 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Ana Carolina Tirado-Garibay | -- | 2167 | 2023-11-07 05:55:54 | | | |
| 2 | Peter Tang | Meta information modification | 2167 | 2023-11-07 06:22:45 | | |
Video Upload Options
Estrogens and their role in cancer are well-studied, and some cancer types are classified in terms of their response to them. A G protein-coupled estrogen receptor (GPER) has been described with relevance in cancer. GPER is a pleiotropic receptor with tissue-specific activity; in normal tissues, its activation is related to correct development and homeostasis, while in cancer cells, it can be pro- or anti-tumorigenic. Also, GPER replaces estrogen responsiveness in estrogen receptor alpha (ERα)-lacking cancer cell lines. One of the most outstanding activities of GPER is its role in epithelial–mesenchymal transition (EMT), which is relevant for metastasis development. In addition, the presence of this receptor in tumor microenvironment cells contributes to the phenotypic plasticity required for the dissemination and maintenance of tumors. These characteristics suggest that GPER could be a promising therapeutic target for regulating cancer development.
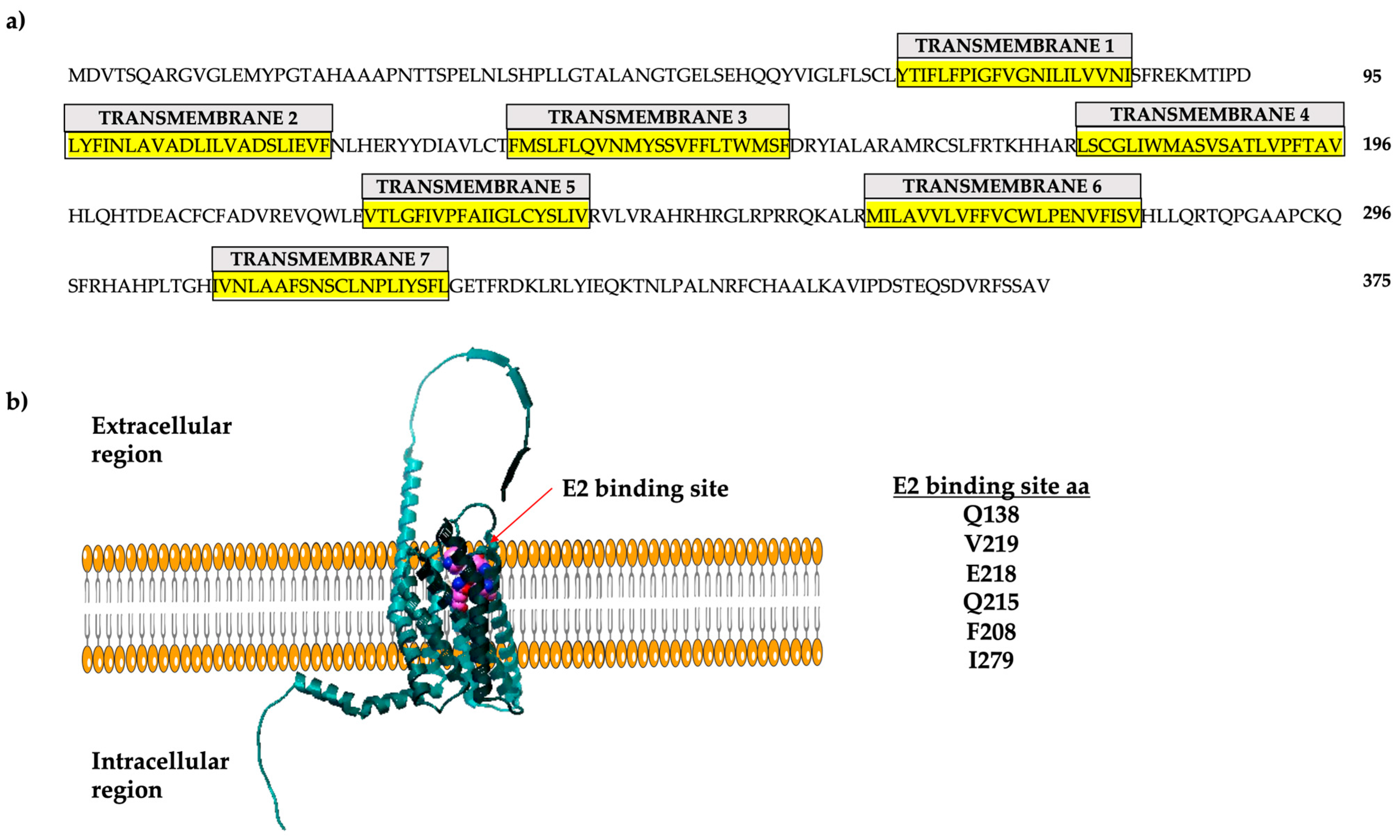
1. The G Protein-Coupled Estrogen Receptor
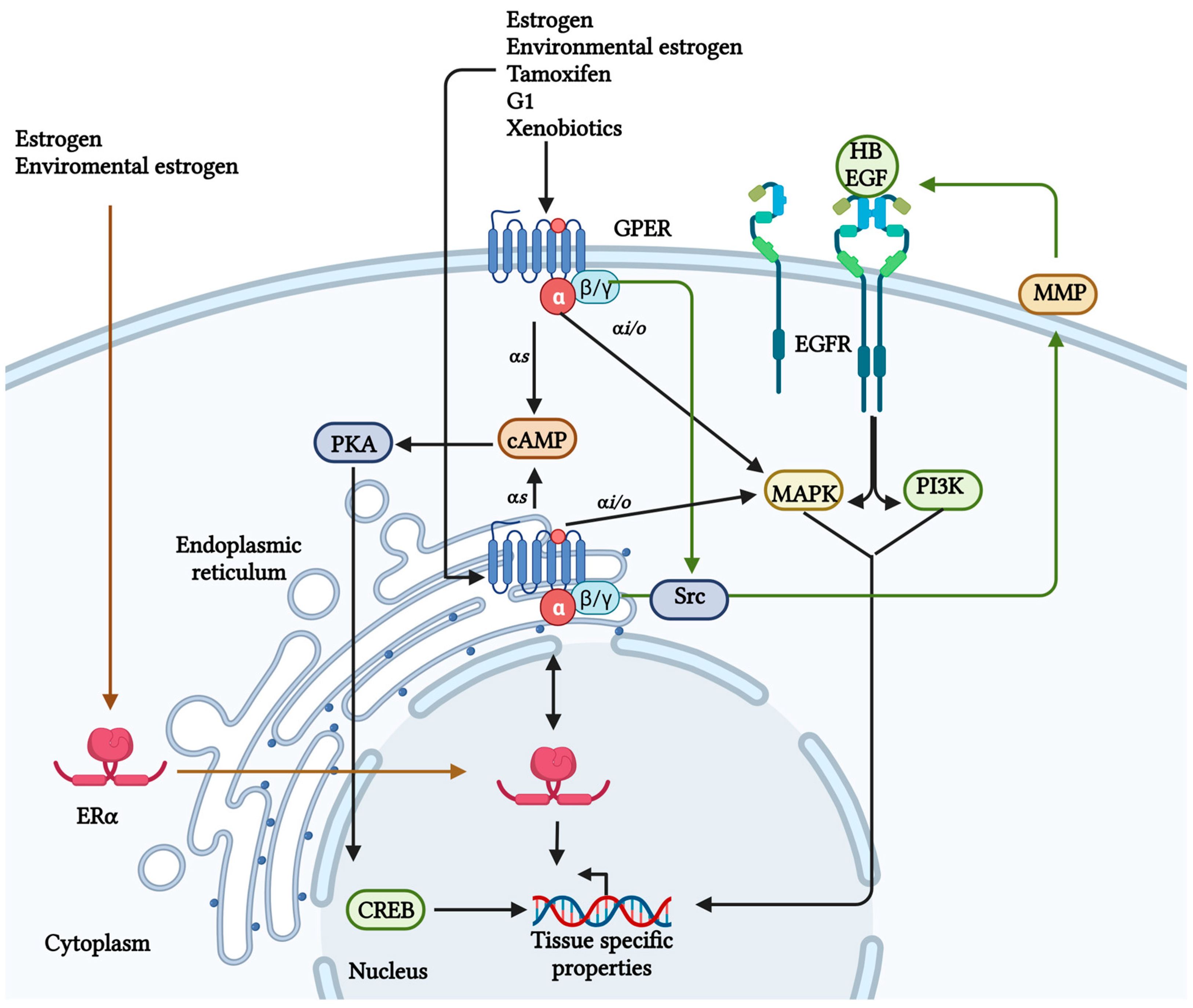
2. GPER/GPR30 Signaling in Normal Tissues
3. GPER Expression in Cancer
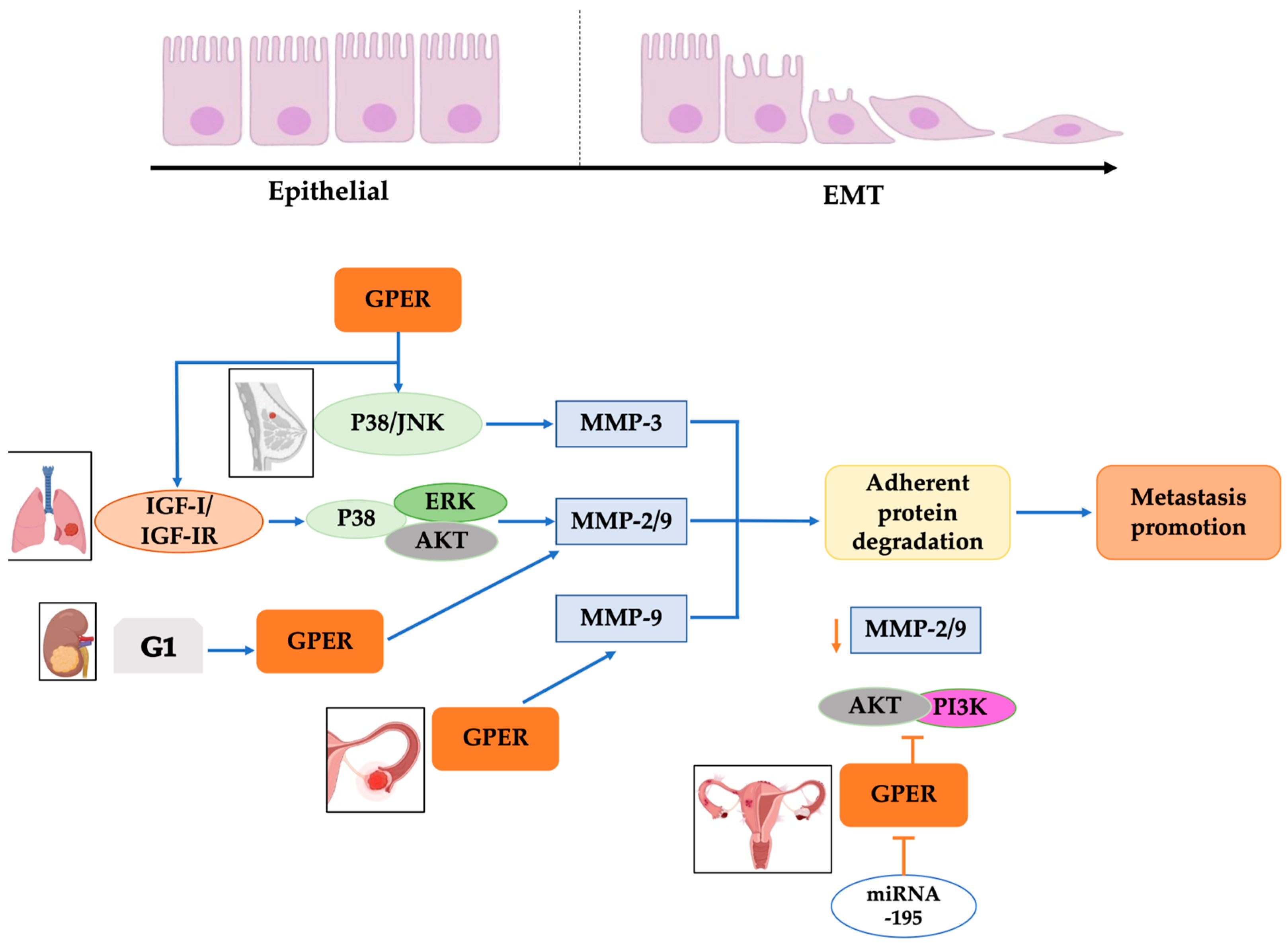
4. Epithelial–Mesenchymal Transition and Metastasis Development
5. Tumor Microenvironment Favors EMT through GPER
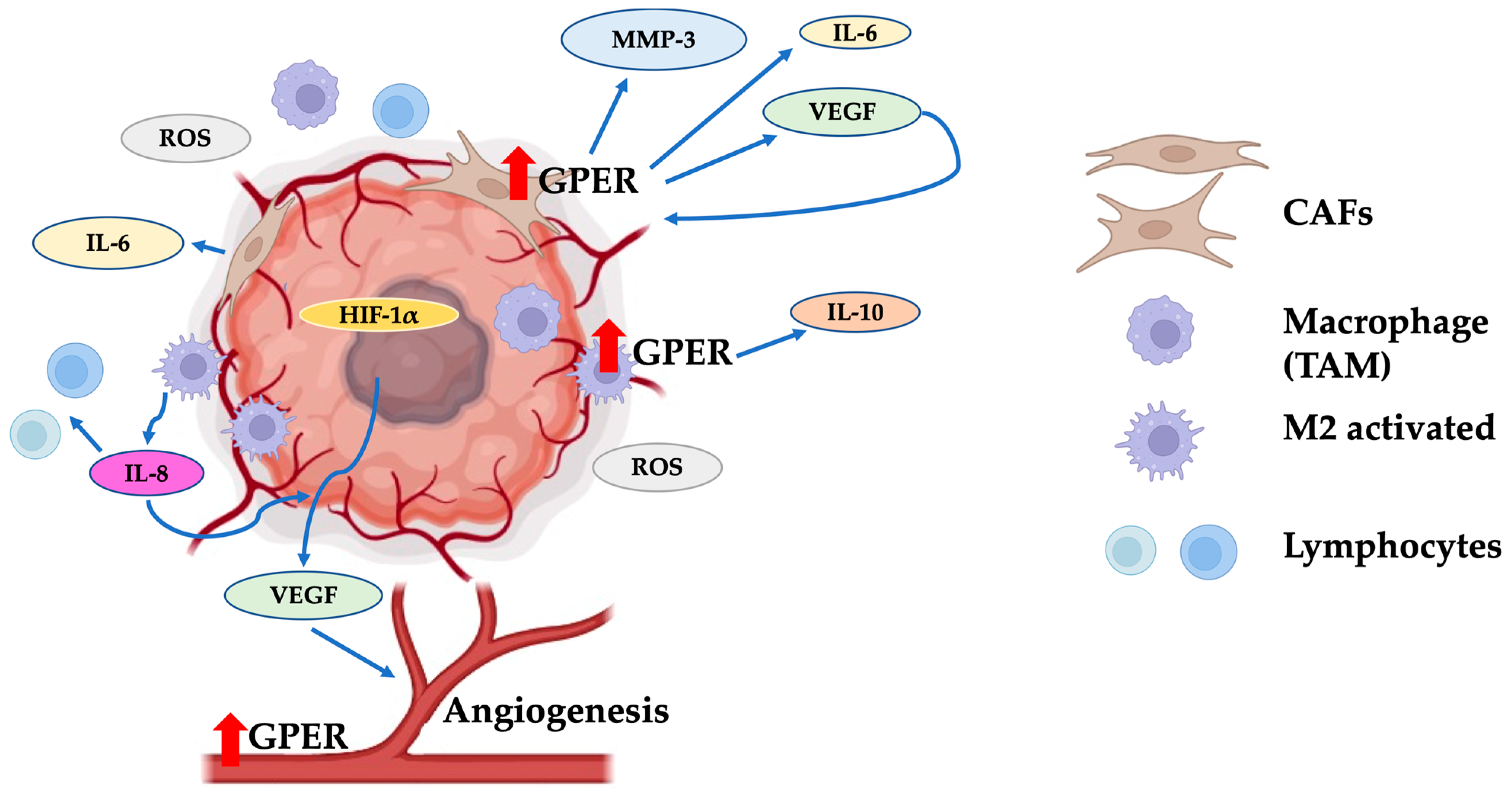
6. Role of GPER in Angiogenesis
7. Therapeutic Alternatives against Cancer Targeting GPER
References
- Owman, C.; Blay, P.; Nilsson, C.; Lolait, S.J. Cloning of Human CDNA Encoding a Novel Heptahelix Receptor Expressed in Burkitt s Lymphoma and Widely Distributed in Brain and Peripheral Tissues Communication Both in CNS and in Peripheral Tissues. Biochem. Biophys. Res. Commun. 1996, 228, 285–292.
- Carmeci, C.; Thompson, D.A.; Ring, H.Z.; Francke, U.; Weigel, R.J. Identification of a Gene (GPR30) With Homology to the G-protein-coupled Receptor Superfamily Associated with Estrogen Receptor Expression in Breast Cancer. Genomics 1997, 45, 607–617.
- Kimura, M.; Mizukami, Y.; Miura, T.; Fujimoto, K.; Kobayashi, S.; Matsuzaki, M. Orphan G Protein-Coupled Receptor, GPR41, Induces Apoptosis via a P53/Bax Pathway during Ischemic Hypoxia and Reoxygenation. J. Biol. Chem. 2001, 276, 26453–26460.
- Toran-Allerand, C.D.; Guan, X.; MacLusky, N.J.; Horvath, T.L.; Diano, S.; Singh, M.; Connolly, E.S.; Nethrapalli, I.S.; Tinnikov, A.A. ER-X: A Novel, Plasma Membrane-Associated, Putative Estrogen Receptor That Is Regulated during Development and after Ischemic Brain Injury. J. Neurosci. 2002, 22, 8391–8401.
- Filardo, E.J.; Quinn, J.; Bland, K.I.; Frackelton, A.R.J. Estrogen-Induced Activation of Erk-1 and Erk-2 Requieres the G Protein-Couple Receptor Homolog, GPER, and Occurs via Trans-Activation of the Epidermal Growth Factor Receptor through Release of HB-EGF. Mol. Endocrinol. 2000, 14, 1649–1660.
- Wyckoff, M.H.; Chambliss, K.L.; Mineo, C.; Yuhanna, I.S.; Mendelsohn, M.E.; Mumby, S.M.; Shaul, P.W. Plasma Membrane Estrogen Receptors Are Coupled to Endothelial Nitric-Oxide Synthase through Gαi. J. Biol. Chem. 2001, 276, 27071–27076.
- Kanda, N.; Watanabe, S. 17β-Estradiol Stimulates the Growth of Human Keratinocytes by Inducing Cyclin D2 Expression. J. Investig. Dermatol. 2004, 123, 319–328.
- Tutzauer, J.; Eilard, I.A.; De Valdivia, E.G.; Sw, K.; Broselid, S.; Kahn, R. Ligand-Independent G Protein—Coupled Estrogen Receptor/G Protein—Coupled Receptor 30 Activity: Lack of Receptor- Dependent Effects of G-1 and 17 b -Estradiol S. Mol. Pharmacol. 2021, 100, 271–282.
- O’Dowd, B.F.; Nguyen, T.; Marchese, A.; Cheng, R.; Lynch, K.R.; Heng, H.H.; Kolakowski, L.F., Jr.; George, S.R. Discovery of Three Novel G-protein-coupled Receptor Genes. Genomics 1998, 47, 310–313.
- Peña-Gutiérrez, K.M.; Hernández-Ortega, K.; Bello-Alvarez, C.; Camacho-Arroyo, I. Expression and Estrogen Regulation of G Protein-coupled Estrogen Receptor in Human Glioblastoma Cells. Oncol. Lett. 2022, 24, 397.
- Thomas, P.; Pang, Y.; Filardo, E.J.; Dong, J. Identity of an Estrogen Membrane Receptor Coupled to a G Protein in Human Breast Cancer Cells. Endocrinology 2005, 146, 624–632.
- Filardo, E.; Quinn, J.; Pang, Y.; Graeber, C.; Shaw, S.; Dong, J.; Thomas, P. Activation of the Novel Estrogen Receptor G Protein-Coupled Receptor 30 (GPER) at the Plasma Membrane. Endocrinology 2007, 148, 3236–3245.
- Otto, C.; Rohde-Schulz, B.; Schwarz, G.; Fuchs, I.; Klewer, M.; Brittain, D.; Langer, G.; Bader, B.; Prelle, K.; Nubbemeyer, R.G. Protein-Coupled Receptor 30 Localizes to the Endoplasmic Reticulum and Is Not Activated by Estradiol. Endocrinology 2008, 149, 4846–4856.
- Mo, Z.; Liu, M.; Yang, F.; Luo, H.; Li, Z.; Tu, G.; Yang, G. GPR30 as an Initiator of Tamoxifen Resistance in Hormone-Dependent Breast Cancer. Breast Cancer Res. 2013, 15, R114.
- Funakoshi, T.; Yanai, A.; Shinoda, K.; Kawano, M.M.; Mizukami, Y. G Protein-Coupled Receptor 30 Is an Estrogen Receptor in the Plasma Membrane. Biochem. Biophys. Res. Commun. 2006, 346, 904–910.
- Unal, H.; Karnik, S. Domain Coupling in GPCRs: The Engine for Induced Conformational Changes. Trends Pharmacol. Sci. 2012, 33, 79–88.
- Christofides, K.; Menon, R.; Jones, C.E. Endocytosis of G Protein-Coupled Receptors and Their Ligands: Is There a Role in Metal Trafficking? Cell Biochem. Biophys. 2018, 76, 329–337.
- Revankar, C.M.; Cimino, D.F.; Sklar, L.A.; Arterburn, J.B.; Prossnitz, E.R. A Transmembrane Intracellular Estrogen Receptor Mediates Rapid Cell Signaling. Science 2005, 307, 1625–1630.
- Méndez-Luna, D.; Martínez-Archundia, M.; Maroun, R.C.; Ceballos-Reyes, G.; Fragoso-Vázquez, M.J.; González-Juárez, D.E.; Correa-Basurto, J. Deciphering the GPER/GPER-Agonist and Antagonists Interactions Using Molecular Modeling Studies, Molecular Dynamics, and Docking Simulations. J. Biomol. Struct. Dyn. 2015, 33, 2161–2172.
- Pepermans, R.A.; Sharma, G.; Prossnitz, E.R. G Protein-Coupled Estrogen Receptor in Cancer and Stromal Cells: Functions and Novel Therapeutic Perspectives. Cells 2021, 10, 672.
- Ding, Q.; Chorazyczewski, J.; Gros, R.; Motulsky, H.J.; Limbird, L.E.; Feldman, R.D. Correlation of Functional and Radioligand Binding Characteristics of GPER Ligands Confirming Aldosterone as a GPER Agonist. Pharmacol. Res. Perspect. 2022, 10, e00995.
- Feng, B.; Wu, J.; Shen, B.; Jiang, F.; Feng, J. Cancer-Associated Fibroblasts and Resistance to Anticancer Therapies: Status, Mechanisms, and Countermeasures. Cancer Cell Int. 2022, 22, 166.
- Lucas, T.F.G.; Royer, C.; Siu, E.R.; Lazari, M.F.M.; Porto, C.S. Expression and Signaling of G Protein-Coupled Estrogen Receptor 1 (GPER) in Rat Sertoli Cells. Biol. Reprod. 2010, 83, 307–317.
- Gaudet, H.M.; Cheng, S.B.; Christensen, E.M.; Filardo, E.J. The G-Protein Coupled Estrogen Receptor, GPER: The inside and inside-out Story. Mol. Cell. Endocrinol. 2015, 418, 207–219.
- Tran, Q.K. Reciprocality Between Estrogen Biology and Calcium Signaling in the Cardiovascular System. Front. Endocrinol. 2020, 11, 568203.
- Tran, Q.K.; VerMeer, M.; Burgard, M.A.; Hassan, A.B.; Giles, J. Hetero-Oligomeric Complex between the G Protein-Coupled Estrogen Receptor 1 and the Plasma Membrane Ca2+-ATPase 4b. J. Biol. Chem. 2015, 290, 13293–13307.
- Xu, S.; Yu, S.; Dong, D.; Lee, L.T.O. G Protein-Coupled Estrogen Receptor: A Potential Therapeutic Target in Cancer. Front. Endocrinol. 2019, 10, 725.
- Pemberton, K.; Xu, F.; Rosato, M.; Dedert, C.; Deleon, C.; Arnatt, C. Differential Effects of the G-Protein-Coupled Estrogen Receptor (GPER) on Rat Embryonic (E18) Hippocampal and Cortical Neurons. eNeuro 2022, 9, 1–23.
- Fredette, N.C.; Meyer, M.R.; Prossnitz, E.R. Role of GPER in Estrogen-Dependent Nitric Oxide Formation and Vasodilation. J. Steroid Biochem. Mol. Biol. 2018, 176, 65–72.
- Prossnitz, E.R.; Maggiolini, M. Mechanisms of Estrogen Signaling and Gene Expression Via GPR30. Mol. Cell. Endocrinol. 2009, 308, 32–38.
- Deng, Y.; Miki, Y.; Nakanishi, A. Estradiol/GPER Affects the Integrity of Mammary Duct-like Structures in Vitro. Sci. Rep. 2020, 10, 1386.
- Scaling, A.L.; Prossnitz, E.R.; Hathaway, H.J. GPER Mediates Estrogen-Induced Signaling and Proliferation in Human Breast Epithelial Cells and Normal and Malignant Breast. Horm. Cancer 2014, 5, 146–160.
- Zhang, Y.Y.; Liu, M.Y.; Liu, Z.; Zhao, J.K.; Zhao, Y.G.; He, L.; Li, W.; Zhang, J.Q. GPER-Mediated Estrogenic Regulation of Actin Polymerization and Spatial Memory Involves SRC-1 and PI3K-MTORC2 in the Hippocampus of Female Mice. CNS Neurosci. Ther. 2019, 25, 714–733.
- Roque, C.; Mendes-Oliveira, J.; Duarte-Chendo, C.; Baltazar, G. The Role of G Protein-Coupled Estrogen Receptor 1 on Neurological Disorders. Front. Neuroendocrinol. 2019, 55, 100786.
- Zhang, C.; Liu, Q.; Yu, C.Y.; Wang, F.; Shao, Y.; Sun, K.S.; Sun, T.; Liu, J. G Protein-Coupled Estrogen Receptor 1 Knockout Deteriorates MK-801-Induced Learning and Memory Impairment in Mice. Front. Behav. Neurosci. 2020, 14, 157.
- Sharma, G.; Prossnitz, E.R. Targeting the G Protein-Coupled Estrogen Receptor (GPER) in Obesity and Diabetes. Endocr. Metab. Sci. 2021, 2, 100080.
- Luo, J.; Liu, D. Does GPER Really Function as a G Protein-Coupled Estrogen Receptor in Vivo? Front. Endocrinol. 2020, 11, 148.
- Vo, D.K.H.; Hartig, R.; Weinert, S.; Haybaeck, J.; Nass, N. G-Protein-Coupled Estrogen Receptor (GPER)-Specific Agonist G1 Induces ER Stress Leading to Cell Death in MCF-7 Cells. Biomolecules 2019, 9, 503.
- Jung, J. Role of G Protein-Coupled Estrogen Receptor in Cancer Progression. Toxicol. Res. 2019, 35, 209–214.
- Notas, G.; Kampa, M.; Castanas, E. G Protein-Coupled Estrogen Receptor in Immune Cells and Its Role in Immune-Related Diseases. Front. Endocrinol. 2020, 11, 579420.
- Tian, S.; Zhan, N.; Li, R.; Dong, W. Downregulation of G Protein-Coupled Estrogen Receptor (GPER) Is Associated with Reduced Prognosis in Patients with Gastric Cancer. Med. Sci. Monit. 2019, 25, 3115–3126.
- Han, N.; Heublein, S.; Jeschke, U.; Kuhn, C.; Hester, A.; Czogalla, B.; Mahner, S.; Rottmann, M.; Mayr, D.; Schmoeckel, E. The G-Protein-Couple Estrogen Receptor (GPER) Regulates Trimethylation of Histone H3 at Lysine 4 and Represses Migration and Proliferation of Ovarian Cancer Cells in Vitro. Cells 2021, 10, 619.
- Qiu, Y.A.; Xiong, J.; Fu, Q.; Dong, Y.; Liu, M.; Peng, M.; Jin, W.; Zhou, L.; Xu, X.; Huang, X. GPER-Induced ERK Signaling Decreases Cell Viability of Hepatocellular Carcinoma. Front. Oncol. 2021, 11, 638171.
- Liu, Q.; Chen, Z.; Jiang, G.; Zhou, Y.; Yang, X.; Huang, H.; Liu, H.; Du, J.; Wang, H. Epigenetic down Regulation of G Protein-Coupled Estrogen Receptor (GPER) Functions as a Tumor Suppressor in Colorectal Cancer. Mol. Cancer 2017, 16, 87.
- Chan, Q.K.Y.; Lam, H.; Ng, C.; Lee, A.Y.Y.; Chan, E.S.Y.; Ng, K.; Ho, S.; Lau, K. Activation of GPER Inhibits Growth of Prostate Cancer Cells via Sustained Activation of Erk1/2, c-Jun/c-Fos-Dependent Upregulation of P21, and Induction of G2 Cell-Cycle Arrest. Cell Death Differ. 2010, 17, 1511–1523.
- Schüler-Toprak, S.; Skrzypczak, M.; Ignatov, T.; Ignatov, A.; Ortmann, O.; Treeck, O.G. Protein-Coupled Estrogen Receptor 1 (GPER-1) and Agonist G-1 Inhibit Growth of Ovarian Cancer Cells by Activation of Anti-Tumoral Transcriptome Responses: Impact of GPER-1 MRNA on Survival. J. Cancer Res. Clin. Oncol. 2020, 146, 3175–3188.
- Cortes, E.; Sarper, M.; Robinson, B.; Lachowski, D.; Chronopoulos, A.; Thorpe, S.D.; Lee, D.A.; Río-Hernández, A.E. GPER Is a Mechanoregulator of Pancreatic Stellate Cells and the Tumor Microenvironment. EMBO Rep. 2019, 20, e46556.
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46.
- Jala, V.R.; Radde, B.N.; Haribabu, B.; Klinge, C.M. Enhanced Expression of G-Protein Coupled Estrogen Receptor (GPER/GPER) in Lung Cancer. BMC Cancer 2012, 12, 624.
- Xu, T.; Ma, D.; Chen, S.; Tang, R.; Yang, J.; Meng, C.; Feng, Y.; Liu, L.; Wang, J.; Luo, H. High GPER Expression in Triple-Negative Breast Cancer Is Linked to pro-Metastatic Pathways and Predicts Poor Patient Outcomes. NPJ Breast Cancer 2022, 8, 100.
- Baghban, R.; Roshangar, L.; Jahanban-Esfahlan, R.; Seidi, K.; Ebrahimi-Kalan, A.; Jaymand, M.; Kolahian, S.; Javaheri, T.; Zare, P. Tumor Microenvironment Complexity and Therapeutic Implications at a Glance. Cell Commun. Signal. 2020, 18, 59.
- Ping, Q.; Yan, R.; Cheng, X.; Wang, W.; Zhong, Y.; Hou, Z.; Shi, Y.; Wang, C.; Li, R. Cancer-Associated Fibroblasts: Overview, Progress, Challenges, and Directions. Cancer Gene Ther. 2021, 28, 984–999.
- Anderson, N.M.; Simon, M.C. Tumor Microencironment. Physiol. Behav. 2020, 30, R921–R925.
- Cortés, M.; Sanchez-Moral, L.; de Barrios, O.; Fernández-Aceñero, M.J.; Martínez-Campanario, M.; Esteve-Codina, A.; Darling, D.S.; Győrffy, B.; Lawrence, T.; Dean, D.C. Tumor-associated Macrophages (TAMs) Depend on ZEB1 for Their Cancer-promoting Roles. EMBO J. 2017, 36, 3336–3355.
- Wu, H.T.; Zhong, H.T.; Li, G.W.; Shen, J.X.; Ye, Q.Q.; Zhang, M.L.; Liu, J. Oncogenic Functions of the EMT-Related Transcription Factor ZEB1 in Breast Cancer. J. Transl. Med. 2020, 18, 51.
- Sun, X.; Mao, Y.; Wang, J.; Zu, L.; Hao, M.; Cheng, G.; Qu, Q.; Cui, D.; Keller, E.T.; Chen, X. IL-6 Secreted by Cancer-Associated Fibroblasts Induces Tamoxifen Resistance in Luminal Breast Cancer. Oncogene 2014, 33, 4450.
- Dittmer, A.; Lange, T.; Leyh, B.; Dittmer, J. Protein- And Growth-Modulatory Effects of Carcinoma-Associated Fibroblasts on Breast Cancer Cells: Role of Interleukin-6. Int. J. Oncol. 2020, 56, 258–272.
- Wu, F.; Yang, J.; Liu, J.; Wang, Y.; Mu, J.; Zeng, Q.; Deng, S.; Zhou, H. Signaling Pathways in Cancer-Associated Fibroblasts and Targeted Therapy for Cancer. Signal Transduct. Target. Ther. 2021, 6, 218.
- Masi, M.; Racchi, M.; Travelli, C.; Corsini, E.; Buoso, E. Molecular Characterization of Membrane Steroid Receptors in Hormone-Sensitive Cancers. Cells. 2021, 10, 2999.
- Avena, P.; Casaburi, I.; Zavaglia, L.; Nocito, M.C.; La Padula, D.; Rago, V.; Dong, J.; Thomas, P.; Mineo, C.; Sirianni, R. 27-Hydroxycholesterol Binds GPER and Induces Progression of Estrogen Receptor-Negative Breast Cancer. Cancers 2022, 14, 1521.
- Qin, S.; Jiang, J.; Lu, Y.; Nice, E.C.; Huang, C.; Zhang, J.; He, W. Emerging Role of Tumor Cell Plasticity in Modifying Therapeutic Response. Signal Transduct. Target 2020, 5, 228.
- Iorga, A.; Cunningham, C.M.; Moazeni, S.; Ruffenach, G.; Umar, S.; Eghbali, M. The Protective Role of Estrogen and Estrogen Receptors in Cardiovascular Disease and the Controversial Use of Estrogen Therapy. Biol. Sex. Differ. 2017, 8, 33.
- Holm, A.; Baldetorp, B.; Olde, B.; Leeb-Lundberg, L.M.F.; Nilsson, B.O. The GPER1 Agonist G-1 Attenuates Endothelial Cell Proliferation by Inhibiting DNA Synthesis and Accumulating Cells in the S and G2 Phases of the Cell Cycle. J. Vasc. Res. 2011, 48, 327–335.
- Chen, Z.; Yuhanna, I.S.; Galcheva-Gargova, Z.; Karas, R.H.; Mendelsohn, M.E.; Shaul, P.W. Estrogen Receptor α Mediates the Nongenomic Activation of Endothelial Nitric Oxide Synthase by Estrogen. J. Clin. Investig. 1999, 103, 401–406.
- Lindner, V.; Kim, S.K.; Karas, R.H.; Kuiper, G.G.J.M.; Mendelsohn, M.E. Increased Expression of Estrogen Receptor-b MRNA in Male Blood Vessels After Vascular Injury. Circ. Res. 1998, 83, 224–229.
- Zhou, L.; Chen, H.; Mao, X.; Qi, H.; Baker, P.N.; Hua, Z. G-Protein-Coupled Receptor 30 Mediates the Effects of Estrogen on Endothelial Cell Tube Formation in Vitro. Int. J. Mol. Med. 2017, 39, 1461–1467.
- Lappano, R.; Rigiracciolo, D.; De Marco, P.; Avino, S.; Cappello, A.R.; Rosano, C.; Maggiolini, M.; De Francesco, E.M. Recent Advances on the Role of G Protein-Coupled Receptors in Hypoxia-Mediated Signaling. AAPS J. 2016, 18, 305–310.
- Holm, A.; Grände, P.O.; Ludueña, R.F.; Olde, B.; Prasad, V.; Leeb-Lundberg, L.M.F.; Nilsson, B.O. The G Protein-Coupled Oestrogen Receptor 1 Agonist G-1 Disrupts Endothelial Cell Microtubule Structure in a Receptor-Independent Manner. Mol. Cell. Biochem. 2012, 366, 239–249.
- De Francesco, E.M.; Pellegrino, M.; Santolla, M.F.; Lappano, R.; Ricchio, E.; Abonante, S.; Maggiolini, M. GPER Mediates Activation of HIF1α/VEGF Signaling by Estrogens. Cancer Res. 2014, 74, 4053–4064.
- Maggiolini, M.; Santolla, M.F.; Avino, S.; Aiello, F.; Rosano, C.; Garofalo, A.; Grande, F. Identification of Two Benzopyrroloxazines Acting as Selective GPER Antagonists in Breast Cancer Cells and Cancer-Associated Fibroblasts. Futur. Med. Chem. 2015, 7, 437–448.
- Rouhimoghadam, M.; Lu, A.S.; Salem, A.K.; Filardo, E.J. Therapeutic Perspectives on the Modulation of G-Protein Coupled Estrogen Receptor, GPER, Function. Front. Endocrinol. 2020, 11, 591217.
- Arterburn, J.B.; Prossnitz, E.R. G Protein-Coupled Estrogen Receptor GPER: Molecular Pharmacology and Therapeutic Applications. Annu. Rev. Pharmacol. Toxicol. 2023, 63, 295–320.
- Geng, X.; Chen, H.; Zhao, L.; Hu, J.; Yang, W.; Li, G.; Cheng, C.; Zhao, Z.; Zhang, T.; Sun, B. Cancer-Associated Fibroblast (CAF) Heterogeneity and Targeting Therapy of CAFs in Pancreatic Cancer. Front. Cell Dev. Biol. 2021, 9, 655152.
- Rihawi, K.; Ricci, A.D.; Rizzo, A.; Brocchi, S.; Marasco, G.; Pastore, L.V.; Llimpe, F.L.R.; Golfieri, R.; Renzulli, M. Tumor-Associated Macrophages and Inflammatory Microenvironment in Gastric Cancer: Novel Translational Implications. Int. J. Mol. Sci. 2021, 22, 3805.



