Studies have demonstrated that many regions in the human brain include multidirectional fiber tracts, in which the diffusion of water molecules within image voxels does not follow a Gaussian distribution. Therefore, the conventional diffusion tensor imaging (DTI) that hypothesizes a single fiber orientation within a voxel is intrinsically incapable of revealing the complex microstructures of brain tissues. Diffusion spectrum imaging (DSI) employs a pulse sequence with different b-values along multiple gradient directions to sample the diffusion information of water molecules in the entire q-space and then quantitatively estimates the diffusion profile using a probability density function with a high angular resolution. Studies have suggested that DSI can reliably observe the multidirectional fibers within each voxel and allow fiber tracking along different directions, which can improve fiber reconstruction reflecting the true but complicated brain structures that were not observed in the previous DTI studies. Moreover, with increasing angular resolution, DSI is able to reveal new neuroimaging biomarkers used for disease diagnosis and the prediction of disorder progression. However, so far, this method has not been used widely in clinical studies, due to its overly long scanning time and difficult post-processing.
1. Introduction
Diffusion magnetic resonance imaging (dMRI) is the only way to noninvasively measure structural connectivity in the human brain, and it has been extensively applied in clinical studies [
1]. As one of the most commonly used dMRI techniques, diffusion tensor imaging (DTI) reconstructs structural connectivity patterns based on the phenomenon of the diffusion anisotropy of water molecules in brain tissue. In the DTI model, two metrics, the apparent diffusion coefficient (ADC) and fraction anisotropy (FA), are particularly sensitive to brain lesions in diseases [
2,
3], and the fiber tract is tracked by the main direction of the diffusion tensor [
4]. However, in the past twenty years, an increasing number of studies have reported that the fiber architectures in the human brain are more complicated than we thought, such as crossing or branching fibers within a single voxel [
5,
6]. The distances revealed by dMRI are far larger than the diffusion scale, implying that each 3D resolution element (voxel) represents many distinct diffusional environments. This provides a complex diffusion profile that is generally underspecified by the six degrees of freedom of the tensor model. Therefore, DTI is incapable of resolving multiple fiber orientations within a single voxel [
7]. Additionally, the FA value is lower when a multidirectional fiber exists in a single voxel, whereas the degeneration of tissue integrity also causes a reduced FA value. Thus, the FA metric may be inappropriate to evaluate the structural integrity of the tissue with crossing fibers. This not only affects the accuracy of the DTI technique in clinical diagnosis but also leads to the failure of fiber tract tracking in complex tissue.
To resolve the multiple fiber orientations within individual voxels, various methods have been proposed. They have been classified into two types: one is model-based, such as multi-tensor diffusion imaging [
8], diffusion kurtosis imaging (DKI) [
9], neurite orientation dispersion and density imaging (NODDI) [
10], the ball and stick model [
11], the persistent angular structure MRI [
12], and diffusion orientation transform [
12]; the other is model-free high-angular-resolution diffusion imaging (HARDI), which describes the diffusion motion by the orientation distribution function (ODF). For instance, diffusion spectrum imaging (DSI) reconstructs the ODF by applying an inverse Fourier transform (FT) to the q-space data from the grid sampling scheme [
13]; Q-ball imaging (QBI) based on a Funk–Radon (FR) transform reconstructs the ODF from a single-shell dataset [
14]; hybrid diffusion imaging (HYDI) concurrently performs DSI, Q-ball, and DTI analysis in multi-shell data [
15]; and generalized-sampling imaging (GQI) describes the diffusion behavior using the spin distribution function (SDF), similar to ODF [
16].
Wedeen et al. first proposed the DSI, a multi-b-value and multidirectional q-space imaging method, which calculates the diffusion ODF by applying the FT to the diffusion MR signals and conducting radial integration [
17]. This method can successfully reveal crossing fibers. Moreover, the general fraction anisotropy (GFA) produced from DSI is more sensitive to tissue degeneration in diseased brains and has better accuracy and precision in identifying the multidirectional fibers than the conventional FA obtained using DTI [
18]. Under a relatively unified standard, one prior study [
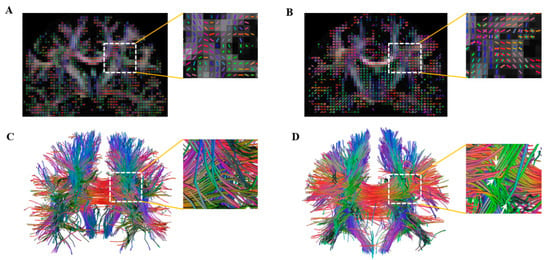
19] compared 19 dMRI approaches, in which the dMRI methods were classified into four types according to the pattern of the data sampling scheme: DTI-like (single ball and lower b-value sample), HARDI-like (single ball and higher b-value sample), DSI-like (Cartesian grid sample), and Strike-like (sparse sample). The results showed that compared with other high-resolution imaging techniques, the DSI was more precise and stable than the DTI in terms of both the angular accuracy and the success rate of reconstructing the crossing fiber and the ability to uncover the minimal angle of the crossing fiber (
Figure 1). However, so far, no study has comprehensively reviewed the research progress of DSI.
Figure 1. A comparison of DTI (A,C) and DSI (B,D) in revealing crossing fiber. (A,B) the color FA map; (C,D) the fiber tracts in the whole brain. The white arrows show the crossing fibers in (D), whereas they are not revealed in (C).
2. DSI Tractography for White-Matter Fibers
Several tissue structures include a number of myofibers aligned along multiple spatial axes at the microscopic scale. However, the DTI cannot uncover such structural characteristics due to its failure to detect multidirectional fibers. Therefore, one of the important applications of DSI tractography is primarily focused on revealing the complex microstructure of the tissue. For instance, for an anterior slice of the lingual core in bovine tongue, DTI depicted it solely as a region with low anisotropy, whereas DSI revealed two different fiber populations with an explicit orthogonal relationship to each other [
48]. Dai et al. found that DSI tractography revealed that the cingulum bundle was less mature when cat myelination was incomplete, whereas DTI tractography tended to terminate in such areas, possibly due to the existence of crossing fibers [
49]. By using DSI, Schmahmann et al. identified the major features of 10 long association fiber bundles that matched the observations in the isotope material using autoradiographic histological tract tracing in the monkey brain, whereas the DTI did not observe such precise structural characteristics due to its inability to visualize the crossing fibers and details of the origins, course, and terminations of the white-matter pathways [
50]. In human brain studies, Wedeen et al. used DSI to clarify the relationships of adjacency and crossing between cerebral fiber pathways in four nonhuman primate species and humans [
51]. They first found that the cerebral fiber pathways formed a rectilinear three-dimensional grid continuous with the three principal axes of development, and cortico-cortical pathways formed parallel sheets of interwoven paths in the longitudinal and medial–lateral axes, in which major pathways were local condensations. Because of the limitation in DTI, the subcomponents and connectivity of the inferior fronto-occipital fasciculus (IFOF) and the superior longitudinal fasciculus (SLF) in human brain are still controversial. The DSI shows high-quality fiber tractography and fewer partial volume effects and false continuation artifacts, and thereby it has been used to reveal more complete connectivity patterns and anatomical details of the IFOF I-V subcomponents [
52] and of the SLF I-III subcomponents [
53], which are connected to different cortical regions. Similar DSI tractography applications have been reported in recent studies in the tractography of other white-matter pathways, such as the thalamic–prefrontal peduncle [
54], pyramidal tracts [
55], anterior commissure [
56], and corpus callosum [
57]. Collectively, these findings suggest a powerful potential of DSI in enhancing tractography for the complexed white-matter fibers.
3. Cortical Parcellation and Connectivity Reconstruction
The DTI has limited angular resolution and cannot adequately assess the cortical regions. Another application of the DSI in resolving the tissue microstructure is cortical parcellation and connectivity reconstruction. Recent studies used the DSI to segment the ventral [
58] and dorsal premotor areas [
59] (VPM/DPM); they found that the VPM consists of four subregions, 6v, 4, 3b, and 3a, and the DPM is divided into three areas, 6a, 6d, and 6v. These brain regions showed consistent inter-hemispheric connection but different intra-hemispheric connection patterns. Based on DSI tractography, two recent studies characterized the connections of the middle frontal gyrus (MFG) and inferior temporal gyrus (ITG) to other cortical areas, respectively. The MFG included two major connections of the superior longitudinal fasciculus (which connected the MFG to parts of the inferior parietal lobule, posterior temporal lobe, and lateral occipital cortex) and the inferior fronto-occipital fasciculus (which connected the MFG to the lingual gyrus and cuneus) [
60]. The ITG is connected to five major fibers: the U-fiber, the inferior longitudinal fasciculus, the vertical occipital fasciculus, the arcuate fasciculus, and the uncinate fasciculus [
61]. Furthermore, a recent study used DSI tractography to organize “pyramid-shaped crossings” of converged U-fibers, which are key anatomical structures to construct the neural network for intricate communications throughout the entire cerebrum [
62]. Using the same method, another study delineated the decussating dentato-rubro-thalamic tract, in which the afferent regions were found mainly in the posterior cerebellum, and the efferent fibers were mainly projected to the contralateral frontal cortex, suggesting segregated and parallel cerebellar outputs to cerebral regions [
63] (see
Table 1).
4. Clinical Applications
With the improvement in DSI data acquisition, more attention has recently been paid to its application in clinical diseases, including attention-deficit/hyperactivity disorder (ADHD) [
2,
64,
65], schizophrenia [
66,
67,
68], stroke [
69,
70,
71,
72], Parkinson’s disease [
73,
74], hypertension [
75], autism [
76], epilepsy [
77], and gliomas [
78] (see
Table 1).
4.1. Disease Diagnosis
The quantitative diffusion scalars of the DSI, especially the track density imaging (TDI) of the crura of fornix (FORX) and the parahippocampal radiation of the cingulum (PHCR), are sensitive enough to define the ipsilateral side for epilepsy patients, with a sensitivity of 89.5% and specificity of 100.0% for PHCR_TDI (AUC = 0.93), and a sensitivity of 95.0% and specificity of 100% for FORX_TDI (AUC = 0.95) [
77]. The DSI-based quantitative anisotropy (QA) values of corticospinal tracts (CSTs) in patients with idiopathic normal pressure hydrocephalus (iNPH) were significantly lower than those in healthy controls (HCs), but no significant differences were found between iNPH patients and HCs in the DTI-based FA values, suggesting the DSI may provide more information that can improve the present understanding of the disease mechanism [
79]. Another study found that the QA value was correlated with the neuronal diameter/density in the cortical layer IIIc, and its asymmetry showed an overall favorable accuracy (sensitivity = 90.9%, specificity = 89.5%, AUC = 0.96) in the diagnostic testing of hippocampal sclerosis patients [
80]. The DSI parameters also showed a good performance, with an accuracy of 83%, sensitivity of 78%, and specificity of 86% in discriminating patients with mild and severe visual defects [
81].
4.2. Progression Prediction
A prior study demonstrated that the DSI could be helpful for the preoperative prediction of human epidermal growth factor receptor 2 (HER2) in patients with breast cancer, with the finding that the AUC values of the DSI quantitative parameters (range from 0.67 to 0.72) were higher than that of the DTI metric apparent diffusion coefficient (AUC = 0.57) [
82]. Another study found that the anatomic integrity of the pyramidal tract (PT) with DSI tractography effectively predicted the postoperative motor function after hemispherectomy; they reported that the AUC of the DSI tractography was 0.84, and the cutoff value of the PT asymmetric ratio was 11.5%, with 100% sensitivity and 75% specificity [
83]. The DSI-derived GFA in the ipsilateral medial geniculate body was related to prognosis (sensitivity = 64.7%; specificity = 85.7%; and AUC = 0.80) in patients with unilateral idiopathic sudden sensorineural hearing loss, indicating the GFA value of the ipsilateral medial geniculate body may help to predict recovery outcomes [
84]. Another study reconstructed a local connectome matrix from DSI data in patients with aphasia after stroke, and their findings challenged dual-stream accounts that denied a role for the arcuate fasciculus in semantic processing and ventral-stream pathways in language production and illuminated limbic contributions to both semantic and phonological processing for word production [
69]. A recent DSI study demonstrated for the first time that distinct aspects of the cortical structural reserve enable basal and complex motor control after stroke. In particular, the recovery of basal motor control may be supported via an alternative route through contralesional M1 and non-crossing fibers of the contralesional CST [
72]. Taken together, these findings suggest the DSI is a very potential and powerful technology in studying the mechanism, diagnosis, and progressive prediction of clinical diseases.
Table 1. A summary of main progresses in DSI applications.
| First Author (Ref. #) |
Type |
Subject |
Main Findings |
| Lacerda et al., 2016 [46] |
Methodology |
Optimization of postprocessing method |
This study proposed a new way of including biophysical constraints to compute the ODF, which removed most of the artifacts due to fast diffusion components like those from pathological tissues and offered improved angular resolution. |
| Tian et al., 2019 [47] |
Methodology |
Optimization of postprocessing method |
This study proposed a generalized DSI framework to compute the ensemble average propagator, which could be used to elucidate the contribution and combination of q-space signals to the diffusion ODF. |
| Gilbert et al., 2006 [48] |
Application |
DSI tractography for white-matter fibers |
Diffusion tensor imaging (DTI) depicted the anterior slice of the lingual core in bovine tongue solely as a region with low anisotropy, whereas DSI revealed two different fiber populations with an explicit orthogonal relationship to each other. |
| Dai et al., 2016 [49] |
Application |
DSI tractography for white-matter fibers |
The cingulum bundle was less mature when cat myelination was incomplete, whereas the DTI tractography tended to terminate in such areas. |
| Schmahmann et al., 2007 [50] |
Application |
DSI tractography for white-matter fibers |
This study identified 10 major long association fiber bundles that matched the observations in autoradiographic histological tract tracing in the monkey brain, and such precise structural characteristics were not observed by DTI. |
| Wedeen et al., 2012 [51] |
Application |
DSI tractography for white-matter fibers |
This study first clarified the relationships of adjacency and crossing between cerebral fiber pathways in four nonhuman primate species and humans. |
Wu et al., 2016 [52];
Wang et al., 2016 [53] |
Application |
DSI tractography for white-matter fibers |
The DSI revealed a more complete connectivity pattern and anatomical details of the IFOF I-V subcomponents and of the SLF I-III subcomponents. |
Sun et al., 2018 [54];
Suo et al., 2021 [55];
Liu et al., 2022 [56];
Wei et al., 2017 [57] |
Application |
DSI tractography for white-matter fibers |
The DSI identified detailed and completed white-matter pathways, including the thalamic–prefrontal peduncle, pyramidal tracts, anterior commissure, and corpus callosum. |
| Sheets et al., 2020, 2021 [58,59] |
Application |
Cortical parcellation |
The DSI segmented the ventral premotor area into four subregions of 6v, 4, 3b, and 3a and the dorsal premotor area into three areas of 6a, 6d, and 6v. |
| Briggs et al., 2021 [60]; Lin et al., 2020 [61] |
Application |
Cortical connectivity reconstruction |
The MFG included two major connections of the superior longitudinal fasciculus and inferior fronto-occipital fasciculus. The ITG connected to five major fibers: the U-fiber, inferior longitudinal fasciculus, vertical occipital fasciculus, arcuate fasciculus, and uncinate fasciculus. |
| Chiang et al., 2020, 2023 [2,64];Tsai et al., 2021 [65] |
Application |
Attention deficit and hyperactivity disorder (ADHD) |
Participants with ADHD showed more rapid development of generalized fractional anisotropy (GFA) in the frontal tracts and showed higher axial diffusivity values in the perpendicular fasciculus, superior longitudinal fasciculus I, corticospinal tract, and corpus callosum compared to the control group. |
| Wen et al., 2020 [73]; Papageorgiou et al., 2021 [74] |
Application |
Parkinson’s disease (PD) |
The PD patients showed impaired global efficiency and characteristic path length in the DSI-based connected network, which were associated with executive function and episodic memory. |
| Wang et al., 2020, 2022 [77,80]; Zhang et al., 2023 [82] |
Application |
Epilepsy |
The AUC of the asymmetric indices of the DSI-derived QA value to the lateralization of epilepsy was 0.96, with 0.91 sensitivity and 0.90 specificity; The AUC of DSI tractography was 0.84, with 100% sensitivity and 75% specificity in discriminating patients with epilepsy from healthy controls. |
| Ni et al., 2020 [76] |
Application |
Autism spectrum disorder (ASD) |
A higher GFA of the tracts was implicated in memory, attention, sensorimotor processing, and perception associated with less dysregulation in TDC but worse dysregulation in ASD. |
| Zhang et al., 2021 [79] |
Application |
Idiopathic normal-pressure hydrocephalus (iNPH) |
The DSI-based QA values of corticospinal tracts (CSTs) in patients with Inph were lower than those in healthy controls (HCs), but such differences in DTI-based FA were observed between iNPH patients and HCs. |
| Liang et al., 2021 [81] |
Application |
Pituitary adenomas |
The DSI parameters also showed a good performance, with an accuracy of 0.83, sensitivity of 0.78, and specificity of 0.86 in discriminating patients with mild and severe visual defects |
| Mao et al., 2022 [82] |
Application |
Breast cancer |
DSI could be helpful for the preoperative prediction of human epidermal growth factor receptor 2 (HER2) in patients with breast cancer, with the findings that the AUC values of DSI quantitative parameters (0.67~0.72) were higher than those of apparent diffusion coefficient (0.57) from DTI. |
| Zhang et al., 2021 [84] |
Application |
Idiopathic sudden sensorineural hearing loss |
The DSI-derived GFA in the ipsilateral medial geniculate body was related to the prognosis (sensitivity = 64.7%; specificity = 85.7%; AUC = 0.796) in patients with unilateral idiopathic sudden sensorineural hearing loss. |
| Paul et al., 2023 [72] |
Application |
Stroke |
This study used DSI to demonstrate for the first time that recovery of basal motor control may be supported via an alternative route through contralesional M1 and non-crossing fibers of the contralesional CST. |
| Salisbury et al., 2023 [68] |
Application |
First-episode psychosis |
White-matter tracts showing associations between QA from DSI and auditory hallucinations were associated with frontal–parietal–temporal connectivity in the cingulum bundle and in the prefrontal interhemispheric connectivity. |
This entry is adapted from the peer-reviewed paper 10.3390/brainsci13101497