 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Eloïse COLLIOU | + 2822 word(s) | 2822 | 2021-09-08 05:05:26 | | | |
| 2 | Peter Tang | Meta information modification | 2822 | 2021-09-22 10:09:14 | | |
Video Upload Options
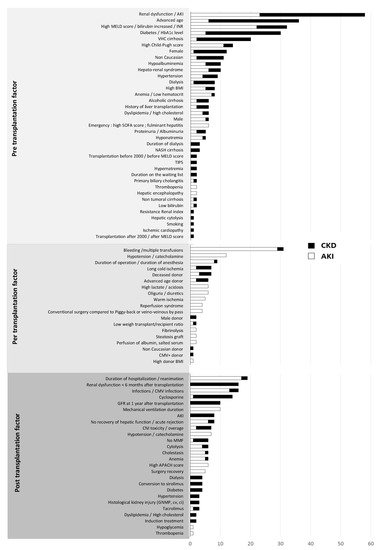
One-third of patients with cirrhosis present kidney failure (AKI and CKD). It has multifactorial causes and a harmful effect on morbidity and mortality before and after liver transplantation. Kidney function does not improve in all patients after liver transplantation, and liver transplant recipients are at a high risk of developing chronic kidney disease. The causes of renal dysfunction can be divided into three groups: pre-operative, perioperative and post-operative factors.
1. Kidney Function and Cirrhosis
2. Change in Kidney Function Post-Transplantation
2.1. Acute Kidney Injury after Liver Transplantation
2.2. Post-Transplantation Chronic Kidney Disease and End-Stage Renal Disease
2.3. The Contribution of Histology in Post-Transplantation Kidney Failure
2.4. The Impact of Kidney Function on Post-Transplantation Mortality
3. Factors Associated with the Risk of Post-Transplantation Renal Dysfunction
4. Markers and Predictive Models of Post-Transplantation Renal Dysfunction
4.1. Markers of Post-Transplantation Renal Dysfunction
4.2. Long-Term CKD Prediction Models
5. Prevention of Post-Liver Transplantation Kidney Failure
5.1. Pre-Transplantation Prevention
5.2. Post-Transplantation Prevention
5.2.1. Control of Cardiovascular Risk Factors
5.2.2. Optimization of Immunosuppressive Treatment
6. The Indication for Liver–Kidney Transplantation
|
Indications for a Combined Liver–Kidney Transplantation |
|---|
|
Patients with AKI associated with:
|
|
Patients with CKD (eGFR < 60 mL/min for at least 3 months) associated with:
|
AKI: acute kidney injury; GFR: glomerular filtration rate; MDRD: modification of diet in renal disease; CKD: chronic kidney disease; HUS: hemolytic uremic syndrome.
References
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver cirrhosis. Lancet 2014, 383, 1749–1761.
- Wong, F.; Reddy, K.R.; O’Leary, J.G.; Tandon, P.; Biggins, S.W.; Garcia-Tsao, G.; Maliakkal, B.J.; Lai, J.C.; Fallon, M.B.; Vargas, H.E.; et al. Impact of chronic kidney disease on outcomes in cirrhosis. Liver Transpl. 2019, 25, 870–880.
- Wong, F. Acute kidney injury in liver cirrhosis: New definition and application. Clin. Mol. Hepatol. 2016, 22, 415–422.
- Cullaro, G.; Verna, E.C.; Lai, J.C. Association between renal function pattern and mortality in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2019, 17, 2364–2370.
- Tanriover, B.; Mejia, A.; Weinstein, J.; Foster, S.V.; Ghalib, R.; Mubarak, A.; Cheng, S.S. Analysis of kidney function and biopsy results in liver failure patients with renal dysfunction: A new look to combined liver kidney allocation in the post-MELD era. Transplantation 2008, 86, 1548–1553.
- Calmus, Y.; Conti, F.; Cluzel, P.; Hill, G.; Antoine, C.; Scatton, O.; Soubrane, O.; Glotz, D.; Pillebout, E.; Nochy, D. Prospective assessment of renal histopathological lesions in patients with end-stage liver disease: Effects on long-term renal function after liver transplantation. J. Hepatol. 2012, 57, 572–576.
- Ginès, P.; Solà, E.; Angeli, P.; Wong, F.; Nadim, M.K.; Kamath, P.S. Hepatorenal syndrome. Nat. Rev. Dis. Primers 2018, 4, 23.
- Nishi, H.; Shibagaki, Y.; Kido, R.; Tamura, S.; Nangaku, M.; Sugawara, Y.; Fujita, T. Chronic renal outcome after living donor liver transplantation. Clin. Transpl. 2013, 27, 90–97.
- Karapanagiotou, A.; Dimitriadis, C.; Papadopoulos, S.; Kydona, C.; Kefsenidis, S.; Papanikolaou, V.; Gritsi-Gerogianni, N. Comparison of RIFLE and AKIN criteria in the evaluation of the frequency of acute kidney injury in post-liver transplantation patients. Transpl. Proc. 2014, 46, 3222–3227.
- Wong, F.; Nadim, M.K.; Kellum, J.A.; Salerno, F.; Bellomo, R.; Gerbes, A.; Angeli, P.; Moreau, R.; Davenport, A.; Jalan, R.; et al. Working Party proposal for a revised classification system of renal dysfunction in patients with cirrhosis. Gut 2011, 60, 702–709.
- Mendizabal, M.; Reddy, K.R. Chronic hepatitis C and chronic kidney disease: Advances, limitations and unchartered territories. J. Viral Hepat. 2017, 24, 442–453.
- Biagioni, E.; Cavazzuti, I.; Busani, S.; Trevisan, D.; Zavatti, L.; Ferrari, E.; Girardis, M.; Massimo, G. Acute renal failure and renal replacement therapy in the postoperative period of orthotopic liver transplant patients versus nonelective abdominal surgery patients. Transpl. Proc. 2011, 43, 1145–1147.
- Cabezuelo, J.B.; Ramírez, P.; Ríos, A.; Acosta, F.; Torres, D.; Sansano, T.; Pons, J.A.; Bru, M.; Montoya, M.; Bueno, F.S.; et al. Risk factors of acute renal failure after liver transplantation. Kidney Int. 2006, 69, 1073–1080.
- Chen, J.; Singhapricha, T.; Hu, K.-Q.; Hong, J.C.; Steadman, R.H.; Busuttil, R.W.; Xia, V.W. Postliver transplant acute renal injury and failure by the RIFLE criteria in patients with normal pretransplant serum creatinine concentrations: A matched study. Transplantation 2011, 91, 348–353.
- Ferreira, A.C.; Nolasco, F.; Carvalho, D.; Sampaio, S.; Baptista, A.; Pessegueiro, P.; Monteiro, E.; Mourão, L.; Barroso, E. Impact of RIFLE classification in liver transplantation. Clin. Transpl. 2010, 24, 394–400.
- Hong, S.H.; Park, C.O.; Park, C.S. Prediction of newly developed acute renal failure using serum phosphorus concentrations after living-donor liver transplantation. J. Int. Med. Res. 2012, 40, 2199–2212.
- Jeong, T.-D.; Kim, S.; Lee, W.; Song, G.-W.; Kim, Y.-K.; Chun, S.; Lee, S.-G.; Min, W.-K. Neutrophil gelatinase-associated lipocalin as an early biomarker of acute kidney injury in liver transplantation. Clin. Transpl. 2012, 26, 775–781.
- Klaus, F.; Keitel da Silva, C.; Meinerz, G.; Carvalho, L.M.; Goldani, J.C.; Cantisani, G.; Zanotelli, M.L.; Duro Garcia, V.; Keitel, E. Acute kidney injury after liver transplantation: Incidence and mortality. Transpl. Proc. 2014, 46, 1819–1821.
- Kundakci, A.; Pirat, A.; Komurcu, O.; Torgay, A.; Karakayalı, H.; Arslan, G.; Haberal, M. Rifle criteria for acute kidney dysfunction following liver transplantation: Incidence and risk factors. Transpl. Proc. 2010, 42, 4171–4174.
- Leithead, J.A.; Ferguson, J.W.; Hayes, P.C. Modifiable patient factors are associated with the late decline in renal function following liver transplantation. Clin. Transpl. 2012, 26, E316–E323.
- Leithead, J.A.; Rajoriya, N.; Gunson, B.K.; Muiesan, P.; Ferguson, J.W. The evolving use of higher risk grafts is associated with an increased incidence of acute kidney injury after liver transplantation. J. Hepatol. 2014, 60, 1180–1186.
- Aksu Erdost, H.; Ozkardesler, S.; Ocmen, E.; Avkan-Oguz, V.; Akan, M.; Iyilikci, L.; Unek, T.; Ozbilgin, M.; Meseri Dalak, R.; Astarcioglu, I. Acute renal injury evaluation after liver transplantation: With RIFLE criteria. Transpl. Proc. 2015, 47, 1482–1487.
- Karapanagiotou, A.; Kydona, C.; Dimitriadis, C.; Sgourou, K.; Giasnetsova, T.; Fouzas, I.; Imvrios, G.; Gritsi-Gerogianni, N. Acute kidney injury after orthotopic liver transplantation. Transpl. Proc. 2012, 44, 2727–2729.
- Lin, Y.-H.; Lin, C.-C.; Wang, C.-C.; Wang, S.-H.; Liu, Y.-W.; Yong, C.-C.; Lin, T.-L.; Li, W.-F.; Concejero, A.M.; Chen, C.-L. The 4-week serum creatinine level predicts long-term renal dysfunction after adult living donor liver transplantation. Transpl. Proc. 2012, 44, 772–775.
- Nadeem, A.; Salahuddin, N.; El Hazmi, A.; Joseph, M.; Bohlega, B.; Sallam, H.; Sheikh, Y.; Broering, D. Chloride-liberal fluids are associated with acute kidney injury after liver transplantation. Crit. Care 2014, 18, 625.
- Nadim, M.K.; Genyk, Y.S.; Tokin, C.; Fieber, J.; Ananthapanyasut, W.; Ye, W.; Selby, R. Impact of the etiology of acute kidney injury on outcomes following liver transplantation: Acute tubular necrosis versus hepatorenal syndrome. Liver Transpl. 2012, 18, 539–548.
- Niemann, C.U.; Walia, A.; Waldman, J.; Davio, M.; Roberts, J.P.; Hirose, R.; Feiner, J. Acute kidney injury during liver transplantation as determined by neutrophil gelatinase-associated lipocalin. Liver Transpl. 2009, 15, 1852–1860.
- O’Riordan, A.; Wong, V.; McQuillan, R.; McCormick, P.A.; Hegarty, J.E.; Watson, A.J. Acute renal disease, as defined by the RIFLE criteria, post-liver transplantation. Am. J. Transpl. 2007, 7, 168–176.
- Sirivatanauksorn, Y.; Parakonthun, T.; Premasathian, N.; Limsrichamrern, S.; Mahawithitwong, P.; Kositamongkol, P.; Tovikkai, C.; Asavakarn, S. Renal dysfunction after orthotopic liver transplantation. Transpl. Proc. 2014, 46, 818–821.
- Tinti, F.; Umbro, I.; Meçule, A.; Rossi, M.; Merli, M.; Nofroni, I.; Corradini, S.G.; Poli, L.; Pugliese, F.; Ruberto, F.; et al. RIFLE criteria and hepatic function in the assessment of acute renal failure in liver transplantation. Transpl. Proc. 2010, 42, 1233–1236.
- Umbro, I.; Tinti, F.; Piselli, P.; Fiacco, F.; Giannelli, V.; Di Natale, V.; Zavatto, A.; Merli, M.; Rossi, M.; Ginanni Corradini, S.; et al. Occurrence of chronic renal failure in liver transplantation: Monitoring of pre- and posttransplantation renal function. Transpl. Proc. 2012, 44, 1956–1959.
- Utsumi, M.; Umeda, Y.; Sadamori, H.; Nagasaka, T.; Takaki, A.; Matsuda, H.; Shinoura, S.; Yoshida, R.; Nobuoka, D.; Satoh, D.; et al. Risk factors for acute renal injury in living donor liver transplantation: Evaluation of the RIFLE criteria. Transpl. Int. 2013, 26, 842–852.
- Wagener, G.; Minhaz, M.; Mattis, F.A.; Kim, M.; Emond, J.C.; Lee, H.T. Urinary neutrophil gelatinase-associated lipocalin as a marker of acute kidney injury after orthotopic liver transplantation. Nephrol. Dial. Transpl. 2011, 26, 1717–1723.
- Iglesias, J.I.; DePalma, J.A.; Levine, J.S. Risk factors for acute kidney injury following orthotopic liver transplantation: The impact of changes in renal function while patients await transplantation. BMC Nephrol. 2010, 11, 30.
- Sung, W.-C.; Yu, H.-P.; Tsai, Y.-F.; Chung, P.C.-H.; Lin, C.-C.; Lee, W.-C. The ratio of plasma interleukin-18 is a sensitive biomarker for acute kidney injury after liver transplantation. Transpl. Proc. 2014, 46, 816–817.
- Zhu, M.; Li, Y.; Xia, Q.; Wang, S.; Qiu, Y.; Che, M.; Dai, H.; Qian, J.; Ni, Z.; Axelsson, J.; et al. Strong impact of acute kidney injury on survival after liver transplantation. Transpl. Proc. 2010, 42, 3634–3638.
- Alvares-da-Silva, M.R.; Waechter, F.L.; Francisconi, C.F.; Barros, E.; Thomé, F.; Traiber, C.; Fonseca, D.L.; Zingani, J.M.; Sampaio, J.A.; Pinto, R.D.; et al. Risk factors for postoperative acute renal failure at a new orthotopic liver transplantation program. Transpl. Proc. 1999, 31, 3050–3052.
- Barri, Y.M.; Sanchez, E.Q.; Jennings, L.W.; Melton, L.B.; Hays, S.; Levy, M.F.; Klintmalm, G.B. Acute kidney injury following liver transplantation: Definition and outcome. Liver Transpl. 2009, 15, 475–483.
- Bilbao, I.; Salcedo, M.; Gómez, M.A.; Jimenez, C.; Castroagudín, J.; Fabregat, J.; Almohalla, C.; Herrero, I.; Cuervas-Mons, V.; Otero, A.; et al. Renal function improvement in liver transplant recipients after early everolimus conversion: A clinical practice cohort study in Spain. Liver Transpl. 2015, 21, 1056–1065.
- Cabezuelo, J.B.; Ramirez, P.; Acosta, F.; Sanchez Bueno, F.; Robles, R.; Pons, J.A.; Miras, M.; Munitiz, V.; Fernandez, J.A.; Lujan, J.; et al. Prognostic factors of early acute renal failure in liver transplantation. Transpl. Proc. 2002, 34, 254–255.
- Faenza, S.; Bernardi, E.; Cimatti, M.; Dante, A.; Mancini, E.; Miklosova, Z.; Piraccini, E.; Pierucci, E.; Riganello, I.; Spedicato, S.; et al. Acute renal failure after liver transplantation in MELD era. Transpl. Proc. 2007, 39, 1945–1946.
- Kim, J.M.; Jo, Y.Y.; Na, S.W.; Kim, S.I.; Choi, Y.S.; Kim, N.O.; Park, J.E.; Koh, S.O. The predictors for continuous renal replacement therapy in liver transplant recipients. Transpl. Proc. 2014, 46, 184–191.
- Koo, M.; Sabaté, A.; Ramos, E.; Dalmau, A.; León, E.; Fabregat, J.; Rafecas, A. Factors related to renal dysfunction after liver transplantation in patients with normal preoperative function. Rev. Esp. Anestesiol. Reanim. 2006, 53, 538–544.
- Lafayette, R.A.; Paré, G.; Schmid, C.H.; King, A.J.; Rohrer, R.J.; Nasraway, S.A. Pretransplant renal dysfunction predicts poorer outcome in liver transplantation. Clin. Nephrol. 1997, 48, 159–164.
- Lima, E.Q.; Zanetta, D.M.T.; Castro, I.; Massarollo, P.C.B.; Mies, S.; Machado, M.M.; Yu, L. Risk factors for development of acute renal failure after liver transplantation. Ren. Fail. 2003, 25, 553–560.
- Paramesh, A.S.; Roayaie, S.; Doan, Y.; Schwartz, M.E.; Emre, S.; Fishbein, T.; Florman, S.; Gondolesi, G.E.; Krieger, N.; Ames, S.; et al. Post-liver transplant acute renal failure: Factors predicting development of end-stage renal disease. Clin. Transpl. 2004, 18, 94–99.
- Rimola, A.; Gavaler, J.S.; Schade, R.R.; el-Lankany, S.; Starzl, T.E.; Van Thiel, D.H. Effects of renal impairment on liver transplantation. Gastroenterology 1987, 93, 148–156.
- Rueggeberg, A.; Boehm, S.; Napieralski, F.; Mueller, A.R.; Neuhaus, P.; Falke, K.J.; Gerlach, H. Development of a risk stratification model for predicting acute renal failure in orthotopic liver transplantation recipients. Anaesthesia 2008, 63, 1174–1180.
- McCauley, J.; Van Thiel, D.H.; Starzl, T.E.; Puschett, J.B. Acute and chronic renal failure in liver transplantation. Nephron 1990, 55, 121–128.
- Chuang, F.-R.; Lin, C.-C.; Wang, P.-H.; Cheng, Y.-F.; Hsu, K.-T.; Chen, Y.-S.; Lee, C.-H.; Chen, C.-L. Acute renal failure after cadaveric related liver transplantation. Transpl. Proc. 2004, 36, 2328–2330.
- Contreras, G.; Garces, G.; Quartin, A.A.; Cely, C.; LaGatta, M.A.; Barreto, G.A.; Roth, D.; Gomez, E. An epidemiologic study of early renal replacement therapy after orthotopic liver transplantation. J. Am. Soc. Nephrol. 2002, 13, 228–233.
- Fraley, D.S.; Burr, R.; Bernardini, J.; Angus, D.; Kramer, D.J.; Johnson, J.P. Impact of acute renal failure on mortality in end-stage liver disease with or without transplantation. Kidney Int. 1998, 54, 518–524.
- Brescia, M.D.G.; Massarollo, P.C.B.; Imakuma, E.S.; Mies, S. Prospective randomized trial comparing hepatic venous outflow and renal function after conventional versus piggyback liver transplantation. PLoS ONE 2015, 10, e0129923.
- Faenza, S.; Santoro, A.; Mancini, E.; Pareschi, S.; Siniscalchi, A.; Zanzani, C.; Pinna, A.D. Acute renal failure requiring renal replacement therapy after orthotopic liver transplantation. Transpl. Proc. 2006, 38, 1141–1142.
- Gainza, F.J.; Valdivieso, A.; Quintanilla, N.; Errazti, G.; Gastaca, M.; Campo, M.; Lampreabe, I.; Ortiz-de-Urbina, J. Evaluation of acute renal failure in the liver transplantation perioperative period: Incidence and impact. Transpl. Proc. 2002, 34, 250–251.
- Hilmi, I.A.; Damian, D.; Al-Khafaji, A.; Sakai, T.; Donaldson, J.; Winger, D.G.; Kellum, J.A. Acute kidney injury after orthotopic liver transplantation using living donor versus deceased donor grafts: A propensity score-matched analysis. Liver Transpl. 2015, 21, 1179–1185.
- Junge, G.; Schewior, L.V.; Kohler, S.; Neuhaus, R.; Langrehr, J.M.; Tullius, S.; Kahl, A.; Frei, U.; Neuhaus, P. Acute renal failure after liver transplantation: Incidence, etiology, therapy, and outcome. Transpl. Proc. 2006, 38, 723–724.
- Paydas, S.; Balal, M.; Demiryurek, H.; Kose, F. Renal function in patients with orthotopic liver transplantation. Ren. Fail. 2006, 28, 103–105.
- Platz, K.P.; Mueller, A.R.; Blumhardt, G.; Bachmann, S.; Bechstein, W.O.; Kahl, A.; Neuhaus, P. Nephrotoxicity after orthotopic liver transplantation in cyclosporin A and FK 506-treated patients. Transpl. Int. 1994, 7 (Suppl. S1), S52–S57.
- Portal, A.J.; McPhail, M.J.W.; Bruce, M.; Coltart, I.; Slack, A.; Sherwood, R.; Heaton, N.D.; Shawcross, D.; Wendon, J.A.; Heneghan, M.A. Neutrophil gelatinase—Associated lipocalin predicts acute kidney injury in patients undergoing liver transplantation. Liver Transpl. 2010, 16, 1257–1266.
- Sanchez, E.Q.; Gonwa, T.A.; Levy, M.F.; Goldstein, R.M.; Mai, M.L.; Hays, S.R.; Melton, L.B.; Saracino, G.; Klintmalm, G.B. Preoperative and perioperative predictors of the need for renal replacement therapy after orthotopic liver transplantation. Transplantation 2004, 78, 1048–1054.
- Velidedeoglu, E.; Bloom, R.D.; Crawford, M.D.; Desai, N.M.; Campos, L.; Abt, P.L.; Markmann, J.W.; Mange, K.C.; Olthoff, K.M.; Shaked, A.; et al. Early kidney dysfunction post liver transplantation predicts late chronic kidney disease. Transplantation 2004, 77, 553–556.
- Wei, Y.; Zhang, L.; Lin, H.; Li, J.; Li, B.; Yan, L.; Wen, T.; Zeng, Y.; Lu, S. Factors related to post-liver transplantation acute renal failure. Transpl. Proc. 2006, 38, 2982–2984.
- Xu, X.; Ling, Q.; Wei, Q.; Wu, J.; Gao, F.; He, Z.-L.; Zhou, L.; Zheng, S.-S. An effective model for predicting acute kidney injury after liver transplantation. Hepatobiliary Pancreat Dis. Int. 2010, 9, 259–263.
- Jindal, R.M.; Popescu, I. Renal dysfunction associated with liver transplantation. Postgrad. Med. J. 1995, 71, 513–524.
- Guitard, J.; Ribes, D.; Kamar, N.; Muscari, F.; Cointault, O.; Lavayssière, L.; Suc, B.; Esposito, L.; Peron, J.-M.; Rostaing, L. Predictive factors for chronic renal failure one year after orthotopic liver transplantation. Ren. Fail. 2006, 28, 419–425.
- Thongprayoon, C.; Kaewput, W.; Thamcharoen, N.; Bathini, T.; Watthanasuntorn, K.; Lertjitbanjong, P.; Sharma, K.; Salim, S.A.; Ungprasert, P.; Wijarnpreecha, K.; et al. Incidence and impact of acute kidney injury after liver transplantation: A meta-analysis. J. Clin. Med. 2019, 8, 372.
- Umbro, I.; Tinti, F.; Scalera, I.; Evison, F.; Gunson, B.; Sharif, A.; Ferguson, J.; Muiesan, P.; Mitterhofer, A.P. Acute kidney injury and post-reperfusion syndrome in liver transplantation. World J. Gastroenterol. 2016, 22, 9314–9323.
- Formica, R.N.; Aeder, M.; Boyle, G.; Kucheryavaya, A.; Stewart, D.; Hirose, R.; Mulligan, D. Simultaneous liver-kidney allocation policy: A proposal to optimize appropriate utilization of scarce resources. Am. J. Transpl. 2016, 16, 758–766.
- Ojo, A.O.; Held, P.J.; Port, F.K.; Wolfe, R.A.; Leichtman, A.B.; Young, E.W.; Arndorfer, J.; Christensen, L.; Merion, R.M. Chronic renal failure after transplantation of a nonrenal organ. N. Engl. J. Med. 2003, 349, 931–940.
- Herlenius, G.; Fistouris, J.; Olausson, M.; Felldin, M.; Bäckman, L.; Friman, S. Early renal function post-liver transplantation is predictive of progressive chronic kidney disease. Scand. J. Gastroenterol. 2008, 43, 344–349.
- Allen, A.M.; Kim, W.R.; Therneau, T.M.; Larson, J.J.; Heimbach, J.K.; Rule, A.D. Chronic kidney disease and associated mortality after liver transplantation—A time-dependent analysis using measured glomerular filtration rate. J. Hepatol. 2014, 61, 286–292.
- Fussner, L.A.; Charlton, M.R.; Heimbach, J.K.; Fan, C.; Dierkhising, R.; Coss, E.; Watt, K.D. The impact of gender and NASH on chronic kidney disease before and after liver transplantation. Liver Int. 2014, 34, 1259–1266.
- Aggarwal, S.; Kang, Y.; Freeman, J.A.; Fortunato, F.L.; Pinsky, M.R. Postreperfusion syndrome: Hypotension after reperfusion of the transplanted liver. J. Crit. Care 1993, 8, 154–160.
- Burra, P.; Senzolo, M.; Masier, A.; Prestele, H.; Jones, R.; Samuel, D.; Villamil, F. Factors influencing renal function after liver transplantation. Results from the MOST, an international observational study. Dig. Liver Dis. 2009, 41, 350–356.
- Fisher, N.C.; Nightingale, P.G.; Gunson, B.K.; Lipkin, G.W.; Neuberger, J.M. Chronic renal failure following liver transplantation: A retrospective analysis. Transplantation 1998, 66, 59–66.
- Gayowski, T.; Wagener, M.M.; Marino, I.R.; Singh, N. Quality of life and functional status of liver transplant recipients with recurrent viral hepatitis C. Transpl. Proc. 1999, 31, 1386–1387.
- Giusto, M.; Berenguer, M.; Merkel, C.; Aguilera, V.; Rubin, A.; Ginanni Corradini, S.; Mennini, G.; Rossi, M.; Prieto, M.; Merli, M. Chronic kidney disease after liver transplantation: Pretransplantation risk factors and predictors during follow-up. Transplantation 2013, 95, 1148–1153.
- Gonwa, T.A.; Mai, M.L.; Melton, L.B.; Hays, S.R.; Goldstein, R.M.; Levy, M.F.; Klintmalm, G.B. End-stage renal disease (ESRD) after orthotopic liver transplantation (OLTX) using calcineurin-based immunotherapy: Risk of development and treatment. Transplantation 2001, 72, 1934–1939.
- Kamar, N.; Guilbeau-Frugier, C.; Servais, A.; Tack, I.; Thervet, E.; Cointault, O.; Esposito, L.; Guitard, J.; Lavayssière, L.; Muscari, F.; et al. Kidney histology and function in liver transplant patients. Nephrol. Dial. Transpl. 2011, 26, 2355–2361.
- Karie-Guigues, S.; Janus, N.; Saliba, F.; Dumortier, J.; Duvoux, C.; Calmus, Y.; Lorho, R.; Deray, G.; Launay-Vacher, V.; Pageaux, G.-P. Long-term renal function in liver transplant recipients and impact of immunosuppressive regimens (calcineurin inhibitors alone or in combination with mycophenolate mofetil): The TRY study. Liver Transpl. 2009, 15, 1083–1091.
- Lamattina, J.C.; Foley, D.P.; Mezrich, J.D.; Fernandez, L.A.; Vidyasagar, V.; D’Alessandro, A.M.; Musat, A.I.; Samaniego-Picota, M.D.; Pascual, J.; Alejandro, M.D.R.; et al. Chronic kidney disease stage progression in liver transplant recipients. Clin. J. Am. Soc. Nephrol. 2011, 6, 1851–1857.
- LaMattina, J.C.; Mezrich, J.D.; Fernandez, L.A.; D’Alessandro, A.M.; Djamali, A.; Musat, A.I.; Pirsch, J.D.; Foley, D.P. Native kidney function following liver transplantation using calcineurin inhibitors: Single-center analysis with 20 years of follow-up. Clin. Transpl. 2013, 27, 193–202.
- Lee, J.P.; Heo, N.J.; Joo, K.W.; Yi, N.J.; Suh, K.-S.; Moon, K.C.; Kim, S.G.; Kim, Y.S. Risk factors for consequent kidney impairment and differential impact of liver transplantation on renal function. Nephrol. Dial. Transpl. 2010, 25, 2772–2785.
- Leithead, J.A.; Ferguson, J.W.; Bates, C.M.; Davidson, J.S.; Simpson, K.J.; Hayes, P.C. Chronic kidney disease after liver transplantation for acute liver failure is not associated with perioperative renal dysfunction. Am. J. Transpl. 2011, 11, 1905–1915.
- Machicao, V.I.; Srinivas, T.R.; Hemming, A.W.; Soldevila-Pico, C.; Firpi, R.J.; Reed, A.I.; Morelli, G.J.; Nelson, D.R.; Abdelmalek, M.F. Impact of implementation of the MELD scoring system on the prevalence and incidence of chronic renal disease following liver transplantation. Liver Transpl. 2006, 12, 754–761.
- Morard, I.; Mentha, G.; Spahr, L.; Majno, P.; Hadengue, A.; Huber, O.; Morel, P.; Giostra, E. Long-term renal function after liver transplantation is related to calcineurin inhibitors blood levels. Clin. Transpl. 2006, 20, 96–101.
- Moreno, J.M.; Cuervas-Mons, V.; Rubio, E.; Pons, F.; de Herreros, A.T.; Turrión, V.S.; Millán, I. Chronic renal dysfunction after liver transplantation in adult patients: Prevalence, risk factors, and impact on mortality. Transpl. Proc. 2003, 35, 1907–1908.
- O’Riordan, A.; Wong, V.; McCormick, P.A.; Hegarty, J.E.; Watson, A.J. Chronic kidney disease post-liver transplantation. Nephrol. Dial. Transpl. 2006, 21, 2630–2636.
- Pawarode, A.; Fine, D.M.; Thuluvath, P.J. Independent risk factors and natural history of renal dysfunction in liver transplant recipients. Liver Transpl. 2003, 9, 741–747.
- Ramachandran, J.; Juneja, R.; John, L.; Dutta, A.K.; Chen, J.W.; Woodman, R.J.; Wigg, A.J. Chronic kidney disease following liver transplantation: A South Australian experience. Transpl. Proc. 2010, 42, 3644–3646.
- Sanchez, E.Q.; Melton, L.B.; Chinnakotla, S.; Randall, H.B.; McKenna, G.J.; Ruiz, R.; Onaca, N.; Levy, M.F.; Goldstein, R.M.; Klintmalm, G.B. Predicting renal failure after liver transplantation from measured glomerular filtration rate: Review of up to 15 years of follow-up. Transplantation 2010, 89, 232–235.
- Schmitz, V.; Laudi, S.; Moeckel, F.; Puhl, G.; Stockmann, M.; Tran, Z.V.; Kahl, A.; Neumann, U.; Neuhaus, P. Chronic renal dysfunction following liver transplantation. Clin. Transpl. 2008, 22, 333–340.
- Sezer, S.; Karakan, S.; Erişmiş, B.; Çolak, T.; Haberal, M. Risk factors for kidney impairment and differential impact of liver transplantation on renal function. Transpl. Proc. 2011, 43, 609–611.
- Shao, Z.-Y.; Yan, L.-N.; Wang, W.-T.; Li, B.; Wen, T.-F.; Yang, J.-Y.; Xu, M.-Q.; Zhao, J.-C.; Wei, Y.-G. Prophylaxis of chronic kidney disease after liver transplantation—Experience from west China. World J. Gastroenterol. 2012, 18, 991–998.
- Sharma, P.; Goodrich, N.P.; Schaubel, D.E.; Guidinger, M.K.; Merion, R.M. Patient-specific prediction of ESRD after liver transplantation. J. Am. Soc. Nephrol. 2013, 24, 2045–2052.
- Sharma, P.; Welch, K.; Eikstadt, R.; Marrero, J.A.; Fontana, R.J.; Lok, A.S. Renal outcomes after liver transplantation in the model for end-stage liver disease era. Liver Transpl. 2009, 15, 1142–1148.
- Cohen, A.J.; Stegall, M.D.; Rosen, C.B.; Wiesner, R.H.; Leung, N.; Kremers, W.K.; Zein, N.N. Chronic renal dysfunction late after liver transplantation. Liver Transpl. 2002, 8, 916–921.
- de Boccardo, G.; Kim, J.-Y.; Schiano, T.D.; Maurette, R.; Gagliardi, R.; Murphy, B.; Emre, S.; Akalin, E. The burden of chronic kidney disease in long-term liver transplant recipients. Transpl. Proc. 2008, 40, 1498–1503.
- Hao, J.-C.; Wang, W.-T.; Yan, L.-N.; Li, B.; Wen, T.-F.; Yang, J.-Y.; Xu, M.-Q.; Zhao, J.-C.; Wei, Y.-G. Effect of low-dose tacrolimus with mycophenolate mofetil on renal function following liver transplantation. World J. Gastroenterol. 2014, 20, 11356–11362.
- Jain, A.; Singhal, A.; Fontes, P.; Mazariegos, G.; DeVera, M.E.; Cacciarelli, T.; Lopez, R.C.; Sindhi, R.; Humar, A.; Marsh, J.W. One thousand consecutive primary liver transplants under tacrolimus immunosuppression: A 17- to 20-year longitudinal follow-up. Transplantation 2011, 91, 1025–1030.
- Kim, S.G.; Kim, H.J.; Lee, J.-P.; Lee, S.G.; Kim, Y.S.; Ahn, C.; Han, J.S.; Kim, S.; Lee, J.S.; Suh, K.-S. Incidence and risk factors of renal dysfunction after liver transplantation in Korea. Transpl. Proc. 2004, 36, 2318–2320.
- Kim, D.Y.; Lim, C.; Parasuraman, R.; Raoufi, M.; Yoshida, A.; Arenas, J.; Denny, J.; Malinzak, L.; Almarastani, M.; Moonka, D.; et al. Renal disease burden following liver transplantation. Transpl. Proc. 2006, 38, 3663–3665.
- Patel, H.K.; Patel, A.; Abouljoud, M.; Divine, G.; Moonka, D.K. Survival after liver transplantation in patients who develop renal insufficiency. Transpl. Proc. 2010, 42, 4167–4170.
- Kalisvaart, M.; Schlegel, A.; Trivedi, P.J.; Roberts, K.; Mirza, D.F.; Perera, T.; Isaac, J.I.; Ferguson, J.; de Jonge, J.; Muiesan, P. Chronic kidney disease after liver transplantation: Impact of extended criteria grafts. Liver Transpl. 2019, 25, 922–933.
- Fabrizi, F.; Dixit, V.; Martin, P.; Messa, P. Pre-transplant kidney function predicts chronic kidney disease after liver transplant: Meta-analysis of observational studies. Dig. Dis. Sci. 2011, 56, 1282–1289.
- Kim, J.-Y.; Akalin, E.; Dikman, S.; Gagliardi, R.; Schiano, T.; Bromberg, J.; Murphy, B.; de Boccardo, G. The variable pathology of kidney disease after liver transplantation. Transplantation 2010, 89, 215–221.
- Kubal, C.; Cockwell, P.; Gunson, B.; Jesky, M.; Hanvesakul, R.; Dronavalli, V.; Bonser, R.S.; Neil, D. Chronic kidney disease after nonrenal solid organ transplantation: A histological assessment and utility of chronic allograft damage index scoring. Transplantation 2012, 93, 406–411.
- Chonchol, M.; Wachs, M.; Taylor, J.; Popovtzer, M.M. Should we biopsy kidneys of patients post-liver transplant? Transpl. Proc. 2003, 35, 3035–3038.
- Beloncle, F.; Sayegh, J.; Duveau, A.; Besson, V.; Croue, A.; Subra, J.-F.; Augusto, J.-F. An unexpected cause of progressive renal failure in a 66-year-old male after liver transplantation: Secondary hyperoxaluria. Int. Urol. Nephrol. 2013, 45, 1209–1213.
- Kamar, N.; Maaroufi, C.; Guilbeau-Frugier, C.; Servais, A.; Meas-Yedid, V.; Tack, I.; Thervet, E.; Cointault, O.; Esposito, L.; Guitard, J.; et al. Do kidney histology lesions predict long-term kidney function after liver transplantation? Clin. Transpl. 2012, 26, 927–934.
- Sharma, P.; Schaubel, D.E.; Guidinger, M.K.; Goodrich, N.P.; Ojo, A.O.; Merion, R.M. Impact of MELD-based allocation on end-stage renal disease after liver transplantation. Am. J. Transpl. 2011, 11, 2372–2378.
- Watt, K.D.S.; Pedersen, R.A.; Kremers, W.K.; Heimbach, J.K.; Charlton, M.R. Evolution of causes and risk factors for mortality post-liver transplant: Results of the NIDDK long-term follow-up study. Am. J. Transpl. 2010, 10, 1420–1427.
- Leithead, J.A.; Armstrong, M.J.; Corbett, C.; Andrew, M.; Kothari, C.; Gunson, B.K.; Muiesan, P.; Ferguson, J.W. Hepatic ischemia reperfusion injury is associated with acute kidney injury following donation after brain death liver transplantation. Transpl. Int. 2013, 26, 1116–1125.
- Boin, I.F.S.F.; de Ataide, E.C.; Dias, E.P.O.; Stucchi, R.S.B.; Seva-Pereira, T.; Calomeni, G.; Capel Junior, C.C.; Mazzali, M. Can pre-liver transplantation renal insufficiency using a creatinine clearance calculator predict long-term survival? Transpl. Proc. 2012, 44, 2452–2454.
- Wenger, U.; Neff, T.A.; Oberkofler, C.E.; Zimmermann, M.; Stehberger, P.A.; Scherrer, M.; Schuepbach, R.A.; Cottini, S.R.; Steiger, P.; Béchir, M. The relationship between preoperative creatinine clearance and outcomes for patients undergoing liver transplantation: A retrospective observational study. BMC Nephrol. 2013, 14, 37.
- Aberg, F.; Lempinen, M.; Hollmén, M.; Nordin, A.; Mäkisalo, H.; Isoniemi, H. Neutrophil gelatinase-associated lipocalin associated with irreversibility of pre-liver transplant kidney dysfunction. Clin. Transpl. 2014, 28, 869–876.
- Afonso, R.C.; Hidalgo, R.; Zurstrassen, M.P.V.C.; Fonseca, L.E.P.; Pandullo, F.L.; Rezende, M.B.; Meira-Filho, S.P.; Ferraz-Neto, B.H. Impact of renal failure on liver transplantation survival. Transpl. Proc. 2008, 40, 808–810.
- Bahirwani, R.; Campbell, M.S.; Siropaides, T.; Markmann, J.; Olthoff, K.; Shaked, A.; Bloom, R.D.; Reddy, K.R. Transplantation: Impact of pretransplant renal insufficiency. Liver Transpl. 2008, 14, 665–671.
- Bahirwani, R.; Forde, K.A.; Mu, Y.; Lin, F.; Reese, P.; Goldberg, D.; Abt, P.; Reddy, K.R.; Levine, M. End-stage renal disease after liver transplantation in patients with pre-transplant chronic kidney disease. Clin. Transpl. 2014, 28, 205–210.
- Braun, N.; Dette, S.; Viebahn, R. Impairment of renal function following liver transplantation. Transpl. Proc. 2003, 35, 1458–1460.
- Campbell, M.S.; Kotlyar, D.S.; Brensinger, C.M.; Lewis, J.D.; Shetty, K.; Bloom, R.D.; Markmann, J.F.; Olthoff, K.M.; Shaked, A.; Reddy, K.R. Renal function after orthotopic liver transplantation is predicted by duration of pretransplantation creatinine elevation. Liver Transpl. 2005, 11, 1048–1055.
- Fujinaga, K.; Usui, M.; Yamamoto, N.; Ishikawa, E.; Nakatani, A.; Kishiwada, M.; Mizuno, S.; Sakurai, H.; Tabata, M.; Isaji, S. Hypertension and hepatitis C virus infection are strong risk factors for developing late renal dysfunction after living donor liver transplantation: Significance of renal biopsy. Transpl. Proc. 2014, 46, 804–810.
- Lebrón Gallardo, M.; Herrera Gutierrez, M.E.; Seller Pérez, G.; Curiel Balsera, E.; Fernández Ortega, J.F.; Quesada García, G. Risk factors for renal dysfunction in the postoperative course of liver transplant. Liver Transpl. 2004, 10, 1379–1385.
- Israni, A.K.; Xiong, H.; Liu, J.; Salkowski, N.; Trotter, J.F.; Snyder, J.J.; Kasiske, B.L. Predicting end-stage renal disease after liver transplant. Am. J. Transpl. 2013, 13, 1782–1792.
- Levitsky, J.; Salomon, D.R.; Abecassis, M.; Langfelder, P.; Horvath, S.; Friedewald, J.; Wang, E.; Kurian, S.M.; Mondala, T.; Gil, S.; et al. Clinical and plasma proteomic markers correlating with chronic kidney disease after liver transplantation. Am. J. Transpl. 2011, 11, 1972–1978.
- Moreno, J.M.; Rubio, E.; Pons, F.; Velayos, B.; Navarrete, E.; Herreros de Tejada, A.; López-Monclús, J.; Sánchez-Turrión, V.; Cuervas-Mons, V. Usefulness of mycophenolate mofetil in patients with chronic renal insufficiency after liver transplantation. Transpl. Proc. 2003, 35, 715–717.
- Northup, P.G.; Argo, C.K.; Bakhru, M.R.; Schmitt, T.M.; Berg, C.L.; Rosner, M.H. Pretransplant predictors of recovery of renal function after liver transplantation. Liver Transpl. 2010, 16, 440–446.
- Ruebner, R.L.; Reese, P.P.; Abt, P.L. Donation after cardiac death liver transplantation is associated with increased risk of end-stage renal disease. Transpl. Int. 2014, 27, 1263–1271.
- Asfandiyar, S.; Abouljoud, M.; Kim, D.; Brown, K.; Yoshida, A.; Arenas, J.; Sherbondy, M.; Divine, G.; Moonka, D. Influence of hepatitis C on renal function after liver transplantation. Transpl. Proc. 2006, 38, 3643–3645.
- Milongo, D.; Bascands, J.-L.; Huart, A.; Esposito, L.; Breuil, B.; Moulos, P.; Siwy, J.; Ramírez-Torres, A.; Ribes, D.; Lavayssière, L.; et al. Pretransplant urinary proteome analysis does not predict development of chronic kidney disease after liver transplantation. Liver Int. 2015, 35, 1893–1901.
- Warnaar, N.; Mallett, S.V.; de Boer, M.T.; Rolando, N.; Burroughs, A.K.; Nijsten, M.W.N.; Slooff, M.J.H.; Rolles, K.; Porte, R.J. The impact of aprotinin on renal function after liver transplantation: An analysis of 1043 patients. Am. J. Transpl. 2007, 7, 2378–2387.
- Bilbao, I.; Charco, R.; Balsells, J.; Lazaro, J.L.; Hidalgo, E.; Llopart, L.; Murio, E.; Margarit, C. Risk factors for acute renal failure requiring dialysis after liver transplantation. Clin. Transpl. 1998, 12, 123–129.
- Hand, W.R.; Whiteley, J.R.; Epperson, T.I.; Tam, L.; Crego, H.; Wolf, B.; Chavin, K.D.; Taber, D.J. Hydroxyethyl starch and acute kidney injury in orthotopic liver transplantation: A single-center retrospective review. Anesth. Analg. 2015, 120, 619–626.
- Tinti, F.; Umbro, I.; Giannelli, V.; Merli, M.; Ginanni Corradini, S.; Rossi, M.; Nofroni, I.; Poli, L.; Berloco, P.B.; Mitterhofer, A.P. Acute renal failure in liver transplant recipients: Role of pretransplantation renal function and 1-year follow-up. Transpl. Proc. 2011, 43, 1136–1138.
- De Boer, J.D.; Blok, J.J.; Braat, A.E. Graft quality and prediction of outcome after liver transplantation. Transplantation 2017, 101, e286.
- Christians, U.; Klawitter, J.; Klawitter, J.; Brunner, N.; Schmitz, V. Biomarkers of immunosuppressant organ toxicity after transplantation: Status, concepts and misconceptions. Expert Opin. Drug Metab. Toxicol. 2011, 7, 175–200.
- Fagundes, C.; Pépin, M.-N.; Guevara, M.; Barreto, R.; Casals, G.; Solà, E.; Pereira, G.; Rodríguez, E.; Garcia, E.; Prado, V.; et al. Urinary neutrophil gelatinase-associated lipocalin as biomarker in the differential diagnosis of impairment of kidney function in cirrhosis. J. Hepatol. 2012, 57, 267–273.
- Verna, E.C.; Brown, R.S.; Farrand, E.; Pichardo, E.M.; Forster, C.S.; Sola-Del Valle, D.A.; Adkins, S.H.; Sise, M.E.; Oliver, J.A.; Radhakrishnan, J.; et al. Urinary neutrophil gelatinase-associated lipocalin predicts mortality and identifies acute kidney injury in cirrhosis. Dig. Dis. Sci. 2012, 57, 2362–2370.
- Singal, A.K.; Jackson, B.; Pereira, G.B.; Russ, K.B.; Fitzmorris, P.S.; Kakati, D.; Axley, P.; Ravi, S.; Seay, T.; Ramachandra Rao, S.P.; et al. Biomarkers of renal injury in cirrhosis: Association with acute kidney injury and recovery after liver transplantation. Nephron 2018, 138, 1–12.
- Kalisvaart, M.; Schlegel, A.; Umbro, I.; de Haan, J.E.; Polak, W.G.; IJzermans, J.N.; Mirza, D.F.; Perera, M.T.P.; Isaac, J.R.; Ferguson, J.; et al. The AKI Prediction Score: A new prediction model for acute kidney injury after liver transplantation. HPB 2019, 21, 1707–1717.
- O’Leary, J.G.; Levitsky, J.; Wong, F.; Nadim, M.K.; Charlton, M.; Kim, W.R. Protecting the kidney in liver transplant candidates: Practice-Based recommendations from the american society of transplantation liver and intestine community of practice. Am. J. Transpl. 2016, 16, 2516–2531.
- Segev, D.L.; Sozio, S.M.; Shin, E.J.; Nazarian, S.M.; Nathan, H.; Thuluvath, P.J.; Montgomery, R.A.; Cameron, A.M.; Maley, W.R. Steroid avoidance in liver transplantation: Meta-analysis and meta-regression of randomized trials. Liver Transpl. 2008, 14, 512–525.
- Sgourakis, G.; Radtke, A.; Fouzas, I.; Mylona, S.; Goumas, K.; Gockel, I.; Lang, H.; Karaliotas, C. Corticosteroid-free immunosuppression in liver transplantation: A meta-analysis and meta-regression of outcomes. Transpl. Int. 2009, 22, 892–905.
- Neal, D.A.; Tom, B.D.; Gimson, A.E.; Gibbs, P.; Alexander, G.J. Hyperuricemia, gout, and renal function after liver transplantation. Transplantation 2001, 72, 1689–1691.
- Durand, F.; Francoz, C.; Asrani, S.K.; Khemichian, S.; Pham, T.A.; Sung, R.S.; Genyk, Y.S.; Nadim, M.K. Acute kidney injury after liver transplantation. Transplantation 2018, 102, 1636–1649.
- Hmoud, B.; Kuo, Y.-F.; Wiesner, R.H.; Singal, A.K. Outcomes of liver transplantation alone after listing for simultaneous kidney: Comparison to simultaneous liver kidney transplantation. Transplantation 2015, 99, 823–828.
- Gonwa, T.A.; McBride, M.A.; Anderson, K.; Mai, M.L.; Wadei, H.; Ahsan, N. Continued influence of preoperative renal function on outcome of orthotopic liver transplant (OLTX) in the US: Where will MELD lead us? Am. J. Transpl. 2006, 6, 2651–2659.
- Schmitt, T.M.; Kumer, S.C.; Al-Osaimi, A.; Shah, N.; Argo, C.K.; Berg, C.; Pruett, T.L.; Northup, P.G. Combined liver-kidney and liver transplantation in patients with renal failure outcomes in the MELD era. Transpl. Int. 2009, 22, 876–883.
- Locke, J.E.; Warren, D.S.; Singer, A.L.; Segev, D.L.; Simpkins, C.E.; Maley, W.R.; Montgomery, R.A.; Danovitch, G.; Cameron, A.M. Declining outcomes in simultaneous liver-kidney transplantation in the MELD era: Ineffective usage of renal allografts. Transplantation 2008, 85, 935–942.
- Sharma, P.; Shu, X.; Schaubel, D.E.; Sung, R.S.; Magee, J.C. Propensity score-based survival benefit of simultaneous liver-kidney transplant over liver transplant alone for recipients with pretransplant renal dysfunction. Liver Transpl. 2016, 22, 71–79.
- Ekser, B.; Mangus, R.S.; Fridell, W.; Kubal, C.A.; Nagai, S.; Kinsella, S.B.; Bayt, D.R.; Bell, T.M.; Powelson, J.A.; Goggins, W.C.; et al. A novel approach in combined liver and kidney transplantation with long-term outcomes. Ann. Surg 2017, 265, 1000–1008.
- Yunhua, T.; Qiang, Z.; Lipeng, J.; Shanzhou, H.; Zebin, Z.; Fei, J.; Zhiheng, Z.; Linhe, W.; Weiqiang, J.; Dongping, W.; et al. Liver transplant recipients with end-stage renal disease largely benefit from kidney transplantation. Transpl. Proc. 2018, 50, 202–210.
- Taner, T.; Heimbach, J.K.; Rosen, C.B.; Nyberg, S.L.; Park, W.D.; Stegall, M.D. Decreased chronic cellular and antibody-mediated injury in the kidney following simultaneous liver-kidney transplantation. Kidney Int. 2016, 89, 909–917.
- Singal, A.K.; Ong, S.; Satapathy, S.K.; Kamath, P.S.; Wiesner, R.H. Simultaneous liver kidney transplantation. Transpl. Int. 2019, 32, 343–352.


