 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Zhiyong Zhao | -- | 2782 | 2023-11-15 05:59:40 | | | |
| 2 | Wendy Huang | -2 word(s) | 2780 | 2023-11-15 12:17:48 | | |
Video Upload Options
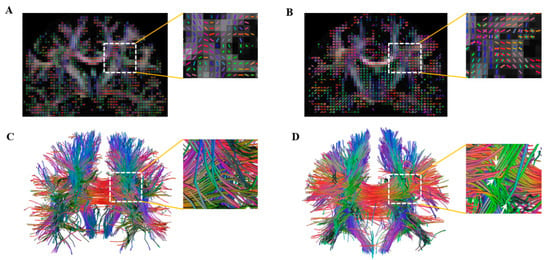
Studies have demonstrated that many regions in the human brain include multidirectional fiber tracts, in which the diffusion of water molecules within image voxels does not follow a Gaussian distribution. Therefore, the conventional diffusion tensor imaging (DTI) that hypothesizes a single fiber orientation within a voxel is intrinsically incapable of revealing the complex microstructures of brain tissues. Diffusion spectrum imaging (DSI) employs a pulse sequence with different b-values along multiple gradient directions to sample the diffusion information of water molecules in the entire q-space and then quantitatively estimates the diffusion profile using a probability density function with a high angular resolution. Studies have suggested that DSI can reliably observe the multidirectional fibers within each voxel and allow fiber tracking along different directions, which can improve fiber reconstruction reflecting the true but complicated brain structures that were not observed in the previous DTI studies. Moreover, with increasing angular resolution, DSI is able to reveal new neuroimaging biomarkers used for disease diagnosis and the prediction of disorder progression. However, this method has not been used widely in clinical studies, due to its overly long scanning time and difficult post-processing.
1. Introduction
2. DSI Tractography for White-Matter Fibers
3. Cortical Parcellation and Connectivity Reconstruction
4. Clinical Applications
4.1. Disease Diagnosis
4.2. Progression Prediction
| First Author (Ref. #) | Type | Subject | Main Findings |
|---|---|---|---|
| Lacerda et al., 2016 [57] | Methodology | Optimization of postprocessing method | This study proposed a new way of including biophysical constraints to compute the ODF, which removed most of the artifacts due to fast diffusion components like those from pathological tissues and offered improved angular resolution. |
| Tian et al., 2019 [58] | Methodology | Optimization of postprocessing method | This study proposed a generalized DSI framework to compute the ensemble average propagator, which could be used to elucidate the contribution and combination of q-space signals to the diffusion ODF. |
| Gilbert et al., 2006 [20] | Application | DSI tractography for white-matter fibers | Diffusion tensor imaging (DTI) depicted the anterior slice of the lingual core in bovine tongue solely as a region with low anisotropy, whereas DSI revealed two different fiber populations with an explicit orthogonal relationship to each other. |
| Dai et al., 2016 [21] | Application | DSI tractography for white-matter fibers | The cingulum bundle was less mature when cat myelination was incomplete, whereas the DTI tractography tended to terminate in such areas. |
| Schmahmann et al., 2007 [22] | Application | DSI tractography for white-matter fibers | This study identified 10 major long association fiber bundles that matched the observations in autoradiographic histological tract tracing in the monkey brain, and such precise structural characteristics were not observed by DTI. |
| Wedeen et al., 2012 [23] | Application | DSI tractography for white-matter fibers | This study first clarified the relationships of adjacency and crossing between cerebral fiber pathways in four nonhuman primate species and humans. |
| Wu et al., 2016 [24]; Wang et al., 2016 [25] |
Application | DSI tractography for white-matter fibers | The DSI revealed a more complete connectivity pattern and anatomical details of the IFOF I-V subcomponents and of the SLF I-III subcomponents. |
| Sun et al., 2018 [26]; Suo et al., 2021 [27]; Liu et al., 2022 [28]; Wei et al., 2017 [29] |
Application | DSI tractography for white-matter fibers | The DSI identified detailed and completed white-matter pathways, including the thalamic–prefrontal peduncle, pyramidal tracts, anterior commissure, and corpus callosum. |
| Sheets et al., 2020, 2021 [30][31] | Application | Cortical parcellation | The DSI segmented the ventral premotor area into four subregions of 6v, 4, 3b, and 3a and the dorsal premotor area into three areas of 6a, 6d, and 6v. |
| Briggs et al., 2021 [32]; Lin et al., 2020 [33] | Application | Cortical connectivity reconstruction | The MFG included two major connections of the superior longitudinal fasciculus and inferior fronto-occipital fasciculus. The ITG connected to five major fibers: the U-fiber, inferior longitudinal fasciculus, vertical occipital fasciculus, arcuate fasciculus, and uncinate fasciculus. |
| Chiang et al., 2020, 2023 [2][36];Tsai et al., 2021 [37] | Application | Attention deficit and hyperactivity disorder (ADHD) | Participants with ADHD showed more rapid development of generalized fractional anisotropy (GFA) in the frontal tracts and showed higher axial diffusivity values in the perpendicular fasciculus, superior longitudinal fasciculus I, corticospinal tract, and corpus callosum compared to the control group. |
| Wen et al., 2020 [45]; Papageorgiou et al., 2021 [46] | Application | Parkinson’s disease (PD) | The PD patients showed impaired global efficiency and characteristic path length in the DSI-based connected network, which were associated with executive function and episodic memory. |
| Wang et al., 2020, 2022 [49][52]; Zhang et al., 2023 [54] | Application | Epilepsy | The AUC of the asymmetric indices of the DSI-derived QA value to the lateralization of epilepsy was 0.96, with 0.91 sensitivity and 0.90 specificity; The AUC of DSI tractography was 0.84, with 100% sensitivity and 75% specificity in discriminating patients with epilepsy from healthy controls. |
| Ni et al., 2020 [48] | Application | Autism spectrum disorder (ASD) | A higher GFA of the tracts was implicated in memory, attention, sensorimotor processing, and perception associated with less dysregulation in TDC but worse dysregulation in ASD. |
| Zhang et al., 2021 [51] | Application | Idiopathic normal-pressure hydrocephalus (iNPH) | The DSI-based QA values of corticospinal tracts (CSTs) in patients with Inph were lower than those in healthy controls (HCs), but such differences in DTI-based FA were observed between iNPH patients and HCs. |
| Liang et al., 2021 [53] | Application | Pituitary adenomas | The DSI parameters also showed a good performance, with an accuracy of 0.83, sensitivity of 0.78, and specificity of 0.86 in discriminating patients with mild and severe visual defects |
| Mao et al., 2022 [54] | Application | Breast cancer | DSI could be helpful for the preoperative prediction of human epidermal growth factor receptor 2 (HER2) in patients with breast cancer, with the findings that the AUC values of DSI quantitative parameters (0.67~0.72) were higher than those of apparent diffusion coefficient (0.57) from DTI. |
| Zhang et al., 2021 [56] | Application | Idiopathic sudden sensorineural hearing loss | The DSI-derived GFA in the ipsilateral medial geniculate body was related to the prognosis (sensitivity = 64.7%; specificity = 85.7%; AUC = 0.796) in patients with unilateral idiopathic sudden sensorineural hearing loss. |
| Paul et al., 2023 [44] | Application | Stroke | This study used DSI to demonstrate for the first time that recovery of basal motor control may be supported via an alternative route through contralesional M1 and non-crossing fibers of the contralesional CST. |
| Salisbury et al., 2023 [40] | Application | First-episode psychosis | White-matter tracts showing associations between QA from DSI and auditory hallucinations were associated with frontal–parietal–temporal connectivity in the cingulum bundle and in the prefrontal interhemispheric connectivity. |
References
- Le Bihan, D.; Iima, M. Diffusion Magnetic Resonance Imaging: What Water Tells Us about Biological Tissues. PLoS Biol. 2015, 13, e1002203.
- Chiang, H.L.; Hsu, Y.C.; Shang, C.Y.; Tseng, W.I.; Gau, S.S. White Matter Endophenotype Candidates for ADHD: A Diffusion Imaging Tractography Study with Sibling Design. Psychol. Med. 2020, 50, 1203–1213.
- Yeh, F.C.; Tang, P.F.; Tseng, W.Y. Diffusion MRI Connectometry Automatically Reveals Affected Fiber Pathways in Individuals with Chronic Stroke. NeuroImage Clin. 2013, 2, 912–921.
- Douglas, D.B.; Iv, M.; Douglas, P.K.; Anderson, A.; Vos, S.B.; Bammer, R.; Zeineh, M.; Wintermark, M. Diffusion Tensor Imaging of TBI: Potentials and Challenges. Top. Magn. Reson. Imaging 2015, 24, 241–251.
- Jeurissen, B.; Leemans, A.; Tournier, J.D.; Jones, D.K.; Sijbers, J. Investigating the Prevalence of Complex Fiber Configurations in White Matter Tissue with Diffusion Magnetic Resonance Imaging. Hum. Brain Mapp. 2013, 34, 2747–2766.
- Raffelt, D.A.; Smith, R.E.; Ridgway, G.R.; Tournier, J.-D.; Vaughan, D.N.; Rose, S.; Henderson, R.; Connelly, A. Connectivity-Based Fixel Enhancement: Whole-Brain Statistical Analysis of Diffusion MRI Measures in the Presence of Crossing Fibres. NeuroImage 2015, 117, 40–55.
- Voskuilen, L.; Mazzoli, V.; Oudeman, J.; Balm, A.J.; van der Heijden, F.; Froeling, M.; de Win, M.M.; Strijkers, G.J.; Smeele, L.E.; Nederveen, A.J. Crossing Muscle Fibers of the Human Tongue Resolved In Vivo Using Constrained Spherical Deconvolution. J. Magn. Reson. Imaging 2019, 50, 96–105.
- Sid, F.A.; Abed-Meraim, K.; Harba, R.; Oulebsir-Boumghar, F. Analytical Performance Bounds for Multi-Tensor Diffusion-MRI. Magn. Reson. Imaging 2017, 36, 146–158.
- Rosenkrantz, A.B.; Padhani, A.R.; Chenevert, T.L.; Koh, D.M.; De Keyzer, F.; Taouli, B.; Le Bihan, D. Body Diffusion Kurtosis Imaging: Basic Principles, Applications, and Considerations For Clinical Practice. J. Magn. Reson. Imaging 2015, 42, 1190–1202.
- Kamiya, K.; Hori, M.; Aoki, S. Noddi in Clinical Research. J. Neurosci. Methods 2020, 346, 108908.
- Afzali, M.; Nilsson, M.; Palombo, M.; Jones, D.K. Spheriously? The Challenges of Estimating Sphere Radius Non-Invasively in the Human Brain from Diffusion MRI. NeuroImage 2021, 237, 118183.
- Schilling, K.G.; Janve, V.; Gao, Y.; Stepniewska, I.; Landman, B.A.; Anderson, A.W. Histological Validation of Diffusion MRI Fiber Orientation Distributions and Dispersion. NeuroImage 2018, 165, 200–221.
- Hsu, Y.C.; Lo, Y.C.; Chen, Y.J.; Wedeen, V.J.; Isaac Tseng, W.Y. NTU-DSI-122: A Diffusion Spectrum Imaging Template with High Anatomical Matching to the ICBM-152 Space. Hum. Brain Mapp. 2015, 36, 3528–3541.
- Jensen, J.H.; Glenn, G.R.; Helpern, J.A. Fiber Ball Imaging. NeuroImage 2016, 124, 824–833.
- Andersson, J.L.; Sotiropoulos, S.N. Non-Parametric Representation and Prediction of Single-and Multi-Shell Diffusion-Weighted MRI Data Using Gaussian Processes. NeuroImage 2015, 122, 166–176.
- Chen, V.C.-H.; Chuang, W.; Chen, C.-W.; Tsai, Y.-H.; McIntyre, R.S.; Weng, J.-C. Detecting Microstructural Alterations of Cerebral White Matter Associated with Breast Cancer and Chemotherapy Revealed by Generalized q-Sampling MRI. Front. Psychiatry 2023, 14, 1161246.
- Wedeen, V.J.; Reese, T.G.; Tuch, D.S.; Weigel, M.R.; Dou, J.G.; Weiskoff, R.M.; Chessler, D. Mapping fiber orientation spectra in cerebral white matter with Fourier-transform diffusion MRI. In Proceedings of the 8th Annual Meeting of ISMRM, Denver, CO, USA, 3–7 April 2000; p. 82.
- Tuch, D.S. Q-Ball Imaging. Magn. Reson. Med. 2004, 52, 1358–1372.
- Daducci, A.; Canales-Rodríguez, E.J.; Descoteaux, M.; Garyfallidis, E.; Gur, Y.; Lin, Y.C.; Mani, M.; Merlet, S.; Paquette, M.; Ramirez-Manzanares, A.; et al. Quantitative Comparison of Reconstruction Methods for Intra-Voxel Fiber Recovery from Diffusion MRI. IEEE Trans. Med. Imaging 2014, 33, 384–399.
- Gilbert, R.J.; Magnusson, L.H.; Napadow, V.J.; Benner, T.; Wang, R.; Wedeen, V.J. Mapping Complex Myoarchitecture in the Bovine Tongue with Diffusion-Spectrum Magnetic Resonance Imaging. Biophys. J. 2006, 91, 1014–1022.
- Dai, G.; Das, A.; Hayashi, E.; Chen, Q.; Takahashi, E. Regional Variation of White Matter Development in the Cat Brain Revealed by Ex Vivo Diffusion MR Tractography. Int. J. Dev. Neurosci. 2016, 54, 32–38.
- Schmahmann, J.D.; Pandya, D.N.; Wang, R.; Dai, G.; D’Arceuil, H.E.; de Crespigny, A.J.; Wedeen, V.J. Association Fibre Pathways of the Brain: Parallel Observations from Diffusion Spectrum Imaging and Autoradiography. Brain 2007, 130 Pt 3, 630–653.
- Wedeen, V.J.; Rosene, D.L.; Wang, R.; Dai, G.; Mortazavi, F.; Hagmann, P.; Kaas, J.H.; Tseng, W.Y. The Geometric Structure of the Brain Fiber Pathways. Science 2012, 335, 1628–1634.
- Wu, Y.; Sun, D.; Wang, Y.; Wang, Y. Subcomponents and Connectivity of the Inferior Fronto-Occipital Fasciculus Revealed by Diffusion Spectrum Imaging Fiber Tracking. Front. Neuroanat. 2016, 10, 88.
- Wang, X.; Pathak, S.; Stefaneanu, L.; Yeh, F.C.; Li, S.; Fernandez-Miranda, J.C. Subcomponents and Connectivity of the Superior Longitudinal Fasciculus in the Human Brain. Brain Struct. Funct. 2016, 221, 2075–2092.
- Sun, C.; Wang, Y.; Cui, R.; Wu, C.; Li, X.; Bao, Y.; Wang, Y. Human Thalamic-Prefrontal Peduncle Connectivity Revealed by Diffusion Spectrum Imaging Fiber Tracking. Front Neuroanat. 2018, 12, 24.
- Suo, X.; Guo, L.; Fu, D.; Ding, H.; Li, Y.; Qin, W. A Comparative Study of Diffusion Fiber Reconstruction Models for Pyramidal Tract Branches. Front. Neurosci. 2021, 15, 777377.
- Liu, X.; Kinoshita, M.; Shinohara, H.; Hori, O.; Ozaki, N.; Nakada, M. A Fiber Dissection Study of the Anterior Commissure: Correlations with Diffusion Spectrum Imaging Tractography and Clinical Relevance in Gliomas. Brain Topogr. 2022, 35, 232–240.
- Wei, P.H.; Mao, Z.Q.; Cong, F.; Wang, B.; Ling, Z.P.; Liang, S.L.; Yu, X.G. Connection between Bilateral Temporal Regions: Tractography Using Human Connectome Data and Diffusion Spectrum Imaging. J. Clin. Neurosci. 2017, 39, 103–108.
- Sheets, J.R.; Briggs, R.G.; Dadario, N.B.; Young, I.M.; Bai, M.Y.; Poologaindran, A.; Baker, C.M.; Conner, A.K.; Sughrue, M.E. A Cortical Parcellation Based Analysis of Ventral Premotor Area Connectivity. Neurol. Res. 2021, 43, 595–607.
- Sheets, J.R.; Briggs, R.G.; Bai, M.Y.; Poologaindran, A.; Young, I.M.; Conner, A.K.; Baker, C.M.; Glenn, C.A.; Sughrue, M.E. Parcellation-Based Modeling of the Dorsal Premotor Area. J. Neurol. Sci. 2020, 415, 116907.
- Briggs, R.G.; Lin, Y.H.; Dadario, N.B.; Kim, S.J.; Young, I.M.; Bai, M.Y.; Dhanaraj, V.; Fonseka, R.D.; Hormovas, J.; Tanglay, O.; et al. Anatomy and White Matter Connections of the Middle Frontal Gyrus. World Neurosurg. 2021, 150, e520–e529.
- Lin, Y.H.; Young, I.M.; Conner, A.K.; Glenn, C.A.; Chakraborty, A.R.; Nix, C.E.; Bai, M.Y.; Dhanaraj, V.; Fonseka, R.D.; Hormovas, J.; et al. Anatomy and White Matter Connections of the Inferior Temporal Gyrus. World Neurosurg. 2020, 143, e656–e666.
- Shinohara, H.; Liu, X.; Nakajima, R.; Kinoshita, M.; Ozaki, N.; Hori, O.; Nakada, M. Pyramid-Shape Crossings and Intercrossing Fibers Are Key Elements for Construction of the Neural Network in the Superficial White Matter of the Human Cerebrum. Cereb. Cortex 2020, 30, 5218–5228.
- Ou, S.Q.; Wei, P.H.; Fan, X.T.; Wang, Y.H.; Meng, F.; Li, M.Y.; Shan, Y.Z.; Zhao, G.G. Delineating the Decussating Dentato-Rubro-Thalamic Tract and Its Connections in Humans Using Diffusion Spectrum Imaging Techniques. Cerebellum 2022, 21, 101–115.
- Chiang, H.L.; Tseng, W.I.; Tseng, W.L.; Tung, Y.H.; Hsu, Y.C.; Chen, C.L.; Gau, S.S. Atypical Development in White Matter Microstructures in ADHD: A Longitudinal Diffusion Imaging Study. Asian J. Psychiatry 2023, 79, 103358.
- Tsai, C.J.; Lin, H.Y.; Tseng, I.W.; Gau, S.S. White Matter Microstructural Integrity Correlates of Emotion Dysregulation in Children with ADHD: A Diffusion Imaging Tractography Study. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 110, 110325.
- Huang, J.Y.; Liu, C.M.; Hwang, T.J.; Chen, Y.J.; Hsu, Y.C.; Hwu, H.G.; Lin, Y.T.; Hsieh, M.H.; Liu, C.C.; Chien, Y.L.; et al. Shared and Distinct Alterations of White Matter Tracts in Remitted and Nonremitted Patients with Schizophrenia. Hum. Brain Mapp. 2018, 39, 2007–2019.
- Salisbury, D.F.; Wang, Y.; Yeh, F.C.; Coffman, B.A. White Matter Microstructural Abnormalities in the Broca’s-Wernicke’s-Putamen “Hoffman Hallucination Circuit” and Auditory Transcallosal Fibers in First-Episode Psychosis With Auditory Hallucinations. Schizophr. Bull. 2020, 47, 149–159.
- Salisbury, D.F.; Seebold, D.; Longenecker, J.M.; Coffman, B.A.; Yeh, F.C. White Matter Tracts Differentially Associated with Auditory Hallucinations in First-Episode Psychosis: A Correlational Tractography Diffusion Spectrum Imaging Study. Schizophr. Res. 2023, in press.
- Hula, W.D.; Panesar, S.; Gravier, M.L.; Yeh, F.C.; Dresang, H.C.; Dickey, M.W.; Fernandez-Miranda, J.C. Structural White Matter Connectometry of Word Production in Aphasia: An Observational Study. Brain A J. Neurol. 2020, 143, 2532–2544.
- Liu, J.; Wang, C.; Qin, W.; Ding, H.; Guo, J.; Han, T.; Cheng, J.; Yu, C. Corticospinal Fibers With Different Origins Impact Motor Outcome and Brain after Subcortical Stroke. Stroke 2020, 51, 2170–2178.
- Wan, X.; Xiao, Y.; Liu, Z. Diffusion Spectrum Imaging of Patients with Middle Cerebral Artery Stenosis. NeuroImage Clin. 2022, 36, 103133.
- Paul, T.; Wiemer, V.M.; Hensel, L.; Cieslak, M.; Tscherpel, C.; Grefkes, C.; Grafton, S.T.; Fink, G.R.; Volz, L.J. Interhemispheric Structural Connectivity Underlies Motor Recovery after Stroke. Ann. Neurol. 2023, 94, 785–797.
- Wen, M.C.; Thiery, A.; Tseng, W.I.; Kok, T.; Xu, Z.; Chua, S.T.; Tan, L.C.S. Apathy Is Associated with White Matter Network Disruption and Specific Cognitive Deficits in Parkinson’s Disease. Psychol. Med. 2020, 52, 264–273.
- Papageorgiou, P.; Rossi-mossuti, F.; Wiest, R.; Kiefer, C.; Zbinden, M.; Pollo, C. Characterisation of Dentatorubrothalamic Tract with Diffusion Spectrum Imaging in Patients Suffering from Parkinson’s Disease; Research Square: Durham, NC, USA, 2021.
- Luo, D.H.; Tseng, W.I.; Chang, Y.L. White Matter Microstructure Disruptions Mediate the Adverse Relationships between Hypertension and Multiple Cognitive Functions in Cognitively Intact Older Adults. NeuroImage 2019, 197, 109–119.
- Ni, H.C.; Lin, H.Y.; Tseng, W.I.; Gau, S.S. Association of Self-Regulation with White Matter Correlates in Boys with and without Autism Spectrum Disorder. Sci. Rep. 2020, 10, 13811.
- Wang, Y.H.; Wang, Z.M.; Wei, P.H.; Lu, C.; Fan, X.T.; Ren, L.K.; Shan, Y.Z.; Lu, J.; Zhao, G.G. Lateralizing the Affected Side of Hippocampal Sclerosis with Quantitative High Angular Resolution Diffusion Scalars: A Preliminary Approach Validated by Diffusion Spectrum Imaging. Ann. Transl. Med. 2021, 9, 297.
- Shibahara, I.; Saito, R.; Kanamori, M.; Sonoda, Y.; Sato, S.; Hide, T.; Tominaga, T.; Kumabe, T. Role of the Parietooccipital Fissure and Its Implications in the Pathophysiology of Posterior Medial Temporal Gliomas. J. Neurosurg. 2021, 137, 505–514.
- Zhang, H.; He, W.J.; Liang, L.H.; Zhang, H.W.; Zhang, X.J.; Zeng, L.; Luo, S.P.; Lin, F.; Lei, Y. Diffusion Spectrum Imaging of Corticospinal Tracts in Idiopathic Normal Pressure Hydrocephalus. Front. Neurol. 2021, 12, 636518.
- Wang, Z.M.; Wei, P.H.; Zhang, M.; Wu, C.; Shan, Y.; Yeh, F.C.; Shan, Y.; Lu, J. Diffusion Spectrum Imaging Predicts Hippocampal Sclerosis In Mesial Temporal Lobe Epilepsy Patients. Ann. Clin. Transl. Neurol. 2022, 9, 242–252.
- Liang, L.; Lin, H.; Lin, F.; Yang, J.; Zhang, H.; Zeng, L.; Hu, Y.; Lan, W.; Zhong, H.; Zhang, H.; et al. Quantitative Visual Pathway Abnormalities Predict Visual Field Defects in Patients with Pituitary Adenomas: A Diffusion Spectrum Imaging Study. Eur. Radiol. 2021, 31, 8187–8196.
- Mao, C.; Jiang, W.; Huang, J.; Wang, M.; Yan, X.; Yang, Z.; Wang, D.; Zhang, X.; Shen, J. Quantitative Parameters of Diffusion Spectrum Imaging: HER2 Status Prediction in Patients With Breast Cancer. Front. Oncol. 2022, 12, 817070.
- Zhang, H.; Wei, P.; Lu, C.; Wang, Z.; Fan, X.; Shan, Y.; Zhao, G. Assessing Structural Integrity of the Pyramidal Tracts with Diffusion Spectrum Imaging to Predict Postoperative Motor Function in Pediatric Epilepsy Patients with Hemispherectomy. Acta Epileptol. 2023, 5, 2.
- Zhang, Y.; Zhang, Z.; Jia, X.; Guan, X.; Lyu, Y.; Yang, J.; Jiang, T. Imaging Parameters of the Ipsilateral Medial Geniculate Body May Predict Prognosis of Patients with Idiopathic Unilateral Sudden Sensorineural Hearing Loss on the Basis of Diffusion Spectrum Imaging. AJNR Am. J. Neuroradiol. 2021, 42, 152–159.
- Lacerda, L.M.; Sperl, J.I.; Menzel, M.I.; Sprenger, T.; Barker, G.J.; Dell’Acqua, F. Diffusion in Realistic Biophysical Systems Can Lead to Aliasing Effects in Diffusion Spectrum Imaging. Magn. Reson. Med. 2016, 76, 1837–1847.
- Tian, Q.; Yang, G.; Leuze, C.; Rokem, A.; Edlow, B.L.; McNab, J.A. Generalized Diffusion Spectrum Magnetic Resonance Imaging (GDSI) for Model-Free Reconstruction of the Ensemble Average Propagator. NeuroImage 2019, 189, 497–515.


