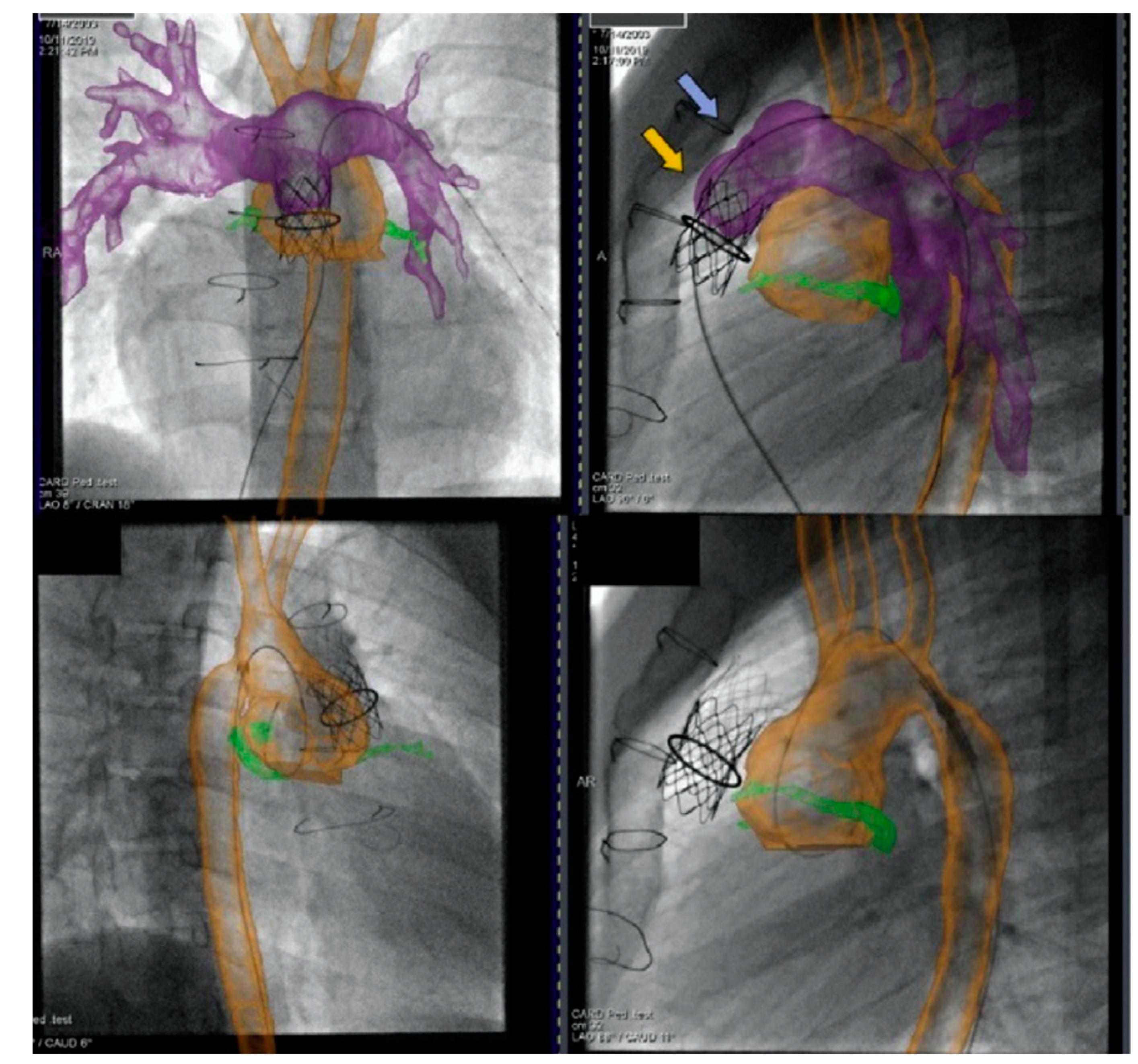
2.4. Cross-Sectional Overlay Fusion in the Catheterization Lab
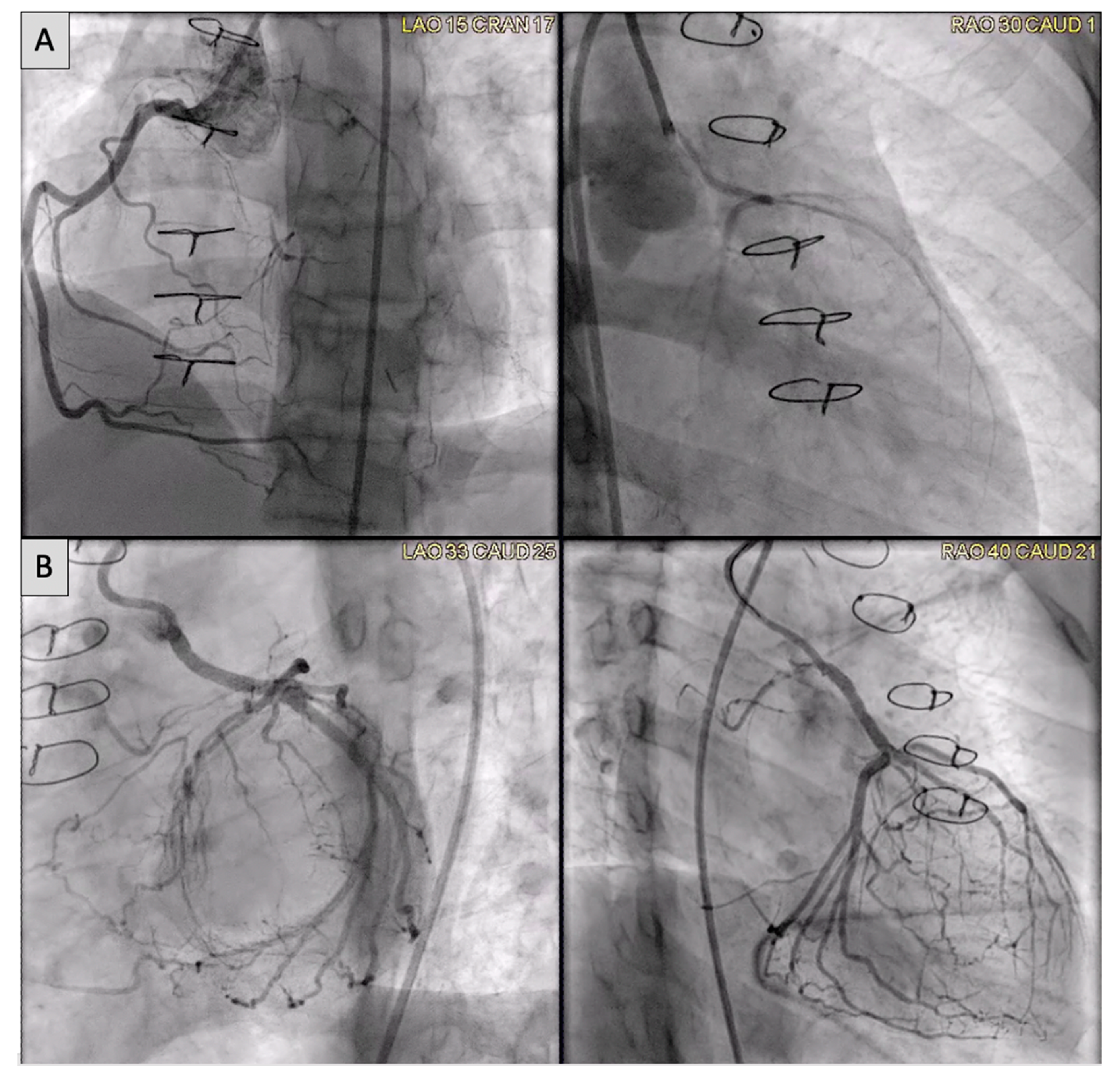
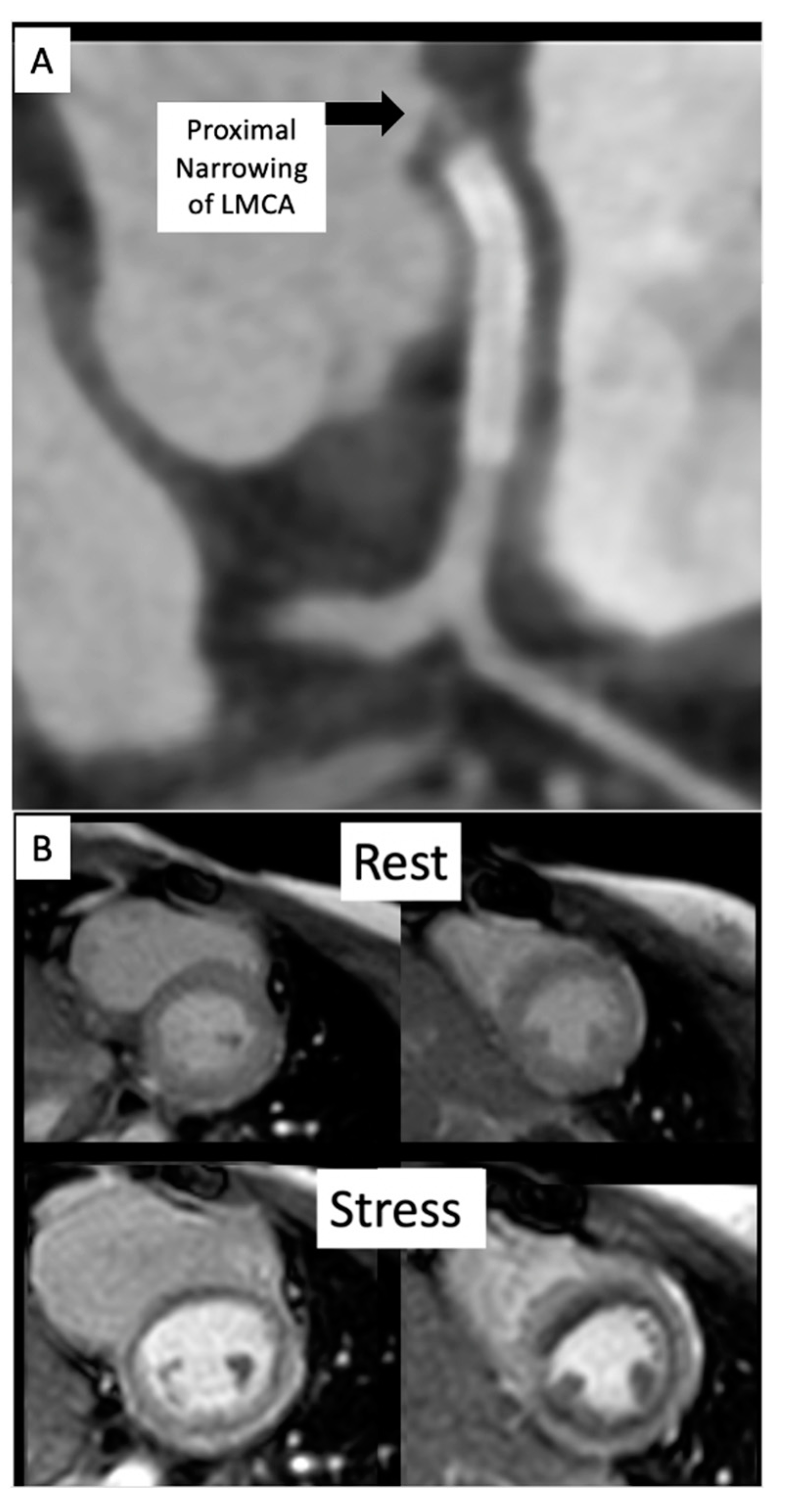
2.5. Coronary Artery Assessment in CHD
References
- Naqvi, N.; McCarthy, K.P.; Ho, S.Y. Anatomy of the atrial septum and interatrial communications. J. Thorac. Dis. 2018, 10, S2837–S2847.
- Li, J.; Al Zaghal, A.M.; Anderson, R.H. The nature of the superior sinus venosus defect. Clin. Anat. 1998, 11, 349–352.
- Van Praagh, S.; Geva, T.; Lock, J.E.; Nido, P.J.; Vance, M.S.; Van Praagh, R. Biatrial or left atrial drainage of the right superior vena cava: Anatomic, morphogenetic, and surgical considerations—Report of three new cases and literature review. Pediatr. Cardiol. 2003, 24, 350–363.
- Hansen, J.H.; Duong, P.; Jivanji, S.G.; Jones, M.; Kabir, S.; Butera, G.; Qureshi, S.A.; Rosenthal, E. Transcatheter Correction of Superior Sinus Venosus Atrial Septal Defects as an Alternative to Surgical Treatment. J. Am. Coll. Cardiol. 2020, 75, 1266–1278.
- Tandon, A.; Burkhardt, B.E.; Batsis, M.; Zellers, T.M.; Forte, M.N.V.; Valverde, I.; McMahan, R.; Guleserian, K.J.; Greil, G.F.; Hussain, T. Sinus Venosus Defects: Anatomic Variants and Transcatheter Closure Feasibility Using Virtual Reality Planning. JACC Cardiovasc. Imaging 2018, 12, 921–924.
- Gibbs, J.L.; Rothman, M.T.; Rees, M.R.; Parsons, J.M.; Blackburn, M.E.; Ruiz, C.E. Stenting of the arterial duct: A new approach to palliation for pulmonary atresia. Heart 1992, 67, 240–245.
- Chamberlain, R.C.; Ezekian, J.E.; Sturgeon, G.M.; Barker, P.C.; Hill, K.D.; Fleming, G.A. Preprocedural three-dimensional planning aids in transcatheter ductal stent placement: A single-center experience. Catheter. Cardiovasc. Interv. 2019, 95, 1141–1148.
- Qureshi, A.M.; Goldstein, B.H.; Glatz, A.C.; Agrawal, H.; Aggarwal, V.; Ligon, R.A.; McCracken, C.; McDonnell, A.; Bs, T.M.B.; Whiteside, W.; et al. Classification scheme for ductal morphology in cyanotic patients with ductal dependent pulmonary blood flow and association with outcomes of patent ductus arteriosus stenting. Catheter. Cardiovasc. Interv. 2018, 93, 933–943.
- Arar, Y.; Dimas, V.V.; Nugent, A.W.; Hussain, T.; Kasraie, N.; Reddy, S.R.V.; Zellers, T.M.; Herbert, C. Pre-procedural CT imaging aids neonatal PDA stenting for ductal-dependent pulmonary blood flow with reduction in overall procedural morbidity. Cardiol. Young 2021, 1–6.
- Goreczny, S.; Dryzek, P.; Morgan, G.J.; Lukaszewski, M.; Moll, J.; Moszura, T. Novel Three-Dimensional Image Fusion Software to Facilitate Guidance of Complex Cardiac Catheterization. Pediatr. Cardiol. 2017, 38, 1133–1142.
- Goreczny, S.; Dryzek, P.; Moszura, T.; Kühne, T.; Berger, F.; Schubert, S. 3Dimage fusion for live guidance of stent implantation in aortic coarctation-mag-netic resonance imaging and computed tomography image overlay enhances interventional technique. Postepy Kardiol. Interwencyjnej 2017, 13, 269–272.
- Arar, Y.; Reddy, S.R.V.; Kim, H.; Dimas, V.V.; Zellers, T.M.; Zahr, R.A.; Vamsee, R.; Greer, J.S.; Tandon, A.; Pontiki, A.; et al. 3D advanced imaging overlay with rapid registration in CHD to reduce radiation and assist cardiac catheterisation interventions. Cardiol. Young 2020, 30, 656–662.
- Vamsee, R.; Reddy, S.; Dimas, V.; Arar, Y.; Pontiki, A.; Hussain, M. Biplane 3D Overlay Guidance for Congenital Heart Disease to Assist Cardiac Catheterization Interventions—A Pilot Study. J. Cardiovasc. Comput. Tomogr. 2021, 15, S13.
- Duran, S.R.; Huffaker, T.; Dixon, B.; Gooty, V.; Zahr, R.A.; Arar, Y.; Greer, J.S.; Butts, R.J.; Hussain, M.T. Feasibility and safety of quantitative adenosine stress perfusion cardiac magnetic resonance imaging in pediatric heart transplant patients with and without coronary allograft vasculopathy. Pediatr. Radiol. 2021, 1–11.
- Gooty, V.D.; Dillenbeck, J.; Arar, Y.; Castellanos, D.A.; Greil, G.F.; Hernandez, N.B.; Kirk, R.; Butts, R.; Hussain, T. Coronary CT Angiography in Pediatric and Young Adult Coronary Allograft Vasculopathy: Single-Center Experience. JACC Cardiovasc. Imaging 2020, 14, 1065–1067.

