Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Masfique Mehedi | + 1603 word(s) | 1603 | 2022-02-14 07:29:05 | | | |
| 2 | Bruce Ren | -10 word(s) | 1593 | 2022-02-21 04:07:03 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Mehedi, M. End-of-Life Care for Patients with Advanced COPD. Encyclopedia. Available online: https://encyclopedia.pub/entry/19667 (accessed on 09 August 2026).
Mehedi M. End-of-Life Care for Patients with Advanced COPD. Encyclopedia. Available at: https://encyclopedia.pub/entry/19667. Accessed August 09, 2026.
Mehedi, Masfique. "End-of-Life Care for Patients with Advanced COPD" Encyclopedia, https://encyclopedia.pub/entry/19667 (accessed August 09, 2026).
Mehedi, M. (2022, February 21). End-of-Life Care for Patients with Advanced COPD. In Encyclopedia. https://encyclopedia.pub/entry/19667
Mehedi, Masfique. "End-of-Life Care for Patients with Advanced COPD." Encyclopedia. Web. 21 February, 2022.
Copy Citation
Exacerbations of chronic obstructive pulmonary disease (COPD) may lead to a rapid decline in health and subsequent death, an unfortunate tyranny of having COPD—an irreversible health condition of 16 million individuals in the USA totaling 60 million in the world. While COPD is the third largest leading cause of death, causing 3.23 million deaths worldwide in 2019 (according to the WHO), most patients with COPD do not receive adequate treatment at the end stages of life. Although death is inevitable, the trajectory towards end-of-life is less predictable in severe COPD. Thus, clinician-patient discussion for end-of-life and palliative care could bring a meaningful life-prospective to patients with advanced COPD.
chronic bronchitis
chronic obstructive pulmonary disease
spirometry
exacerbation
bronchodilators
end-of-life care
palliative care
global initiative for chronic obstructive lung disease
β2-agonists
corticosteroids
dyspnea
emphysema
1. Introduction
Chronic obstructive pulmonary disease (COPD) affects more than 10 million people in the United States [1][2]. COPD is a diseased state in which an individual experiences irreversible airflow limitation and persistent respiratory symptoms. COPD pathophysiology includes emphysema, chronic bronchitis, and other minor airway disorders. COPD is more prevalent among smokers than non-smokers and is more prevalent among men than women [1]. Though men have a higher prevalence than women overall, women are more likely to require hospitalization for severe disease cases due to anatomical and physiological differences [3]. Importantly, the presence of comorbidities impacts COPD patients negatively, increasing the likelihood of hospitalization and mortality and reducing the quality of life [4][5][6].
The current general clinical management of COPD is aimed at treating and preventing acute exacerbation, focusing on the underlying pathophysiology, e.g., treating bronchoconstriction, reducing hyperinflation, and airway inflammation [7]. Unfortunately, advanced COPD is often a progressive and terminal illness [8]. The optimal management of symptoms in patients with advanced COPD is often neglected under the current COPD disease management model. However, the total traditional therapy for advanced COPD produces a modest relief of symptoms, leaving these patients vulnerable and substantially reducing the health-related quality of life [9][10][11]. When needed the most, many patients with advanced COPD receive inadequate end-of-life care, probably due to the lack of patient-physician communication and uncertainty in predicting prognosis for patients with COPD [8].
2. Patients Centered Conversation on End-of-Life Care
The debilitating symptoms of COPD have a significant impact on the lives of patients with COPD and lead to decreased quality of life [12]. These symptoms include breathlessness, cough, pain, anorexia, fatigue, and psychological symptoms [13]. The burden of these symptoms is high and thus patients with advanced COPD symptoms should be informed of the benefits of end-of-life and palliative care. Palliative care not only reduces COPD symptoms leading to increased quality of life, but can also decrease the use of invasive procedures, increase psychosocial support and mood, and decrease health care costs. Many patients may also benefit from the early introduction of palliative care before severe symptoms are present [12]. As each person’s COPD is different, a patient-centered management plan is important. A patient-centered COPD treatment team may include a primary care physician, pulmonologist, respiratory therapist, dietician or nutritionist, therapist or counselor, and palliative care specialist [14][15]. Patients’ family members need to be involved as part of the treatment team for COPD patients, as they can be an extension of the physician’s voice. Family members and caregivers can be very instrumental in monitoring COPD patients’ treatment management plan by making sure the patient takes his or her medications, recognizes signs of exacerbation, and helps them to carry out tasks in the home environment. For patients with advanced COPD, a family member can act on behalf of the patient [16].
However, the lack of an effective end-of-life care strategy for patients with advanced COPD may bring dissatisfaction to the patients and relevant stakeholders associated with the treatment and palliative care. One of the main reasons for dissatisfaction or poor outcome of end-of-life care is the lack of good communication between patients, families, and physicians while planning for the advanced directives [8][17]. Studies show that advanced directives are useful among patients with COPD because of their likely illness, potential risk for severe illness, and sudden death of critically ill patients due to disease exacerbation [18]. In some cases, patients with COPD may have an opinion about the decision to forgo CPR and mechanical ventilation for acute respiratory failure [19]. Several studies have suggested that advanced directives can reduce stress among family members of dying patients [20][21].
Many clinicians acknowledge the importance of end-of-life planning early in the process of COPD, however; for chronic respiratory diseases, such as COPD, advanced care planning is rare [22]. Furthermore, it appears that patients diagnosed with COPD often “underutilize” palliative care when compared to other lung diseases such as lung cancer and thus may have “worse dying experiences” [23]. Patients with advanced COPD are more likely to undergo invasive procedures such as mechanical ventilation and are less likely to receive hospice care and end-of-life planning compared to patients with lung cancer [24]. Thus, delaying access to end-of-life care reduces the ability to increase the quality of life and promote end-of-life discussions [22].
Clinicians play a central role in the quality of care received during the end stages of COPD, but there are major barriers that they face toward providing quality end-of-life care for patients with advanced COPD. These barriers include a lack of continuity of care affecting the relationship of physicians and patients, as well as a lack of education on the roles and goals of palliative care. Most patients would like to receive comprehensive and accurate information about disease progression, treatment options, and prognosis; however, this information is often lacking [12]. Pulmonologists have skills and expertise for overcoming difficulties in COPD diagnosis and for providing the best treatment for managing COPD. Many pulmonology providers have acknowledged misconceptions toward palliative care, including the fear that palliative care clinicians would manage symptoms with high doses of opioids and benzodiazepines. Other barriers include a lack of education regarding when and how to have end-of-life discussions with patients [22]. Poor communication is more likely to lead to poor palliative care in COPD [8]. Despite these barriers, it has been shown that COPD patients benefit from prompt access to palliative care [13]. The goal of palliative care is to prevent and relieve suffering from COPD exacerbation regardless of the stage of the disease [25]. However, the unpredictable nature of disease progression in patients with COPD makes proper planning of end-of-life care difficult. This unpredictability is further complicated during periods of acute exacerbations, where an initial complaint of respiratory discomfort can progress rapidly into respiratory failure. This often puts the patient in an incapacitated state, depriving them of the opportunity to actively participate in the process of end-of-life care planning. For this reason, improving prognostication skills is key, so clinicians may identify COPD patients that are at greater risk for worse outcomes, and promptly commence end-of-life care planning from the initial encounter [26].
Many clinicians find communicating about end-of-life care difficult due to the nature of the discussion, especially with patients in the early stages of COPD. Therefore, adopting the right communication technique is crucial in the overall improvement of end-of-life care (Figure 1) [8]. Patients with COPD more than often want to know information about five specific areas: diagnosis and disease process, treatment, prognosis, what dying might be like, and advance care planning [8]. There are several published studies that provide some specific directions for clinicians in their communications about end-of-life discussion to their patients with advanced COPD. For example, most COPD patients would like more information about prognosis, while patients with advanced COPD and limited life expectancy want to know more about their life expectancy [27][28][29]. It is not unusual that family members request this information even the patient themself does not want to know [30]. Therefore, clinicians should be aware of patients’ and family members’ interests in obtaining information about the disease. It has been found that describing information about a disease with numeric experiences of risk (e.g., eight out of ten people will have side effects from this drug) allowed for better comprehension than describing information about a disease with qualitative expressions of risk [31].
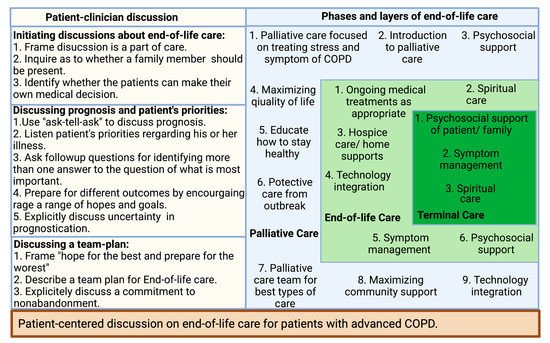
Figure 1. Patient-centered discussion on end-of-life care for patients with advanced COPD.
Patients with COPD may receive poor-quality palliative care due to the lack of patient–physician communication about end-of-life care, or if it occurs too late in the illness [32][33][34]. By understanding the barriers to communication, clinicians can improve patient–clinician discussions about end-of-life care [8]. A recent study suggests that inpatient palliative care consultation has a positive impact on patient outcomes and transitions to the community [35]. A short survey from both pulmonary and palliative clinicians suggested early care adds value to disease-focused COPD care. In the study, the clinicians from both specialties not only supported early palliative care in COPD but also emphasized addressing pulmonologists’ misconception of palliative care, establishing consensus referral criteria, and executing a novel early palliative care model [22]. Clinicians should be prepared to listen and provide appropriate information in the most caring and respectful manner. Practical strategies that can be employed begin with building a relationship based on trust between a COPD patient and their provider. Discussions about end-of-life care must be initiated during the early course of the disease focusing on the implication of the patient’s diagnosis and interventions to be taken at every step of disease progression [36]. A phased introduction of supportive and palliative care can be triggered at key disease milestones during a lifelong journey with COPD, especially during an inpatient visit for an exacerbation [37]. To ensure patients’ wishes regarding end-of-life care are current, the advanced care directive should be reviewed at every visit [36]. Clinician–patient conversations can bring a successful end-of-life care plan with active participation by patients, clinicians, and caregivers (Figure 1) [8].
References
- GOLD 2021. Global Strategy for Prevention, Diagnosis and Management of COPD; In 2021 GOLD Report. 2021, Global Initiative for Chronic Obstructive Lung Disease—GOLD. Available online: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf (accessed on 1 December 2021).
- Silverman, E.K.; Crapo, J.D.; Make, B.J. Chronic obstructive pulmonary disease. In Harrison’s Principles of Internal Medicine; Jameson, J., Fauci, A.S., Kasper, D.L., Hauser, S.L., Longo, D.L., Loscalzo, J., Eds.; McGraw-Hill Education: New York, NY, USA, 2018.
- Barnes, P.J. Sex Differences in Chronic Obstructive Pulmonary Disease Mechanisms. Am. J. Respir. Crit. Care. Med. 2016, 193, 813–814.
- Sin, D.D.; Anthonisen, N.R.; Soriano, J.B.; Agusti, A.G. Mortality in COPD: Role of comorbidities. Eur. Respir. J. 2006, 28, 1245–1257.
- Iglesias, J.R.; Díez-Manglano, J.; García, F.L.; Peromingo, J.A.D.; Almagro, P.; Aguilar, J.M.V. Management of the COPD Patient with Comorbidities: An Experts Recommendation Document. Int. J. Chron. Obs. Pulmon. Dis. 2020, 15, 1015–1037.
- Díez-Manglano, J.; López-García, F. Protocolos: Manejo Diagnóstico y Terapéutico de las Comorbilidades en la EPOC ; Sociedad Española de Medicina Interna (SEMI) y Elsevier SL: Madrid, Spain; Amsterdam, The Netherlands, 2014; pp. 1–259.
- Zhou, H.-X.; Ou, X.-M.; Tang, J.-Y.; Wang, L.; Feng, Y.-L. Advanced Chronic Obstructive Pulmonary Disease: Innovative and Integrated Management Approaches. Chin. Med. J. 2015, 128, 2952–2959.
- Curtis, J.R. Palliative and end-of-life care for patients with severe COPD. Eur. Respir. J. 2008, 32, 796–803.
- Weingaertner, V.; Scheve, C.; Gerdes, V.; Schwarz-Eywill, M.; Prenzel, R.; Bausewein, C.; Higginson, I.J.; Voltz, R.; Herich, L.; Simon, S.T.; et al. Breathlessness, functional status, distress, and palliative care needs over time in patients with advanced chronic obstructive pulmonary disease or lung cancer: A cohort study. J. Pain Symptom Manag. 2014, 48, 569–581.e1.
- Janssen, D.J.; Spruit, M.A.; Uszko-Lencer, N.H.; Schols, J.M.; Wouters, E.F. Symptoms, Comorbidities, and Health Care in Advanced Chronic Obstructive Pulmonary Disease or Chronic Heart Failure. J. Palliat. Med. 2011, 14, 735–743.
- Okutan, O.; Tas, T.; Demirer, E.; Kartalogu, Z. Evaluation of quality of life with the chronic obstructive pulmonary disease assessment test in chronic obstructive pulmonary disease and the effect of dyspnea on disease-specific quality of life in these patients. Yonsei Med. J. 2013, 54, 1214–1219.
- Tavares, N.; Hunt, K.J.; Jarrett, N.; Wilkinson, T.M. The preferences of patients with chronic obstructive pulmonary disease are to discuss palliative care plans with familiar respiratory clinicians, but to delay conversations until their condition deteriorates: A study guided by interpretative phenomenological analysis. Palliat. Med. 2020, 34, 1361–1373.
- Smallwood, N.; Currow, D.; Booth, S.; Spathis, A.; Irving, L.; Philip, J. Attitudes to specialist palliative care and advance care planning in people with COPD: A multi-national survey of palliative and respiratory medicine specialists. BMC Palliat. Care 2018, 17, 115.
- Kuzma, A.M.; Meli, Y.; Meldrum, C.; Jellen, P.; Butler-Lebair, M.; Koczen-Doyle, D.; Rising, P.; Stavrolakes, K.; Brogan., F. Multidisciplinary care of the patient with chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2008, 5, 567–571.
- Team of Specialists. National Jewish Health. Available online: https://www.nationaljewish.org/directory/copd/team (accessed on 2 December 2021).
- Family Members Share in the Care of COPD Patients. Available online: https://www.medicaleconomics.com/view/family-members-share-care-copd-patients. (accessed on 2 December 2021).
- Tonelli, M.R. Pulling the plug on living wills. A critical analysis of advance directives. Chest 1996, 110, 816–822.
- Murray, S.A.; Kendall, M.; Boyd, K.; Sheikh, A. Illness trajectories and palliative care. BMJ 2005, 330, 1007–1011.
- Dales, R.E.; O’Connor, A.; Hebert, P.; Sullivan, K.; Mc Kim, D.; Llewellyn-Thomas, H. Intubation and mechanical ventilation for COPD: Development of an instrument to elicit patient preferences. Chest 1999, 116, 792–800.
- Tilden, V.P.; Tolle, S.W.; Drach, L.L.; Perrin, N.A. Out-of-hospital death: Advance care planning, decedent symptoms, and caregiver burden. J. Am. Geriatr. Soc. 2004, 52, 532–539.
- Norris, K.; Merriman, M.P.; Curtis, J.R.; Asp, C.; Tuholske, L.; Byock, I.R. Next of kin perspectives on the experience of end-of-life care in a community setting. J. Palliat. Med. 2007, 10, 1101–1115.
- Iyer, A.S.; Dionne-Odom, J.N.; Khateeb, D.M.; O’Hare, L.; Tucker, R.O.; Brown, C.J.; Dransfield, M.T.; Bakitas, M.A. A Qualitative Study of Pulmonary and Palliative Care Clinician Perspectives on Early Palliative Care in Chronic Obstructive Pulmonary Disease. J. Palliat. Med. 2020, 23, 513–526.
- Kendzerska, T.; Nickerson, J.W.; Hsu, A.T.; Gershon, A.S.; Talarico, R.; Mulpuru, S.; Pakhale, S.; Tanuseputro, P. End-of-life care in individuals with respiratory diseases: A population study comparing the dying experience between those with chronic obstructive pulmonary disease and lung cancer. Int. J. Chron. Obs. Pulmon. Dis. 2019, 14, 1691–1701.
- Fu, P.K.; Yang, M.C.; Wang, C.Y.; Lin, S.P.; Kuo, C.T.; Hsu, C.Y.; Tung, Y.C. Early Do-Not-Resuscitate Directives Decrease Invasive Procedures and Health Care Expenses During the Final Hospitalization of Life of COPD Patients. J. Pain Symptom Manag. 2019, 58, 968–976.
- American Academy of Hospice and Palliative Medicine; Center to Advance Palliative Care; Hospice and Palliative Nurses Association, Last Acts Partnership; National Hospice and Palliative Care Organization. National consensus project for quality palliative care: Clinical practice guidelines for quality palliative care, executive summary. J. Palliat. Med. 2004, 7, 611–627.
- Spathis, A.; Booth, S. End of life care in chronic obstructive pulmonary disease: In search of a good death. Int. J. Chron. Obs. Pulmon. Dis. 2008, 3, 11–29.
- Curtis, J.R.; Wenrich, M.D.; Carline, J.D.; Shannon, S.E.; Ambrozy, D.M.; Ramsey, P.G. Patients’ perspectives on physician skill in end-of-life care: Differences between patients with COPD, cancer, and AIDS. Chest 2002, 122, 356–362.
- Jones, I.; Kirby, A.; Ormiston, P.; Loomba, Y.; Chan, K.K.; Rout, J.; Nagle, J.; Wardman, L.; Hamilton, S. The needs of patients dying of chronic obstructive pulmonary disease in the community. Fam. Pr. 2004, 21, 310–313.
- Fried, T.R.; Bradley, E.H.; O’Leary, J. Prognosis communication in serious illness: Perceptions of older patients, caregivers, and clinicians. J. Am. Geriatr. Soc. 2003, 51, 1398–1403.
- Curtis, J.R.; Engelberg, R.; Young, J.P.; Vig, L.K.; Reinke, L.F.; Wenrich, M.D.; McGrath, B.; McCown, E.; Back, A.L. An approach to understanding the interaction of hope and desire for explicit prognostic information among individuals with severe chronic obstructive pulmonary disease or advanced cancer. J. Palliat. Med. 2008, 11, 610–620.
- Paling, J. Strategies to help patients understand risks. BMJ 2003, 327, 745–748.
- Curtis, J.; Engelberg, R.; Nielsen, E.; Au, D.; Patrick, D. Patient-physician communication about end-of-life care for patients with severe COPD. Eur. Respir. J. 2004, 24, 200–205.
- Heffner, J.E.; Fahy, B.; Hilling, L.; Barbieri, C. Outcomes of advance directive education of pulmonary rehabilitation patients. Am. J. Respir. Crit. Care Med. 1997, 155, 1055–1059.
- Heffner, J.E.; Fahy, B.; Hilling, L.; Barbieri, C. Attitudes regarding advance directives among patients in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 1996, 154, 1735–1740.
- Scott, M.; Shaver, N.; Lapenskie, J.; Isenberg, S.R.; Saunders, S.; Hsu, A.T.; Tanuseputro, P. Does inpatient palliative care consultation impact outcomes following hospital discharge? A narrative systematic review. Palliat. Med. 2020, 34, 5–15.
- Halpin, D.M.G.; Dionne-Odom, J.N.; Khateeb, D.M.; O’Hare, L.; Tucker, R.O.; Brown, C.J.; Dransfield, M.T.; Bakitas, M.A. Palliative care for people with COPD: Effective but underused. Eur. Respir. J. 2018, 51, 1702645.
- Pinnock, H.; Kendall, M.; Murray, S.A.; Worth, A.; Levack, P.; Porter, M.; MacNee, W.; Sheikh, A. Living and dying with severe chronic obstructive pulmonary disease: Multi-perspective longitudinal qualitative study. BMJ 2011, 342, D142.
More
Information
Contributor
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
845
Revisions:
2 times
(View History)
Update Date:
21 Feb 2022
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No