Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Madalina La Rocca | -- | 1610 | 2023-12-13 10:04:53 | | | |
| 2 | Catherine Yang | Meta information modification | 1610 | 2023-12-14 02:09:18 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
La Rocca, M.; Leonardi, B.F.; Lo Greco, M.C.; Marano, G.; Finocchiaro, I.; Iudica, A.; Milazzotto, R.; Liardo, R.L.E.; La Monaca, V.A.; Salamone, V.; et al. Radiotherapy of Orbital and Ocular Adnexa Lymphoma. Encyclopedia. Available online: https://encyclopedia.pub/entry/52673 (accessed on 03 July 2026).
La Rocca M, Leonardi BF, Lo Greco MC, Marano G, Finocchiaro I, Iudica A, et al. Radiotherapy of Orbital and Ocular Adnexa Lymphoma. Encyclopedia. Available at: https://encyclopedia.pub/entry/52673. Accessed July 03, 2026.
La Rocca, Madalina, Barbara Francesca Leonardi, Maria Chiara Lo Greco, Giorgia Marano, Irene Finocchiaro, Arianna Iudica, Roberto Milazzotto, Rocco Luca Emanuele Liardo, Viviana Anna La Monaca, Vincenzo Salamone, et al. "Radiotherapy of Orbital and Ocular Adnexa Lymphoma" Encyclopedia, https://encyclopedia.pub/entry/52673 (accessed July 03, 2026).
La Rocca, M., Leonardi, B.F., Lo Greco, M.C., Marano, G., Finocchiaro, I., Iudica, A., Milazzotto, R., Liardo, R.L.E., La Monaca, V.A., Salamone, V., Basile, A., Foti, P.V., Palmucci, S., David, E., Parisi, S., Pontoriero, A., Pergolizzi, S., & Spatola, C. (2023, December 13). Radiotherapy of Orbital and Ocular Adnexa Lymphoma. In Encyclopedia. https://encyclopedia.pub/entry/52673
La Rocca, Madalina, et al. "Radiotherapy of Orbital and Ocular Adnexa Lymphoma." Encyclopedia. Web. 13 December, 2023.
Copy Citation
Orbital and ocular adnexa lymphomas are rare neoplasms confined to the orbital region. The prognosis is generally favorable, with a high proportion of localized disease, indolent clinical course, prolonged disease-free intervals, and low lymphoma-related mortality rate.
orbital tumors
lymphoma
ocular oncology
radiation oncology
1. Introduction
Orbital and ocular adnexa lymphomas (OOAL) are a rare localization of lymphomas confined to the orbital region, accounting for approximately 7–8% of all non-Hodgkin’s lymphomas (NHLs) [1][2]. These neoplasms develop from B-lymphocytes, T-lymphocytes, or NK lymphocytic cells [3][4]. It is recognizable by its morphological heterogeneous appearance with variable presence of germinal centers, plasma cells, and/or monocytic lymphocytes [4]. Within the NHLs, histological subtypes can be divided into indolent or low-grade lymphoma (i.e., extranodal marginal zone lymphoma (EMZL)) involving mucosa-associated lymphoid tissue (MALT), follicular lymphoma (FL) or lymphoplasmacytic lymphoma) and aggressive or high-grade lymphomas (e.g., diffuse large B-cell lymphoma (DLBCL) or mantle-cell lymphoma (MCL)) with different patterns of response to local and systemic treatment, local or distant recurrence [5][6]. An 80% of lymphomas involving ocular adnexa (conjunctiva, orbit, lacrimal gland, and eyelid) have mature B-cell origin [4] as a response to persistent antigenic stimulation in case of chronic inflammatory or autoimmune disorders [7]. Association with C. psittaci infection is also documented, especially in Eastern nations, even if there is no overall acceptance [8][9]. These types of lesions must be distinguished from intraocular lymphoma, a subtype of primary central nervous system lymphoma that represents a high-grade process with a distinct therapeutic strategy, but is not the subject of this review [10]. Lymphoma occurs predominantly in elder individuals [11] with an incidence peak amongst the fifth and seventh decade of life (median age ∼65 years), with a female predominance (male/female = 1:1.5/2) in the Western population. In contrast, a Korean study by Cho et al. revealed a significantly younger age at diagnosis (median age of 46 y/o), with a male predominance [11]. Ucgul et al. reported the rarity of this pathology in the pediatric population [12]. Treatment may include radiotherapy (RT), chemotherapy (CHT), immunomodulating therapy, primary antibiotic treatment, surgical excision, or combination therapy. The choice of treatment depends on a variety of factors: histopathologic type, systemic staging at the initial presentation, and patient comorbidities. When in the early stage, radiotherapy alone is the curative option in patients diagnosed with indolent lymphoma to achieve high response rates with manageable toxicity [13][14].
2. Treatment Options
Various strategies of treatment are available depending on the initial stage of the neoplasm: surgical excision, radiotherapy, chemotherapy, anti-chlamydial antibiotic (doxycycline and clarithromycin) [7][9], and immunomodulating therapy or combination therapy. Tailoring the treatment requires a multidisciplinary approach which should consider extensions, patient comorbidities, disease-related prognostic factors, short and long-term efficacy, and toxicities impact on a patient’s quality of life [7]. Radiotherapy alone is usually the treatment of choice, in early stage and indolent OOAL (stage I–IIE) [15]. Patients with stage III or IV or with aggressive OOAL’s histotypes need a systemic treatment chemotherapy/immunotherapy combined with local radiotherapy [16]. However, no prospective clinical trials have been conducted to evaluate these therapeutic options or define the optimal treatment approach for these patients. Radiotherapy and non-radiotherapy therapeutic options are summarized in detail in Figure 1.
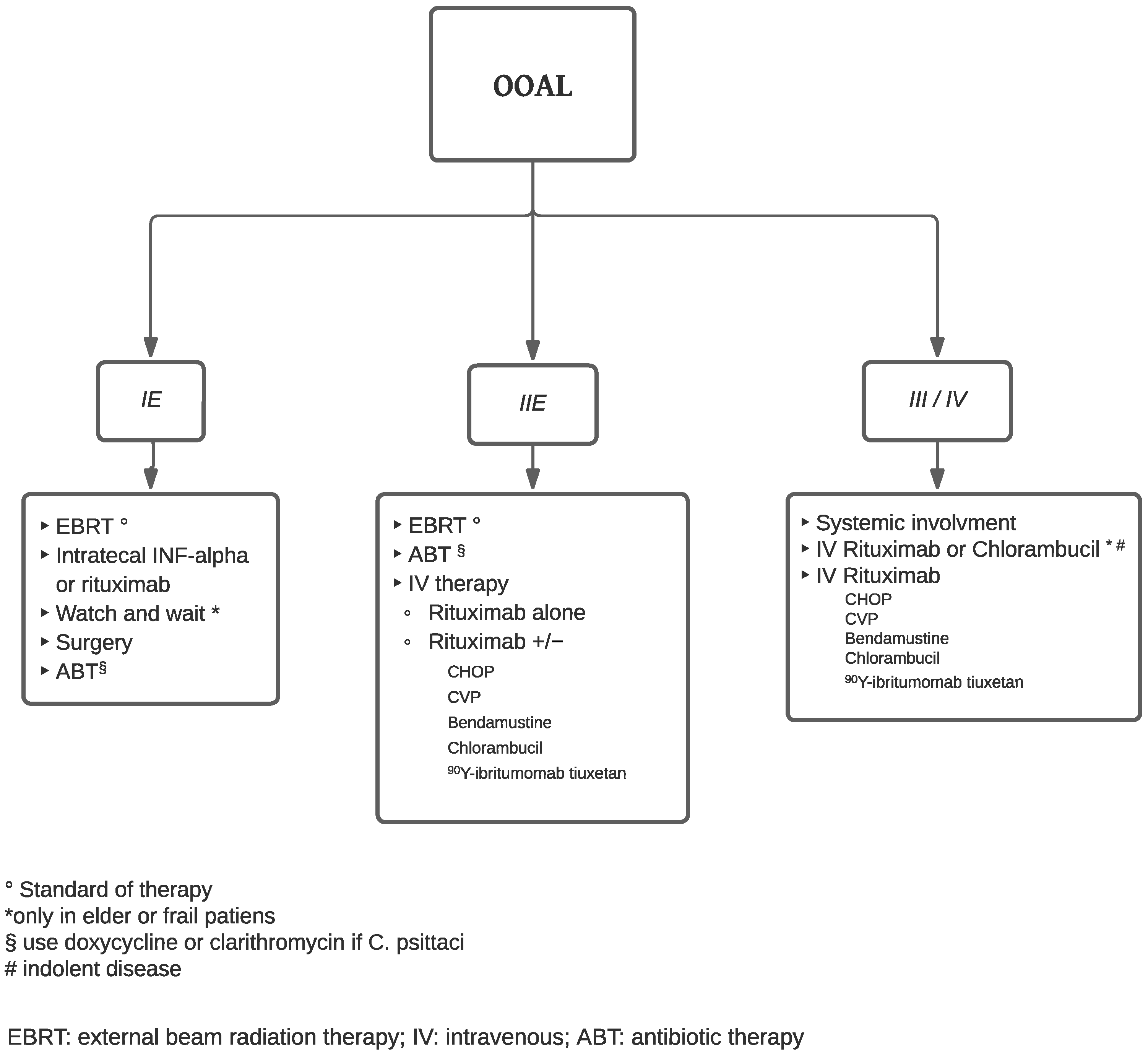
Figure 1. Flow chart of treatment.
2.1. Non-Radiotherapy Treatment Options
“Watch and wait” is not recommended due to the high incidence of local and systemic recurrence, but it can be taken under consideration in the setting of frail elderly patients with low-grade, asymptomatic, and unilateral disease with severe comorbidities that preclude other and more aggressive therapeutic approaches [17][18]. Surgical resection may be used to treat small or encapsulated tumors (e.g., conjunctival and lacrimal gland tumors). However, surgery alone showed a high risk of recurrence if not associated with adjuvant chemotherapy or radiotherapy [19]. In case of aggressive histological subtypes (i.e., MCL, DLBCL, T-cell lymphoma), bilateral disease, high-risk of local or distant relapse, chemotherapy regimen containing cyclophosphamide (CHOP (cyclophosphamide, adriamycin, vincristine, prednisone), COP/CVP (cyclophosphamide, vincristine, prednisone), C-MOPP (cyclophosphamide, vincristine, procarbazine, prednisone), and schemes containing Chlorambucil or Bendamustine can be taken under consideration with or without radiotherapy [20][21][22][23]. If infection with C. psittaci is detected, especially in Eastern countries, antibiotics, such as Doxycycline, can be used [7][8][9]. Interferon-alpha (INF-α) is an option for OOAL localized in the conjunctiva or the lacrimal glands. This glycoprotein has already been used in other neoplasm treatments, which possess antiviral, antiproliferative, and immunomodulatory functions (i.e., apoptosis, producing tumor suppressor gene p53, inhibition of tumoral neo angiogenesis). Cellini et al. and Holds et al. documented the successful use of intralesional INF-α in the treatment of conjunctival lymphoma [24][25]. Generally, 1 million IU of INF-α are administrated weekly, with optimal local control rate. INF-α showed low toxicity, and in general, no significant local side effects after injection. Rituximab is a monoclonal chimeric anti-CD20 antibody that targets the surface antigen CD20, overexpressed on CD20-positive NHL B cells. It can be administered intralesionally in case of recurrence and local relapse [26] or intravenously for bilateral or systemic involvement [27]. As previously mentioned, it can be used alone or in combination with other chemotherapy drugs. Monoclonal antibodies can be used to deliver radioisotopes to the site of OOAL [7], with the same or better outcome compared to rituximab. Esmaeli et al., in their study, promoted a protocol where Yttrium 90-ibritumomab tiuxetan (Zevalin®, IDEC Pharmaceuticals Corporation, San Diego, California), a radiolabeled anti-CD20 monoclonal antibody, is administrated after 2 weekly intravenous rituximab 250 mg/mq [28].
2.2. Radiotherapy Treatment Options
OOALs are characterized by high radiosensitivity [29][30]. External beam radiation therapy (EBRT) is the gold standard treatment in OOAL classified as Ann Arbor Stage IE-IIE thanks to high response rates and outstanding local control [31]. Radiotherapy can be administrated as a solo treatment, with adjuvant systemic therapy, or as salvage therapy after partial or incomplete response or in case of relapse [32]. Clinical exams to evaluate the extension of orbital disease is utilized for radiotherapy plans. A review of a CT scans, MRI and/or PET scans are utilized when available in order to create a deformable fusion. The gross tumor volume (GTV) includes the tumor extent, and the clinical target volume (CTV) includes the entire GTV plus an adequate margin to fully encompass the anatomical region involving the mass. The planning target volume (PTV) includes CTV with a 10 mm to 15 mm margin [30][33]. A bolus is positioned on the skin to facilitate the superficialization of the dose, especially when palpebral skin is involved. Different particles can be adapted to deliver the dose: electrons, photons, and protons. An electron beam can be used for superficial lymphomas of the eyelid and/or conjunctiva that do not infiltrate the ocular bulb. Electron energies typically cover the entire orbit. For patients with superficial disease limited to the eyelids or conjunctiva, treatment is generally delivered using electron beams (6–12 MeV) with or without bolus to provide optimal surface dose coverage. Deeper lesions are generally treated with higher energy electron beams (9–16 MeV) or photon beams (4–6 MV) [34][35]. The photon beam has been used widely for deeper lesions involving lacrimal glands, orbital soft tissue, muscles, or for bulky mass that extends beyond the globe equator. Proton beam therapy (PBT) is a valid option for the treatment of most ocular and periorbital malignancies (e.g., melanomas, lymphomas, squamous cell carcinomas, rhabdomyosarcoma hemangioma, metastases of solid tumors) with excellent control rates [35][36][37][38][39]. Compared with conventional photon radiotherapy, PBT uses heavier subatomic particles to deliver energy with higher accuracy, conformal treatment isodoses without dose fall-off and with less scattering to the healthy surrounding tissues. Proton beams are generated by a cyclotron or synchrotron and then accelerated to proper target energy [40][41]. The proton dose distribution that may be achieved is generally superior to the dose distribution of conventional photon radiotherapy. PBT may improve the survival rate of patients by improving the local tumor treatment rate, sparing adjacent tissues and lowering collateral damage. Cirrone et al. performed a study on 4 patients with orbital non-Hodgkin lymphoma ranging between 30 and 48 Gy [RBE], with 4 fractions on 4 consecutive days [37]. Nonetheless, due to the high treatment costs for facility building and maintenance, PBT is not very diffuse. Despite the consensus on the primary role of radiotherapy, there is no universally accepted optimal radiation dose and fractionation for patients with OOAL [15]. Historically, patients have received treatment with conventional doses of 24–36 Gy with local control rates >95% and a minimum dose required of 25 Gy [6][16][42][43] Le et al. found no differences in terms of distant progression-free survival (dPFS) or local recurrence (LR) after EBRT in pts with ≤34 Gy compared with higher doses; the only difference was the increase in local toxicities observed [43]. Bhatia et al. [44] and Letschert et al. [45] treated low-grade with a median dose of 30 Gy and intermediate to high-grade tumors with a median dose of 40 Gy.
3. Treatment Toxicity
Treatment-independent factors, especially in elderly patients, must be considered (i.e., diabetes, glaucoma, sicca syndrome, Sjögren syndrome) because they may influence cataract development. Most patients experienced mild acute toxicities, such as skin erythema in the periorbital area, conjunctival hyperemia, chemosis, swelling, and excessive tearing, during or immediately after the radiotherapy course, which were mainly self-limited or responded to a short course of lubricant gels or skin moisturizers. These symptoms generally resolve in a few months after completion of radiotherapy [32][34]. Long-term toxicities include: radiation-induced cataracts, persistent dry eyes, and iris neovascularization [46][47]. Serious toxicities such as corneal or skin ulceration, telangiectasia, neovascular glaucoma, and radiation retinopathy are extremely rare [48][49]. Radiation-related severe late side-effects incidence increases when patients are treated with RT doses ≥35 Gy, resulting in considerable late toxic effects, including keratitis, severe dry eye syndrome, glaucoma, retinopathy, and cataract formation [16][50][51]. Stafford et al. reported a 52% rate of acute complications with doses ranging from 19 to 48 Gy [50]. Retinal toxicity may result in visual impairment, which can significantly impact quality of life [52][53]. During treatment, shielding, such as a contact lens under the eyelid, can lower the dose for healthy and sensible organs [43][54].
References
- Raderer, M.; Kiesewetter, B.; Ferreri, A.J.M. Clinicopathologic Characteristics and Treatment of Marginal Zone Lymphoma of Mucosa-Associated Lymphoid Tissue (MALT Lymphoma). CA Cancer J. Clin. 2016, 66, 153–171.
- Yen, M.T.; Bilyk, J.R.; Wladis, E.J.; Bradley, E.A.; Mawn, L.A. Treatments for Ocular Adnexal Lymphoma: A Report by the American Academy of Ophthalmology. Ophthalmology 2018, 125, 127–136.
- Olsen, T.G.; Holm, F.; Mikkelsen, L.H.; Rasmussen, P.K.; Coupland, S.E.; Esmaeli, B.; Finger, P.T.; Graue, G.F.; Grossniklaus, H.E.; Honavar, S.G. Orbital Lymphoma-An International Multicenter Retrospective Study. Am. J. Ophthalmol. 2019, 199, 44–57.
- White, V.A. Understanding and Classification of Ocular Lymphomas. Ocul. Oncol. Pathol. 2019, 5, 379–386.
- Ferry, J.A.; Fung, C.Y.; Zukerberg, L.; Lucarelli, M.J.; Hasserjian, R.P.; Preffer, F.I.; Harris, N.L. Lymphoma of the Ocular Adnexa: A Study of 353 Cases. Am. J. Surg. Pathol. 2007, 31, 170–184.
- Fung, C.Y.; Tarbell, N.J.; Lucarelli, M.J.; Goldberg, S.I.; Linggood, R.M.; Harris, N.L.; Ferry, J.A. Ocular Adnexal Lymphoma: Clinical Behavior of Distinct World Health Organization Classification Subtypes. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 1382–1391.
- Stefanovic, A.; Lossos, I.S. Extranodal Marginal Zone Lymphoma of the Ocular Adnexa. Blood 2009, 114, 501–510.
- Ferreri, A.J.M.; Guidoboni, M.; Ponzoni, M.; De Conciliis, C.; Dell’Oro, S.; Fleischhauer, K.; Caggiari, L.; Lettini, A.A.; Dal Cin, E.; Ieri, R. Evidence for an Association between Chlamydia Psittaci and Ocular Adnexal Lymphomas. J. Natl. Cancer Inst. 2004, 96, 586–594.
- Chanudet, E.; Zhou, Y.; Bacon, C.M.; Wotherspoon, A.C.; Müller-Hermelink, H.-K.; Adam, P.; Dong, H.Y.; de Jong, D.; Li, Y.; Wei, R. Chlamydia Psittaci Is Variably Associated with Ocular Adnexal MALT Lymphoma in Different Geographical Regions. J. Pathol. 2006, 209, 344–351.
- Ferreri, A.J.M.; Blay, J.Y.; Reni, M.; Pasini, F.; Gubkin, A.; Tirelli, U.; Calderoni, A.; Zucca, E.; Cortelazzo, S.; Chassagne, C.; et al. Relevance of Intraocular Involvement in the Management of Primary Central Nervous System Lymphomas. Ann. Oncol. 2002, 13, 531–538.
- Shields, J.A.; Shields, C.L.; Scartozzi, R. Survey of 1264 Patients with Orbital Tumors and Simulating Lesions: The 2002 Montgomery Lecture, Part 1. Ophthalmology 2004, 111, 997–1008.
- Ucgul, A.Y.; Tarlan, B.; Gocun, P.U.; Konuk, O. Primary Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma of the Lacrimal Drainage System in Two Pediatric Patients. Eur. J. Ophthalmol. 2020, 30, NP18–NP23.
- Fakhrian, K.; Klemm, S.; Keller, U.; Bayer, C.; Riedl, W.; Molls, M.; Geinitz, H. Radiotherapy in Stage I-III Follicular Non-Hodgkin Lymphoma. Retrospective Analysis of a Series of 50 Patients. Strahlenther. Onkol. 2012, 188, 464–470.
- Heinzelmann, F.; Engelhard, M.; Ottinger, H.; Bamberg, M.; Weinmann, M. Nodal Follicular Lymphoma: The Role of Radiotherapy for Stages I and II. Strahlenther. Onkol. 2010, 186, 191–196.
- Yahalom, J.; Illidge, T.; Specht, L.; Hoppe, R.T.; Li, Y.-X.; Tsang, R.; Wirth, A. Modern Radiation Therapy for Extranodal Lymphomas: Field and Dose Guidelines From the International Lymphoma Radiation Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 11–31.
- König, L.; Stade, R.; Rieber, J.; Debus, J.; Herfarth, K. Radiotherapy of Indolent Orbital Lymphomas: Two Radiation Concepts. Strahlenther. Onkol. 2016, 192, 414–421.
- Tanimoto, K.; Kaneko, A.; Suzuki, S.; Sekiguchi, N.; Maruyama, D.; Kim, S.W.; Watanabe, T.; Kobayashi, Y.; Kagami, Y.; Maeshima, A.; et al. Long-Term Follow-up Results of No Initial Therapy for Ocular Adnexal MALT Lymphoma. Ann. Oncol. 2006, 17, 135–140.
- Mannami, T.; Yoshino, T.; Oshima, K.; Takase, S.; Kondo, E.; Ohara, N.; Nakagawa, H.; Ohtsuki, H.; Harada, M.; Akagi, T. Clinical, Histopathological, and Immunogenetic Analysis of Ocular Adnexal Lymphoproliferative Disorders: Characterization of Malt Lymphoma and Reactive Lymphoid Hyperplasia. Mod. Pathol. 2001, 14, 641–649.
- Cho, E.Y.; Han, J.J.; Ree, H.J.; Ko, Y.H.; Kang, Y.; Ahn, H.S.; Ahn, S.D.; Park, C.J.; Huh, J. Clinicopathologic Analysis of Ocular Adnexal Lymphomas: Extranodal Marginal Zone b-Cell Lymphoma Constitutes the Vast Majority of Ocular Lymphomas among Koreans and Affects Younger Patients. Am. J. Hematol. 2003, 73, 87–96.
- Song, E.-K.; Kim, S.-Y.; Kim, T.M.; Lee, K.-W.; Yun, T.; Na, I.-I.; Shin, H.; Lee, S.H.; Kim, D.W.; Khwarg, S.I. Efficacy of Chemotherapy as a First-Line Treatment in Ocular Adnexal Extranodal Marginal Zone B-Cell Lymphoma. Ann. Oncol. 2008, 19, 242–246.
- Mikkelsen, L.H.; Würtz, N.S.; Heegaard, S. Recent Advances in Treating Extra-Ocular Lymphomas. Expert. Rev. Ophthalmol. 2018, 13, 205–217.
- Tsai, P.S.; Colby, K.A. Treatment of Conjunctival Lymphomas. Semin. Ophthalmol. 2005, 20, 239–246.
- Martin, P.; Chen, Z.; Cheson, B.D.; Robinson, K.S.; Williams, M.; Rajguru, S.A.; Friedberg, J.W.; van der Jagt, R.H.; LaCasce, A.S.; Joyce, R. Long-Term Outcomes, Secondary Malignancies and Stem Cell Collection Following Bendamustine in Patients with Previously Treated Non-Hodgkin Lymphoma. Br. J. Haematol. 2017, 178, 250–256.
- Cellini, M.; Possati, G.L.; Puddu, P.; Caramazza, R. Interferon Alpha in the Therapy of Conjunctival Lymphoma in An Hiv+ Patient. Eur. J. Ophthalmol. 1996, 6, 475–477.
- Holds, J.; Buchanan, A.; Hanson, R. Intralesional Interferon-α for the Treatment of Bilateral Conjunctival Mucosa-associated Lymphoid Tissue Lymphoma. Pediatr. Blood Cancer 2012, 59, 176–178.
- Laurenti, L.; De Padua, L.; Battendieri, R.; Tarnani, M.; Sica, S.; Blasi, M.A.; Savino, G.; Leone, G. Intralesional Administration of Rituximab for Treatment of CD20 Positive Orbital Lymphoma: Safety and Efficacy Evaluation. Leuk. Res. 2011, 35, 682–684.
- Cvetković, R.S.; Perry, C.M. Rituximab: A Review of Its Use in Non-Hodgkin’s Lymphoma and Chronic Lymphocytic Leukaemia. Drugs 2006, 66, 791–820.
- Esmaeli, B.; Murray, J.L.; Ahmadi, M.A.; Naderi, A.; Singh, S.; Romaguera, J.; White, C.A.; McLaughlin, P. Immunotherapy for Low-Grade Non-Hodgkin Secondary Lymphoma of the Orbit. Arch. Ophthalmol. 2002, 120, 1225–1227.
- Russo, A.L.; Chen, Y.-H.; Martin, N.E.; Vinjamoori, A.; Luthy, S.K.; Freedman, A.; Michaelson, E.M.; Silver, B.; Mauch, P.M.; Ng, A.K. Low-Dose Involved-Field Radiation in the Treatment of Non-Hodgkin Lymphoma: Predictors of Response and Treatment Failure. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 121–127.
- Fasola, C.E.; Jones, J.C.; Huang, D.D.; Le, Q.-T.; Hoppe, R.T.; Donaldson, S.S. Low-Dose Radiation Therapy (2 Gy × 2) in the Treatment of Orbital Lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 930–935.
- Kharod, S.M.; Herman, M.P.; Morris, C.G.; Lightsey, J.; Mendenhall, W.M.; Mendenhall, N.P. Radiotherapy in the Management of Orbital Lymphoma: A Single Institution’s Experience Over 4 Decades. Am. J. Clin. Oncol. 2018, 41, 100–106.
- Goda, J.S.; Le, L.W.; Lapperriere, N.J.; Millar, B.-A.; Payne, D.; Gospodarowicz, M.K.; Wells, W.; Hodgson, D.C.; Sun, A.; Simpson, R. Localized Orbital Mucosa-Associated Lymphoma Tissue Lymphoma Managed with Primary Radiation Therapy: Efficacy and Toxicity. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, e659–e666.
- Ohga, S.; Nakamura, K.; Shioyama, Y.; Sasaki, T.; Yamaguchi, T.; Yoshitake, T.; Terashima, K.; Asai, K.; Matsumoto, K.; Honda, H. Treatment Outcome of Radiotherapy for Localized Primary Ocular Adnexal MALT Lymphoma—Prognostic Effect of the AJCC Tumor-Node-Metastasis Clinical Staging System. Anticancer Res. 2015, 35, 3591–3597.
- Pereira-Da Silva, M.V.; Di Nicola, M.L.; Altomare, F.; Xu, W.; Tsang, R.; Laperriere, N.; Krema, H. Radiation Therapy for Primary Orbital and Ocular Adnexal Lymphoma. Clin. Transl. Radiat. Oncol. 2023, 38, 15–20.
- Spatola, C.; Privitera, G. Clinical aspects and potential clinical applications of laser accelerated proton beams. In Proceedings of the 2nd Elimed Workshop and Panel, Catania, Italy, 18–19 October 2012; AIP Publishing: Melville, NY, USA, 2013; Volume 1546, pp. 108–111.
- Regmi, R.; Maes, D.; Nevitt, A.; Toltz, A.; Leuro, E.; Chen, J.; Halasz, L.; Rengan, R.; Bloch, C.; Saini, J. Treatment of Ocular Tumors through a Novel Applicator on a Conventional Proton Pencil Beam Scanning Beamline. Sci. Rep. 2022, 12, 4648.
- Cirrone, G.A.P.; Cuttone, G.; Raffaele, L.; Salamone, V.; Avitabile, T.; Privitera, G.; Spatola, C.; Amico, A.G.; Larosa, G.; Leanza, R.; et al. Clinical and Research Activities at the CATANA Facility of INFN-LNS: From the Conventional Hadrontherapy to the Laser-Driven Approach. Front. Oncol. 2017, 7, 223.
- Spatola, C.; Liardo, R.L.E.; Milazzotto, R.; Raffaele, L.; Salamone, V.; Basile, A.; Foti, P.V.; Palmucci, S.; Cirrone, G.A.P.; Cuttone, G.; et al. Radiotherapy of Conjunctival Melanoma: Role and Challenges of Brachytherapy, Photon-Beam and Protontherapy. Appl. Sci. 2020, 10, 9071.
- Milazzotto, R.; Liardo, R.L.E.; Privitera, G.; Raffaele, L.; Salamone, V.; Arena, F.; Pergolizzi, S.; Cuttone, G.; Cirrone, G.A.P.; Russo, A.; et al. Proton Beam Radiotherapy of Locally Advanced or Recurrent Conjunctival Squamous Cell Carcinoma: Experience of the CATANA Centre. J. Radiother. Pr. 2022, 21, 97–104.
- Tian, X.; Liu, K.; Hou, Y.; Cheng, J.; Zhang, J. The Evolution of Proton Beam Therapy: Current and Future Status (Review). Mol. Clin. Oncol. 2017, 8, 15–21.
- Tocco, A. Porocarcinoma Of The Eyelid Treated With Proton Beam Radiotherapy: Case Report And Literature Review. Acta Medica Mediterr. 2018, 709–712.
- Bolek, T.W.; Moyses, H.M.; Marcus, R.B.; Gorden, L.; Maiese, R.L.; Almasri, N.M.; Mendenhall, N.P. Radiotherapy in the Management of Orbital Lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 31–36.
- Le, Q.T.; Eulau, S.M.; George, T.I.; Hildebrand, R.; Warnke, R.A.; Donaldson, S.S.; Hoppe, R.T. Primary Radiotherapy for Localized Orbital MALT Lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 657–663.
- Bhatia, S.; Paulino, A.C.; Buatti, J.M.; Mayr, N.A.; Wen, B.-C. Curative Radiotherapy for Primary Orbital Lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 818–823.
- Letschert, J.G.; González González, D.; Oskam, J.; Koornneef, L.; van Dijk, J.D.; Boukes, R.; Bras, J.; van Heerde, P.; Bartelink, H. Results of Radiotherapy in Patients with Stage I Orbital Non-Hodgkin’s Lymphoma. Radiother. Oncol. 1991, 22, 36–44.
- Kim, S.E.; Yang, H.J.; Yang, S.-W. Effects of Radiation Therapy on the Meibomian Glands and Dry Eye in Patients with Ocular Adnexal Mucosa-Associated Lymphoid Tissue Lymphoma. BMC Ophthalmol. 2020, 20, 24.
- Xu, L.; Tang, X.; Jiang, N.; Zhang, S.; Cao, Y.; Sun, X. Radiation Therapy Efficacy and Toxicity for Orbital and Ocular Adnexal Mucosa-Associated Lymphoid Tissue (OAMALT): A Single-Center, Retrospective Study of 32 Cases. CMAR 2021, 13, 8017–8024.
- Ferrufino-Ponce, Z.K.; Henderson, B.A. Radiotherapy and Cataract Formation. Semin. Ophthalmol. 2006, 21, 171–180.
- Ainsbury, E.A.; Bouffler, S.D.; Dörr, W.; Graw, J.; Muirhead, C.R.; Edwards, A.A.; Cooper, J. Radiation Cataractogenesis: A Review of Recent Studies. Radiat. Res. 2009, 172, 1–9.
- Stafford, S.L.; Kozelsky, T.F.; Garrity, J.A.; Kurtin, P.J.; Leavitt, J.A.; Martenson, J.A.; Habermann, T.M. Orbital Lymphoma: Radiotherapy Outcome and Complications. Radiother. Oncol. 2001, 59, 139–144.
- Uno, T.; Isobe, K.; Shikama, N.; Nishikawa, A.; Oguchi, M.; Ueno, N.; Itami, J.; Ohnishi, H.; Mikata, A.; Ito, H. Radiotherapy for Extranodal, Marginal Zone, B-cell Lymphoma of Mucosa-associated Lymphoid Tissue Originating in the Ocular Adnexa: A Multiinstitutional, Retrospective Review of 50 Patients. Cancer 2003, 98, 865–871.
- Pfeffer, M.R.; Rabin, T.; Tsvang, L.; Goffman, J.; Rosen, N.; Symon, Z. Orbital Lymphoma: Is It Necessary to Treat the Entire Orbit? Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 527–530.
- Luthy, S.K.; Ng, A.K.; Silver, B.; Degnan, K.O.; Fisher, D.C.; Freedman, A.S.; Mauch, P.M. Response to Low-Dose Involved-Field Radiotherapy in Patients with Non-Hodgkin’s Lymphoma. Ann. Oncol. 2008, 19, 2043–2047.
- Parikh, R.R.; Moskowitz, B.K.; Maher, E.; Della Rocca, D.; Della Rocca, R.; Culliney, B.; Shapira, I.; Grossbard, M.L.; Harrison, L.B.; Hu, K. Long-Term Outcomes and Patterns of Failure in Orbital Lymphoma Treated with Primary Radiotherapy. Leuk. Lymphoma 2015, 56, 1266–1270.
More
Information
Subjects:
Oncology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
782
Revisions:
2 times
(View History)
Update Date:
14 Dec 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No