Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Gerardo Cazzato | + 3389 word(s) | 3389 | 2021-09-06 11:22:17 | | | |
| 2 | Vivi Li | Meta information modification | 3389 | 2021-09-08 08:36:20 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Cazzato, G. Urological Melanoma. Encyclopedia. Available online: https://encyclopedia.pub/entry/13926 (accessed on 08 February 2026).
Cazzato G. Urological Melanoma. Encyclopedia. Available at: https://encyclopedia.pub/entry/13926. Accessed February 08, 2026.
Cazzato, Gerardo. "Urological Melanoma" Encyclopedia, https://encyclopedia.pub/entry/13926 (accessed February 08, 2026).
Cazzato, G. (2021, September 06). Urological Melanoma. In Encyclopedia. https://encyclopedia.pub/entry/13926
Cazzato, Gerardo. "Urological Melanoma." Encyclopedia. Web. 06 September, 2021.
Copy Citation
Melanoma is reported as the 19th most common cancer worldwide, with estimated age-standardized incidence rates of 2.8–3.1 per 100,000. Although the origin is most frequently cutaneous, mucosal melanoma has been described several times in literature, and despite its rarity (only 1% of all melanomas), increasing attention is being paid to this disease form. Within this subgroup, melanomas of the uropoetic apparatus are a rarity among rarities. Indeed, less than 50 cases of primary melanoma originating from the urinary bladder have been described, and even less originating from the kidney, renal pelvis and urethra.
melanoma
mucosal melanoma
urology
1. Introduction
Mucosal melanoma (MML) accounts for only 0.03% of all cancer diagnoses and 1.3% of all melanomas [1]. Typically, the median age at diagnosis is older: 67 years compared to 55 years for cutaneous melanoma [1]; about 65% of MML occurs in women. There does not seem to be a clear etiological association with ultraviolet (UV) rays, although no definitive results are yet available; trauma has been suggested as the possible etiological agent [2][3]. Among the different localizations, MML most frequently arises from mucous membranes of the head and neck (45–55%), anorectal region (25%), and genitourinary tract (15–20%) [4][5]. In both males and females, 5% of cases present in the distal urethra [6]. Primary urinary system melanomas are the least common among mucosal melanomas and account for less than 4% of all mucosal melanomas [1][6]. The urethra is the most common site for this type of melanoma, followed by the bladder and ureter (Figure 1). Patients with this form of melanoma are usually elderly (over 60) and asymptomatic or have hematuria symptoms [6][7]. The general approach for mucosal melanomas is wide resection surgery with lymph node dissection, followed by chemotherapy or immunotherapy [7]. However, the rarity of this neoplasm and difficulties in collecting large case series for observational and therapeutic studies have hampered the possibility of devising innovative therapies, including targeted therapies. Molecular studies of urinary tract melanoma are limited [7] although it has been shown that a small subgroup of primary urinary tract melanomas (about 14%) are characterized by the c-kit mutation, while the BRAF mutation is rare, being infrequently observed, unlike in cutaneous melanoma [7].
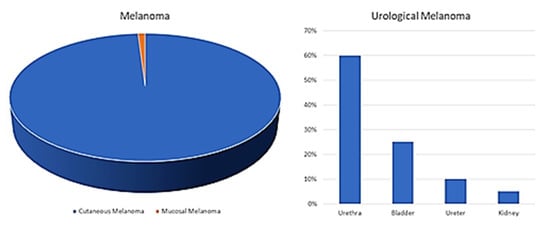
Figure 1. Primary melanoma of the urinary tract is a rarity among rarities (<4% of all the mucosal melanoma). The urethra is the most common location for this type of melanoma (50%), followed by the bladder and ureter with decreasing incidences [7].
2. Discussion
Primary mucosal melanoma of the uropoietic apparatus is a very rare disease entity as compared to the cutaneous melanoma counterpart [1][2][3]; such forms account for just under 4% of all mucosal melanomas [7]. The sites most commonly affected are, in declining order, the kidney, ureter, bladder and urethra [7][8].
2.1. Kidney
Fujimoto et al. [8], Frasier et al. [9] and Tajima et al. [10] were the first authors to publish case reports of suspected primary MM of the kidney and/or renal pelvis in 3 patients. In 2002, Yildirim Bayazit et al. [11] described the third known case of primary MM of the kidney, originating from the medial lobe, in a 37-year-old patient. This patient had previously undergone fine needle aspiration cytology (FNAC), which had revealed a cell population of uncertain classification. The patient underwent therapy with Interferon 2b but died of systemic progression of the disease.
Later, in 2011, a new report was made by Tasdemir et al. [12] of a case of MM of the kidney, incidentally discovered in a 67-year-old male. The question as to whether primary MM of the kidney really exists had by then been much debated among dermatopathologists and uropathologists. It was discussed in 2000, in a paper by Ribalta et al. [13], who reported the clinical case of a 73-year-old man who presented with a hemorrhagic renal tumor initially interpreted as renal cell carcinoma (RCC). Then, after he suffered a retroperitoneal recurrence infiltrating the duodenal wall, immunohistochemistry showed positivity to HMB45, S-100 protein, actin and vimentin. The authors proposed considering this kidney cancer as a malignant epithelioid, pigmented, clear cell (“sugar”) variant of angiomyolipoma, rather than a primary MM of the kidney, raising doubts about the existence of this latter. In this context, a complete medical history and accurate dermatological, ophthalmological and internal medicine studies are fundamental to exclude any possibility that an unidentified, regressed melanocytic lesion could actually be responsible for the kidney involvement. Criteria have been developed, originally for MM of the bladder, but that are well suited also to all types of mucosal melanoma. Ainsworth et al. [14] and Stein-Kendall [15] stressed the importance of ascertaining any previous or current history of cutaneous melanoma and making a meticulous analysis of the entire cutaneous surface (including the use of a Woods lamp to exclude the presence of any depigmented area indicating regression of a possible melanoma). Necessary examinations include a thorough clinical study to exclude any ophthalmic or visceral site of onset, and microscopic study of any atypical melanocytes present in the mucosa adjacent to the main tumoral mass. When one or more of these criteria are present, then a metastatic melanoma may be hypothesized. The authors Cunningham et al. [16], Boughan et al. [17], Klatte et al. [18] and Levin et al. [19] reported cases of metastatic MM of the kidney of an ascertained primary nature. This is the essential watershed in this field. In the paper by Levin et al. [19], the very first case of renal metastasis of a primary ocular melanoma was reported, 20 years after the histological diagnosis. In conclusion, it seems to be absolutely essential to fully reconstruct the patient’s history, and to remember that one of the greatest risks of misdiagnosis for the histopathologist is in cases of “epithelioid” and/or atypical variants of renal angiomyolipoma, which can be taken for MM. This risk is well known and described in the literature [20][21]. Table 1 summarizes all studies related to kidney melanoma.
2.2. Ureter
More than 90% of cases of melanoma of the ureter are metastatic localizations of a previous cutaneous melanoma [6][7], although case histories and anecdotes have been reported, describing primary lesions likely originating from the ureteral mucosa.
One of the very first cases in the literature dates back to 1962, when Judd et al. [22] described the case of a 63-year-old man with no history of cutaneous melanoma, who developed a primary lesion of the ureter. Only after autopsy was this revealed to be secondary to a previous lesion of the superior renal calyx in the right kidney. After another case described by Garcia et al. in 1969 [23], more recently (2016), Khan et al. [24] described the case of a 78-year-old man with hematuria. Following cystectomy, histology revealed a synchronous melanoma of the bladder and ureter. In this paper, the authors highlighted the importance of multidisciplinary therapeutic management for this type of lesions, although therapy has not yet been standardized. Gakis et al. [25], Macneil et al. [26] and March et al. [27] described cases of metastatic involvement of the ureters in cases of primary cutaneous MM: this is the scenario most commonly observed. Table 2 summarizes all studies related to ureter melanoma.
2.3. Urinary Bladder
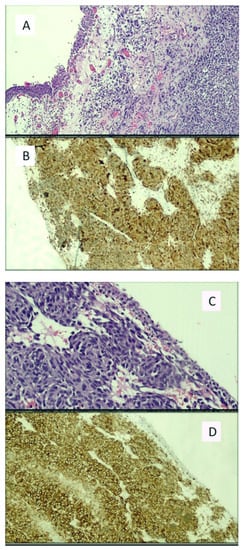
The earliest cases of primary melanoma of the bladder in literature were published in 1980, when Willis et al. [28] and Anichkov and Nikonov (1982) [29] reported the first four patients affected by a presumed bladder MM, with no clinical history of primary cutaneous melanocytic neoplasia. Then, in 1988, adding to the very few cases yet described, Goldschmidt et al. [30] detailed their experience of a 53-year-old woman who complained of persistent hematuria that had lasted some time, although she did not remember precisely how long. Urography and cystoscopy revealed a “mushroom-like” lesion on the bladder wall, and after targeted biopsy, the diagnosis of MM was made and radical cystectomy was performed. After 6 months of close follow-up, no recurrence had been observed. In the second case reported by the same authors, a 56-year-old woman presented with a nodule at the angle of the mandible. Biopsy demonstrated a proliferation of melanocytic cells attributable to melanoma. Following histomorphological and ultrastructural studies, the authors concluded that it was a subcutaneous metastasis of a primary melanoma originating in the bladder mucosa. An example of bladder melanoma (found during our practice) is presented in Figure 2A–D.
Figure 2. (A) Histological micrograph including urothelial mucosa and subepithelial proliferation of pleomorphic cells disposition, with atypia and nuclear pleomorphism but without evident presence of melanic pigment. (Hematoxylin-Eosin, Original Magnification: 10×). (B) The proliferation was shown to be constituted by melanocytes immunoreactive to the anti-HMB-45 antibody (Immunohistochemistry, Original Magnification: 10×). (C) Histological detail of the bladder mucosa including melanocytes proliferation nested around the blood vessels. (Hematoxylin-Eosin, Original Magnification: 20×). (D) Diffuse, strongly positive immunoreaction to the anti-HMB45 antibody. (Immunohistochemistry, Original Magnification: 20×). The sample belonged to a patient with primary bladder melanoma who died a few months after the histological diagnosis. Molecular investigations revealed the presence of the BRAFV600E mutation.
In 1992, Van Ahlen H. et al. [31] reported the clinical case of an 82-year-old patient who had been referring to their outpatients clinic for some years for bladder symptoms. Initially, these had been misinterpreted as due to an Escherichia coli infection, but antibiotic therapy had not resolved nor improved the symptoms in any way. Cystoscopy demonstrated a papillary lesion at the base of the bladder, with no anomalous pigmentation at macroscopic examination. The patient underwent transurethral resection of the bladder trigon (TURBT). Histology revealed a solid tumor with many necrotic areas, showing positivity to S-100 protein and MM was therefore diagnosed. Another case was reported in 2011 by Ammari El. et al. [32], and then in 2012, Schindler et al. [33] described the only case (until now) of primary melanoma of the urinary bladder, with a rhabdoid phenotype, in a female patient. She was treated with the anti-CTLA4 antibody Ipilimumab, which yielded a partial response. In the same paper, the diagnostic problems of this very rare disease were discussed, and the possibility was highlighted that at immunohistochemistry (IHC) the tumoral cells could be positive for S-100 protein, Vimentin and CD56 (NCAM), and negative for routine melanocytic markers such as Melan-A and HMB-45, was highlighted. Other reports of primary melanoma of the bladder were made in the following years [34][35][36][37][38][39][40][41]. Very recently, in 2021, Snajdar E. et al. [42] reported the case of a 78-year-old woman who presented to the Emergency Department for a new onset of incontinence and macroscopic hematuria. After the first examination and various tests, she underwent TURBT. Histopathologic analysis of the tumor revealed a primary MM of the bladder, in which the tumor cells stained positive for HMB-45 and S-100 protein. After the histopathologic result, fluorodeoxyyglucose (FDG) positron emission tomography (PET) was performed, yielding positive results only in the bladder and negative imaging of the chest. The diagnosis of a primary MM of the bladder was confirmed. After about 8 months, the patient underwent radical cystectomy and pelvic lymph nodes dissection; histology confirmed the previous TURBT diagnosis. A few months later, the patient died of metastatic disease progression. Various reports [43][44][45][46][47][48][49][50][51][52][53] have dealt with cases of secondary involvement of the bladder by a previous cutaneous skin melanoma. In one of the most recent of these papers, Topal et al. [51] reported their experience of a 70-year-old patient who had presented to the Urology Department for macrohematuria. Both the TURBT, and the later operative specimen from radical cystectomy, were positive for MM, that appeared to be primary. However, close study and reconstruction of the clinical history demonstrated that 15 years before, the woman had undergone enucleation of the left ocular bulb for primary ocular MM. This case was, therefore, the third report in literature of this very rare occurrence [48][49]. In light of the results of this review of MM of the urinary bladder, we can state that we believe the above-mentioned criteria for the kidney, proposed by Ainsworth et al., remain valid today. These authors consider that primary MM of the bladder is a diagnosis based on exclusion, to be made only after having very carefully reconstructed the entire personal and family history of the affected patient.
It is important, in our view, to underline the lack of agreement in the scientific community also as regards whether primary melanoma of the bladder actually exists. For example, in 2000, García Montes et al. [54] presented the case of a 30-year-old patient with a diagnosis of suspected primary melanoma of the bladder, discussed the relatively stringent criteria for such a diagnosis, but concluded that no test could definitively demonstrate that there had been no previous complete regression of a hypothetical primary cutaneous melanocytic lesion that could no longer be identified.
As regards the best treatment, it should be remembered that the prognosis of primary and/or metastatic melanoma of the bladder is always poor. Some more recent works have attempted to define a therapeutic algorithm [55]. In 2019, Chaus et al. [56] reported the clinical case of a 27-year-old woman with a family history of melanoma and evidence of a malignant melanoma of the urinary bladder. After TURBT, various instrumental examinations such as CT/abdominal-pelvic MRI and total-body PET were negative for distant recurrence, so the CARIS molecular intelligence tumor profiling was characterized. This showed positivity for the following mutations: BRAF V600E, PTEN Exon 9, PDL1-2+, and a high tumor mutation burden. The patient was therefore subjected to partial robot-assisted cystectomy and immunotherapy with Pembrolizumab, a PD-1 anti-immune checkpoint. During the subsequent 2-year follow-up, the patient was disease-free and showed no signs of major toxicity. Recently, in 2021, Rapisarda et al. [57] described the clinical history of a 74-year-old man with primary melanoma of the bladder. He was treated with TURBT plus intravesical chemotherapy with Bacillus Calmette-Guérin (BCG), that offers a further treatment option for this neoplasia, but only in selected cases.
To conclude, it must be borne in mind both that the survival rate at three years in patients affected by bladder melanoma is very low, and that the disease is so rare that a standardized treatment protocol is still lacking. Table 3 summarizes all studies related to bladder melanoma.
2.4. Urethra and Penis
One of the first reports in literature of a primary melanoma of the urethra or penis in a male patient dates back to 1976, when Konigsberg H. et al. and Gray G.F. et al. [58] presented two rare cases, one of penile melanosis and the other of a primary melanoma of the penis. The authors underlined the rarity of both clinical pictures, the clinical difficulties of making a differential diagnosis between the two conditions (the first of which is benign but the second overtly malignant) and suggested what might be the best therapeutic approaches (at the time). After that, growing numbers of reports were made [59][60][61][62][63][64][65][66][67]. Then, in 1993, Rashid et al. [66] reported two cases of primary melanoma, one of the male urethra and one of the penis, in two middle-aged subjects. They probed the difficulties in diagnosing such lesions. Although some suggestions had already been made (such as staining for melanin according to Fontana-Masson), the authors stressed the different biological behavior of melanocytic lesions at the genital level and discussed the various treatment options available at the time. The survival rate of patients affected by primary melanoma of the urethra or penis was very low (<5% at 3 years) [68], although in 1996 a patient with urethral melanoma was reported, who unexpectedly survived, disease-free, for several years [69].
In 2005, Ortis S. et al. [70] reported their experience of 10 patients, enrolled over a period of about 42 years (1962–2000), affected by primary melanoma of the penis/urethra, as well as 6 patients affected by primary melanoma of the scrotal skin. They evaluated the clinical and pathologic characteristics, the Breslow thickness, surgical treatment and clinical course. Of the 10 patients enrolled, 4 had stage T1 (according to the American Joint Committee on Cancer), with a depth of less than 0.75 mm; 3 had stage T2 (0.75–1.5 mm) and 3, stage T3 (1.51–4 mm). In only one of 4 cases with palpable inguinal lymph nodes did lymphadenectomy (BILND) demonstrate inguinal lymph node metastases. In 7 patients with stage T1-2N0M0, no local recurrence occurred after wide local excision (WLE) or partial penectomy, after a mean follow-up of 35 months. Six of the seven men remained disease-free. In all the patients with melanoma of the penis, the specific actuarial survival and disease-free rates at 5 years were 80% and 60%, respectively, at a median follow-up of 39 months (range 20 to 210). The six patients with scrotal melanoma were treated with WLE and no local recurrence occurred. Three of the 6 patients presented palpable inguinal lymph nodes, and 2 of them died after chemotherapy for non resectable disease, while 1 died of other causes, 51 months after a negative BILND. The 3 men with clinically negative inguinal lymph nodes, who did not undergo BILND prophylaxis, developed distant (1) or regional metastases (2) and died of disease progression. In the patients with scrotal melanoma, the specific actuarial survival and disease-free rates at 5 years were 33.3% and 33.3%, respectively, after a median follow-up of 36 months.
Many other reports [71][72][73][74][75][76][77][78][79][80][81][82][83][84][85][86][87][88][89][90][91][92][93][94][95][96] have described cases of primary melanoma of the penis/male urethra. Instead, in 2020, Naktra et al. [97] presented a curious case of primary melanoma of the female urethra with neuroendocrine differentiation, in a 62-year-old woman with urinary obstruction symptoms. Clinical and radiological examination revealed a large urethral mass with liver and lymph nodes metastases. Biopsies were made of the urethral and hepatic lesions, demonstrating poorly differentiated tumor cells with a small cell morphology and the presence of melanic pigment. These cells were immunopositive for melanocytic and neuroendocrine markers. Ultrastructural examination demonstrated the presence of melanosomes and neurosecretory granules in the tumor cells. This was the very first case report of this disease entity originating in the female urethra (in itself extremely rare, accounting for 0.2% of all forms of melanoma) with a “small cell” appearance at histology.
Still more recently (2021), Burity et al. [98] presented a case of primary melanoma of the urethra in a 79-year-old male patient, with a blackened lesion of the urethral meatus, 1.5 cm in size. Biopsy demonstrated a malignant neoplasia, and the patient underwent partial penectomy, with 2 cm excision margins, and deep bilateral lymphadenectomy. No disease recurrence was observed at follow-up. In the conclusions, the authors underlined the fact that the tumoral mutation burden of melanoma in uncommon sites such as the urethra/penis is lower overall than in sunrays-exposure cutaneous melanoma. This can also influence the response rate, to immunotherapy, for example. Moreover, in mucosal melanoma a distinct model of chromosomal aberrations has been reported, as well as a higher rate of copy number alterations, and frequent KIT mutations in urogenital melanomas. Table 4 summarizes all studies related to urethra and penis melanoma.
Finally, in 2020, a series of authors developed UK national guidelines [99], aiming to make the diagnostic-therapeutic assistance (PDTA) pathways of patients with uro-genital tract melanoma more uniform, clear and easily accessible, starting from the evidence in the literature. After briefly summarizing the evidence from case reports and case series present in the literature and discussing the main histomorphological and immunophenotypic characteristics, as well as molecular biology, the authors underline that the best treatment approach aimed at modifying the (rather low) survival rates of patients with MM should be based on the most up-to-date guidelines, and in this regard their recommendations are to: (1) use single-agent programmed cell death protein 1 (PD1) antibodies in patients with unresectable stage III or stage IV tumors, but taking into account any contraindications to this therapy; (2) consider combination immunotherapy, for example, anti-CTLA (cytotoxic T-lymphocyte-associated protein and anti-PD1/PD-L1 (programmed cell death ligand monoclonal antibodies in selected, fit patients; (3) consider BRAF + MEK inhibitors as a treatment option for the small number of patients with BRAF mutated unresectable stage III or stage IV MM: (4) in all cases where there is no clearly predominant risk/benefit ratio for any therapeutic approach, inform the patient about all the existing possibilities and choose together.
3. Conclusions
Due to the rarity of these disease entities, their diagnosis and treatment still pose a challenge. Primary melanoma of the urological tract is a very rare and aggressive neoplasm. Despite the controversies that have arisen about the appropriate surgical treatment, early diagnosis and treatment are essential to allow a successful clinical outcome and patient survival. Targeted therapy may be a good treatment alternative for this rare and poorly diagnosed tumor type. For example, in one of the most recent works in the literature [7], it is clearly demonstrated how next generation sequencing is opening up new avenues for studying mutations also in this subgroup of pathology. In particular, mutations were found in more recurrent genes as also BRAF V600E, BRAF V600K, but also amplifications of genes such as ERBB2, FGFR1, and MET. In addition, a subset of patients had KIT gene mutations. Considering the potential difficulty in diagnosis and the lack of an optimized management algorithm, we believe that more research, including the identification of molecular targets, will add value to the literature on the diagnosis and treatment of urinary melanoma.
References
- World Health Organization (WHO). Classification of Skin Tumours; IARC: Lyon, France, 2018.
- Yde, S.S.; Sjoegren, P.; Heje, M.; Stolle, L.B. Mucosal Melanoma: A Literature Review. Curr. Oncol. Rep. 2018, 20, 28.
- Sánchez, R.B.; Bustos, B.D.U.; Mira, M.N.; Estrada, R.B. Mucosal Melanoma: An Update. Actas Dermo-Sifiliográficas 2015, 106, 96–103.
- Chang, A.E.; Karnell, L.H.; Menck, H.R. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: A summary of 84,836 cases from the past decade. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer 1998, 15, 1664–1678.
- Gru, A.A.; Becker, N.; Dehner, L.P.; Pfeifer, J.D. Mucosal melanoma: Correlation of clinicopathologic, prognostic, and molecular features. Melanoma Res. 2014, 24, 360–370.
- Nguyen, A.T.; Kavolius, J.P.; Russo, P.; Grimaldi, G.; Katz, J.; Brady, M.S. Primary genitourinary melanoma. Urology 2001, 57, 633–638.
- Acikalin, A.; Bagir, E.; Karim, S.; Bisgin, A.; Izol, V.; Erdogan, S. Primary melanoma of the urinary tract; Clinicopathologic and molecular review of a case series. Pathol. Res. Pract. 2020, 216, 153095.
- Fujimoto, H.; Chitose, K.; Tobisu, K.; Yamazaki, N.; Sakamoto, M.; Kakizoe, T. Solitary renal melanoma? A case with long survival after initial treatment. J. Urol. 1995, 153, 1887–1889.
- Frasier, B.L.; Wachs, B.H.; Watson, L.R.; Tomasulo, J.P. Malignant Melanoma of the Renal Pelvis Presenting as a Primary Tumor. J. Urol. 1988, 140, 812–814.
- Tajima, K.; Saito, K.; Umeda, Y.; Murata, T.; Satani, H. Malignant Melanoma of the Kidney Presenting as a Primary Tumor. Int. J. Urol. 1997, 4, 94–96.
- Hor Bayazit, Y.; Aridoğan, I.A.; Zeren, S.; Gönlüşen, G.; Tansug, Z. Primary malignant melanoma of the kidney. Scand. J. Urol. Nephrol. 2002, 36, 77–79.
- Tasdemir, C.; Samdanci, E.T.; Dogan, M.; Elmali, C.; Sargin, S.Y. Primer malignant melanoma of kidney: A case report. Eur. Rev. Med. Pharmacol. Sci. 2011, 15, 971–972.
- Ribalta, T.; Lloreta, J.; Munné, A.; Serrano, S.; Cardesa, A. Malignant pigmented clear cell epithelioid tumor of the kidney:Clear cell (“SUGAR”) tumor versus malignant melanoma. Hum. Pathol. 2000, 31, 516–519.
- Ainsworth, A.M.; Clark, W.H.; Mastrangelo, M.; Conger, K.B. Primary malignant melanoma of the urinary bladder. Cancer 1976, 37, 1928–1936.
- Stein, B.S.; Kendall, A.R. Malignant Melanoma of the Genitourinary Tract. J. Urol. 1984, 132, 859–868.
- Cunningham, J.A.; Fendler, J.-P.; Nichols, P.J.; Skinner, D.G. Metastatic malignant melanoma: An unusual case presentation. Urology 1994, 44, 924–926.
- Boughan, K.M.; Setrakian, S.; Lee, C.H.; Spiro, T.P.; Daw, H.A. A Renal Mass in a Patient with Melanoma. Clin. Genitourin. Cancer 2009, 7, E98–E100.
- Klatte, T.; Rao, J.Y.; Ribas, A.; Pantuck, A.J. Metastatic Melanoma to the Kidney Presenting with Renal Vein Tumor Thrombus. Urology 2007, 69, 982.e7–982.e9.
- Levin, B.M.; Boulos, F.I.; Herrell, S.D. Metastatic ocular melanoma to the kidney 20 years after initial diagnosis. Urology 2005, 66, 658.e11–658.e12.
- Makhlouf, H.R.; Ishak, K.G.; Shekar, R.; Sesterhenn, I.A.; Young, D.Y.; Fanburg-Smith, J.C. Melanoma markers in angiomyo-lipoma of the liver and kidney: A comparative study. Arch. Pathol. Lab. Med. 2002, 126, 49–55.
- Esheba Gel, S.; Esheba Nel, S. Angiomyolipoma of the kidney: Clinicopathological and immunohistochemical study. J. Egypt. Natl. Canc. Inst. 2013, 25, 125–134.
- Judd, R.L. Melanoma of the Ureter: A Case Report. J. Urol. 1962, 87, 805–807.
- Garcia, A.; Monserrat, J.M.; Martin, G.G. Melanoma of the ureter. Rev. Argent. Urol. Nefrol. 1969, 38, 58–61.
- Khan, M.; O’Kane, D.; Du Plessis, J.; Hoag, N.; Lawrentschuk, N. Primary malignant melanoma of the urinary bladder and ureter. Can. J. Urol. 2016, 23, 8171–8175.
- Gakis, G.; Merseburger, A.S.; Sotlar, K.; A Kuczyk, M.; Sievert, K.-D.; Stenzl, A. Metastasis of malignant melanoma in the ureter: Possible algorithms for a therapeutic approach. Int. J. Urol. 2009, 16, 407–409.
- MacNeil, J.; Hossack, T. A Case of Metastatic Melanoma in the Ureter. Case Rep. Urol. 2016, 2016, 1853015.
- March, B.; Calopedos, R.J.S.; Latif, E.; Ouyang, R. Ureteric Obstruction from Malignant Melanoma in Both Right Double Moiety and Left Single Moiety Ureters. Urology 2017, 103, e7–e8.
- Willis, A.J.; Huang, A.H.; Carroll, P. Primary Melanoma of the Bladder: A Case Report and Review. J. Urol. 1980, 123, 278–281.
- Anichkov, N.M.; Nikonov, A.A. Primary Malignant Melanomas of the Bladder. J. Urol. 1982, 128, 813–815.
- Goldschmidt, P.; Py, J.M.; Kostakopoulos, A.; Jacqmin, D.; Grosshans, E.; Bollack, C. Primary Malignant Melanomas of the Urinary Bladder. BJU Int. 1988, 61, 359.
- Van Ahlen, H.; Nicolas, V.; Lenz, W.; Boldth, I.; Bockisch, A.; Vahlensieck, W. Primary melanoma of urinary bladder. Urology 1992, 40, 550–554.
- El Ammari, J.E.; Ahallal, Y.; El Fassi, M.J.; Farih, M.H. Primary malignant melanoma of the urinary bladder. Case Rep. Urol. 2011, 2011, 932973.
- Schindler, K.; Schicher, N.; Kunstfeld, R.; Pehamberger, H.; Toepker, M.; Haitel, A.; Hoeller, C.; Harmankaya, K. A rare case of primary rhabdoid melanoma of the urinary bladder treated with ipilimumab, an anti-CTLA 4 monoclonal antibody. Melanoma Res. 2012, 22, 320–325.
- Lange-Welker, U.; Papadopoulos, I.; Wacker, H. Primary Malignant Melanoma of the Bladder. A case report and literature review. Urol. Int. 1993, 50, 226–228.
- Pacella, M.; Gallo, F.; Gastaldi, C.; Ambruosi, C.; Carmignani, G. Primary malignant melanoma of the bladder. Int. J. Urol. 2006, 13, 635–637.
- Truong, H.; Sundi, D.; Sopko, N.; Xing, D.; Lipson, E.J.; Bivalacqua, T.J. A Case Report of Primary Recurrent Malignant Mel-anoma of the Urinary Bladder. Urol. Case Rep. 2013, 12, 2–4.
- Karabulut, Y.Y.; Erdogan, S.; Sayar, H.; Ergen, A.; Baydar, D.E. Primary malignant melanoma of the urinary bladder: Clinical, morphological, and molecular analysis of five cases. Melanoma Res. 2016, 26, 616–624.
- Laudisio, A.; Giua, R.; Papalia, R.; Taffon, C.; Muto, G.; Incalzi, R.A. An Unusual Cause of Hematuria: Primary Bladder Melanoma in an Older Man. J. Am. Geriatr. Soc. 2016, 64, e122–e123.
- Buscarini, M.; Conforti, C.; Incalzi, R.A.; Falavolti, C.; Taffon, C.; Muto, G.; Dianzani, C. Primary Malignant Melanoma of the Bladder. Skinmed 2017, 15, 395–397.
- Singh, V.; Gupta, K.; Dewana, S.; Mandal, A.K. Spotting the pigmented ‘Monster’: Primary melanoma in urinary bladder. BMJ Case Rep. 2019, 23, e231950.
- Kirigin, M.; Lež, C.; Šarčević, B.; Šoipi, Š.; Jaić, G.; Ulamec, M.; Krušlin, B. Primary Malignant Melanoma of the Urinary Bladder: Case Report. Acta Clin. Croat. 2019, 58, 180–182.
- Snajdar, E.; Ajo, A.R.; Rosen, K.; Miller, R.; Mohammed, S.; Gordon, C.; Pui, J.C.; McIntosh, G. Primary Malignant Melanoma of the Urinary Bladder. Cureus 2021, 23, e14067.
- Maeda, T.; Uchida, Y.; Kouda, T.; Matsui, H.; Kawahara, Y.; Sato, T.; Nakajima, F. Metastatic malignant melanoma of the urinary bladder presenting with hematuria: A case report. Hinyokika Kiyo Acta Urol. Jpn. 2008, 54, 787–790.
- Nohara, T.; Sakai, A.; Fuse, H.; Imamura, Y. Metastatic Malignant Melanoma of the Urinary Bladder: A Case Report. Jpn. J. Urol. 2009, 100, 707–711.
- Siroy, A.E.; MacLennan, G.T. Primary Melanoma of the Bladder. J. Urol. 2011, 185, 1096–1097.
- Efesoy, O.; Çayan, S. Bladder metastasis of malignant melanoma: A case report and review of literature. Med. Oncol. 2010, 28, 667–669.
- Meunier, R.; Pareek, G.; Amin, A. Metastasis of Malignant Melanoma to Urinary Bladder: A Case Report and Review of the Literature. Case Rep. Pathol. 2015, 2015, 173870.
- Theocharides, C.; Chatzopoulos, K.; Papanikolaou, D.; Siokas, V.; Amplianitis, I.; Papanikolaou, A. Metastatic Melanoma to the Urinary Bladder of Ocular Origin Accompanied with Primary Cutaneous Melanoma: Diagnostic Challenge—A Report of a Case. Case Rep. Pathol. 2017, 2017, 4818537.
- Paterson, A.; Sut, M.; Kaul, A.; Altieri, V.; Mutch, F.; Patel, J.; Sharma, H. Metastatic malignant melanoma of the urinary bladder: Case report and literature review. Cent. Eur. J. Urol. 2012, 65, 232–234.
- Ikeda, A.; Miyagawa, T.; Kurobe, M.; Uchida, M.; Kojima, T.; Tsutsumi, M.; Ito, S.; Sugita, S.; Nishiyama, H. Case of metastatic malignant melanoma of the urinary bladder. Hinyokika Kiyo Acta Urol. Jpn. 2013, 59, 579–582.
- Topal, C.; Kır, G.; Daş, T.; Sarbay, B.; Tosun, M.I. Metastatic malignant melanoma of the urinary bladder: A case report and review of the literature. Indian J. Pathol. Microbiol. 2016, 59, 532–534.
- Patil, R.V.; Woldu, S.L.; Lucas, E.; Quinn, A.M.; Francis, F.; Margulis, V. Metastatic Melanoma to the Bladder: Case Report and Review of the Literature. Urol. Case Rep. 2017, 11, 33–36.
- Barillaro, F.; Camilli, M.; Dessanti, P.; Chiesa, F.G.N.; Villa, A.; Pastorino, A.; Aschele, C.; Conti, E. Primary melanoma of the bladder: Case report and review of the literature. Arch. Ital. Urol. Androl. 2018, 30, 224–226.
- Montes, F.G.; Gómez, M.F.L.; Boyd, J. Does primary melanoma of the bladder exist? Actas Urológicas Españolas 2000, 24, 433–436.
- Lee, C.S.D.; Komenaka, I.K.; Hurst-Wicker, K.S.; DeRaffele, G.; Mitcham, J.; Kaufman, H.L. Management of metastatic malignant melanoma of the bladder. Urology 2003, 62, 351.
- Chaus, F.M.; Craig, M.; Bracamonte, E.; Sundararajan, S.; Lee, B.R. Primary Malignant Melanoma of the Bladder Treated by Robotic Partial Cystectomy and Immunotherapy. J. Endourol. Case Rep. 2019, 5, 151–153.
- Rapisarda, S.; Bada, M.; Polara, A.; Crocetto, F.; Creta, M.; Chiancone, F.; Occhipinti, M.; Bertoloni, R.; Marciano, A.; Aresu, L.; et al. Conservative management of primary malignant melanoma of the bladder: A case report. J. Med. Case Rep. 2021, 15, 1–4.
- Konigsberg, H.A.; Gray, G.F. Benign melanosis and malignant melanoma of penis and male urethra. Urology 1976, 7, 323–326.
- Yamamoto, N.; Maeda, S.; Takeuchi, T.; Tokuyama, H.; Kanematsu, M.; Kuriyama, M.; Ban, Y.; Kawada, Y.; Mizoguchi, Y.; Kasahara, M. Malignant melanoma of male urethra: A case report. Hinyokika Kiyo Acta Urol. Jpn. 1989, 35, 121–126.
- Primus, G.; Soyer, H.P.; Smolle, J.; Mertl, G.; Pummer, K.; Kerl, H. Early ‘Invasive’ Malignant Melanoma of the Glans penis and the Male Urethra. Report of a case and review of the literature. Eur. Urol. 1990, 18, 156–159.
- Calcagno, L.; Casarico, A.; Bandelloni, R.; Gambini, C. Primary malignant melanoma of male urethra. Urology 1991, 37, 366–368.
- Fujimoto, N.; Oda, M.; Shimoe, S. Primary Malignant Melanoma of the Male Urethra. Urol. Int. 1991, 47, 176–177.
- Ander, H.; Esen, T.; Tellaloğlu, S.; Uysal, V. Successful management of malignant melanoma of male urethra with local excision and adjuvant radiochemotherapy. Prog. Clin. Biol. Res. 1991, 370, 379–383.
- Arai, K.; Joko, M.; Kagebayashi, Y.; Tsumatani, K.; Kimura, S.; Sasaki, K.; Samma, S.; Okajima, E.; Nakaoka, S. Primary ma-lignant melanoma of the female urethra: A case report. Jpn. J. Clin. Oncol. 1993, 23, 74–77.
- Kim, C.J.; Pak, K.; Hamaguchi, A.; Ishida, A.; Arai, Y.; Konishi, T.; Okada, Y.; Tomoyoshi, T. Primary malignant melanoma of the female urethra. Cancer 1993, 71, 448–451.
- Rashi, A.-M.; Williams, R.M.; Horton, L. Malignant melanoma of penis and male urethra Is it a difficult tumor to diagnose? Urology 1993, 41, 470–471.
- Aragona, F.; Maio, G.; Piazza, R.; Salmaso, R. Primary malignant melanoma of the female urethra: A case report. Int. Urol. Nephrol. 1995, 27, 107–111.
- Touyama, H.; Hatano, T.; Ogawa, Y. Primary malignant melanoma of the female urethra: A case report. Hinyokika Kiyo Acta Urol. Jpn. 1997, 43, 597–598.
- Girgin, C.; Tarhan, H.; Sezer, A.; Ermete, M.; Gürel, G. A large primary malignant melanoma of the female urethra. Urol. Int. 1999, 63, 198–200.
- Sánchez-Ortiz, R.; Huang, S.F.; Tamboli, P.; Prieto, V.G.; Hester, G.; Pettaway, C.A. Melanoma of the penis, scrotum and male urethra: A 40-year single institution experience. J. Urol. 2005, 173, 1958–1965.
- Katz, E.E.; Suzue, K.; Wille, M.A.; Krausz, T.; Rapp, D.E.; Sokoloff, M.H. Primary malignant melanoma of the urethra. Urology 2005, 65, 389.
- Kato, H.; Hayashi, K.; Saida, T.; Kontani, K.; Nishizawa, O. Urethral Advancement Procedure for Reconstruction after Excision of Male Parameatal Melanoma in situ. Urol. Int. 2005, 74, 183–184.
- Yoshizawa, T.; Kawata, N.; Sato, K.; Hirakata, H.; Igarashi, T.; Ichinose, T.; Yamaguchi, K.; Takahashi, S. Primary Malignant Melanoma of the Female Urethra. Urology 2007, 70, 1222.e13–1222.e16.
- Nakamoto, T.; Inoue, Y.; Ueki, T.; Niimi, N.; Iwasaki, Y. Primary amelanotic malignant melanoma of the female urethra. Int. J. Urol. 2007, 14, 153–155.
- Inoue, M.; Ishioka, J.-I.; Kageyama, Y.; Fukuda, H.; Higashi, Y. Primary malignant melanoma of the male urethra: A case report. Hinyokika Kiyo Acta Urol. Jpn. 2008, 54, 305–308.
- Comploj, E.; Palermo, S.; Trenti, E.; Lodde, M.; Mian, C.; Carella, R.; Pycha, A. Unexpected Long Survival in Primary Malignant Melanoma of the Male Urethra. Case Rep. Dermatol. 2009, 1, 93–99.
- Akbas, A.; Akman, T.; Erdem, M.R.; Antar, B.; Kilicaslan, I.; Şinasi, Y.Ö. Female Urethral Malignant Melanoma with Vesical Invasion: A Case Report. Kaohsiung J. Med. Sci. 2010, 26, 96–98.
- Yoshii, T.; Horiguchi, A.; Shirotake, S.; Tobe, M.; Tasaki, S.; Hayakawa, M.; Sumitomo, M.; Asano, T. A case of primary amelanotic malignant melanoma of the female urethra. Jpn. J. Urol. 2010, 101, 734–737.
- Cho, S.T.; Song, H.C.; Cho, B.; Choi, W.S.; Lee, W.K.; Lee, Y.S.; Lee, Y.G.; Kim, K.K.; Park, S.-H.; Kim, J.W. Primary Malignant Melanoma of the Female Urethra. Korean J. Urol. 2012, 53, 206–208.
- Karaman, H.; Yesil, Y. Primary melanoma of the male urethra. Turk. J. Urol. 2014, 39, 201–203.
- Maruyama, T.; Matsui, T.; Kobayashi, Y.; Kuwae, H. Case of primary malignant melanoma of the female urethra at age 94: A case report. Hinyokika Kiyo Acta Urol. Jpn. 2014, 60, 571–574.
- Papeš, D.; Altarac, S.; Arslani, N.; Rajković, Z.; Antabak, A.; Ćaćić, M. Melanoma of the glans penis and urethra. Urology 2014, 83, 6–11.
- Li, Y.; Yuan, H.; Wang, A.; Zhang, Z.; Wu, J.; Wei, Q. Malignant melanoma of the penis and urethra: One case report. World J. Surg. Oncol. 2014, 12, 340.
- Pandey, P.K.; Vijay, M.K.; Goel, H.; Shukla, S. Primary malignant melanoma of female urethra: A rare neoplasm. J. Cancer Res. Ther. 2014, 10, 758–760.
- Broussard, A.P.; Chaudoir, C.; Gomelsky, A. Urethral melanoma in an elderly woman. Int. Urogynecol. J. 2014, 26, 149–150.
- Safadi, A.; Schwalb, S.; Ben-Shachar, I.; Katz, R. Primary malignant urethral melanoma resembling a urethral caruncle. Urol. Case Rep. 2017, 15, 28–29.
- Suzuki, H.; Nakanishi, Y.; Yoshino, K.; Kataoka, M.; Fukushima, H.; Tobisu, K.; Koga, F. Primary malignant melanoma of the female urethra: A case report. Jpn. J. Urol. 2018, 109, 111–115.
- Davuluri, M.; Long, B.; Semple, S.; Villanueva-Siles, E.; Aboumohamed, A. Primary Urethral Melanoma: A Case Report and Literature Review. Urology 2018, 126, 1–4.
- Aoki, Y.; Soma, T.; Nakamura, Y.; Fukui, N.; Sakai, Y.; Kageyama, Y. Malignant melanoma of the male urethra with increased 5-S-cysteinyldopa: A case report. IJU Case Rep. 2019, 2, 215–217.
- Tokita, T.; Kawahara, T.; Ito, Y.; Tsutsumi, S.; Abe, K.; Namura, K.; Sano, F.; Shioi, K.; Takamoto, D.; Yumura, Y.; et al. Primary amelanotic malignant melanoma of the male urethra with inguinal lymph node metastasis successfully controlled by nivolumab: A case report. Urol. Case Rep. 2018, 18, 54–56.
- Maruyama, Y.; Sadahira, T.; Mitsui, Y.; Wada, K.; Tanimoto, R.; Kobayashi, Y.; Araki, M.; Watanabe, M.; Watanabe, T.; Nasu, Y. Red nodular melanoma of the penile foreskin: A case report and literature review. Mol. Clin. Oncol. 2018, 9, 449–452.
- Bansal, N.; Garg, G.; Vashist, S. Primary malignant melanoma of urethra mimicking as urethral caruncle. BMJ Case Rep. 2018, 2018, bcr2018226056.
- El-Safadi, S.; Estel, R.; Mayser, P.; Muenstedt, K. Primary malignant melanoma of the urethra: A systematic analysis of the current literature. Arch. Gynecol. Obstet. 2013, 289, 935–943.
- McComiskey, M.; Iavazzo, C.; Datta, M.; Slade, R.; Winter-Roach, B.; Lambe, G.; Sangar, V.K.; Smith, M. Balloon Cell Urethral Melanoma: Differential Diagnosis and Management. Case Rep. Obstet. Gynecol. 2015, 2015, 919584.
- Fahmy, O.; Scharpf, M.; Fend, F.; Stenzl, A.; Gakis, G. Feasibility of Penis-Preserving Surgery for Urethral Melanoma: Proposal for a Therapeutic Algorithm. Clin. Genitourin. Cancer 2015, 13, e411–e413.
- Sandru, F.; Draghici, C.; Predescu, T.; Constantin, M.M.; Petca, R.-C.; Constantin, T.; Petca, A.; Dumitrașcu, M.C. Regressive melanoma in a female patient: A case report. Exp. Ther. Med. 2020, 20, 87–90.
- Nakra, T.; Dadhwal, R.; Nayyar, R.; Rastogi, S.; Kakkar, A.; Sharma, M.C.; Yadav, R. Primary urethral small cell melanoma with neuroendocrine differentiation: A case report. J. Egypt. Natl. Cancer Inst. 2020, 32, 40.
- Burity, C.R.T.; Linica, S.B.; Saade, R.D.; Ferreira, F.T.; Schultz, L.; Bezerra, E.S.; Franco, H.C.; Oliveira, R.A.; Costa, M.V.S. Lo-calized primary melanoma of male urethra with a 4-year follow up. Urol. Case Rep. 2021, 10, 101702.
- Smith, H.G.; Bagwan, I.; Board, R.E.; Capper, S.; Coupland, S.E.; Glen, J.; Lalondrelle, S.; Mayberry, A.; Muneer, A.; Nugent, K.; et al. Ano-uro-genital mucosal melanoma UK national guidelines. Eur. J. Cancer 2020, 135, 22–30.
More
Information
Subjects:
Oncology
Contributor
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.1K
Revisions:
2 times
(View History)
Update Date:
08 Sep 2021
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No