3. Reported Possible Causal Factors of HCC in Non-Fibrotic Liver (F0)
When investigating HCC arising from a normal liver, the following contributing factors must be considered.
3.1. Family History and Genetic Factors
Familial aggregation of HCC has been reported without any clear suggestions of an underlying genetic predisposition [
48,
49,
50]. However, these clinical studies did not provide any detailed information [
48,
49,
50]. To date, no studies have shown a strict association between family history and genetic factors and the risk of developing HCC in a non-fibrotic liver [
41,
45].
3.2. Aging and Sex
As has been investigated by many studies, aging is characterized by a progressive deterioration of all physiological functions [
51]. These changes, together with an increase in accumulating risk factors, predispose individuals to develop many cancers [
52,
53]. Thus, elders are thought to have an increased risk of developing HCC [
54,
55]. This idea can be applied to HCCs in non-fibrotic livers. In fact, according to a relatively large sample case series [
45], the average age of patients who present with HCC in a non-fibrotic liver at initial diagnosis is more than 70, which is approximately 10 years older than the average age of patients with HCC (mainly with liver cirrhosis) [
56], emphasizing the association between aging and HCC. As regards sex, Naganuma’s series of twelve patients consisted of eight men and four women. Thus, aging and sex are possible contributing factors to the development of HCC in a non-fibrotic liver.
3.3. Alcohol Consumption
A strong association between alcohol abuse and HCC development has been emphasized [
57], but mainly through the formation of liver cirrhosis [
58]. The effects of alcohol consumption on the development of HCC are considered to be stronger with advancing age, but usually through the formation of liver cirrhosis [
58]. Except for Takahashi’s case study [
41], in the other cases of HCC in non-fibrotic livers, the patients consumed almost no alcohol. Thus, alcohol is not thought to be a contributing factor to HCC in a non-fibrotic liver.
3.4. Obesity and Diabetes Mellitus (DM)
In obese patients, HCC usually appears as a late consequence of long-standing metabolically associated fatty liver disease (MAFLD) [
59]. MAFLD refers to liver steatosis in addition to obesity, overweight, DM type2, and/or metabolic dysregulation [
59]. Patients with MAFLD-related HCC have been reported to be older than patients with HCC and other underlying diseases (73 years vs. 66 years) and to have a shorter survival time after the occurrence of HCC [
60]. In patients with obesity and/or DM, HCC generally appears in fatty liver with fibrosis. In a case series of HCC in non-fibrotic livers, three of twelve cases (25%) were associated with DM, but all of them were well-controlled with drug therapy, and DM was likely to be a causal factor also in HCC in non-fibrotic liver [
45].
3.5. Viral Infection
Infection with hepatitis B or C is the most common etiology of HCC, occurring in more than 50% of all HCC patients [
61,
62,
63]. However, this association was found to be extremely uncommon in patients with HCC in a non-fibrotic liver [
38,
39,
40,
41,
42,
43,
45,
46,
47]. As a result, viral hepatitis infection was not considered to be a causal factor of HCC in non-fibrotic livers.
3.6. Autoimmune Hepatitis
Autoimmune liver diseases, including autoimmune hepatitis, primary biliary cholangitis, and primary sclerosing cholangitis, are well-known pathologies that occur mainly in women and are associated with HCC in some cases [
64,
65]. However, no cases have been reported in patients with non-fibrotic livers associated with autoimmune diseases.
3.7. Exposure to Chemicals
Exposure to chemicals, including polyvinyl chloride and arsenic, is known to induce hepatic malignancies [
66]. However, hepatic angiosarcoma represents the majority of chemical-induced hepatic tumors, and the occurrence of HCC is not common.
3.8. Multiple Primary Malignancies (MPMs)
The association of multiple primary malignancies (MPMs) and HCC has rarely been reported [
67,
68,
69], but this incidence is probably underestimated. The criteria for MPMs are as follows: (1) each tumor must present a definite picture of malignancy and (2) must be histologically distinct, and (3) one tumor being a metastasis of another must be excluded [
67,
68,
69]. The incidence of MPM-related HCC was thought to be approximately 2–5%. In Naganuma’s series, three of thirteen cases (23%) were MPM-related, much higher than usually expected. Although this series had a small sample size, this phenomenon must be taken into consideration when caring for patients with HCC in non-fibrotic liver.
3.9. Hepatocellular Adenoma (HCA)
HCA comprises a group of rare benign tumors that occur predominantly in women who use oral contraception, but also in patients who have diabetes mellitus, use androgens, or have glycogen storage disease [
70]. HCA is divided into four subtypes: beta-catenin, inflammatory, HNF1alpha-mutated, and unclassified. HCA is basically a benign tumor but has malignant potential. The risk of malignant transformation has been reported to be 4–5% in patients with hepatocellular adenoma [
71], and the risk factors for malignant transformation include the size (>5 cm), male gender, and an activating mutation in β-catenin [
72].
3.10. The Other Less Common Risk Factors
These include aflatoxin exposure, tobacco smoking, hemochromatosis, alpha- antitrypsin deficiency, and porphyria cutanea tarda [
8]. However, the reported cases of HCC in non-fibrotic livers were not associated with these factors. They also included Abernethy malformation, Alagille syndrome, ataxia telangioectasia, bile salt protein deficiency, tyrosinemia type 1, hypercitrullinemia, fructosemia, and others in children HCC [
73].
The histopathogenic pathways of the evolution of HCC arising from non-fibrotic hepatic parenchyma remain difficult to determine due to the lack of fibrosis. One of the most likely possibilities is that an HCC focus may be generated from precursor cells derived from the existing adenomatous tissues. The origin of HCC tissue is an important problem to be resolved in the near future.
Additionally, the problems of aging and MPMs are not negligible. Aging has been considered as a major risk factor for developing cancer through some underlying mechanisms including long-standing DNA damage, cellular senescence, and immunosenescence [
65,
66,
67,
68,
69,
74,
75]. On the other hand, cancer patients have received increasing survival benefits from continuous progress in early cancer detection and intensive treatments. Along with increased life expectancy, cancer survivors are at high risk of developing another cancer compared with the general population [
67,
68,
69].
4. Clinical Manifestation and Diagnosis
Cho et al. [
76] and Nishikawa et al. [
77] have noted some clinical and tumor characteristics seen in HCC in elderly patients: (a) clinically, a lack of surveillance and no risk factors; (b) macroscopically, a single large lesion; and (c) microscopically, a well-differentiated encapsulated lesion without vascular invasion. Although these HCC cases were associated with a fibrotic liver, their tumor characteristics were also seen in HCC arising from a non-fibrotic liver [
45]. The radiological findings faithfully represented these histologic characteristics, and the radiological diagnosis was straightforward according to Liver Imaging and Data System (LI-RADS) category 5 (definitely HCC), consisting of arterial phase hyperenhancement and late-phase wash-out [
78,
79]. Although recent meta-analyses have shown that contrast-enhanced ultrasound (CEUS) has higher sensitivity than CT or MRI for the diagnosis of HCC in chronic hepatic disease, there is currently insufficient evidence to strongly recommend CEUS for HCC in a non-fibrotic liver over the other two modalities, and further cases are necessary to draw a definitive conclusion. Homogeneous arterial enhancement on CEUS is worth noting. The most likely explanation for this enhanced pattern is the absence of a poorly differentiated HCC component in HCC arising from a non-fibrotic liver, despite its large size (
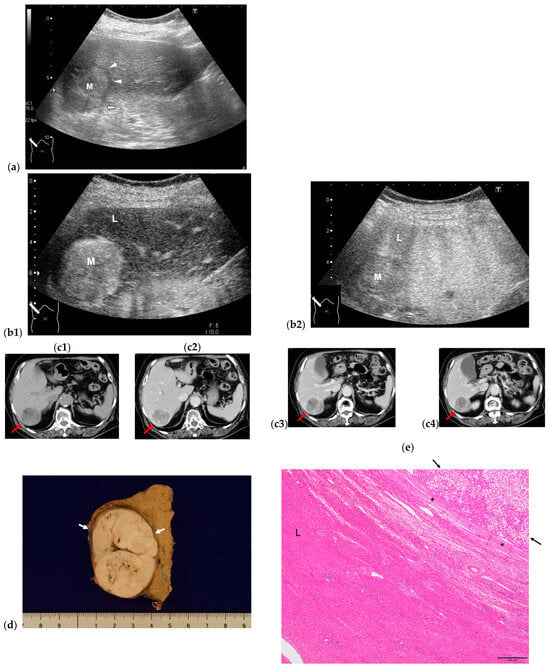
Figure 3).
Figure 3. Representative case of HCC in non-fibrotic liver (F0). (a) A large 4.6 cm× 3.5 cm hypoechoic round mass (M) with halo (arrowheads) and lateral shadowing (arrow) is seen on B-mode US. L: liver. CEUS clearly shows arterial hyperenhancement (b1), with iso-enhancement in the portal venous phase, and late wash-out (b2). CT findings reveals a solitary mass in S7 in pre-contrast scanning (arrow) (c1). Lesion shows arterial hyperenhancement (c2) and late wash-out (c3) portal venous phase, and (c4) equilibrium phase. (d) Macroscopically, lesion (arrows) is well-demarcated in non-fibrotic liver. (e) Microscopically, lesion mainly consists of well-differentiated HCC (arrows). Surrounding liver parenchyma (L) appears to be normal. *: capsule. This patient is symptom-and recurrence-free 7 years after HCC resection.
5. Differential Diagnosis
Strictly speaking, any large solitary hypervascular mass in a non-fibrotic liver must be included in the differential diagnosis. It must be considered that the pathologies listed below. Most of these lesions are asymptomatic, with tumor markers found to be within the normal range. Thus, accurate radiologic evaluation is critical.
5.1. Fibrolamellar Hepatocellular Carcinoma (FL-HCC)
FL-HCC accounts for less than 1% of all primary malignant tumors of the liver [
80]. These tumors occur predominantly in young patients without underlying liver disease [
80]. FL-HCC lesions are usually large, single, and well-defined, but they usually contain a calcified central scar, unlike HCC in non-fibrotic livers. FL-HCC lesions show hypervascularity in the arterial phase and isovascularity in the venous phase. No lateral shadowing around FL-HCC lesions is seen on US.
5.2. Hepatocellular Adenoma
It is usually very challenging to distinguish HCA from well-differentiated HCC, mainly due to the lack of a unified definition and variability in interpretation among pathologists, especially of biopsy specimens [
81]. HCA usually shows marked hypervascularity and/or slow, faint wash-out, mimicking HCC in a non-fibrotic liver. Thus, at present, it is almost impossible to differentiate HCC in a non-fibrotic liver from HCA via medical imaging or small biopsy specimens. Thus, a resection of the lesion and detailed interpretation of the surgical specimen are indispensable for establishing a definitive diagnosis of HCC in non-fibrotic livers [
45].
5.3. Focal Nodular Hyperplasia (FNH)
CEUS plays a crucial role in differentiating FNH from other liver tumors. FNH presents the following characteristic findings: (a) hyperenhancement of the whole lesion, with fast centrifugal filling of the lesion, composed of central vessels and radial vascular branches at the early arterial phase (so-called “spoke-wheel appearance”) and (b) iso-enhancement of the whole lesion in the portal phase and afterward [
82,
83]. The visualization or non-visualization of a central scar in the delayed phase is usually not included in the diagnostic criteria because the visualization of an avascular area largely depends on the size of the central scar, and clear visualization of the central scar is thought to be possible less than 50% of the time [
83,
84]. In a word, these CEUS findings lead to the final diagnosis of FNH, regardless of the lesion size.
5.4. Hypervascular Hemangioma (Hy-Heman)
It has long been well known that a small number of hepatic hemangiomas are markedly hypervascular, mainly due to developed arterioportal shunts [
85]. In the past, clinicians had difficulty differentiating hemangiomas of this type from other hypervascular tumors. However, since the introduction of CEUS in the clinical setting as a detailed diagnostic tool for liver tumors, this differentiation is not so difficult. CEUS reveals not only the hypervascularity of lesions due to arterioportal shunts, but also a “cotton-wool” appearance in the periphery, leading to the diagnosis of hypervascular hemangioma [
86].
5.5. Solitary Metastasis
Colon cancer and sarcoma are frequently associated with solitary hypervascular liver metastasis, mimicking HCC [
87]. However, colon cancer metastasis usually involves many calcifications, and this B-mode finding helps in diagnosing lesions as liver metastasis from colon cancer [
88]. In addition, a high serum level increases the likelihood of diagnosing hypervascular solitary metastasis, such as CEA.
The most important point in the differential diagnosis of HCC in non-fibrotic liver from other hypervascular tumors is the presence of a capsule, which is imaged most clearly by B-mode US as lateral shadowing, which is a phenomenon caused by the refraction of US beams when passing through the capsule [
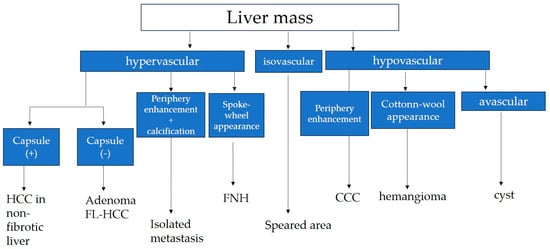
89]. A diagnostic algorithm for general clinicians is shown in
Figure 4.
Figure 4. Diagnostic algorithm of liver mass in normal hepatic function. HCC: hepatocellular carcinoma; FL-HCC: fibrolamellar HCC; FNH: focal nodular hyperplasia; CCC: cholangiocellular carcinoma.