 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Hiroko Nagamuna | -- | 2621 | 2023-11-14 12:41:40 | | | |
| 2 | Mona Zou | Meta information modification | 2621 | 2023-11-15 08:50:04 | | |
Video Upload Options
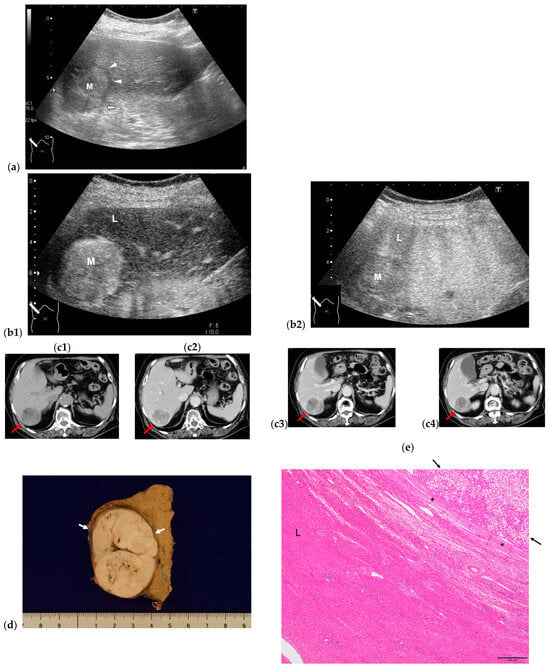
Hepatocellular carcinoma (HCC) in a non-fibrotic liver (F0) is considered to be rare, and there is a marked paucity of studies in the literature on this HCC type. A review of the literature shows some important clinical and tumor characteristics: (a) it occurs mainly in young female and elder male patients; (b) clinically, under normal hepatic function, alpha-fetoprotein level is often normal, and there are no risk factors; (c) associated with metabolic disease; (d) macroscopically, single large lesions are noted; and (e) microscopically, the lesions are well-differentiated and encapsulated. Radiological imaging results are straightforward, showing arterial hyperenhancement and later wash-out. The combined use of B-mode and contrast-enhanced (CE) ultrasound (US) is the most reliable and cost-effective diagnostic method. Few peri-and post-operative complications are noted and 5-year survival is not inferior to patients with HCC on fibrosis liver despite the lesion’s large size. Most clinicians believe that HCC is unlikely to occur if patients have no symptoms and normal hepatic function.
1. Introduction
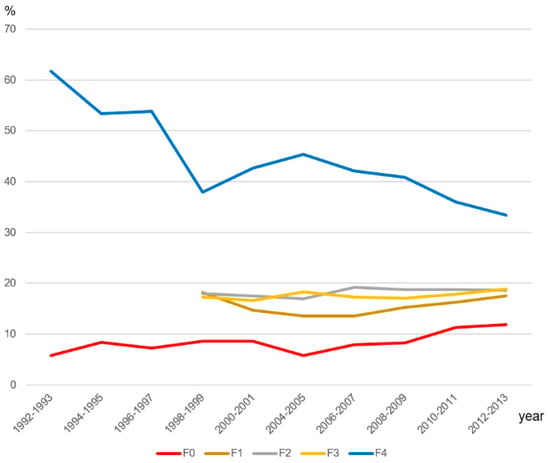
2. Incidence of HCC in Non-Fibrotic Liver (F0)
3. Reported Possible Causal Factors of HCC in Non-Fibrotic Liver (F0)
3.1. Family History and Genetic Factors
3.2. Aging and Sex
3.3. Alcohol Consumption
3.4. Obesity and Diabetes Mellitus (DM)
3.5. Viral Infection
3.6. Autoimmune Hepatitis
3.7. Exposure to Chemicals
3.8. Multiple Primary Malignancies (MPMs)
3.9. Hepatocellular Adenoma (HCA)
3.10. The Other Less Common Risk Factors
4. Clinical Manifestation and Diagnosis
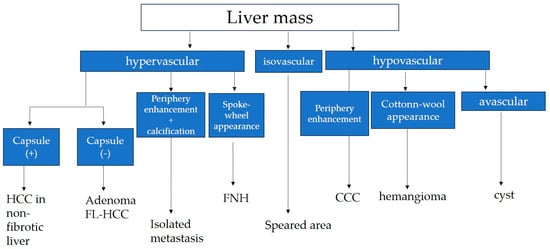
5. Differential Diagnosis
5.1. Fibrolamellar Hepatocellular Carcinoma (FL-HCC)
5.2. Hepatocellular Adenoma
5.3. Focal Nodular Hyperplasia (FNH)
5.4. Hypervascular Hemangioma (Hy-Heman)
5.5. Solitary Metastasis
References
- Mcglynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemilogy of hepatocellular carcinoma. Hepatology 2021, 73 (Suppl. S1), 4–13.
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA Cancer J. Clin. 2014, 64, 9–29.
- Samant, H.; Amiri, H.S.; Zibari, G.B. Addressing the worldwide hepatocellular carcinoma: Epidemiology, prevention and management. J. Gastrointest. Oncol. 2021, 12, S361–S373.
- Shi, Y.; Wu, Y.H.; Wu, W.; Zhang, W.J.; Yang, J.; Chen, Z. Association between occult hepatitis B infection and the risk of hepatocellular carcinoma: A meta-analysis. Liver Int. 2012, 32, 231–240.
- Donato, F.; Tagger, A.; Gelatti, U.; Parrinello, G.; Boffetta, P.; Albertini, A.; Decarli, A.; Trevisi, P.; Ribero, M.L.; Martelli, C.; et al. Alcohol and hepatocellular carcinoma: The effect of lifetime intake and hepatitis virus infection and women. Am. J. Epidemiol. 2002, 155, 323–331.
- Sanyal, A.J.; Harrison, S.A.; Ratziu, V.; Abdelmalek, M.F.; Diehl, A.M.; Caldwell, S.; Shiffman, M.L.; Schall, R.A.; Jia, C.; McColgan, B.; et al. The natural history of advanced fibrosis due to nonalcoholic steatohepatitis: Data from the simtuzumab trials. Hepatology 2019, 70, 1913–1927.
- Fazel, Y.; Koenig, A.B.; Sayiner, M.; Goodman, Z.D.; Younossi, Z.M. Epidemiology and natural history of non-alcoholic liver disease. Metabolism 2016, 65, 1017–1025.
- Lu, W.; Zheng, F.; Li, Z.; Zhou, R.; Deng, L.; Xiao, W.; Chen, W.; Zhao, R.; Chen, Y.; Tan, Y.; et al. Association between environmental and socioeconomic risk factors and hepatocellular carcinoma: A meta-analysis. Front. Public. Health 2022, 10, 741490.
- Bralet, M.P.; Réginbeau, J.M.; Pineau, P.; Dubois, S.; Loas, G.; Degos, F.; Valla, D.; Belghiti, J.; Degott, C.; Terris, B.; et al. Hepatocellular carcinoma occurring in nonfibrotic liver: Epidemiologic and histopathologic analysis of 80 french cases. Hepatology 2000, 32, 200–204.
- Roey, G.V.; Fevery, J.; Van Steenbergen, W. Hepatocellular carcinoma in Belgium: Clinical and virological characteristics of 154 consecutive cirrhotic and non-cirrhotic patients. Eur. J. Gastroenterol. Hepatol. 2000, 12, 61–66.
- Okuda, K.; Nakashima, T.; Kojiro, M.; Kondo, Y.; Wada, K. Hepatocellular carcinoma without cirrhosis in Japanese patients. Gastroenterology 1989, 97, 140–146.
- Desai, A.; Sandhu, S.; Lai, J.P.; Sandhu, D.S. Hepatocellular carcinoma in non-cirrhotic liver: A comprehensive review. World J. Hepatol. 2019, 11, 1–18.
- Pinyopornpanish, K.; Al-Yaman, W.; Dasarathy, S.; Romero-Marrero, C.; McCullough, A. Hepatocellular carcinoma in patients without cirrhosis: The fibrosis stage distribution, characteristics and survival. Dig. Dis. Sci. 2022, 67, 2677–2687.
- Yip, V.S.; Gomez, D.; Tan, C.Y.; Staettner, S.; Terlizzo, M.; Fenwick, S.; Malik, H.Z.; Ghaneh, P.; Poston, G. Tumor size and differentiation predict survival after liver resection for hepatocellular carcinoma arising from non-cirrhotic and non-fibrotic liver: A case-controlled study. Int. J. Surg. 2013, 11, 1078–1082.
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. Hepatology 1996, 24, 289–293.
- Chopinet, S.; Cauchy, F.; Hobeika, C.; Beaufrère, A.; Poté, N.; Farges, O.; Dokmak, S.; Bouattour, M.; Ronot, M.; Vilgrain, V.; et al. Long-term outcomes following resection of hepatocellular adenomas with small foci of malignant transformation or malignant adenomas. JHEP Rep. 2021, 3, 100326.
- Bismuth, H.; Chiche, L.; Castaing, D. Surgical treatment of hepatocellular carcinoma in noncirrhotic liver: Experience with 68 liver resections. World J. Surg. 1995, 19, 35–41.
- Lubrano, J.; Huet, E.; Tsillividis, B.; François, A.; Goria, O.; Ghassan Riachi, G.; Scotté, M. Long-term outcomes of liver resection for hepatocellular carcinoma in noncirrhotic liver with no viral hepatitis or alcohol abuse. World J. Surg. 2008, 32, 104–109.
- Okuda, K. Liver Cancer Study Group of Japan: Primary liver cancers in Japan. Cancer 1980, 45, 2663–2669.
- Anonymous. Liver Cancer Study Group of Japan: Primary liver cancer in Japan. Cancer 1984, 54, 747–755.
- Anonymous. Liver Cancer Study Group of Japan: Primary liver cancer in Japan. Sixth report. Cancer 1987, 60, 1400–1411.
- Liver Cancer Study Group of Japan. Primary liver cancer in Japan. Clinicopathologic features and results of surgical treatment. Ann. Surg. 1990, 211, 277–287.
- Tobe, T.; Kameda, H.; Okudaira, M.; Ohto, M.; Endo, Y.; Mito, M.; Okamoto, E.; Tanikawa, K.; Kojiro, M. (Eds.) Primary Liver Cancer in Japan; Springer: Tokyo, Japan, 1992.
- Ikai, I.; Itai, Y.; Okita, K.; Omata, M.; Kojiro, M.; Kobayashi, K.; Nakanuma, Y.; Futagawa, S.; Makuuchi, M.; Yamaoka, Y. Report of the 15th follow-up survey of primary liver cancer. Hepatol. Res. 2004, 28, 21–29.
- Ikai, I.; Arii, S.; Ichida, T.; Okita, K.; Omata, M.; Kojiro, M.; Takayasu, K.; Nakanuma, Y.; Makuuchi, M.; Matsuyama, Y.; et al. Report of the 16th follow-up survey of primary liver cancer. Hepatol. Res. 2005, 32, 163–172.
- Ikai, I.; Arii, S.; Okazaki, M.; Okita, K.; Omata, M.; Kojiro, M.; Takayasu, K.; Nakanuma, Y.; Makuuchi, M.; Matsuyama, Y.; et al. Report of the 17th Nationwide Follow-up Survey of Primary Liver Cancer in Japan. Hepatol. Res. 2007, 37, 676–691.
- Ikai, I.; Kudo, M.; Arii, S.; Omata, M.; Kojiro, M.; Sakamoto, M.; Takayasu, K.; Hayashi, N.; Makuuchi, M.; Matsuyama, Y.; et al. Report of the 18th follow-up survey of primary liver cancer in Japan. Hepatol. Res. 2010, 40, 1043–1059.
- Kudo, M.; Izumi, N.; Ichida, T.; Ku, Y.; Kokudo, N.; Sakamoto, M.; Takayama, T.; Nakashima, O.; Matsui, O.; Matsuyama, Y. Report of the 19th follow-up survey of primary liver cancer in Japan. Hepatol. Res. 2016, 46, 372–390.
- Kudo, M.; Izumi, N.; Kubo, S.; Kokudo, N.; Sakamoto, M.; Shiina, S.; Tateishi, R.; Nakashima, O.; Murakami, T.; Matsuyama, Y.; et al. Report of the 20th Nationwide follow-up survey of primary liver cancer in Japan. Hepatol. Res. 2020, 50, 15–46.
- Kudo, M.; Izumi, N.; Kokudo, N.; Sakamoto, M.; Shiina, S.; Takayama, T.; Tateishi, R.; Nakashima, O.; Murakami, T.; Matsuyama, Y.; et al. Report of the 21st Nationwide Follow-up Survey of Primary Liver Cancer in Japan (2010–2011). Hepatol. Res. 2021, 51, 355–405.
- Kudo, M.; Izumi, N.; Kokudo, N.; Sakamoto, M.; Shiina, S.; Takayama, T.; Tateishi, R.; Nakashima, O.; Murakami, T.; Matsuyama, Y.; et al. Report of the 22nd nationwide follow-up Survey of Primary Liver Cancer in Japan (2012–2013). Hepatol. Res. 2022, 52, 5–66.
- Stroffolini, T.; Andreone, P.; Andriulli, A.; Ascione, A.; Craxi, A.; Chiaramonte, M.; Galante, D.; Manghisi, O.G.; Mazzanti, R.; Medaglia, C.; et al. Characteristics of hepatocellular carcinoma in Italy. J. Hepatol. 1998, 29, 944–952.
- Shrestha, A. Liver Cancer in Nepal. Euro. J. Hepatogastroenterol. 2018, 8, 63–65.
- Kar, P. Risk factors for hepatocellular carcinoma in India. J. Clin. Exp. Hepatol. 2014, 4, S34–S42.
- Global Burden of Disease Liver Cancer Collaboration; Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Ale Mayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; et al. The burden of primary liver cancer and underlying etiologies from 1990 to 2015 at the global, regional, and national level: Results from the global burden of disease study 2015. JAMA Oncol. 2017, 3, 1683–1691.
- Petrick, J.L.; Florio, A.A.; Znaor, A.; Ruggieri, D.; Laversanne, M.; Alvarez, C.S.; Ferlay, J.; Valery, P.C.; Bray, F.; McGlynn, K.A. International trends in hepatocellular carcinoma incidence, 1978–2012. Int. J. Cancer 2020, 147, 317–330.
- Pembroke, T.P.I.; John, G.; Puyk, B.; Howkins, K.; Clarke, R.; Yousuf, F.; Czajkowski, M.; Godkin, A.; Salmon, J.; Yeoman, A. Rising incidence, progression and changing patterns of liver disease in Wales 1999–2019. World J. Hepatol. 2023, 15, 89–106.
- Liu, L.; Li, L.; Zhou, S.; Jiang, Q.; Chen, S.; Gao, Y.; Chen, Y. Familial correlations of onset age of hepatocellular carcinomas: A population-based case-control family study. PLoS ONE 2014, 9, e108391.
- An, J.; Chang, S.; Kim, H.I.; Song, G.W.; Shim, J.H. The clinical behavior and survival of patients with hepatocellular carcinoma and a family history of the disease. Cancer Med. 2019, 8, 6624–6633.
- Villanuev, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462.
- Takahashi, A.; Saito, H.; Kanno, Y.; Abe, K.; Yokokawa, J.; Irisawa, A.; Kenjo, A.; Saito, T.; Gotoh, M.; Ohira, H. Case of clear-cell hepatocellular carcinoma that developed in the normal liver of a middle-aged woman. World J. Gastroenterol. 2008, 14, 129–131.
- Naganuma, H.; Ishida, H.; Ogawa, M.; Sato, T.; Sageshima, M.; Suzuki, K.; Ohyama, Y. Hetaocellular carcinoma in otherwise sonographically normal liver. J. Clin. Ultrasound 2019, 47, 325–330.
- Tajiri, K.; Shimizu, Y. Liver physiology and liver diseases in the elderly. World J. Gastroenterol. 2013, 19, 8459–8467.
- Hashim, D.; Carioli, G.; Malvezzi, M.; Bertuccio, P.; Waxman, S.; Negri, E.; La Vecchia, C.; Boffetta, P. Cancer mortality in the oldest old: A global overview. Aging 2020, 12, 16744–16758.
- Fane, M.; Weeraratna, A. How the aging microenvironment influences tumour progression. Nat. Rev. Cancer 2020, 20, 89–106.
- Macias, R.I.R.; Monte, M.J.; Serrano, M.A.; Macias, R.I.R.; Monte, M.J.; Serrano, M.A.; González-Santiago, J.M.; Martín-Arribas, I.; Simão, A.L.; Castro, R.E.; et al. Impact of aging on primary liver cancer: Epidemiology, pathogenesis and therapeutics. Aging 2021, 13, 23416–23434.
- Chen, X.; Wang, L.; Hong, L.; Su, Z.; Zhong, X.; Zhou, H.; Zhang, X.; Wu, J.; Shao, L. Identification of aging-related genes associated with clinical and prognostic features of hepatocellular carcinoma. Front. Genet. 2021, 12, 661988.
- European Association for the Study of the Liver. EASL clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236.
- Asrani, S.K.; Mellinger, J.; Arab, J.P.; Shah, V.H. Reducing the global burden alcohol-associated liver disease: A blueprint for action. Hepatology 2021, 73, 2039–2050.
- Yi, S.W.; Cjoi, J.S.; Yi, J.J.; Lee, Y.H.; Han, K.J. Risk factors for hepatocellular carcinoma by age, sex, and liver disorder status. A prospective cohort study in Korea. Cancer 2018, 24, 2748–2757.
- Myers, S.; Neyroud-Caspar, I.; Spahr, L.; Gkouvatsos, K.; Fournier, E.; Giostra, E.; Magini, G.; Frossard, J.L.; Bascaron, M.E.; Vernaz, N.; et al. NAFLD and MAFLD as emerging causes of HCC: A populational study. JHEP Rep. 2021, 3, 100231.
- Younossi, Z.M.; Otogonsuren, M.; Henry, L.; Venkatesan, C.; Mishra, A.; Erario, M.; Hunt, S. Association of nonalcoholic fatty liver disease (NAFLD) with hepatocellular carcinoma (HCC) in the united states from 2004 to 20009. Hepatology 2015, 62, 1723–1730.
- Fujiwara, N.; Friedman, S.L.; Goossens, N.; Hoshida, Y. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J. Hepatol. 2018, 68, 526–549.
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 77–491.e1.
- Kemp, L.; Clare, K.E.; Brennan, P.N.; Dillon, J.F. New horizons in hepatitis B and C in the older adult. Age Ageing 2019, 48, 32–37.
- Eguchi, S.; Ijtsma, A.J.; Slooff, M.J.; Porte, R.J.; de Jong, K.P.; Peeters, P.M.; Gouw, A.S.; Kanematsu, T. Outcome and pattern of recurrence after curative resection for hepatocellular carcinoma in patients with a normal liver compared to patients with a diseased liver. Hepatogastroenterology 2006, 53, 592–596.
- Bège, T.; LeTreut, Y.P.; Hardwigsen, J.; Hardwigsen, J.; Ananian, P.; Richa, H.; Campan, P.; Garcia, S. Prognostic factors after resection for hepatocellular carcinoma in nonfibrotic or moderately fibrotic liver. A 116-case European series. J. Gastrointest. Surg. 2007, 11, 619–625.
- Guzman, G.; Brunt, E.M.; Petrovic, L.M.; Chejfec, G.; Layden, T.J.; Costler, S.J. Does nonalcoholic fatty liver disease predispose patints to hepatocellular carcinoma in the absence of cirrhosis? Arch. Pathol. Lab. Med. 2008, 132, 1761–1766.
- Lewis, S.; Roayaie, S.; Ward, S.C.; Shyknevsky, I.; Jibara, G.; Taouli, B. Hepatocellular carcinoma in chronic hepatitis C in the absence of advanced fibrosis or cirrhosis. Am. J. Roentgenol. 2013, 200, W610–W616.
- Komiyama, S.; Okazaki, H.; Nakao, S.; Nishigori, S.; Terada, M.; Hamanaka, J.; Miura, Y.; Oka, H.; Suzaki, F.; Tanaka, K. Diffuse fatty metamorphosis of a large, well-differentiated hepatocellular carcinoma originating in the normal liver: A case report and literature review. Clin. J. Gastroenterol. 2015, 8, 345–350.
- Ogasawara, N.; Saitoh, S.; Denpou, H.; Kinowaki, K.; Akuta, N.; Suzuki, F.; Hashimoto, M.; Fujiyama, S.; Kawamura, Y.; Sezaki, H.; et al. Poorly differentiated hepatocellular carcinoma in a low-risk patient with an otherwise normal liver. Intern. Med. 2020, 59, 365–372.
- Onishi, S.; Tajika, M.; Tanaka, T.; Yamada, K.; Kamiya, T.; Natsume, S.; Shimizu, Y.; Niwa, Y. Juvenile hepatocellular carcinoma in a healthy liver. Intern. Med. 2022, 61, 1531–1536.
- Van Gerven, N.M.; de Boer, Y.S.; Mulder, C.J.; van Nieuwkerk, C.M.; Bouma, G. Autoimmune hepatitis. World J. Gastroenterol. 2016, 22, 4651–4661.
- Rigopoulou, E.I.; Dalekos, G.N. Current trends and characteristics of hepatocellular carcinoma in patients with autoimmune liver diseases. Cancers 2021, 13, 1023.
- Bolt, H.M. Vinyl chloride-a classical industrial toxicant of new interest. Crit. Rev. Toxicol. 2005, 35, 307–323.
- Zeng, Q.A.; Qiu, J.; Zou, R.; Li, Y.; Li, S.; Li, B.; Huang, P.; Hong, J.; Zheng, Y.; Lao, X.; et al. Clinical features and outcome of multiple primary malignancies involving hepatocellular carcinoma: A long-term follow-up study. BMC Cancer 2012, 12, 148.
- Xu, W.; Liao, W.; Ge, P.; Ren, J.; Xu, H.; Yang, H.; Sang, X.; Lu, X.; Mao, Y. Multiple primary malignancies in patients with hepatocellular carcinoma: A largest series with 26-year follow-up. Medicine 2016, 95, e3491.
- Sung, H.; Hyun, N.; Learch, C.R.; Yabroff, K.R.; Jemal, A. Association of first primary cancer with risk of subsequent primary cancer among survivors of adult-onset cancers in the United States. JAMA 2020, 324, 2521–2535.
- Thevathasan, T.; Colbatzky, T.; Schmelzle, M.; Pratschke, J.; Krenzien, F. Risk factors for malignant transformation of hepatocellular adenoma to hepat ocellular carcinoma: Protocol for systematic review and meta-analysis. BMJ Open 2021, 11, e045733.
- Sempoux, C.; Balabaud, C.; Bioulac-Sage, P. Pictures of focal nodular hyperplasia and hepatocellular adenomas. World J. Hepatol. 2014, 6, 580–595.
- van Rosmalen, B.V.; Furumaya, A.; Klompenhouwer, A.J.; Tushuizen, M.E.; Braat, A.E.; Reinten, R.J.; Ligthart, M.A.P.; Haring, M.P.D.; de Meijer, V.E.; van Voorthuizen, T.; et al. Hepatocellular adenoma in men: A nationwide assessment of pathology and correlation with clinical course. Liver Int. 2021, 41, 2474–2484.
- Khanna, R.; Verma, S.K. Pediatric hepatocellular carcinoma. World J. Gastroenterol. 2018, 24, 3980–3999.
- Berben, L.; Floris, G.; Wildiers, H.; Sigrid Hatse, S. Cancer and Aging: Two Tightly Interconnected Biological Processes. Cancers 2021, 13, 1400.
- Patel, J.; Baptiste, B.A.; Kim, E.; Hussain, M.; Croteau, D.L.; Bohr, V.A. DNA damage and mitochondria in cancer and aging. Carcinogenesis 2020, 41, 1625–1634.
- Cho, E.; Cho, H.A.; Jun, C.H.; Kim, H.J.; Cho, S.B.; Choi, S.K. A review of hepatocellular carcinoma in elderly patients focused on management and outcomes. Vivo 2019, 33, 1411–1420.
- Nishikawa, H.; Kimura, T.; Kita, R.; Osaki, Y. Treatment for hepatocellular carcinoma in elderly patients: A literature review. J. Cancer 2013, 4, 635–643.
- Centonze, L.; Di Sandro, S.; Lauterio, A.; De Carlis, R.; Frassoni, S.; Rampoldi, A.; Tuscano, B.; Bagnardi, V.; Vanzulli, A.; De Carlis, L. Surgical resection vs. percutaneous ablation for single hepatocellular carcinoma: Exploring the impact of Li-RADS classification on oncological outcomes. Cancers 2021, 13, 1671.
- Strobel, D. Using contrast-enhanced ultrasound in the diagnosis of hepatocellular carcinoma—What we have and have not achieved. Ultraschall Med. 2021, 42, 120–124.
- Mayo, S.C.; Mavros, M.N.; Nathan, H.; Cosgrove, D.; Herman, J.M.; Kamel, I.; Anders, R.A.; Pawlik, T.M. Treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma: A national perspective. J. Am. Coll. Surg. 2014, 218, 196–205.
- Wang, X.; Zhang, X. Hepatocellular adenoma: Where are we now? World J. Gastroenterol. 2022, 28, 1384–1393.
- Trillaud, H.; Bruel, J.M.; Valette, P.J.; Vilgrain, V.; Schmutz, G.; Oyen, R.; Jakubowski, W.; Danes, J.; Valek, V.; Greis, C. Characterization of focal liver lesions with SonoVue-enhanced sonography: International multicenter-study in comparison to CT and MRI. World J. Gastroenterol. 2009, 15, 3748–3756.
- Naganuma, H.; Ishida, H.; Ogawa, M.; Watanabe, Y.; Watanabe, D.; Ohyama, Y.; Watanabe, T. Focal nodular hyperplasia: Our experience of 53 Japanese cases. J. Med. Ultrason. 2017, 44, 79–88.
- Roche, V.; Pigneur, F.; Tselikas, L.; Roux, M.; Baranes, L.; Djabbari, M.; Costentin, C.; Calderaro, J.; Laurent, A.; Rahmouni, A.; et al. Differentiation of focal nodular hyperplasia from hepatocellular adenomas with low-mechanical-index contrast-enhanced sonography (CEUS): Effect of size on diagnostic confidence. Eur Radiol. 2015, 25, 186–195.
- Naganuma, H.; Ishida, H.; Konno, K.; Hamashima, Y.; Komatsuda, T.; Ishida, J.; Masamune, O. Hepatic hemangioma with arterioportal shunts. Abdom. Imaging 1999, 24, 42–46.
- Xian, M.F.; Li, W.; Lan, W.; Zeng, D.; Xie, W.; Lu, M.; Huang, Y.; Wang, W. Strategy for accurate diagnosis by contrast-enhanced ultrasound of focal liver lesions in patients not at high risk for hepatocellular carcinoma. J. Ultrasound Med. 2023, 42, 1333–1344.
- Kim, E.K.; Song, M.J.; Jung, Y.; Lee, W.S.; Jang, H.H. Proteomic Analysis of Primary Colon Cancer and Synchronous Solitary Liver Metastasis. Cancer Genom. Proteom. 2019, 16, 583–592.
- Aloia, T.A.; Vauthey, J.N.; Loyer, E.M.; Ribero, D.; Pawlik, T.M.; Wei, S.H.; Curley, S.A.; Zorzi, D.; Abdalla, E.K. Solitary colorectal liver metastasis: Resection determines outcome. Arch. Surg. 2006, 141, 460–466, discussion 466–467.
- Naganuma, H.; Hideaki Ishida, H.; Uno, A.; Nagai, H.; Ogawa, M.; Kamiyama, N. Refraction artifact on abdominal sonogram. J. Med. Ultrason. 2021, 48, 273–283.

