 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Lisa F.P. Ng | + 6951 word(s) | 6951 | 2021-05-20 08:36:02 | | | |
| 2 | Peter Tang | -4 word(s) | 6947 | 2021-06-01 03:31:53 | | |
Video Upload Options
Alphaviruses are mosquito-borne pathogens distributed worldwide in tropical and temperate areas causing a wide range of symptoms ranging from inflammatory arthritis-like manifestations to the induction of encephalitis in humans. Historically, large outbreaks in susceptible populations have been recorded followed by the development of protective long-lasting antibody responses suggesting a potential advantageous role for a vaccine.
1. Introduction
2. Antibody-Mediated Alphavirus Immunity
2.1. Virus-Specific Antibody Kinetics Upon Natural Infection with Alphaviruses
2.2. Experimental Evidence of the Role of Antibodies in Alphavirus Immunity
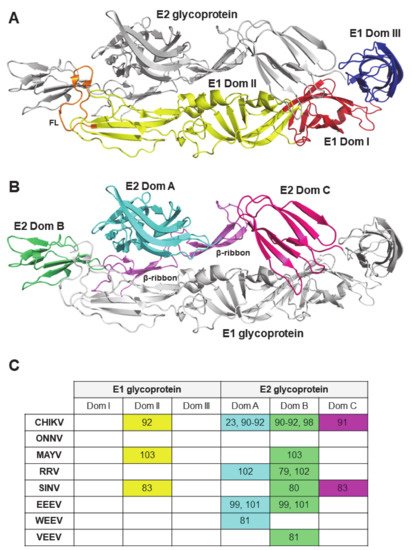
2.3. Viral Antigenic Regions Targeted by Neutralizing Antibodies
3. Alphavirus Vaccine Development
|
Vaccine Against Virus |
Name |
Strain Vaccine Modelled After |
Phase |
Immunization |
Challenge |
Humoral Immune Response(s) |
Ref |
|||
|---|---|---|---|---|---|---|---|---|---|---|
|
Dose |
Route |
Schedule |
Dose (Strain, Genotype) |
Route |
||||||
|
Live-attenuated |
||||||||||
|
CHIKV, ONNV |
RH-CHIKV EV-CHIKV RHEV-CHIKV |
LR2006 OPY1 |
C57BL/6 mice, 3 week old |
106 PFU |
s.c. in the ventral side of the right hind footpad |
Single dose |
106 PFU LR2006 OPY1 or WT-ONNV IMTSSA/5163, 3 mpim |
s.c. in the ventral side of the right hind footpad |
IC50, 613 (RH-CHIKV), 3407 (EV-CHIKV), 921 (RHEV-CHIKV) |
[130] |
|
CHIKV |
Δ5nsP3 (VLA1553-301 in clinical trials) and Δ6K |
LR2006 OPY1 |
C57BL/6 mice, 5 to 6 week old |
104 or 105 PFU |
s.c. in both flanks |
Single dose |
106 PFU LR2006 OPY1, 7 wpim |
s.c. |
NT50, 100 to 1000 |
|
|
Cynomolgus macaques, 3–4 years old |
105 PFU |
s.c. in the right upper back side |
Single dose |
100 AID50 (corresponding to 7000–10,000 PFU) LR2006 OPY1, 123 dpim |
i.v. |
NT50, >1000 |
||||
|
Human clinical trial, Phase 1 |
3.2 × 103, 3.2 × 104 or 3.2 × 105 TCID50 |
i.m. |
Two doses (0 and 6 months, or 0 and 12 months) |
NA |
NA |
GMT, 592.6 to 686.9 |
||||
|
CHIKV |
CHIKV-NoLS |
LR2006 OPY1 |
C57BL/6 mice, 21 days of age |
104 PFU |
s.c. |
Single dose |
104 PFU of LR2006 OPY1 or Ross River virus, 30 dpim |
s.c. |
<10% cells infected at 10-1 serum dilution |
[127] |
|
CHIKV |
Stop CHIKV SuperStop CHIKV |
LR2006 OPY1 |
C57BL/6 mice, 5 week old |
104 PFU |
s.c. |
Single dose |
ND |
ND |
~5–25 (Stop CHIKV) and ~10–25 (SuperStop CHIKV) fold reduction compared to mock |
[134] |
|
CHIKV |
ChikV HR |
37997 |
C57BL/6 mice, 28 days of age |
∼103 PFU |
s.c. into the left footpad |
Single dose |
103 PFU CHIKV SL15649, 28 dpim |
s.c. in the footpad |
PRNT50, 5 to ~500 |
[135] |
|
CHIKV |
Heparin sulfate cell culture adapted |
LR2006 OPY1 |
CD-1 mice, 21 days old |
105 GE |
s.c. in the rear footpad |
Single dose |
103 PFU LR2006 OPY1, 21 dpim |
NA |
~40 to 1000 fold change compared to mock |
[136] |
|
VEEV |
V3526 |
IA/B Trinidad donkey |
BALB/c, 6 to 8 week oldC3H/HeN mice, 6 to 8 week old |
105 PFU |
s.c. |
Single dose |
105 PFU of TrD, 28 dpim |
NP |
ND |
|
|
Cynomolgus macaques (age not specified) |
2.5 × 106 PFU |
s.c. |
Single dose |
∼108 PFU VEEV IE 68U201, 8 wpim |
aerosol |
PRNT80, 28 to 2560 |
||||
|
Rhesus macaques (2 to 4 years old) |
1.3 × 105 or 7.5 × 104 PFU |
s.c. or i.t./i.s. |
Single dose |
ND |
ND |
PRNT80, ~80 to 300 |
||||
|
Human clinical trial, Phase 1 |
25 or 125 PFU |
s.c. |
Single dose |
NA |
NA |
NA |
||||
|
VEEV |
V4020 |
IA/B Trinidad donkey |
BALB/c mice, 4 to 8 week old |
104 PFU |
s.c. |
Single dose |
104 PFU of VEEV TrD, 28 dpim |
s.c. |
PRNT80, 160 to1280 |
|
|
Cynomolgus macaques (age not specified) |
~104 PFU |
s.c. in the right leg |
Single dose (or second dose at 2 x 104 PFU i.m. if did not seroconvert) |
106 to 107 PFU of the VEEV TrD, 73 dpim |
aerosol |
PRNT80, >640 |
||||
|
EEEV |
5′U4&6 C65-69 E71-77 3′U11337 mutants |
FL93-939 |
CD-1 mice, 5 to 6 week old |
1.5 × 105 GE |
s.c. in footpad, or i.c. |
Single dose |
105 PFU EEEV FL93, 21 dpim |
s.c. in both footpads |
PRNT80, 16 to ~4000 |
[143] |
|
Live-attenuated (IRES) |
||||||||||
|
CHIKV |
CHIKV/IRES |
LR2006 OPY1 |
A129 mice, 3 or 10 week old |
104 PFU |
i.d. |
Single dose |
100 PFU LR2006 OPY1, 94 dpim |
i.d. |
PRNT80, >320 |
|
|
C57BL/6 mice, 3 week old |
105 PFU |
s.c. in the hind leg |
Single dose |
106.5 PFU Ross CHIKV, 21 dpim |
i.n. |
Mean PRNT80, 62 |
||||
|
A129 mice, 8 to 10 week old |
105 TCID50 |
s.c. |
Single dose |
100 PFU LR2006 OPY1, 50 dpim |
i.d. |
Mean PRNT80, 1152 |
||||
|
Cynomolgus macaques, >3 years old |
105 PFU |
s.c. or i.d. |
Single dose |
105 PFU LR2006 OPY1, 52 dpim |
s.c. in the upper deltoid |
PRNT80, 40 to 640PRNT50, 160 to 1280 |
||||
|
ONNV |
CHIKV/IRES |
LR2006 OPY1 |
A129 mice, 6 to 7 week old |
104 PFU |
i.d. |
Single dose |
105 PFU ONNV SG650, 38 dpim |
i.d. |
PRNT80, 160 |
[146] |
|
VEEV |
ZPC/IRESv1, ZPC/IRESv2 |
ID ZPC738 |
CD-1 mice, 6 to 8 week old |
105 PFU |
s.c. in the scruff of the back |
Single dose |
105 PFU VEEV 3908, 4 wpim |
s.c. or aerosol |
PRNT80, 40 to 324 |
[114] |
|
Cynomologous macaques, age not specified |
105 PFU |
s.c. in the upper deltoid |
Single dose |
~ 8 × 105 to 9 × 106 PFU VEEV 3908, 35 dpim |
aerosol |
PRNT80, <20 to 20PRNT50, <20 to 160 |
||||
|
EEEV |
EEE/IRES |
FL93-939 |
NIH Swiss mice, 3 to 4 week old |
104 PFU |
s.c. in the medial thigh |
Single dose |
103 PFU of FL93-939, 4 wpim |
i.p. |
PRNT80, 160 to 640 |
[147] |
|
VEEV |
68U201/IRESv1 68U201/IRESv2 |
IE 68U201 |
CD1 mice, 6 to 8 week old |
105 PFU |
s.c. in right hind leg |
Single dose |
(Lethal dose, NP) 68U201 at 1, 3, or 12 mpim |
s.c. |
PRNT80, 64 to ~300 |
|
|
Cynomolgus macaques (age not specified) |
105 PFU |
s.c. in the upper deltoid |
Single dose |
4 × 104 PFU VEEV IE 68U201, 49 dpim |
aerosol |
PRNT80, ~100 to 340 |
||||
|
VEEV |
VEEV/IRES/C |
IA/B Trinidad donkey |
CD-1 mice, 8 week old |
105 PFU |
s.c. |
Single dose |
104 PFU of VEEV 3908, 6 wpim |
s.c. |
Mean PRNT80, 184 |
[150] |
|
MAYV |
MAYV/IRES |
MAYV-CH |
BALB/c, 6 week old |
2 × 105 PFU |
s.c. i.pl. route |
Single dose |
2 × 105 PFU of WT MAYV, 28 dpim |
s.c. i.pl. route |
PRNT50, >640 (at 21dpi) |
|
|
AG129 |
2 × 104, 2 × 103 or 2 × 102 PFU |
s.c. i.pl. route |
Single dose |
2 × 103 PFU of WT MAYV, 14 dpim |
s.c. i.pl. route |
ND |
||||
|
CD-1, 28-day old |
105 PFU |
s.c. over the dorsum |
Single dose |
ND |
ND |
PRNT80, 160 to ≥ 640 |
||||
|
AG129, 5 to 8 week old |
104 PFU |
i.d. on the left foot |
Single dose |
104 PFU of WT MAYV, 29 dpim |
s.c. |
PRNT80, 320 to ≥ 640 |
||||
|
Inactivated |
||||||||||
|
CHIKV |
Vero cell adapted |
DRDE-06 |
Swiss albino mice, 3 to 4 week old |
10, 25 or 50 ug |
s.c. |
Three doses (0, 14 and 28 days) |
ND |
ND |
PRNT90, 6400 |
[153] |
|
CHIKV |
BPL/formalin-inactivated CHIKV BBV87 (in clinical trials) |
IND-06-AP3 |
BALB/c mice, 4 to 6 week old |
10, 20 or 50 μg |
i.m. |
Two doses (0 and 14 days) |
2.5 x 104 TCID50 IND-06-AP3, 4 or 22 wpim |
i.n. |
GMT, NT50, 80 to 1280 |
[154] |
|
Human clinical trial, Phase 1 |
10, 20 or 30 μg |
i.m. |
Three doses (0, 29 and 57 days) |
NA |
NA |
NA |
[155] |
|||
|
RRV |
Vero cell culture-derived whole-virus RRV vaccine Ross River Virus (RRV) Vaccine |
T48 |
CD-1 mice, 7 to 8 week old |
0.0025, 0.01, 0.039, 0.156, 0.625, 2.5 or 10 μg |
s.c. |
Two doses (0 and 28 days) |
106 TCID50 RRV T48, 42 dpim |
i.v. |
Mean NT, ≤2.9 to 46.2 |
|
|
A129 mice, 7 to 8 week old |
0.063, 0.25 or 1 μg |
i.m. |
Two doses (0 and 21 days) |
102.5 TCID50 T48, 42 dpim |
s.c. into left footpad |
Mean NT, ≤14 to 21 |
||||
|
CD-1 mice, age not specified |
10 μg |
s.c. |
Two doses (0 and 28 days) |
106 TCID50 T48, 6 wpim |
i.v. |
1000 TCID50 |
||||
|
Guinea pigs (Duncan Hartley), age not specified |
10 μg |
s.c. |
Single or two doses (0 and 6 weeks) |
106 TCID50 T48, 10 or 34 wpim |
i.v. |
NP |
||||
|
Human clinical trial, Phase 1/2 |
1.25, 2.5, 5, or 10 μg |
i.m. |
Three doses in escalation (0, 21 days, 6 months) |
NA |
NA |
GMT, 50 to 520.9 |
||||
|
Human clinical trial, Phase 3 |
2.5 ug |
i.m. |
Three doses (0, 3 weeks, 6 months) |
NA |
NA |
μNT GMT, ~0 to 85 |
||||
|
EEEV |
TSI-GSD-104 (formalin inactivated) |
PE-6 |
Human clinical trial, Phase 2 |
NP |
s.c. (0 and 28 days), i.d. (6 months) |
Three doses (0, 28 days and 6 months) |
NA |
NA |
PRNT80 >40 in 60% subjects (primary doses) versus 84% subjects (completed the 2-dose primary series and the 6-month dose) |
|
|
EEEV |
fCVEV1219 iCVEV1219 gCVEV1219 |
CVEV1219 |
BALB/c mice, 6 to 8 week old |
0.1 to 5 µg of inactivated EEEV |
i.n., s.c. or i.m. |
Single dose or two doses (0 and 28 days) |
Lethal dose of EEEV FL93-939, at 28 dpim (single dose) or 56 dpim (two doses) |
aerosol |
PRNT80, ~1 to 1000 |
[159] |
|
VEEV |
V3526 virus |
V3526 |
BALB/c mice, 6 week old |
0.2 μg (s.c.) or 0.04 μg (i.m.) |
s.c. or i.m. |
Two doses (0 and 28 days) |
104 PFU VEEV TrD, 56 dpim |
aerosol or s.c. |
GMT PRNT80, ~60 to 2500 |
[160] |
|
VEEV |
F-iV3526 |
V3526 |
BALB/c mice, 8 to 10 weeks old |
1, 3 or 5 μg |
i.n., s.c. (under the skin over the neck) or i.m. (thigh muscle of the hind leg) |
Single dose |
454 (i.n.), 897 (i.m.) or 55 (s.c.) PFU VEEV-TrD, 56 dpim |
aerosol |
Microneutralization titer of 100 to 3500 |
|
|
Virus-like particle |
||||||||||
|
CHIKV |
VRC 311 Or VRC-CHKVLP059-00-VP/ PXVX0317 (in clinical trials) |
37997 |
BALB/c mice, 6 to 8 week old |
19 μg |
i.m. |
2 doses (2 and 5 weeks) |
ND |
ND |
IC50, 10703 to 54600 |
|
|
Cynomolgus macaques, 3 to 4 years old |
20 μg |
i.m. |
3 doses (0, 4 and 24 weeks) |
1010 PFU LR2006 OPY1, 15 wpim |
i.v. |
IC50, 10219 to 15072 |
||||
|
Human clinical trial, Phase 1 |
10, 20 or 40 μg |
i.m. |
3 doses (0, 4 and 24 weeks) |
NA |
NA |
IC50, 4525 to 8745 |
||||
|
Human, clinical trial Phase 2 |
20 μg |
i.m. |
2 doses (0 and 28 days) |
NA |
NA |
EC50 GMT, 2005 |
||||
|
Human clinical trial (Phase 2b, recruitment completed) |
6, 10 or 20 μg |
NP |
Two doses (0 and 14 or 28 days) |
NA |
NA |
NA |
||||
|
CHIKV |
Baculovirus-expressed VLP |
S27 |
AG129, 6 week old |
1 μg |
s.c. |
2 doses (0 and 21 days) |
1000 TCID50 S27, 6 wpim |
i.p. |
PRNT95, 40 to 80 |
|
|
C57BL/6 mice, 6 to 12 week old |
0.1 or 1 μg |
s.c. |
Single dose |
104 CCID50 LR2006 OPY1, 6 wpim |
s.c. |
NT95, ~1,100 |
||||
|
CHIKV |
Yeast-expressed VLP |
DRDE06/DRDE07 |
BALB/c mice, 4 week or 2 days old |
10, 20 or 40 ug |
s.c. |
Three doses (0, 14 and 28 days) |
ND |
ND |
NT50, 128 to 2048 |
[166] |
|
VEEV |
Venezuelan Equine Encephalitis Monovalent Virus-Like Particle Vaccine (VEEV) |
NA |
Human clinical trial (Phase 1, not recruiting) |
2, 10, or 20 μg |
i.m. |
Dose escalation (0, 28 days, and day 140 booster) |
NA |
NA |
NA |
[167] |
|
WEEV, EEEV, and VEEV |
VRC-WEVVLP073-00-VP (Trivalent vaccine) |
WEEV CBA87, EEEV PE-6 and VEEV TC-83 |
BALB/c mice, 6 to 8 week old |
monovalent (5 μg) or trivalent (5 μg each) |
i.m. |
Two doses (0 and 21 days) |
2.5 × 103 PFU WEEV CBA87, 8.9 × 103 PFU EEEV FL93-939, and 1.3 × 103 PFU VEEV Trinidad donkey, 56 dpim |
aerosol |
PRNT80, ~250 to 100000 |
[168] |
|
Cynomolgus macaques, age not specified |
Monovalent (20 μg) or trivalent (20 μg each) |
i.m. |
Two doses (0 and 28 days) |
106 PFU WEEV CBA87, 108 PFU EEEV FL93-939, and 108 VEEV Trinidad donkey, 56 dpim |
aerosol |
PRNT80, ~1000 to 10000 |
||||
|
Human clinical trial, Phase 1 |
6, 30 or 60 μg |
i.m. |
Dose escalation (0 and 8 weeks) |
NA |
NA |
NA |
[169] |
|||
|
DNA/RNA |
||||||||||
|
VEEV |
VEEV 26S DNA plasmid |
I/AB TrD |
BALB/c mice, 6 to 8 week old |
∼3 μg |
DNA/gene gun, delivered to two sites on the abdomen of each mouse |
Three doses (at 3-week intervals) |
∼104 PFU of TrD, 9 wpim |
s.c., aerosol |
PRNT50, GMT <1.6 to 2.5 |
|
|
Hartley guinea pigs, age not specified |
~5 μg |
DNA/gene gun, delivered to two sites on the abdomen of each mouse |
Three doses (0, 4 and 8 weeks) |
∼104 PFU of TrD, 21 wpim |
aerosol |
PRNT50, 0 to 640 |
||||
|
VEEV |
DNA-Ad |
TC-83 |
BALB/c mice, 6 to 8 week old |
1 μg of DNA per dose and 107 PFU of RAd/VEEV #3 per boost |
gene guni.n. |
immunised with the DNA vaccines on day 0, 14 and 28 and Ad-based vaccine on day 42 |
100 LD50 of virulent airborne VEEV, 63 dpim |
aerosol |
PRNT50, 160 |
[172] |
|
VEEV |
AG4-1C7 AG4-1G2 AG2-5A7 AG2-5A10 plasmid DNA |
I/AB TrD |
BALB/c mice, 6 to 8 week old |
4 μg |
particle-mediated epidermal delivery (i.d.) |
Three doses (at 3-week intervals) |
∼104 PFU of VEEV TrD (≥1000 LD50), 70 dpim |
aerosol |
PRNT80, ~1 to 5.5 log10 GMT |
[173] |
|
VEEV |
pTC83 iDNA |
TC-83 |
BALB/c mice, 3 week old |
50 μg |
i.m. electroporation |
Single dose |
105 PFU VEEV 3908, 21 dpim |
s.c. |
PRNT80, 10 to 320 |
[174] |
|
WEEV |
pE3-E2-6K-E1 pE3-E2 P6K-E1 |
71V-1658 |
BALB/c, age not specified |
2 μg |
gene gun |
Three doses (14 days apart) |
1500 PFU WEEV 71V-1658, Fleming, or CBA87, 42 dpim |
i.n. |
ND |
[175] |
|
CHIKV |
pCHIKV-Capsid, pCHIKV-Envelope (pMCE321) |
Consensus |
C57BL/6 mice, 3 to 4 week old |
25 µg, 2–3 times |
Electroporation |
Two doses (2 weeks apart) |
ND |
ND |
ND |
|
|
C57BL/6 mice, 6 to 8 week old |
25 μg |
i.m. electroporation |
Three doses (0, 14 and 21 days) |
7log10 PFU of PC-08, 35 dpim |
i.n. |
NP |
||||
|
BALB/c mice |
25 μg |
i.m. electroporation |
Two doses (2 weeks apart) |
7log10 PFU PC-08 |
i.n. |
TCID50, 20 to 320 |
||||
|
Rhesus macaques, age not specified |
1 mg |
i.m. electroporation |
Three doses (4 weeks apart) |
ND |
ND |
TCID50, 80 to 1280 |
||||
|
CHIKV |
Δ5nsP3 and Δ6K DNA |
LR2006 OPY1 |
C57BL/6 mice, 5 to 6 week old |
20 μg |
i.d. with DermaVax electroporation |
Single dose or two doses (0 and 3 weeks) |
106 PFU LR2006 OPY1, 7 wpim |
s.c. |
NT50, 100 to 10000 |
[131] |
|
CHIKV |
CHIKV-NoLS RNA |
LR2006 OPY1 |
C57BL/6 mice, 28 days of age |
2 μg |
s.c. in the ventral/lateral side of the right foot |
Single dose |
104 PFU LR2006 OPY1, 30 dpim |
s.c. in the ventral/lateral side of the right (ipsilateral) or left (contralateral) |
PRNT80, 0 |
[126] |
|
AG129 mice, 28 days old |
2 μg |
s.c. in the ventral/lateral side of the right foot |
Single dose |
104 PFU LR2006 OPY1, 30 dpim |
s.c. in the ventral/lateral side of the right (ipsilateral) or left (contralateral) |
ND |
||||
|
VEEV, WEEV and EEEV |
3-EEV |
VEEV IAB TrD, WEEV CBA874 and EEEV FL91-46794 |
C57BL/6 mice, 6 to 8 week old |
15 μg |
i.m. electroporation |
Two doses (0 and 21 days) |
104 PFU VEEV IAB TrD or 2 × 104 PFU WEEV CBA874 or 105 PFU EEEV FL91-46794, 7 wpim |
aerosol |
PRNT80, ~1 to 1000 |
[179] |
|
MAYV |
scMAYV-E |
NA |
C57BL/6 mice, 5 to 8 week old |
25 μg |
i.m. electroporation |
Single, two doses or three doses (at 2 week intervals) |
ND |
ND |
PRNT50, 789.8 |
[180] |
|
A129 mice, 4 to 6 week old |
25 μg |
i.m. electroporation |
Single, two doses or three doses (at 2 week intervals) |
102 PFU MAYV 15537 |
i.p. |
ND |
||||
|
CHIKV |
p181/25-7 |
TSI-GSD-28 |
BALB/c mice, 3 week old |
10 μg |
i.m. electroporation |
Single dose |
6 × 106 PFU CHIKV Ross, 28 dpim |
i.n. |
PRNT80, 160 to 1280 |
[181] |
|
CHIKV |
dMaB |
NA |
BALB/c mice, age not specified |
100 μg |
Electroporation |
Single dose |
107 PFU Del-03 |
s.c. or i.n. |
IC50, 3 to 4.5log10 |
[182] |
|
CHIKV |
iRNAΔ5nsP3 iDNAΔ5nsP3 |
LR2006 OPY1 |
C57BL/6 mice, 8 week old |
0.125, 1.25 or 10 μg |
i.m. in the gastrocnemius muscle of the left hind leg |
Single dose |
106 PFU LR2006 OPY1, 5 wpim |
s.c. at the dorsal side of each hind foot |
NT50, ~1 to 104 |
[183] |
|
VEEV |
pMG4020 DNA plasmid |
TC-83 |
BALB/c, 4 to 8 week old |
0.5 or 5 ug |
i.m. electroporation |
Single dose |
104 PFU VEEV TrD, 28 dpim |
s.c. |
PRNT80, 320 to >1280 |
[141] |
|
VEEV |
VEEVWT VEEVCOCAP VEEVCO |
IAB TrD |
BALB/c, 6 to 8 week old |
25, 5, or 1 μg |
i.m. electroporation |
Two doses (3 weeks apart) |
∼104 PFU VEEV IAB strain TrD, 7 wpim |
aerosol |
PRNT80, 1 to ~4.5log10 |
|
|
New Zealand White rabbits, age not specified |
500 μg of VEEVCO |
i.m. electroporation |
Three doses (0, 28 and 230 days) |
ND |
ND |
PRNT80, ~3log10 to 5log10 |
||||
|
Cynomolgus macaques, age not specified |
50 or 500 μg of VEEVCO |
i.m. electroporation |
Two doses (0 and 56 days) |
3 × 108 PFU VEEV IAB TrD |
aerosol |
PRNT80, ~0.8log10 to 3.5log10 |
||||
|
Human clinical trial, Phase 1 |
0.5 or 2 mg |
i.m. electroporation or i.d. electroporation |
Three doses (days 0, 28, and 56) |
NA |
NA |
GMT PRNT80, 7 to 78 |
||||
|
WEEV |
pVHX-671V-1658 pVHX-6 CBA87 pVHX-6 Fleming |
Fleming, CBA 87 or 71V-1658, |
BALB/c mice, age not specified |
2 shots × 2.5 μg precipitated on 0.5 mg gold |
gene gun |
Four doses (2 weeks apart) |
1.5 × 103 PFU WEEV Fleming, CBA 87 or 71V-1658, 8 wpim |
i.n. |
ND |
[186] |
|
WEEV and EEEV |
LANAC E1ecto |
WEEV McMillan |
CD-1 mice, 4 to 6 week old |
10 μg |
s.c. injection dorsal to the cervical spine |
Two doses (2 weeks apart) |
104 PFU WEEV McMillan, Montana-64, or EEEV Florida-93, 4, 5, 9, 11, or 13 wpim |
i.n. or s.c. |
PRNT50, <40 to 200 |
[187] |
|
CHIKV |
mRNA-1388 (or VAL-181388 in clinical trials) |
NA |
Human clinical trial, Phase 1 |
25, 50 or 100 μg |
i.m. |
Dose escalation procedure (0 and 4 weeks) |
ND |
ND |
‘dose-dependent increase’ in neutralizing and binding antibody titers |
[188] |
|
CHIKV |
mRNA-1944 |
SL15649 |
AG129, age not specified |
0.4, 1 or 10 mg/kg |
i.v. tail vein injection |
Single dose |
102.5 TCID50 of CHK |
subcutaneous injection in the footpad and hock of the right leg |
ND |
|
|
Cynomolgus macaques, 2 to 3 year old |
0.5 mg/kg |
i.v. |
Single dose |
ND |
ND |
FRNT50, 5 to 12 |
||||
|
Human clinical trial, Phase 1 (active, not recruiting) |
0.1, 0.3 and 0.6 mg/kg |
i.v. |
Dose escalation |
NA |
NA |
NT50, ‘all participants also showed circulating neutralizing antibody activity’ |
||||
|
Subunit |
||||||||||
|
CHIKV |
CHIKV-sE1 and -sE2 |
S27 |
AG129 mice, 6 week old |
2 μg |
s.c. |
Two doses (0 and 21 days) |
1000 TCID50 of S27 isolate, 9 wpim |
i.p. |
NT95, <25 |
|
|
CHIKV |
rE2p |
IND-06-AP3 |
BALB/c, 6 to 8 week old |
10, 20 or 50 μg |
i.m. |
Two doses (2 weeks apart) |
Mice immunized with 50 μg challenged with 7 log10 TCID50 /mL, 4 or 22 wpim |
i.n. |
NT50, 0.25log10 to 2.5log10 |
[154] |
|
CHIKV |
CHIKE1 and CHIKE2 recombinant proteins |
DRDE-06 |
BALB/c |
40 μg |
s.c. |
Three doses (0, 21 and 35 days) |
ND |
ND |
PRNT90, 32 to 512 |
[192] |
|
Chimeric virus |
||||||||||
|
Measles virus-based chimeras |
||||||||||
|
CHIKV (VLP) |
MV-CHIKV |
06–49 |
CD46-IFNAR, 6 week old |
103 to 105 TCID50 |
i.p. |
Single or two doses (30 days apart) |
100 PFU of CHIKV 06-49, 2 mpim |
i.p. |
PRNT50, 450 to 4050 PRNT90, 50 to 450 |
|
|
Cynomolgus macaques, age not specified |
5 × 105 (± 0.5 log) TCID50 |
i.m. |
Two doses (28 days apart) |
1.4 × 105 PFU LR2006 OPY1, 56 dpim |
s.c. |
PRNT80, 40 to >640 |
||||
|
Human clinical trial, Phase 1 |
1.5 × 104, 7.5 × 104 or 3.0 × 105 TCID50 |
i.m. or s.c. |
Dose escalation (0 and 28 days, or 0 and 90 days) |
NA |
NA |
PRNT50, 5 to 433 |
||||
|
Human clinical trial, Phase 2 |
5 × 104 or 5 × 105 TCID50 |
i.m. |
Three doses (0, 28, and 196 days) |
NA |
NA |
PRNT50, ~5 to 5000 |
||||
|
Alphavirus-based chimeras |
||||||||||
|
CHIKV |
VEE/CHIKV EEE/CHIKV SIN/CHIKV |
LR2006 OPY1 |
NIH Swiss, C57BL/6, >3 week old |
5.8 log10 PFU (VEE/CHIKV and SIN/CHIKV), 5.3 log10 PFU (EEE/CHIKV) |
s.c. in the medial thigh |
Single dose |
6.5 log10 PFU (Ross CHIKV strain), 21 dpim |
i.n. |
PRNT80, 20 to 320 |
[198] |
|
CHIKV |
VEE/IRES-CHIKV VEE/IRES-C/CHIKV |
NA |
A129 mice, 6 to 9 week old |
104 PFU |
s.c. |
Single dose |
102 PFU of LR2006 OPY1, 5 weeks post immunization |
s.c. |
PRNT80, >640 |
[199] |
|
CHIKV |
EILV-CHIKV |
CHIKV 996659 |
C57BL/6 mice, 4 week old |
8.8 log10 PFU |
s.c. |
Single dose |
6 log10 PFU 99659, 30 dpim |
i.d. |
PRNT80, ≥ 80 |
|
|
IFNα/βR−/−, 6 week old |
8.8 log10 PFU |
s.c. |
Single dose |
3 log10 PFU 99659, 292 dpim |
i.d. |
PRNT80, 160 to 1280 |
||||
|
Cynomolgus macaques, 3 to 5 years |
8.1 log10 PFU |
i.m. into the right quadriceps |
Single dose |
5 log10 PFU LR2006 OPY1, 31 dpim |
s.c. |
PRNT80, 80 to 640 |
||||
|
EEEV |
EILV/EEEV |
EEEV FL-93 |
Adult CD-1 mice (age not specified) |
108 PFU |
s.c. |
Single dose |
105 PFU EEEV-FL93, 70 dpim |
i.p. |
PRNT80, 80 to 640 |
|
|
EEEV |
Trivalent EILV/EEEV EILV/VEEV EILV/CHIKV |
EEEV FL-93, VEEV IAB TC-83, CHIKV 996659 |
Adult CD-1 mice (age not specified) |
108 PFU |
s.c. |
Single dose |
105 PFU EEEV-FL93, 70 dpim |
i.p. |
PRNT80, 40 to 640 and 20 to 640 for mono- and trivalent vaccines respectively |
|
|
VEEV |
EILV/EEEV |
VEEV IAB TC-83 |
Adult CD-1 mice (age not specified) |
108 PFU |
s.c. |
Single dose |
103 PFU VEEV-IC 3908, 70 dpim |
s.c. |
PRNT80, 80 to 1280 |
|
|
VEEV |
Trivalent EILV/EEEV, EILV/VEEV EILV/CHIKV |
EEEV FL-93, VEEV IAB TC-83, CHIKV 996659 |
Adult CD-1 mice (age not specified) |
108 PFU |
s.c. |
Single dose |
103 PFU VEEV-IC 3908, 70 dpim |
s.c. |
PRNT80, 40 to 640 and 20 to 80 for mono- and trivalent vaccines respectively |
|
|
EEEV (Sindbis virus) |
SIN/NAEEEV |
EEEV FL93-939 |
NIH Swiss mice, 8 week old |
3.7, 4.7 or 5.7 log10 PFU |
s.c. |
Single dose |
6 log10 PFU FL93-939, 28 dpim |
i.p. |
PRNT80, 125 to 660 |
[200] |
|
SIN/SAEEEV |
EEEV BeAr436087 |
NIH Swiss mice, 8 week old |
3.8, 4.8 or 5.8 log10 PFU |
s.c. |
Single dose |
6 log10 PFU FL93-939, 28 dpim |
i.p. |
PRNT80, 28 to 308 |
||
|
VEEV |
SIN-83 |
VEEV IAB TC-83 |
Weanling NIH Swiss mice, 6 day old |
103, 104, 105 or 106 PFU |
s.c. |
Single dose |
106 PFU VEEV IC ZPC738 IC SH3 |
s.c.in medial thigh |
PRNT80, 30 to 960 |
|
|
NIH Swiss mice, 6 week old |
5 × 105 PFU |
s.c. |
Two doses |
2 x 105 or 106 PFU VEEV ZPC738, 8 wpim |
s.c., i.c., or i.n. |
PRNT80, 55 to 73 (single), 100 to 160 (booster) |
||||
|
SAAR/TRD |
VEEV IAB TrD |
NIH Swiss mice, 6 week old |
5 × 105 PFU |
s.c. |
Two doses |
2 x 105 or 106 PFU VEEV ZPC738, 8 wpim |
s.c., i.c., or i.n. |
PRNT80, 126 to 167 (single), 152 to 160 (booster) |
||
|
SIN/TRD |
VEEV IAB TrD |
NIH Swiss mice, 6 week old |
5 × 105 PFU |
s.c. |
Two doses |
2 x 105 or 106 PFU VEEV ZPC738, 8 wpim |
s.c., i.c., or i.n. |
PRNT80, 37 to 57 (single), 50 to 73 (booster) |
||
|
SIN/ZPC |
VEEV ID ZPC738 |
NIH Swiss mice, 6 week old |
5 × 105 PFU |
s.c. |
Two doses |
2 x 105 or 106 PFU VEEV ZPC738, 8 wpim |
s.c., i.c., or i.n. |
PRNT80, 187 to 253 (single), 253 to 487 (booster) |
||
|
All the above |
VEEV IAB TC-83, IAB TrD, ID ZPC738 |
Syrian golden hamsters, 6 week old |
5 × 105 PFU |
s.c. in the medial thigh |
Single dose |
106 PFU |
s.c.in medial thigh |
ND |
||
|
WEEV |
SIN/CO92 |
WEEV CO92-1356 |
NIH Swiss mice, 6 week old |
3.5, 4.5, or 5.0 log10 PFU |
s.c. in the medial thigh |
Single dose |
5.3 log10 PFU WEEV TBT235, 28 dpim |
i.n. |
PRNT80, 20 to 640 |
[203] |
|
SIN/SIN/McM |
WEEV McMillan |
NIH Swiss mice, 6 week old |
4.8 or 5.8 log10 PFU |
s.c. in the medial thigh |
Single dose |
5.0 log10 PFU WEEV McMillan, 28 dpim |
i.n. |
PRNT80, 600 to 604 |
||
|
SIN/EEE/McM |
EEEV 436087 and WEEV McMillan |
NIH Swiss mice, 6 week old |
4.6 or 5.6 log10 PFU |
s.c. in the medial thigh |
Single dose |
5.0 log10 PFU WEEV McMillan, 28 dpim |
i.n. |
PRNT80, 416 to 420 |
||
|
Vaccinia virus-based chimeras |
||||||||||
|
CHIKV |
MVA-CHIKV |
LR2006-OPY1 |
C57BL/6 mice, 6 to 8 week old |
107 PFU (first dose), 2 × 107 PFU (second dose) |
i.p. |
Two doses (2 weeks apart) |
106 PFU LR2006-OPY1, 9 wpim |
s.c. in the dorsal side of each hind foot |
NT50, ~100 to 3000 |
[204] |
|
CHIKV |
MVA-CHIK |
LR2006-OPY1 |
BALB/c mice, 4 to 6 week old |
107 TCID50 units |
i.d. injection into the left hind footpad. |
Single or two doses (28 days apart) |
104 LR2006 OPY1 TCID50 units at 39 or 42 dpim |
i.d. |
TCID50, 5 to 15 |
[205] |
|
AG129, 6 to 10 week old |
107 TCID50 units |
i.d. injection into the left hind footpad. |
Single or two doses (28 days apart) |
102 LR2006 OPY1 TCID50 units at 39 or 42 dpim |
i.d. |
TCID50, 4 to 8 |
||||
|
CHIKV |
MVA-6KE1, MVA-E3E2, MVA-6KE1E3E2 |
CHIKV S27 |
AG129 mice, 7 week old |
5 × 106 TCID50 |
i.m. into the quadriceps muscles of the left leg |
Two doses (3 weeks apart) |
103 TCID50 CHIKV-S27 and CHIKV-IND/NL10, 63 dpim |
i.p. |
NT100, 10 to 160 |
[206] |
|
EEEV, VEEV, and WEEV |
MVA-BN-E/V/W (monovalent) MVA-BN-E + MVA-BN-V + MVA-BN-W (triple mixture of monovalent vaccines) MVA-BN-WEV (trivalent) |
WEEV 71 V-1658, EEEV FL93-939NA and VEEV TrD |
BALB/c mice, age not specified |
108 TCID50 |
s.c. or i.m. |
Two doses (28 days apart) |
5 × 103 or 104 PFU of WEEV Fleming, EEEV PE6, or VEEV TrD, 14 days post booster |
i.n. |
NT50, ~750 to 3800 (monovalent), ~<60 to 340 (triple mixture of monovalent vaccines) and ~<60 to 380 (trivalent) |
[207] |
|
Adenovirus-based chimeras |
||||||||||
|
CHIKV |
CAdVax-CHIK |
LR2006 OPY1 |
CD-1 or C57BL/6, 6 to 8 week old |
108 IU |
i.p. |
Single dose |
104 CCID50 LR2006 OPY1 or QIMR, 6.5 wpim |
s.c. into side of each hind foot towards the ankle |
NT100, ~2000 |
[208] |
|
CHIKV |
ChAdOx1 Chik |
NA |
BALB/c, 6 to 8 week old |
108 IU |
i.m. |
Single dose |
ND |
ND |
NT50, 5.39 × 103 |
|
|
AG129, 5 week old |
108 IU |
i.m. in each leg |
Single dose |
9.7 × 104 PFU LR2006 OPY1, 30 dpim |
i.d. into the left foot |
ND |
||||
|
ChAdOx1 Chik ChAdOx1 Chik ΔCap |
AG129, 5 week old |
108 IU |
i.m. in each hind leg |
Single dose |
9.7 × 104 PFU of LR2006 OPY1, 30 dpim |
i.d. into the left foot towards the ankle |
PRNT80, 32 to 64 (Chik), 16 to 32 (Chik ΔCap) |
[211] |
||
|
CHIK001 (in clinical trials) |
Human clinical trial, Phase 1 |
5 × 109, 2.5 × 1010 or 5 × 1010 vp |
i.m. |
Single dose |
ND |
ND |
ND |
[212] |
||
|
MAYV |
ChAdOx1 May |
NA |
AG129, 5 week old |
1.6 × 104 PFU |
i.m. in each leg |
Single dose |
1.6 × 104 PFU MAYV-CH, 30 dpim |
i.d. into the left foot |
PRNT50, 160 to 620 |
[210] |
|
VEEV |
Rad/VEEV#3 |
VEEV IAB TC-83 |
BALB/c, 6 to 8 week old |
107 PFU |
i.n. |
Three doses (at 0, 7 and 21 days) |
Dose ND, 28 dpim |
aerosol |
PRNT50 (NP) |
[213] |
|
BALB/c, 6 to 8 week old |
107 PFU |
i.n. |
Two doses (at 0, 21 days) |
5000 LD50 TrD, 42 dpim |
aerosol |
ND |
[214] |
|||
|
WEEV |
Ad5-WEEV |
WEEV 71V-1658 |
BALB/c mice, age not specified |
107 PFU |
i.m. |
Single or two doses (at 4 weeks) |
1.5 × 103 PFU Fleming or 71V-1658, 13 wpim |
i.n. |
PRNT50, 160 |
[215] |
|
WEEV |
Ad5-E1 |
WEEV 71V-1658 |
BALB/c mice, 6 to 9 week old |
107 PFU |
i.m. in both leg |
Single dose |
50 LD50 of 71V-1658, 7 dpim, or 400 LD50 CBA87, 1, 3, 5 or 7 dpim |
i.n. |
PRNT50, <10 |
[216] |
|
Vesiculovirus-based chimeras |
||||||||||
|
CHIKV |
rVSVΔG-CHIKV |
CHIKV S27 |
C57BL/6, 3 week old |
106 PFU |
i.m. into the right hind leg muscle |
Single dose |
104 PFU LR 2006 OPY1, 30 dpim |
s.c. in the left rear footpad |
PRNT80, 80 to 640 |
[217] |
|
VEEV |
rVSIV-VEEV |
VEEV ZPC738 |
CD-1, 4 to 6 week old |
108/107 PFU |
i.m. |
Single dose |
104 PFU VEEV ZPC738, 35 or 245 dpim |
s.c. |
PRNT80, 288 to 600 at 25 and 35 dpim, 304 to 360 at 245 dpim |
[218] |
|
VEEV |
rISFV-VEEV |
VEEV ZPC738 |
CD-1, 4 to 6 week old |
108 PFU |
i.m. |
Single dose |
104 PFU VEEV ZPC738, 28 dpim |
s.c. |
PRNT80, ≥20 |
|
|
CD-1, 4 to 6 week old |
108 PFU |
i.m. |
Single dose |
104 PFU VEEV ZPC738, 35 or 245 dpim |
s.c. |
PRNT80, 40 to 160 at 25 and 35 dpim, 25 to 64 at 245 dpim |
||||
|
EEEV |
rISFV-EEEV |
EEEV FL93-939 |
CD-1, 4 to 6 week old |
108 PFU |
i.m. |
Single dose |
104 PFU EEEV FL93-939, 28 dpim |
s.c. |
PRNT80, ≥20 |
|
|
Epitope-based |
||||||||||
|
CHIKV |
E2EP3 |
NA |
C57BL/6 mice, 3 week old |
100 μg (50 μg for booster doses) |
s.c. in the abdominal flank |
Three doses (0, 14 and 21 days) |
106 PFU CHIKV SGP11, 30 dpim |
s.c. region at the ventral side of the right hind footpad, towards the ankle |
~40% reduction from mock control |
[23] |
1 s.c., subcutaneous; i.v., intravenous; i.m., intramuscular; i.d., intradermal; i.p., intraperitoneal; i.n., intranasal; i.t./i.s., intrathalamic/ intraspinal; i.pl., intraplantar; i.c., intracranial; dpim, days post immunization; wpim, weeks post immunization; mpim, months post immunization; IRES, internal ribosome entry site; PFU, plaque forming units; TCID50, 50% tissue culture infective dose; CCID50, 50% cell culture infectious dose; IC50, 50% inhibitory concentration; GE, genomic equivalents; IU, infectious units; AID50, 50% animal infectious dose; PRNT50, 50% plaque reduction neutralizing antibody titer; PRNT80, 80% plaque reduction neutralizing antibody titer; PRNT90, 90% plaque reduction neutralizing antibody titer; LD50, median lethal dose; NT50, 50% neutralizing titer; GMT, geometric mean titer; μNT, neutralizing titer; SIN, Sindbis virus; ISFV, Isfahan virus; May, Mayaro virus; EILV, Eilat virus, VSV/VSIV, vesicular stomatitis virus; MV, measles virus; MVA, modified vaccinia virus Ankara; NP, not provided; NA, not applicable; WT, wild type. Data curated from literature reported through February 2021.
References
- Atkins, G.J. The Pathogenesis of Alphaviruses. ISRN Virol. 2013, 2013, 22.
- Zaid, A.; Burt, F.J.; Liu, X.; Poo, Y.S.; Zandi, K.; Suhrbier, A.; Weaver, S.; Texeira, M.; Mahalingam, S. Arthritogenic alphaviruses: Epidemiological and clinical perspective on emerging arboviruses. Lancet Infect. Dis. 2020.
- Suhrbier, A.; Jaffar-Bandjee, M.C.; Gasque, P. Arthritogenic alphaviruses—An overview. Nat. Rev. Rheumatol. 2012, 8, 420–429.
- Zacks, M.A.; Paessler, S. Encephalitic alphaviruses. Vet. Microbiol. 2010, 140, 281–286.
- Wahid, B.; Ali, A.; Rafique, S.; Idrees, M. Global expansion of chikungunya virus: Mapping the 64-year history. Int. J. Infect. Dis. 2017, 58, 69–76.
- Haddow, A.; Davies, C.W.; Walker, A.J. O’nyong-nyong fever: An epidemic virus disease in East Africa 1. Introduction. Trans. R. Soc. Trop. Med. Hyg. 1960, 54, 517–522.
- Bessaud, M.; Peyrefitte, C.N.; Pastorino, B.A.; Tock, F.; Merle, O.; Colpart, J.J.; Dehecq, J.S.; Girod, R.; Jaffar-Bandjee, M.C.; Glass, P. J.; et al. Chikungunya virus strains, Reunion Island outbreak. Emerg. Infect. Dis. 2006, 12, 1604–1606.
- Aaskov, J.G.; Mataika, J.U.; Lawrence, G.W.; Rabukawaqa, V.; Tucker, M.M.; Miles, J.A.; Dalglish, D.A. An epidemic of Ross River virus infection in Fiji, 1979. Am. J. Trop. Med. Hyg. 1981, 30, 1053–1059.
- Tsetsarkin, K.A.; Vanlandingham, D.L.; McGee, C.E.; Higgs, S. A single mutation in chikungunya virus affects vector specificity and epidemic potential. PLoS Pathog. 2007, 3, e201.
- Tsetsarkin, K.A.; McGee, C.E.; Volk, S.M.; Vanlandingham, D.L.; Weaver, S.C.; Higgs, S. Epistatic roles of E2 glycoprotein mutations in adaption of chikungunya virus to Aedes albopictus and Ae. aegypti mosquitoes. PLoS ONE 2009, 4, e6835.
- Rezza, G.; Chen, R.; Weaver, S.C. O’nyong-nyong fever: A neglected mosquito-borne viral disease. Pathog. Glob. Health 2017, 111, 271–275.
- Acosta-Ampudia, Y.; Monsalve, D.M.; Rodriguez, Y.; Pacheco, Y.; Anaya, J.M.; Ramirez-Santana, C. Mayaro: An emerging viral threat? Emerg. Microbe. Infect. 2018, 7, 163.
- Ganjian, N.; Riviere-Cinnamond, A. Mayaro virus in Latin America and the Caribbean. Rev. Panam. Salud. Publica 2020, 44, 14.
- Pezzi, L.; LaBeaud, A.D.; Reusken, C.B.; Drexler, J.F.; Vasilakis, N.; Diallo, M.; Simon, F.; Jaenisch, T.; Gallian, P.; Sall, A.; et al. GloPID-R report on chikungunya, o’nyong-nyong and Mayaro virus, part 2: Epidemiological distribution of o’nyong-nyong virus. Antivir. Res. 2019, 172, 104611.
- Pezzi, L.; Rodriguez-Morales, A.J.; Reusken, C.B.; Ribeiro, G.S.; LaBeaud, A.D.; Lourenço-de-Oliveira, R.; Brasil, P.; Lecuit, M.; Failloux, A.B.; Gallian, P.; et al. GloPID-R report on chikungunya, o’nyong-nyong and Mayaro virus, part 3: Epidemiological distribution of Mayaro virus. Antivir. Res. 2019, 172, 104610.
- Pezzi, L.; Reusken, C.B.; Weaver, S.C.; Drexler, J.F.; Busch, M.; LaBeaud, A.D.; Diamond, M. S.; Vasilakis, N.; Drebot, M. A.; Siqueira, A.M.; et al. GloPID-R report on Chikungunya, O’nyong-nyong and Mayaro virus, part I: Biological diagnostics. Antivir. Res. 2019, 166, 66–81.
- Seyler, T.; Hutin, Y.; Ramanchandran, V.; Ramakrishnan, R.; Manickam, P.; Murhekar, M. Estimating the burden of disease and the economic cost attributable to chikungunya, Andhra Pradesh, India, 2005–2006. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 133–138.
- Alvis-Zakzuk, N.J.; Diaz-Jimenez, D.; Castillo-Rodriguez, L.; Castaneda-Orjuela, C.; Paternina-Caicedo, A.; Pinzon-Redondo, H.; Carrasquilla-Sotomayor, M.; Alvis-Guzmán, N.; De La Hoz-Restrepo, F. Economic Costs of Chikungunya Virus in Colombia. Value Health Reg. Issues 2018, 17, 32–37.
- Thompson, R.; del Martin Campo, J.; Constenla, D. A review of the economic evidence of Aedes-borne arboviruses and Aedes-borne arboviral disease prevention and control strategies. Expert Rev. Vaccin. 2020, 19, 143–162.
- Cunha, R.V.D.; Trinta, K.S. Chikungunya virus: Clinical aspects and treatment—A Review. Mem. Inst. Oswaldo Cruz 2017, 112, 523–531.
- Lundstrom, K. Alphavirus-based vaccines. Viruses 2014, 6, 2392–2415.
- Panning, M.; Grywna, K.; van Esbroeck, M.; Emmerich, P.; Drosten, C. Chikungunya fever in travelers returning to Europe from the Indian Ocean region, 2006. Emerg. Infect. Dis. 2008, 14, 416–422.
- Kam, Y.W.; Lum, F.M.; Teo, T.H.; Lee, W.W.; Simarmata, D.; Harjanto, S.; Chua, C.L.; Chan, Y.F.; Wee, J.K.; Chow, A.; et al. Early neutralizing IgG response to Chikungunya virus in infected patients targets a dominant linear epitope on the E2 glycoprotein. EMBO Mol. Med. 2012, 4, 330–343.
- Pierro, A.; Rossini, G.; Gaibani, P.; Finarelli, A.C.; Moro, M.L.; Landini, M.P.; Sambri, V. Persistence of anti-chikungunya virus-specific antibodies in a cohort of patients followed from the acute phase of infection after the 2007 outbreak in Italy. New Microbe. New Infect. 2015, 7, 23–25.
- Chua, C.L.; Sam, I.C.; Chiam, C.W.; Chan, Y.F. The neutralizing role of IgM during early Chikungunya virus infection. PLoS ONE 2017, 12, e0171989.
- Borgherini, G.; Poubeau, P.; Staikowsky, F.; Lory, M.; Le Moullec, N.; Becquart, J.P.; Wengling, C.; Michault, A.; Paganin, F. Outbreak of chikungunya on Reunion Island: Early clinical and laboratory features in 157 adult patients. Clin. Infect. Dis. 2007, 44, 1401–1407.
- Malvy, D.; Ezzedine, K.; Mamani-Matsuda, M.; Autran, B.; Tolou, H.; Receveur, M-C.; Pistone, T.; Rambert, J.; Moynet, D.; Mossalayi, D. Destructive arthritis in a patient with chikungunya virus infection with persistent specific IgM antibodies. BMC Infect. Dis. 2009, 9, 200.
- Bozza, F.A.; Moreira-Soto, A.; Rockstroh, A.; Fischer, C.; Nascimento, A.D.; Calheiros, A.S.; Drosten, C.; Bozza, P.T.; Souza, T.; Ulbert, S.; et al. Differential Shedding and Antibody Kinetics of Zika and Chikungunya Viruses, Brazil. Emerg. Infect. Dis. 2019, 25, 311–315.
- Nitatpattana, N.; Kanjanopas, K.; Yoksan, S.; Satimai, W.; Vongba, N.; Langdatsuwan, S.; Nakgoi, K.; Ratchakum, S.; Wauquier, N.; Souris, M.; et al. Long-term persistence of Chikungunya virus neutralizing antibodies in human populations of North Eastern Thailand. Virol. J. 2014, 11, 183.
- Shore, H. O’nyong-nyong fever: An epidemic virus disease in East Africa: III Some clinical and epidemiological observations in the Northern Province of Uganda. Trans. R. Soc. Trop. Med. Hyg. 1961, 55, 361–373.
- Williams, M.C.; Woodall, J.P.; Corbet, P.S.; Gillett, J.D. O’nyong-Nyong Fever: An Epidemic Virus Disease in East Africa. 8. Virus Isolations from Anopheles Mosquitoes. Trans. R. Soc. Trop. Med. Hyg. 1965, 59, 300–306.
- Kiwanuka, N.; Sanders, E.J.; Rwaguma, E.B.; Kawamata, J.; Ssengooba, F.P.; Najjemba, R.; Were, W.A.; Lamunu, M.; Bagambisa, G.; Burkot, T.R.; et al. O’nyong-nyong fever in south-central Uganda, 1996–1997: Clinical features and validation of a clinical case definition for surveillance purposes. Clin. Infect. Dis. 1999, 29, 1243–1250.
- Tappe, D.; Kapaun, A.; Emmerich, P.; de Mendonca Campos, R.; Cadar, D.; Gunther, S.; Schmidt-Chanasit, J. O’nyong-nyong virus infection imported to Europe from Kenya by a traveler. Emerg. Infect. Dis. 2014, 20, 1766–1767.
- Bessaud, M.; Peyrefitte, C.N.; Pastorino, B.A.; Gravier, P.; Tock, F.; Boete, F.; Tolou, H.J.; Grandadam, M. O’nyong-nyong Virus, Chad. Emerg. Infect. Dis. 2006, 12, 1248–1250.
- Diagne, C.T.; Bengue, M.; Choumet, V.; Hamel, R.; Pompon, J.; Misse, D. Mayaro Virus Pathogenesis and Transmission Mechanisms. Pathogens 2020, 9, 738.
- Mourao, M.P.; Bastos, M.D.S.; de Figueiredo, R.P.; Gimaque, J.B.; Galusso Edos, S.; Kramer, V.M.; de Oliveira, C.M.; Naveca, F.G.; Figueiredo, L.T. Mayaro fever in the city of Manaus, Brazil, 2007–2008. Vector Borne Zoonotic Dis. 2012, 12, 42–46.
- Halsey, E.S.; Siles, C.; Guevara, C.; Vilcarromero, S.; Jhonston, E.J.; Ramal, C.; Aguilar, P.V.; Ampuero, J.S. Mayaro virus infection, Amazon Basin region, Peru, 2010–2013. Emerg. Infect. Dis. 2013, 19, 1839–1842.
- Figueiredo, L.T.; Nogueira, R.M.; Cavalcanti, S.M.; Schatzmayr, H.; da Rosa, A.T. Study of two different enzyme immunoassays for the detection of Mayaro virus antibodies. Mem. Inst. Oswaldo Cruz 1989, 84, 303–307.
- Santiago, F.W.; Halsey, E.S.; Siles, C.; Vilcarromero, S.; Guevara, C.; Silvas, J.A.; Ramal, C.; Ampuero, J.S.; Aguilar, P.V. Long-Term Arthralgia after Mayaro Virus Infection Correlates with Sustained Pro-inflammatory Cytokine Response. PLoS Negl. Trop. Dis. 2015, 9, e0004104.
- Harley, D.; Sleigh, A.; Ritchie, S. Ross River virus transmission, infection, and disease: A cross-disciplinary review. Clin. Microbiol. Rev. 2001, 14, 909–932.
- Farmer, J.F.; Suhrbier, A. Interpreting paired serology for Ross River virus and Barmah Forest virus diseases. Aust. J. Gen. Pract. 2019, 48, 645–649.
- Barton, A.J.; Bielefeldt-Ohmann, H. Clinical Presentation, Progression, and Management of Five Cases of Ross River Virus Infection in Performance Horses Located in Southeast Queensland: A Longitudinal Case Series. J. Equin. Vet. Sci. 2017, 51, 34–40.
- Azuolas, J.K.; Wishart, E.; Bibby, S.; Ainsworth, C. Isolation of Ross River virus from mosquitoes and from horses with signs of musculo-skeletal disease. Aust. Vet. J. 2003, 81, 344–347.
- Kapeleris, J.; Lowe, P.; Phillips, D.; Wyatt, D.; Batham, M.; Devine, P. IgG avidity in the diagnosis of acute Ross River virus infection. Dis. Marker. 1996, 12, 279–282.
- Calisher, C.H.; Meurman, O.; Brummer-Korvenkontio, M.; Halonen, P.E.; Muth, D.J. Sensitive enzyme immunoassay for detecting immunoglobulin M antibodies to Sindbis virus and further evidence that Pogosta disease is caused by a western equine encephalitis complex virus. J. Clin. Microbiol. 1985, 22, 566–571.
- Kurkela, S.; Manni, T.; Myllynen, J.; Vaheri, A.; Vapalahti, O. Clinical and laboratory manifestations of Sindbis virus infection: Prospective study, Finland, 2002–2003. J. Infect. Dis. 2005, 191, 1820–1829.
- Niklasson, B.; Espmark, A.; Lundstrom, J. Occurrence of arthralgia and specific IgM antibodies three to four years after Ockelbo disease. J. Infect. Dis. 1988, 157, 832–835.
- Griffin, D.E. Neurotropic Alphaviruses. In Neurotropic Viral Infections, 2nd ed.; Reis, C.S., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 175–204.
- Calisher, C.H.; Berardi, V.P.; Muth, D.J.; Buff, E.E. Specificity of immunoglobulin M and G antibody responses in humans infected with eastern and western equine encephalitis viruses: Application to rapid serodiagnosis. J. Clin. Microbiol. 1986, 23, 369–372.
- Gardner, J.; Anraku, I.; Le, T.T.; Larcher, T.; Major, L.; Roques, P.; Schroder, W.A.; Higgs, S.; Suhrbier, A. Chikungunya virus arthritis in adult wild-type mice. J. Virol. 2010, 84, 8021–8032.
- Poo, Y.S.; Rudd, P.A.; Gardner, J.; Wilson, J.A.; Larcher, T.; Colle, M.A.; Le, T.T.; Nakaya, H.I.; Warrilow, D.; Allcock, R.; et al. Multiple immune factors are involved in controlling acute and chronic chikungunya virus infection. PLoS Negl. Trop. Dis. 2014, 8, e3354.
- Hawman, D.W.; Stoermer, K.A.; Montgomery, S.A.; Pal, P.; Oko, L.; Diamond, M.S.; Morrison, T.E. Chronic joint disease caused by persistent Chikungunya virus infection is controlled by the adaptive immune response. J. Virol. 2013, 87, 13878–13888.
- Johnson, R.T. Virus Invasion of the Central Nervous System: A Study of Sindbis Virus Infection in the Mouse Using Fluorescent Antibody. Am. J. Pathol. 1965, 46, 929–943.
- Burdeinick-Kerr, R.; Wind, J.; Griffin, D.E. Synergistic roles of antibody and interferon in noncytolytic clearance of Sindbis virus from different regions of the central nervous system. J. Virol. 2007, 81, 5628–5636.
- Nilaratanakul, V.; Chen, J.; Tran, O.; Baxter, V.K.; Troisi, E.M.; Yeh, J.X.; Griffin, D.E. Germ Line IgM Is Sufficient, but Not Required, for Antibody-Mediated Alphavirus Clearance from the Central Nervous System. J. Virol. 2018, 92, e02081-17.
- Fragkoudis, R.; Ballany, C.M.; Boyd, A.; Fazakerley, J.K. In Semliki Forest virus encephalitis, antibody rapidly clears infectious virus and is required to eliminate viral material from the brain, but is not required to generate lesions of demyelination. J. Gen. Virol. 2008, 89, 2565–2568.
- Amor, S.; Scallan, M.F.; Morris, M.M.; Dyson, H.; Fazakerley, J.K. Role of immune responses in protection and pathogenesis during Semliki Forest virus encephalitis. J. Gen. Virol. 1996, 77, 281–291.
- Fazakerley, J.K.; Webb, H.E. Semliki Forest virus-induced, immune-mediated demyelination: Adoptive transfer studies and viral persistence in nude mice. J. Gen. Virol. 1987, 68, 377–385.
- Metcalf, T.U.; Baxter, V.K.; Nilaratanakul, V.; Griffin, D.E. Recruitment and retention of B cells in the central nervous system in response to alphavirus encephalomyelitis. J. Virol. 2013, 87, 2420–2429.
- Metcalf, T.U.; Griffin, D.E. Alphavirus-induced encephalomyelitis: Antibody-secreting cells and viral clearance from the nervous system. J. Virol. 2011, 85, 11490–11501.
- Teo, T.H.; Lum, F.M.; Claser, C.; Lulla, V.; Lulla, A.; Merits, A.; Renia, L.; Ng, L. F. A pathogenic role for CD4+ T cells during Chikungunya virus infection in mice. J. Immunol. 2013, 190, 259–269.
- Lum, F.M.; Teo, T.H.; Lee, W.W.; Kam, Y.W.; Renia, L.; Ng, L.F. An essential role of antibodies in the control of Chikungunya virus infection. J. Immunol. 2013, 190, 6295–6302.
- Olitsky, P.K.; Cox, H.R. Active Immunication of Guinea Pigs with the Virus of Equine Encephalomyelitis: I. Quantitative Experiments with Various Preparations of Active Virus. J. Exp. Med. 1936, 63, 311–324.
- Cox, H.R.; Olitsky, P.K. Active Immunization of Guinea Pigs with the Virus of Equine Encephalomyelitis: Iii. Quantitative Studies of Serum Antiviral Bodies in Animals Immunized with Active and Inactive Virus. J. Exp. Med. 1936, 64, 217–222.
- Cox, H.R.; Olitsky, P.K. Active Immunization of Guinea Pigs with the Virus of Equine Encephalomyelitis: Iv. Effect of Immune Serum on Antigenicity of Active and Inactive Virus. J. Exp. Med. 1936, 64, 223–232.
- Olitsky, P.K.; Harford, C.G. Intraperitoneal and Intracerebral Routes in Serum Protection Tests with the Virus of Equine Encephalomyelitis: Iii. Comparison of Antiviral Serum Constituents from Guinea Pigs Immunized with Active or Formolized Inactive Virus. J. Exp. Med. 1938, 68, 779–787.
- Morgan, I.M.; Schlesinger, R.W.; Olitsky, P.K. Induced Resistance of the Central Nervous System to Experimental Infection with Equine Encephalomyelitis Virus: I. Neutralizing Antibody in the Central Nervous System in Relation to Cerebral Resistance. J. Exp. Med. 1942, 76, 357–369.
- Griffin, D.E.; Johnson, R.T. Role of the immune response in recovery from Sindbis virus encephalitis in mice. J. Immunol. 1977, 118, 1070–1075.
- Kimura, T.; Griffin, D.E. Extensive immune-mediated hippocampal damage in mice surviving infection with neuroadapted Sindbis virus. Virology 2003, 311, 28–39.
- Rabinowitz, S.G.; Adler, W.H. Host defenses during primary Venezuelan equine encephalomyelitis virus infection in mice. I. Passive transfer of protection with immune serum and immune cells. J. Immunol. 1973, 110, 1345–1353.
- Couderc, T.; Khandoudi, N.; Grandadam, M.; Visse, C.; Gangneux, N.; Bagot, S.; Prost, J. F.; Lecuit, M. Prophylaxis and therapy for Chikungunya virus infection. J. Infect. Dis. 2009, 200, 516–523.
- Lee, C.Y.; Kam, Y.W.; Fric, J.; Malleret, B.; Koh, E.G.; Prakash, C.; Huang, W.; Lee, W. W.; Lin, C.; Lin, R. T. Chikungunya virus neutralization antigens and direct cell-to-cell transmission are revealed by human antibody-escape mutants. PLoS Pathog. 2011, 7, e1002390.
- Holzer, G.W.; Coulibaly, S.; Aichinger, G.; Savidis-Dacho, H.; Mayrhofer, J.; Brunner, S.; Schmid, K.; Kistner, O.; Aaskov, J. G.; Falkner, F.G.; et al. Evaluation of an inactivated Ross River virus vaccine in active and passive mouse immunization models and establishment of a correlate of protection. Vaccine 2011, 29, 4132–4141.
- Kraaijeveld, C.A.; Benaissa-Trouw, B.J.; Harmsen, M.; Snippe, H. Adoptive transfer of immunity against virulent Semliki Forest virus with immune spleen cells from mice infected with avirulent Semliki Forest virus. Arch. Virol. 1986, 91, 83–92.
- Jose, J.; Snyder, J.E.; Kuhn, R.J. A structural and functional perspective of alphavirus replication and assembly. Future Microbiol. 2009, 4, 837–856.
- Stec, D.S.; Waddell, A.; Schmaljohn, C.S.; Cole, G.A.; Schmaljohn, A.L. Antibody-selected variation and reversion in Sindbis virus neutralization epitopes. J. Virol. 1986, 57, 715–720.
- Boere, W.A.; Harmsen, T.; Vinje, J.; Benaissa-Trouw, B.J.; Kraaijeveld, C.A.; Snippe, H. Identification of distinct antigenic determinants on Semliki Forest virus by using monoclonal antibodies with different antiviral activities. J. Virol. 1984, 52, 575–582.
- Roehrig, J.T.; Mathews, J.H. The neutralization site on the E2 glycoprotein of Venezuelan equine encephalomyelitis (TC-83) virus is composed of multiple conformationally stable epitopes. Virology 1985, 142, 347–356.
- Vrati, S.; Fernon, C.A.; Dalgarno, L.; Weir, R.C. Location of a major antigenic site involved in Ross River virus neutralization. Virology 1988, 162, 346–353.
- Navaratnarajah, C.K.; Kuhn, R.J. Functional characterization of the Sindbis virus E2 glycoprotein by transposon linker-insertion mutagenesis. Virology 2007, 363, 134–147.
- Hunt, A.R.; Frederickson, S.; Maruyama, T.; Roehrig, J.T.; Blair, C.D. The first human epitope map of the alphaviral E1 and E2 proteins reveals a new E2 epitope with significant virus neutralizing activity. PLoS Negl. Trop. Dis. 2010, 4, e739.
- Kam, Y.W.; Lee, W.W.; Simarmata, D.; Le Grand, R.; Tolou, H.; Merits, A.; Roques, P.; Ng, L. F. Unique epitopes recognized by antibodies induced in Chikungunya virus-infected non-human primates: Implications for the study of immunopathology and vaccine development. PLoS ONE 2014, 9, e95647.
- Adouchief, S.; Smura, T.; Vapalahti, O.; Hepojoki, J. Mapping of human B-cell epitopes of Sindbis virus. J. Gen. Virol. 2016, 97, 2243–2254.
- Chanas, A.C.; Gould, E.A.; Clegg, J.C.; Varma, M.G. Monoclonal antibodies to Sindbis virus glycoprotein E1 can neutralize, enhance infectivity, and independently inhibit haemagglutination or haemolysis. J. Gen. Virol. 1982, 58, 37–46.
- Despres, P.; Griffin, J.W.; Griffin, D.E. Antiviral activity of alpha interferon in Sindbis virus-infected cells is restored by anti-E2 monoclonal antibody treatment. J. Virol. 1995, 69, 7345–7348.
- Despres, P.; Griffin, J.W.; Griffin, D.E. Effects of anti-E2 monoclonal antibody on sindbis virus replication in AT3 cells expressing bcl-2. J. Virol. 1995, 69, 7006–7014.
- Mendoza, Q.P.; Stanley, J.; Griffin, D.E. Monoclonal antibodies to the E1 and E2 glycoproteins of Sindbis virus: Definition of epitopes and efficiency of protection from fatal encephalitis. J. Gen. Virol. 1988, 69, 3015–3022.
- Stanley, J.; Cooper, S.J.; Griffin, D.E. Monoclonal antibody cure and prophylaxis of lethal Sindbis virus encephalitis in mice. J. Virol. 1986, 58, 107–115.
- Boere, W.A.; Benaissa-Trouw, B.J.; Harmsen, T.; Erich, T.; Kraaijeveld, C.A.; Snippe, H. Mechanisms of monoclonal antibody-mediated protection against virulent Semliki Forest virus. J. Virol. 1985, 54, 546–551.
- Smith, S.A.; Silva, L.A.; Fox, J.M.; Flyak, A.I.; Kose, N.; Sapparapu, G.; Khomandiak, S.; Ashbrook, A. W.; Kahle, K. M.; Fong, R. H; et al. Isolation and Characterization of Broad and Ultrapotent Human Monoclonal Antibodies with Therapeutic Activity against Chikungunya Virus. Cell Host Microbe 2015, 18, 86–95.
- Chua, C.L.; Chan, Y.F.; Sam, I.C. Characterisation of mouse monoclonal antibodies targeting linear epitopes on Chikungunya virus E2 glycoprotein. J. Virol. Method. 2014, 195, 126–133.
- Pal, P.; Dowd, K.A.; Brien, J.D.; Edeling, M.A.; Gorlatov, S.; Johnson, S.; Lee, I.; Akahata, W.; Nabel, G. J.; Richter, M. K.; et al. Development of a highly protective combination monoclonal antibody therapy against Chikungunya virus. PLoS Pathog. 2013, 9, e1003312.
- Goh, L.Y.; Hobson-Peters, J.; Prow, N.A.; Baker, K.; Piyasena, T.B.; Taylor, C.T.; Rana, A.; Hastie, M. L.; Gorman, J. J.; Hall, R. A. The Chikungunya Virus Capsid Protein Contains Linear B Cell Epitopes in the N- and C-Terminal Regions that are Dependent on an Intact C-Terminus for Antibody Recognition. Viruses 2015, 7, 2943–2964.
- Goh, L.Y.H.; Hobson-Peters, J.; Prow, N.A.; Gardner, J.; Bielefeldt-Ohmann, H.; Suhrbier, A.; Hall, R. A. Monoclonal antibodies specific for the capsid protein of chikungunya virus suitable for multiple applications. J. Gen. Virol. 2015, 96, 507–512.
- Sun, S.; Xiang, Y.; Akahata, W.; Holdaway, H.; Pal, P.; Zhang, X.; Diamond, M. S.; Nabel, G. J.; Rossmann, M. G. Structural analyses at pseudo atomic resolution of Chikungunya virus and antibodies show mechanisms of neutralization. eLife 2013, 2, e00435.
- Voss, J.E.; Vaney, M.C.; Duquerroy, S.; Vonrhein, C.; Girard-Blanc, C.; Crublet, E.; Thompson, A.; Bricogne, G.; Rey, F. A. Glycoprotein organization of Chikungunya virus particles revealed by X-ray crystallography. Nature 2010, 468, 709–712.
- Broeckel, R.; Fox, J.M.; Haese, N.; Kreklywich, C.N.; Sukulpovi-Petty, S.; Legasse, A.; Smith, P. P.; Denton, M.; Corvey, C.; Krishnan, S.; et al. Therapeutic administration of a recombinant human monoclonal antibody reduces the severity of chikungunya virus disease in rhesus macaques. PLoS Negl. Trop. Dis. 2017, 11, e0005637.
- Fox, J.M.; Long, F.; Edeling, M.A.; Lin, H.; van Duijl-Richter, M.K.S.; Fong, R.H.; Kahle, K. M.; Smit, J. M.; Jin, J.; Simmons, G.; et al. Broadly Neutralizing Alphavirus Antibodies Bind an Epitope on E2 and Inhibit Entry and Egress. Cell 2015, 163, 1095–1107.
- Kim, A.S.; Austin, S.K.; Gardner, C.L.; Zuiani, A.; Reed, D.S.; Trobaugh, D.W.; Sun, C.; Basore, K.; Williamson, L. E.; Crowe, J. E; et al. Protective antibodies against Eastern equine encephalitis virus bind to epitopes in domains A and B of the E2 glycoprotein. Nat. Microbiol. 2019, 4, 187–197.
- Zhao, J.; Sun, E.C.; Liu, N.H.; Yang, T.; Xu, Q.Y.; Qin, Y.L.; Yang, Y. H.; Wu, D. L. Phage display identifies an Eastern equine encephalitis virus glycoprotein E2-specific B cell epitope. Vet. Immunol. Immunopathol. 2012, 148, 364–368.
- Sun, E.C.; Zhao, J.; Yang, T.; Xu, Q.Y.; Qin, Y.L.; Wang, W.S.; Wei, P.; Sun, L.; Sun, J.; Wu, D.L. Analysis of murine B-cell epitopes on Eastern equine encephalitis virus glycoprotein E2. Appl. Microbiol. Biotechnol. 2013, 97, 6359–6372.
- Powell, L.A.; Fox, J.M.; Kose, N.; Kim, A.S.; Majedi, M.; Bombardi, R.; Carnahan, R. H.; Slaughter, J. C.; Morrison, T. E.; Diamond, M.; et al. Human monoclonal antibodies against Ross River virus target epitopes within the E2 protein and protect against disease. PLoS Pathog. 2020, 16, e1008517.
- Earnest, J.T.; Basore, K.; Roy, V.; Bailey, A.L.; Wang, D.; Alter, G.; Fremont, D. H.; Diamond, M. S. Neutralizing antibodies against Mayaro virus require Fc effector functions for protective activity. J. Exp. Med. 2019, 216, 2282–2301.
- Zhang, R.; Kim, A.S.; Fox, J.M.; Nair, S.; Basore, K.; Klimstra, W.B.; Rimkunas, R.; Fong, R. H.; Lin, H.; Poddar, S.; et al. Mxra8 is a receptor for multiple arthritogenic alphaviruses. Nature 2018, 557, 570–574.
- Zhang, R.; Earnest, J.T.; Kim, A.S.; Winkler, E.S.; Desai, P.; Adams, L.J.; Hu, G.; Bullock, C.; Gold, B.; Cherry, S.; et al. Expression of the Mxra8 Receptor Promotes Alphavirus Infection and Pathogenesis in Mice and Drosophila. Cell Rep. 2019, 28, 2647–2658.e5.
- Basore, K.; Kim, A.S.; Nelson, C.A.; Zhang, R.; Smith, B.K.; Uranga, C.; Vang, L.; Cheng, M.; Gross, M. L.; Smith, J.; et al. Cryo-EM Structure of Chikungunya Virus in Complex with the Mxra8 Receptor. Cell 2019, 177, 1725–1737.e16.
- Song, H.; Zhao, Z.; Chai, Y.; Jin, X.; Li, C.; Yuan, F.; Liu, S.; Gao, Z.; Wang, H.; Song, J.; et al. Molecular Basis of Arthritogenic Alphavirus Receptor MXRA8 Binding to Chikungunya Virus Envelope Protein. Cell 2019, 177, 1714–1724.e12.
- Gould, E.; Pettersson, J.; Higgs, S.; Charrel, R.; de Lamballerie, X. Emerging arboviruses: Why today? One Health 2017, 4, 1–13.
- Weaver, S.C. Urbanization and geographic expansion of zoonotic arboviral diseases: Mechanisms and potential strategies for prevention. Trends Microbiol. 2013, 21, 360–363.
- Zahouli, J.B.Z.; Koudou, B.G.; Muller, P.; Malone, D.; Tano, Y.; Utzinger, J. Urbanization is a main driver for the larval ecology of Aedes mosquitoes in arbovirus-endemic settings in south-eastern Cote d’Ivoire. PLoS Negl. Trop. Dis. 2017, 11, e0005751.
- Kilpatrick, A.M.; Randolph, S.E. Drivers, dynamics, and control of emerging vector-borne zoonotic diseases. Lancet 2012, 380, 1946–1955.
- Vazeille, M.; Moutailler, S.; Pages, F.; Jarjaval, F.; Failloux, A.B. Introduction of Aedes albopictus in Gabon: What consequences for dengue and chikungunya transmission? Trop. Med. Int. Health 2008, 13, 1176–1179.
- Naish, S.; Hu, W.; Mengersen, K.; Tong, S. Spatio-temporal patterns of Barmah Forest virus disease in Queensland, Australia. PLoS ONE 2011, 6, e25688.
- Reed, D.S.; Glass, P.J.; Bakken, R.R.; Barth, J.F.; Lind, C.M.; da Silva, L.; Hart, M.K.; Rayner, J.; Alterson, K.; Custer, M.; et al. Combined alphavirus replicon particle vaccine induces durable and cross-protective immune responses against equine encephalitis viruses. J. Virol. 2014, 88, 12077–12086.
- Wressnigg, N.; van der Velden, M.V.; Portsmouth, D.; Draxler, W.; O’Rourke, M.; Richmond, P.; Hall, S.; McBride, W.J.H.; Redfern, A.; Aaskvo, J.; et al. An inactivated Ross River virus vaccine is well tolerated and immunogenic in an adult population in a randomized phase 3 trial. Clin. Vaccine Immunol. 2015, 22, 267–273.
- Chang, L.J.; Dowd, K.A.; Mendoza, F.H.; Saunders, J.G.; Sitar, S.; Plummer, S.H.; Yamshchikov, G.; Sarwar, U.N.; Hu, Z.; Enama, M.E.; et al. Safety and tolerability of chikungunya virus-like particle vaccine in healthy adults: A phase 1 dose-escalation trial. Lancet 2014, 384, 2046–2052.
- Chen, G.L.; Coates, E.E.; Plummer, S.H.; Carter, C.A.; Berkowitz, N.; Conan-Cibotti, M.; Cox, J.H.; Beck, A.; O’Callahan, M.; Andrews, C.; et al. Effect of a Chikungunya Virus-Like Particle Vaccine on Safety and Tolerability Outcomes: A Randomized Clinical Trial. JAMA 2020, 323, 1369–1377.
- Akahata, W.; Nabel, G.J. A specific domain of the Chikungunya virus E2 protein regulates particle formation in human cells: Implications for alphavirus vaccine design. J. Virol. 2012, 86, 8879–8883.
- Chen, R.; Puri, V.; Fedorova, N.; Lin, D.; Hari, K.L.; Jain, R.; Rodas, J.D.; Das, S.R.; Shabman, R.S.; Weaver, S.C. Comprehensive Genome Scale Phylogenetic Study Provides New Insights on the Global Expansion of Chikungunya Virus. J. Virol. 2016, 90, 10600–10611.
- Xavier, J.; Fonseca, V.; Bezerra, J.F.; do Monte Alves, M.; Mares-Guia, M.A.; Claro, I.M.; de Jesus, R.; Adelino, T.; Araújo, E.; Cavalcante, K.R.L.J; et al. Chikungunya virus ECSA lineage reintroduction in the northeasternmost region of Brazil. Int. J. Infect. Dis. 2021, 105, 120–123.
- Phadungsombat, J.; Imad, H.; Rahman, M.; Nakayama, E.E.; Kludkleeb, S.; Ponam, T.; Rahim, R.; Hasan, A.; Poltep, K.; Yamanaka, A.; et al. A Novel Sub-Lineage of Chikungunya Virus East/Central/South African Genotype Indian Ocean Lineage Caused Sequential Outbreaks in Bangladesh and Thailand. Viruses 2020, 12, 1319.
- Fabri, A.A.; Rodrigues, C.; Santos, C.C.D.; Chalhoub, F.L.L.; Sampaio, S.A.; Faria, N.; Torres, M.C.; Fonseca, V.; Brasil, P.; Calvet, G.; et al. Co-Circulation of Two Independent Clades and Persistence of CHIKV-ECSA Genotype during Epidemic Waves in Rio de Janeiro, Southeast Brazil. Pathogens 2020, 9, 984.
- Harsha, P.K.; Reddy, V.; Rao, D.; Pattabiraman, C.; Mani, R.S. Continual circulation of ECSA genotype and identification of a novel mutation I317V in the E1 gene of Chikungunya viral strains in southern India during 2015–2016. J. Med. Virol. 2020, 92, 1007–1012.
- Akahata, W.; Yang, Z.Y.; Andersen, H.; Sun, S.; Holdaway, H.A.; Kong, W.P; Lewis, M.G.; Higgs, S.; Rossmann, M.G.; Rao, S.; et al. A virus-like particle vaccine for epidemic Chikungunya virus protects nonhuman primates against infection. Nat. Med. 2010, 16, 334–338.
- Erasmus, J.H.; Seymour, R.L.; Kaelber, J.T.; Kim, D.Y.; Leal, G.; Sherman, M.B.; Frolov, I.; Chiu, W.; Weaver, S.C.; Nasar, F. Novel Insect-Specific Eilat Virus-Based Chimeric Vaccine Candidates Provide Durable, Mono- and Multivalent, Single-Dose Protection against Lethal Alphavirus Challenge. J. Virol. 2018, 92, e01274-17.
- Abeyratne, E.; Tharmarajah, K.; Freitas, J.R.; Mostafavi, H.; Mahalingam, S.; Zaid, A.; Zaman, M.; Taylor, A. Liposomal Delivery of the RNA Genome of a Live-Attenuated Chikungunya Virus Vaccine Candidate Provides Local, but Not Systemic Protection After One Dose. Front. Immunol. 2020, 11, 304.
- Taylor, A.; Liu, X.; Zaid, A.; Goh, L.Y.; Hobson-Peters, J.; Hall, R.A.; Merits, A.; Mahalingam, S. Mutation of the N-Terminal Region of Chikungunya Virus Capsid Protein: Implications for Vaccine Design. mBio 2017, 8, e01970-16.
- Kistner, O.; Barrett, N.; Bruhmann, A.; Reiter, M.; Mundt, W.; Savidis-Dacho, H.; Schober-Bendixen, S.; Dorner, F.; Aaskov, J. The preclinical testing of a formaldehyde inactivated Ross River virus vaccine designed for use in humans. Vaccine 2007, 25, 4845–4852.
- Aichinger, G.; Ehrlich, H.J.; Aaskov, J.G.; Fritsch, S.; Thomasser, C.; Draxler, W.; Wolzt, M.; Muller, M.; Pinl, F.; Van Damme, P.; et al. Safety and immunogenicity of an inactivated whole virus Vero cell-derived Ross River virus vaccine: A randomized trial. Vaccine 2011, 29, 9376–9384.
- Chan, Y.H.; Teo, T.H.; Utt, A.; Tan, J.J.; Amrun, S.N.; Abu Bakar, F.; Yee, W.-X.; Becht, E.; Lee, C.Y.-P.; Lee, B.; et al. Mutating chikungunya virus non-structural protein produces potent live-attenuated vaccine candidate. EMBO Mol. Med. 2019, 11, e10092.
- Hallengard, D.; Kakoulidou, M.; Lulla, A.; Kummerer, B.M.; Johansson, D.X.; Mutso, M.; Lulla, V.; Fazakerley, J.K.; Roques, P.; Le Grand, R.; et al. Novel attenuated Chikungunya vaccine candidates elicit protective immunity in C57BL/6 mice. J. Virol. 2014, 88, 2858–2866.
- Roques, P.; Ljungberg, K.; Kummerer, B.M.; Gosse, L.; Dereuddre-Bosquet, N.; Tchitchek, N.; Hallengard, D.; Garcia-Arriaza, J.; Meinke, A.; Esteban, M.; et al. Attenuated and vectored vaccines protect nonhuman primates against Chikungunya virus. JCI Insight 2017, 2, e83527.
- Wressnigg, N.; Hochreiter, R.; Zoihsl, O.; Fritzer, A.; Bezay, N.; Klingler, A.; Lingnau, K.; Schneider, M.; Lundberg, U.; Meinke, A.; et al. Single-shot live-attenuated chikungunya vaccine in healthy adults: A phase 1, randomised controlled trial. Lancet Infect. Dis. 2020, 20, 1193–1203.
- Carrau, L.; Rezelj, V.V.; Noval, M.G.; Levi, L.I.; Megrian, D.; Blanc, H.; Weger-Lucarelli, J.; Moratorio, G.; Stapleford, K.A.; Vignuzzi, M. Chikungunya Virus Vaccine Candidates with Decreased Mutational Robustness Are Attenuated In Vivo and Have Compromised Transmissibility. J. Virol. 2019, 93, e00775-19.
- Piper, A.; Ribeiro, M.; Smith, K.M.; Briggs, C.M.; Huitt, E.; Nanda, K.; Spears, C.J.; Quiles, M.; Cullen, J.; Thomas, M.E.; et al. Chikungunya virus host range E2 transmembrane deletion mutants induce protective immunity against challenge in C57BL/6J mice. J. Virol. 2013, 87, 6748–6757.
- Gardner, C.L.; Hritz, J.; Sun, C.; Vanlandingham, D.L.; Song, T.Y.; Ghedin, E.; Higgs, S.; Klimstra, W.B.; Ryman, K.D. Deliberate attenuation of chikungunya virus by adaptation to heparan sulfate-dependent infectivity: A model for rational arboviral vaccine design. PLoS Negl. Trop. Dis. 2014, 8, e2719.
- Ludwig, G.V.; Turell, M.J.; Vogel, P.; Kondig, J.P.; Kell, W.K.; Smith, J.F.; Pratt, W.D. Comparative neurovirulence of attenuated and non-attenuated strains of Venezuelan equine encephalitis virus in mice. Am. J. Trop. Med. Hyg. 2001, 64, 49–55.
- Reed, D.S.; Lind, C.M.; Lackemeyer, M.G.; Sullivan, L.J.; Pratt, W.D.; Parker, M.D. Genetically engineered, live, attenuated vaccines protect nonhuman primates against aerosol challenge with a virulent IE strain of Venezuelan equine encephalitis virus. Vaccine 2005, 23, 3139–3147.
- Fine, D.L.; Roberts, B.A.; Terpening, S.J.; Mott, J.; Vasconcelos, D.; House, R.V. Neurovirulence evaluation of Venezuelan equine encephalitis (VEE) vaccine candidate V3526 in nonhuman primates. Vaccine 2008, 26, 3497–3506.
- Main, C.F.D.; Snow, D.; Mallory, R.M.; Helber, S.; Terpening, S.; Holley, H.P. Safety of an Attenuated Venezuelan Equine Encephalitis Virus (VEEV) Vaccine in Humans. In Proceedings of the America Infectious Diseases Society of America 2008 Annual Meeting, Washington, DC, USA, 25–28 October 2008.
- Tretyakova, I.; Tibbens, A.; Jokinen, J.D.; Johnson, D.M.; Lukashevich, I.S.; Pushko, P. Novel DNA-launched Venezuelan equine encephalitis virus vaccine with rearranged genome. Vaccine 2019, 37, 3317–3325.
- Tretyakova, I.; Plante, K.S.; Rossi, S.L.; Lawrence, W.S.; Peel, J.E.; Gudjohnsen, S.; Wang, E.; Mirchandani, D.; Tibbens, A.; Lamichhane, T.N.; et al. Venezuelan equine encephalitis vaccine with rearranged genome resists reversion and protects non-human primates from viremia after aerosol challenge. Vaccine 2020, 38, 3378–3386.
- Trobaugh, D.W.; Sun, C.; Dunn, M.D.; Reed, D.S.; Klimstra, W.B. Rational design of a live-attenuated eastern equine encephalitis virus vaccine through informed mutation of virulence determinants. PLoS Pathog. 2019, 15, e1007584.
- Plante, K.; Wang, E.; Partidos, C.D.; Weger, J.; Gorchakov, R.; Tsetsarkin, K.; Borland, E.M.; Powers, A.M.; Seymour, R.; Stinchcomb, D.T.; et al. Novel chikungunya vaccine candidate with an IRES-based attenuation and host range alteration mechanism. PLoS Pathog. 2011, 7, e1002142.
- Roy, C.J.; Adams, A.P.; Wang, E.; Plante, K.; Gorchakov, R.; Seymour, R.L.; Vinet-Oliphant, H.; Weaver, S.C. Chikungunya vaccine candidate is highly attenuated and protects nonhuman primates against telemetrically monitored disease following a single dose. J. Infect. Dis. 2014, 209, 1891–1899.
- Partidos, C.D.; Paykel, J.; Weger, J.; Borland, E.M.; Powers, A.M.; Seymour, R.; Weaver, S.C.; Stinchcomb, D.T.; Osorio, J.E. Cross-protective immunity against o’nyong-nyong virus afforded by a novel recombinant chikungunya vaccine. Vaccine 2012, 30, 4638–4643.
- Pandya, J.; Gorchakov, R.; Wang, E.; Leal, G.; Weaver, S.C. A vaccine candidate for eastern equine encephalitis virus based on IRES-mediated attenuation. Vaccine 2012, 30, 1276–1282.
- Rossi, S.L.; Guerbois, M.; Gorchakov, R.; Plante, K.S.; Forrester, N.L.; Weaver, S.C. IRES-based Venezuelan equine encephalitis vaccine candidate elicits protective immunity in mice. Virology 2013, 437, 81–88.
- Rossi, S.L.; Russell-Lodrigue, K.E.; Killeen, S.Z.; Wang, E.; Leal, G.; Bergren, N.A.; Vinet-Oliphant, H.; Weaver, S.C. IRES-Containing VEEV Vaccine Protects Cynomolgus Macaques from IE Venezuelan Equine Encephalitis Virus Aerosol Challenge. PLoS Negl. Trop. Dis. 2015, 9, e0003797.
- Guerbois, M.; Volkova, E.; Forrester, N.L.; Rossi, S.L.; Frolov, I.; Weaver, S.C. IRES-driven expression of the capsid protein of the Venezuelan equine encephalitis virus TC-83 vaccine strain increases its attenuation and safety. PLoS Negl. Trop. Dis. 2013, 7, e2197.
- Mota, M.T.O.; Costa, V.V.; Sugimoto, M.A.; Guimaraes, G.F.; Queiroz, C.M., Jr.; Moreira, T.P.; de Sousa, C.D.; Santos, F.M.; Queiroz, V.F.; Passos, I.; et al. In-depth characterization of a novel live-attenuated Mayaro virus vaccine candidate using an immunocompetent mouse model of Mayaro disease. Sci. Rep. 2020, 10, 5306.
- Weise, W.J.; Hermance, M.E.; Forrester, N.; Adams, A.P.; Langsjoen, R.; Gorchakov, R.; Wang, E.; Alcorn, M.D.H.; Tsetsarkin, K.; Weaver, S.C. A novel live-attenuated vaccine candidate for mayaro Fever. PLoS Negl. Trop. Dis. 2014, 8, e2969.
- Tiwari, M.; Parida, M.; Santhosh, S.R.; Khan, M.; Dash, P.K.; Rao, P.V. Assessment of immunogenic potential of Vero adapted formalin inactivated vaccine derived from novel ECSA genotype of Chikungunya virus. Vaccine 2009, 27, 2513–2522.
- Kumar, M.; Sudeep, A.B.; Arankalle, V.A. Evaluation of recombinant E2 protein-based and whole-virus inactivated candidate vaccines against chikungunya virus. Vaccine 2012, 30, 6142–6149.
- Mohan, K. Phase-I Open Label, Dose-Escalation Clinical Trial to Evaluate the Safety, Tolerability and Immunogenicity of Chikungunya Vaccine in Healthy Adults of 18 to 50 Years Age: U.S National Library of Medicine. 2020. Available online: (accessed on 18 March 2021).
- Pittman, P.R.; Liu, C.T.; Cannon, T.L.; Mangiafico, J.A.; Gibbs, P.H. Immune interference after sequential alphavirus vaccine vaccinations. Vaccine 2009, 27, 4879–4882.
- Maryam, K.-J.; Reisler, R.B.; Purcell, B.K.; Rivard, R.G.; Cardile, A.P.; Liggett, D.; Norris, S.; Pitttman, P.R. 2773. Safety and Immunogenicity Study of Eastern Equine Encephalitis Vaccine. Open Forum Infect. Dis. 2019, 6, 978–979.
- Rivard, R. Phase 2 Open-Label Safety and Immunogenicity Study of the Eastern Equine Encephalitis (EEE) Vaccine, Inactivated, Dried, TSI-GSD 104, Lot 2-1-89, in Healthy Adult Subjects at Risk of Exposure to Eastern Equine Encephalitis Virus: U.S. National Library of Medicine. 2016. Available online: (accessed on 18 March 2021).
- Honnold, S.P.; Bakken, R.R.; Fisher, D.; Lind, C.M.; Cohen, J.W.; Eccleston, L.T.; Spurgers, K.B.; Maheshwari, R.K.; Glass, P.J. Second generation inactivated eastern equine encephalitis virus vaccine candidates protect mice against a lethal aerosol challenge. PLoS ONE 2014, 9, e104708.
- Martin, S.S.; Bakken, R.R.; Lind, C.M.; Garcia, P.; Jenkins, E.; Glass, P.J.; Parker, M.D.; Hart, M.K.; Fine, D.L. Evaluation of formalin inactivated V3526 virus with adjuvant as a next generation vaccine candidate for Venezuelan equine encephalitis virus. Vaccine 2010, 28, 3143–3151.
- Gupta, P.; Sharma, A.; Spurgers, K.B.; Bakken, R.R.; Eccleston, L.T.; Cohen, J.W.; Honnold, S.P.; Glass, P.J.; Maheshwari, R.K. 1,5-Iodonaphthyl azide-inactivated V3526 protects against aerosol challenge with virulent venezuelan equine encephalitis virus. Vaccine 2016, 34, 2762–2765.
- Fine, D.L.; Jenkins, E.; Martin, S.S.; Glass, P.; Parker, M.D.; Grimm, B. A multisystem approach for development and evaluation of inactivated vaccines for Venezuelan equine encephalitis virus (VEEV). J. Virol. Method. 2010, 163, 424–432.
- McCarty, J. A Phase 2 Parallel-Group, Randomized, Double-Blind Study to Assess the Safety and Immunogenicity of PXVX0317 (Chikungunya Virus Virus-Like Particle Vaccine [CHIKV-VLP], Unadjuvanted or Alum-adjuvanted): U.S. National Library of Medicine. 2018. Available online: (accessed on 18 March 2021).
- Metz, S.W.; Martina, B.E.; van den Doel, P.; Geertsema, C.; Osterhaus, A.D.; Vlak, J.M.; Pijlman, G.P. Chikungunya virus-like particles are more immunogenic in a lethal AG129 mouse model compared to glycoprotein E1 or E2 subunits. Vaccine 2013, 31, 6092–6096.
- Metz, S.W.; Gardner, J.; Geertsema, C.; Le, T.T.; Goh, L.; Vlak, J.M.; Pijlman, G.P. Effective chikungunya virus-like particle vaccine produced in insect cells. PLoS Negl. Trop. Dis. 2013, 7, e2124.
- Saraswat, S.; Athmaram, T.N.; Parida, M.; Agarwal, A.; Saha, A.; Dash, P.K. Expression and Characterization of Yeast Derived Chikungunya Virus Like Particles (CHIK-VLPs) and Its Evaluation as a Potential Vaccine Candidate. PLoS Negl. Trop. Dis. 2016, 10, e0004782.
- Goonewardena, S. A Phase 1 Dose Escalation Study to Assess the Safety and Immunogenicity of a Monovalent Virus-Like Particle (VLP) Venezuelan Equine Encephalitis Vaccine in Healthy Adults: U.S. National Library of Medicine. 2017. Available online: (accessed on 18 March 2021).
- Ko, S.Y.; Akahata, W.; Yang, E.S.; Kong, W.P.; Burke, C.W.; Honnold, S.P.; Nichols, D.K.; Huang, Y.-J.S.; Schieber, G.L.; Carlton, K.; et al. A virus-like particle vaccine prevents equine encephalitis virus infection in nonhuman primates. Sci. Transl. Med. 2019, 11, 492.
- Ledgerwood, J.C.G. A Phase 1 Open Label, Dose-Escalation Clinical Trial to Evaluate the Safety and Immunogenicity of a Trivalent Virus-Like Particle (VLP) Encephalitis Vaccine, VRC-WEVVLP073-00-VP, in Healthy Adults: U.S. National Library of Medicine. 2019. Available online: (accessed on 18 March 2021).
- Riemenschneider, J.; Garrison, A.; Geisbert, J.; Jahrling, P.; Hevey, M.; Negley, D.; Schmaljohn, A.; Lee, J.; Hart, M.K.; Vanderzanden, L.; et al. Comparison of individual and combination DNA vaccines for B. anthracis, Ebola virus, Marburg virus and Venezuelan equine encephalitis virus. Vaccine 2003, 21, 4071–4080.
- Hart, M.K.; Pratt, W.; Panelo, F.; Tammariello, R.; Dertzbaugh, M. Venezuelan equine encephalitis virus vaccines induce mucosal IgA responses and protection from airborne infection in BALB/c, but not C3H/HeN mice. Vaccine 1997, 15, 363–369.
- Perkins, S.D.; O‘Brien, L.M.; Phillpotts, R.J. Boosting with an adenovirus-based vaccine improves protective efficacy against Venezuelan equine encephalitis virus following DNA vaccination. Vaccine 2006, 24, 3440–3445.
- Dupuy, L.C.; Locher, C.P.; Paidhungat, M.; Richards, M.J.; Lind, C.M.; Bakken, R.; Parker, M.D.; Wahlen, R.G.; Schmaljohn, C.S. Directed molecular evolution improves the immunogenicity and protective efficacy of a Venezuelan equine encephalitis virus DNA vaccine. Vaccine 2009, 27, 4152–4160.
- Tretyakova, I.; Lukashevich, I.S.; Glass, P.; Wang, E.; Weaver, S.; Pushko, P. Novel vaccine against Venezuelan equine encephalitis combines advantages of DNA immunization and a live attenuated vaccine. Vaccine 2013, 31, 1019–1025.
- Gauci, P.J.; Wu, J.Q.; Rayner, G.A.; Barabe, N.D.; Nagata, L.P.; Proll, D.F. Identification of Western equine encephalitis virus structural proteins that confer protection after DNA vaccination. Clin. Vaccine Immunol. 2010, 17, 176–179.
- Muthumani, K.; Lankaraman, K.M.; Laddy, D.J.; Sundaram, S.G.; Chung, C.W.; Sako, E.; Wu, L.; Khan, A.; Sardesai, N.; Kim, J.J.; et al. Immunogenicity of novel consensus-based DNA vaccines against Chikungunya virus. Vaccine 2008, 26, 5128–5134.
- Bao, H.; Ramanathan, A.A.; Kawalakar, O.; Sundaram, S.G.; Tingey, C.; Bian, C.B.; Muruganandam, N.; Vijauachari, P.; Sardesai, N.Y.; Weiner, D.B.; et al. Nonstructural protein 2 (nsP2) of Chikungunya virus (CHIKV) enhances protective immunity mediated by a CHIKV envelope protein expressing DNA Vaccine. Viral Immunol. 2013, 26, 75–83.
- Mallilankaraman, K.; Shedlock, D.J.; Bao, H.; Kawalekar, O.U.; Fagone, P.; Ramanathan, A.A.; Ferraro, B.; Stabenow, J.; Vijayachari, P.; Sundaran, S.G.; et al. A DNA vaccine against chikungunya virus is protective in mice and induces neutralizing antibodies in mice and nonhuman primates. PLoS Negl. Trop. Dis. 2011, 5, e928.
- Dupuy, L.C.; Richards, M.J.; Livingston, B.D.; Hannaman, D.; Schmaljohn, C.S. A Multiagent Alphavirus DNA Vaccine Delivered by Intramuscular Electroporation Elicits Robust and Durable Virus-Specific Immune Responses in Mice and Rabbits and Completely Protects Mice against Lethal Venezuelan, Western, and Eastern Equine Encephalitis Virus Aerosol Challenges. J. Immunol. Res. 2018, 2018, 8521060.
- Choi, H.; Kudchodkar, S.B.; Reuschel, E.L.; Asija, K.; Borole, P.; Ho, M.; Wojtak, K.; Reed, C.; Ramos, S.; Bopp, N.E.; et al. Protective immunity by an engineered DNA vaccine for Mayaro virus. PLoS Negl. Trop. Dis. 2019, 13, e0007042.
- Tretyakova, I.; Hearn, J.; Wang, E.; Weaver, S.; Pushko, P. DNA vaccine initiates replication of live attenuated chikungunya virus in vitro and elicits protective immune response in mice. J. Infect. Dis. 2014, 209, 1882–1890.
- Muthumani, K.; Block, P.; Flingai, S.; Muruganantham, N.; Chaaithanya, I.K.; Tingey, C.; Wise, M.; Reuschel, E.L.; Chung, C.; Muthumani, A.; et al. Rapid and Long-Term Immunity Elicited by DNA-Encoded Antibody Prophylaxis and DNA Vaccination Against Chikungunya Virus. J. Infect. Dis. 2016, 214, 369–378.
- Szurgot, I.; Ljungberg, K.; Kummerer, B.M.; Liljestrom, P. Infectious RNA vaccine protects mice against chikungunya virus infection. Sci. Rep. 2020, 10, 21076.
- Dupuy, L.C.; Richards, M.J.; Ellefsen, B.; Chau, L.; Luxembourg, A.; Hannaman, D.; Livingston, B.D.; Schmaljohn, C.S. A DNA vaccine for venezuelan equine encephalitis virus delivered by intramuscular electroporation elicits high levels of neutralizing antibodies in multiple animal models and provides protective immunity to mice and nonhuman primates. Clin. Vaccine Immunol. 2011, 18, 707–716.
- Hannaman, D.; Dupuy, L.C.; Ellefsen, B.; Schmaljohn, C.S. A Phase 1 clinical trial of a DNA vaccine for Venezuelan equine encephalitis delivered by intramuscular or intradermal electroporation. Vaccine 2016, 34, 3607–3612.
- Nagata, L.P.; Hu, W.G.; Masri, S.A.; Rayner, G.A.; Schmaltz, F.L.; Das, D.; Wu, J.; Long, M.C.; Chan, C.; Proll, D.; et al. Efficacy of DNA vaccination against western equine encephalitis virus infection. Vaccine 2005, 23, 2280–2283.
- Phillips, A.T.; Schountz, T.; Toth, A.M.; Rico, A.B.; Jarvis, D.L.; Powers, A.M.; Olson, K.E. Liposome-antigen-nucleic acid complexes protect mice from lethal challenge with western and eastern equine encephalitis viruses. J. Virol. 2014, 88, 1771–1780.
- Shaw, C.; Panther, L.; August, A.; Zaks, T.; Smolenov, I.; Bart, S.; Watson, M. Safety and immunogenicity of a mRNA-based chikungunya vaccine in a phase 1 dose-ranging trial. Int. J. Infect. Dis. 2019, 79, 17.
- Kose, N.; Fox, J.M.; Sapparapu, G.; Bombardi, R.; Tennekoon, R.N.; de Silva, A.D.; Elbashir, S.M.; Theisen, M.A.; Humphris-Narayanan, E.; Ciaramella, G.; et al. A lipid-encapsulated mRNA encoding a potently neutralizing human monoclonal antibody protects against chikungunya infection. Sci. Immunol. 2019, 4, eaaw6647.
- Moderna, T.X. A Phase 1, Randomized, Placebo-Controlled, Dose Ranging Study to Evaluate the Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of mRNA-1944, Encoding for an Anti-Chikungunya Virus Monoclonal Antibody, in Healthy Adults: U.S. National Library of Medicine. 2019. Available online: (accessed on 18 March 2021).
- Metz, S.W.; Geertsema, C.; Martina, B.E.; Andrade, P.; Heldens, J.G.; van Oers, M.M.; Goldbach, R.W.; Vlak, J.M.; Pijlman, G.P. Functional processing and secretion of Chikungunya virus E1 and E2 glycoproteins in insect cells. Virol. J. 2011, 8, 353.
- Khan, M.; Dhanwani, R.; Rao, P.V.; Parida, M. Subunit vaccine formulations based on recombinant envelope proteins of Chikungunya virus elicit balanced Th1/Th2 response and virus-neutralizing antibodies in mice. Virus Res. 2012, 167, 236–246.
- Brandler, S.; Ruffie, C.; Combredet, C.; Brault, J.B.; Najburg, V.; Prevost, M.C.; Habel, A.; Tauber, E.; Despres, P.; Tangy, F. A recombinant measles vaccine expressing chikungunya virus-like particles is strongly immunogenic and protects mice from lethal challenge with chikungunya virus. Vaccine 2013, 31, 3718–3725.
- Gerke, C.; Frantz, P.N.; Ramsauer, K.; Tangy, F. Measles-vectored vaccine approaches against viral infections: A focus on Chikungunya. Expert Rev. Vaccines 2019, 18, 393–403.
- Rossi, S.L.; Comer, J.E.; Wang, E.; Azar, S.R.; Lawrence, W.S.; Plante, J.A.; Ramsauer, K.; Schrauf, S.; Weaver, S.C. Immunogenicity and Efficacy of a Measles Virus-Vectored Chikungunya Vaccine in Nonhuman Primates. J. Infect. Dis. 2019, 220, 735–742.
- Ramsauer, K.; Schwameis, M.; Firbas, C.; Mullner, M.; Putnak, R.J.; Thomas, S.J.; Despres, P.; Tauber, E.; Jilma, B.; Tangy, F. Immunogenicity, safety, and tolerability of a recombinant measles-virus-based chikungunya vaccine: A randomised, double-blind, placebo-controlled, active-comparator, first-in-man trial. Lancet Infect. Dis. 2015, 15, 519–527.
- Reisinger, E.C.; Tschismarov, R.; Beubler, E.; Wiedermann, U.; Firbas, C.; Loebermann, M.; Pfeiffer, A.; Muellner, M.; Tauber, E.; Ramsauer, L. Immunogenicity, safety, and tolerability of the measles-vectored chikungunya virus vaccine MV-CHIK: A double-blind, randomised, placebo-controlled and active-controlled phase 2 trial. Lancet 2019, 392, 2718–2727.
- Wang, E.; Volkova, E.; Adams, A.P.; Forrester, N.; Xiao, S.Y.; Frolov, I.; Weaver, S.C. Chimeric alphavirus vaccine candidates for chikungunya. Vaccine 2008, 26, 5030–5039.
- Wang, E.; Kim, D.Y.; Weaver, S.C.; Frolov, I. Chimeric Chikungunya viruses are nonpathogenic in highly sensitive mouse models but efficiently induce a protective immune response. J. Virol. 2011, 85, 9249–9252.
- Wang, E.; Petrakova, O.; Adams, A.P.; Aguilar, P.V.; Kang, W.; Paessler, S.; Volk, S.M.; Frolov, I.; Weaver, S.C. Chimeric Sindbis/eastern equine encephalitis vaccine candidates are highly attenuated and immunogenic in mice. Vaccine 2007, 25, 7573–7581.
- Paessler, S.; Fayzulin, R.Z.; Anishchenko, M.; Greene, I.P.; Weaver, S.C.; Frolov, I. Recombinant sindbis/Venezuelan equine encephalitis virus is highly attenuated and immunogenic. J. Virol. 2003, 77, 9278–9286.
- Paessler, S.; Ni, H.; Petrakova, O.; Fayzulin, R.Z.; Yun, N.; Anishchenko, M.; Weaver, S.C.; Frolov, I. Replication and clearance of Venezuelan equine encephalitis virus from the brains of animals vaccinated with chimeric SIN/VEE viruses. J. Virol. 2006, 80, 2784–2796.
- Atasheva, S.; Wang, E.; Adams, A.P.; Plante, K.S.; Ni, S.; Taylor, K.; Miller, M.E.; Frolov, I.; Weaver, S.C. Chimeric alphavirus vaccine candidates protect mice from intranasal challenge with western equine encephalitis virus. Vaccine 2009, 27, 4309–4319.
- Garcia-Arriaza, J.; Cepeda, V.; Hallengard, D.; Sorzano, C.O.; Kummerer, B.M.; Liljestrom, P.; Esteban, M. A novel poxvirus-based vaccine, MVA-CHIKV, is highly immunogenic and protects mice against chikungunya infection. J. Virol. 2014, 88, 3527–3547.
- Weger-Lucarelli, J.; Chu, H.; Aliota, M.T.; Partidos, C.D.; Osorio, J.E. A novel MVA vectored Chikungunya virus vaccine elicits protective immunity in mice. PLoS Negl. Trop. Dis. 2014, 8, e2970.
- Van den Doel, P.; Volz, A.; Roose, J.M.; Sewbalaksing, V.D.; Pijlman, G.P.; van Middelkoop, I.; Duiverman, V.; van de Wetering, E.; Sutter, G.; Osterhaus, A.D.M.E.; et al. Recombinant modified vaccinia virus Ankara expressing glycoprotein E2 of Chikungunya virus protects AG129 mice against lethal challenge. PLoS Negl. Trop. Dis. 2014, 8, e3101.
- Hu, W.G.; Steigerwald, R.; Kalla, M.; Volkmann, A.; Noll, D.; Nagata, L.P. Protective efficacy of monovalent and trivalent recombinant MVA-based vaccines against three encephalitic alphaviruses. Vaccine 2018, 36, 5194–5203.
- Wang, D.; Suhrbier, A.; Penn-Nicholson, A.; Woraratanadharm, J.; Gardner, J.; Luo, M.; Le, T.T.; Anraku, I.; Sakalian, M.; Einfeld, D.; et al. A complex adenovirus vaccine against chikungunya virus provides complete protection against viraemia and arthritis. Vaccine 2011, 29, 2803–2809.
- Lopez-Camacho, C.; Kim, Y.C.; Blight, J.; Lazaro Moreli, M.; Montoya-Diaz, E.; Huiskonen, J.T.; Kummerer, B.M.; Reyes-Sandoval, A. Assessment of Immunogenicity and Neutralisation Efficacy of Viral-Vectored Vaccines Against Chikungunya Virus. Viruses 2019, 11, 322.
- Kroon Campos, R.; Preciado-Llanes, L.; Azar, S.R.; Kim, Y.C.; Brandon, O.; Lopez-Camacho, C.; Reyes-Sandoval, A.; Rossi, S.L. Adenoviral-Vectored Mayaro and Chikungunya Virus Vaccine Candidates Afford Partial Cross-Protection From Lethal Challenge in A129 Mouse Model. Front. Immunol. 2020, 11, 591885.
- Campos, R.K.; Preciado-Llanes, L.; Azar, S.R.; Lopez-Camacho, C.; Reyes-Sandoval, A.; Rossi, S.L. A Single and Un-Adjuvanted Dose of a Chimpanzee Adenovirus-Vectored Vaccine against Chikungunya Virus Fully Protects Mice from Lethal Disease. Pathogens 2019, 8, 231.
- Hill, A.V. Safety and Immunogenicity of a Candidate CHIKV Vaccine (CHIK001): National Library of Medicine (U.S.). 2018. Available online: (accessed on 18 March 2021).
- Phillpotts, R.J.; O’Brien, L.; Appleton, R.E.; Carr, S.; Bennett, A. Intranasal immunisation with defective adenovirus serotype 5 expressing the Venezuelan equine encephalitis virus E2 glycoprotein protects against airborne challenge with virulent virus. Vaccine 2005, 23, 1615–1623.
- Perkins, S.D.; Williams, A.J.; O’Brien, L.M.; Laws, T.R.; Phillpotts, R.J. CpG used as an adjuvant for an adenovirus-based Venezuelan equine encephalitis virus vaccine increases the immune response to the vector, but not to the transgene product. Viral. Immunol. 2008, 21, 451–457.
- Wu, J.Q.; Barabe, N.D.; Chau, D.; Wong, C.; Rayner, G.R.; Hu, W.G.; Nagata, L.P. Complete protection of mice against a lethal dose challenge of western equine encephalitis virus after immunization with an adenovirus-vectored vaccine. Vaccine 2007, 25, 4368–4375.
- Swayze, R.D.; Bhogal, H.S.; Barabe, N.D.; McLaws, L.J.; Wu, J.Q. Envelope protein E1 as vaccine target for western equine encephalitis virus. Vaccine 2011, 29, 813–820.
- Chattopadhyay, A.; Wang, E.; Seymour, R.; Weaver, S.C.; Rose, J.K. A chimeric vesiculo/alphavirus is an effective alphavirus vaccine. J. Virol. 2013, 87, 395–402.
- Nasar, F.; Matassov, D.; Seymour, R.L.; Latham, T.; Gorchakov, R.V.; Nowak, R.M.; Leal, G.; Hamm, S.; Eldridge, J.H.; Tesh, R.B.; et al. Recombinant Isfahan Virus and Vesicular Stomatitis Virus Vaccine Vectors Provide Durable, Multivalent, Single-Dose Protection against Lethal Alphavirus Challenge. J. Virol. 2017, 91, e01729-16.
- Fierro, C. Phase 1 Vaccination Trial to Evaluate Safety, Tolerability and Immunogenicity of a Recombinant MVA-BN-WEV Vaccine in Healthy Adult Subjects: National Library of Medicine (U.S.). 2019. Available online: (accessed on 18 March 2021).
- Erasmus, J.H.; Auguste, A.J.; Kaelber, J.T.; Luo, H.; Rossi, S.L.; Fenton, K.; Leal, G.; Kim, D.Y.; Chiu, W.; Wang, T.; et al. A chikungunya fever vaccine utilizing an insect-specific virus platform. Nat. Med. 2017, 23, 192–199.

