 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Nandita Menon | -- | 2994 | 2023-09-13 20:30:11 | | | |
| 2 | Lindsay Dong | Meta information modification | 2994 | 2023-09-15 03:03:05 | | |
Video Upload Options
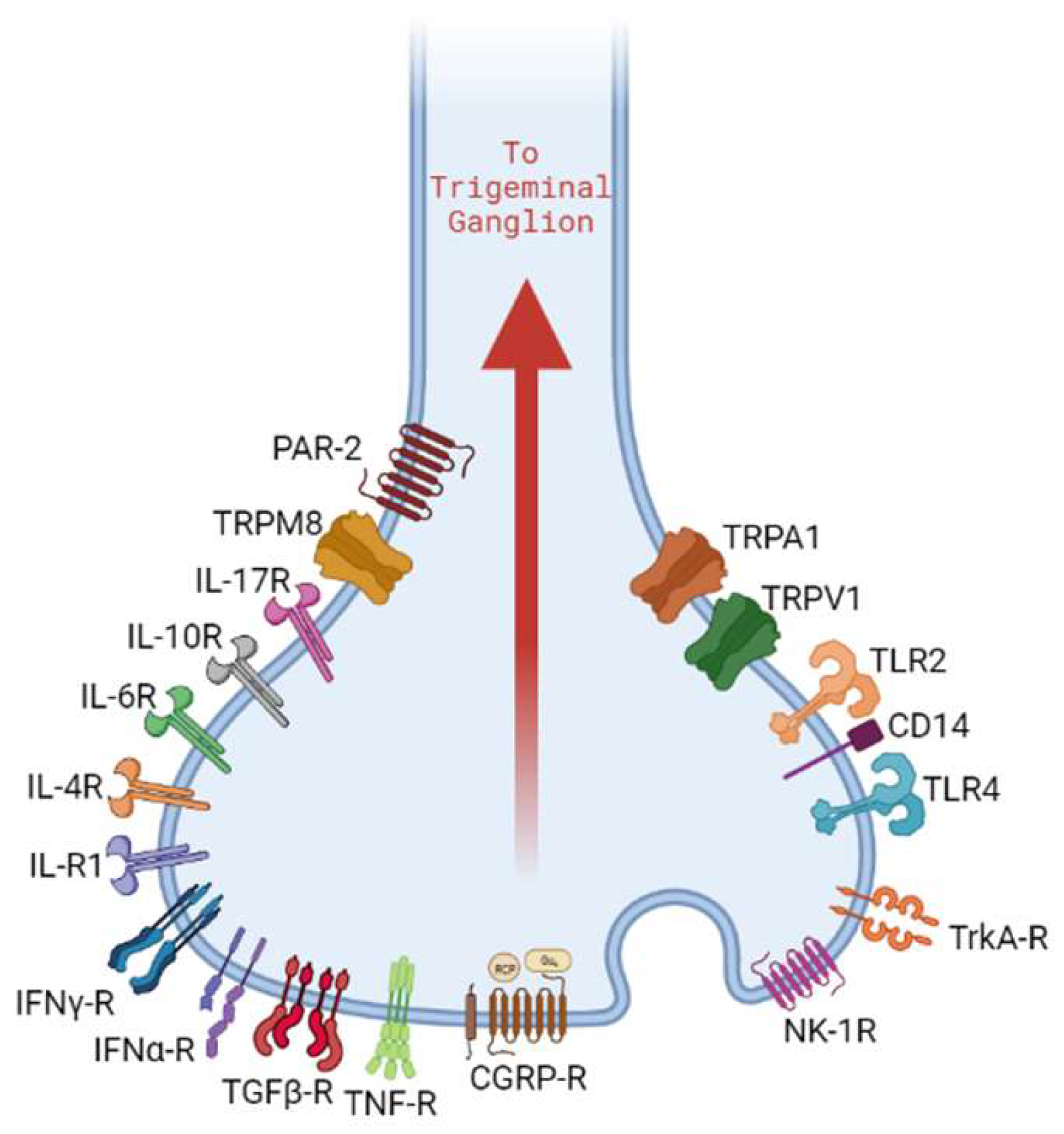
Periradicular tissues have a rich supply of peripheral afferent neurons, also known as nociceptive neurons, originating from the trigeminal nerve. While their primary function is to relay pain signals to the brain, these are known to be involved in modulating innate and adaptive immunity by initiating neurogenic inflammation (NI).
1. Introduction
2. Macrophages in Apical Periodontitis
3. Role of Macrophages in Alveolar Bone Resorption
4. Sensory Neuronal Activation in Apical Periodontitis
5. Role of Sensory Neuropeptides in Pain and Inflammation
CGRP was discovered in 1982 by Amara et al. [62]. This 37-residue peptide was found to be expressed in the central and peripheral nervous systems, promoting sensory, motor, and autonomic functions in the brain [63]. CGRP has two isoforms, α-CGRP and β-CGRP, which have over 90% similar homology and share similar biological effects in humans [64]. CALC I gene undergoes alternate splicing to generate α-CGRP, while β-CGRP is a product of CALC II gene transcription. While α-CGRP is predominant in the central and peripheral nervous systems, β-CGRP is found mainly in the enteric nervous system [64].
The CGRP receptor molecule is a G protein-coupled receptor and is composed of three components: receptor activity modifying protein 1 (RAMP1), Calcitonin-like receptor (CLR), and receptor component protein (RCP). All three components are required to form a fully functional CGRP receptor (CGRP-R). Upon activation by binding with CGRP, CGRP-R may couple with G protein α subunit, increasing the cyclical adenosine monophosphate (cAMP) levels, which activate protein kinase A (PKA).
Substance P (SP) is an undecapeptide that was first discovered in 1931 by Von Euler and Gaddum [65]. SP, neurokinin A (NKA), neuropeptide K (NPK), and neuropeptide γ (NPγ) are tachykinin neuropeptides encoded by the TAC1 gene; alternate RNA splicing and differential post-translational processing result in the expression of specific tachykinin peptides [66]. SP is best known for its role as a modulator of pain perception by altering cellular signaling pathways using G protein-coupled receptors called neurokinin 1 receptor (NK-1R) that can act through the cAMP secondary messenger system or inositol triphosphate (IP3)-diacylglycerol (DAG) system [67].
6. Neuro-Immune Interactions Modulate Inflammation and Healing in AP
7. Association of Pain with Nociceptor-Macrophage Cross-talk in AP
References
- Nair, P.N.R. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281.
- Korona-Glowniak, I.; Piatek, D.; Fornal, E.; Lukowiak, A.; Gerasymchuk, Y.; Kedziora, A.; Bugla-Płoskonska, G.; Grywalska, E.; Bachanek, T.; Malm, A. Patterns of Oral Microbiota in Patients with Apical Periodontitis. J. Clin. Med. 2021, 10, 2707.
- Hassell, M.T. Tissues and cells of the periodontium. Periodontology 2000 1993, 3, 9–38.
- Nanci, A.; Bosshardt, D.D. Structure of periodontal tissues in health and disease*. Periodontology 2000 2006, 40, 11–28.
- Hussein, H.; Kishen, A. Local Immunomodulatory Effects of Intracanal Medications in Apical Periodontitis. J. Endod. 2022, 48, 430–456.
- Jonasson, P.; Kvist, T. Diagnosis of apical periodontitis in root-filled teeth. Clin. Dent. Rev. 2018, 2, 15.
- Li, F.-C.; Kishen, A. 3D Organoids for Regenerative Endodontics. Biomolecules 2023, 13, 900.
- Chiu, I.M.; von Hehn, C.A.; Woolf, C.J. Neurogenic inflammation and the peripheral nervous system in host defense and immunopathology. Nat. Neurosci. 2012, 15, 1063–1067.
- Assas, B.M.; Pennock, J.I.; Miyan, J.A. Calcitonin gene-related peptide is a key neurotransmitter in the neuro-immune axis. Front. Neurosci. 2014, 8, 23.
- Kabata, H.; Artis, D. Neuro-immune crosstalk and allergic inflammation. J. Clin. Investig. 2019, 129, 1475–1482.
- Crosson, T.; Roversi, K.; Balood, M.; Othman, R.; Ahmadi, M.; Wang, J.-C.; Seadi Pereira, P.J.; Tabatabaei, M.; Couture, R.; Eichwald, T.; et al. Profiling of how nociceptor neurons detect danger—New and old foes. J. Intern. Med. 2019, 286, 268–289.
- Baliu-Piqué, M.; Jusek, G.; Holzmann, B. Neuroimmunological communication via CGRP promotes the development of a regulatory phenotype in TLR4-stimulated macrophages. Eur. J. Immunol. 2014, 44, 3708–3716.
- Zehnder, M.; Belibasakis, G.N. On the dynamics of root canal infections—What we understand and what we don′t. Virulence 2015, 6, 216–222.
- Azeredo, S.V.; Brasil, S.C.; Antunes, H.; Marques, F.V.; Pires, F.R.; Armada, L. Distribution of macrophages and plasma cells in apical periodontitis and their relationship with clinical and image data. J. Clin. 2017, 9, e1060–e1065.
- Márton, I.J.; Kiss, C. Overlapping Protective and Destructive Regulatory Pathways in Apical Periodontitis. J. Endod. 2014, 40, 155–163.
- Nair, P.N.R. Pathogenesis of Apical Periodontitis and the Causes of Endodontic Failures. Crit. Rev. Oral Biol. Med. 2004, 15, 348–381.
- Akamine, A.; Anan, H.; Hamachi, T.; Maeda, K. A histochemical study of the behavior of macrophages during experimental apical periodontitis in rats. J. Endod. 1994, 20, 474–478.
- Sims, M.R. A model of the anisotropic distribution of microvascular volume in the periodontal ligament of the mouse mandibular molar. Aust. Orthod. J. 1987, 10, 21–24.
- Masset, A.; Staszyk, C.; Gasse, H. The blood vessel system in the periodontal ligament of the equine cheek teeth—Part II: The micro-architecture and its functional implications in a constantly remodelling system. Ann. Anat. Anat. Anz. 2006, 188, 535–539.
- Graunaite, I.; Lodiene, G.; Maciulskiene, V. Pathogenesis of apical periodontitis: A literature review. J. Oral Maxillofac. Res. 2012, 2, e1.
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontology 2000 2014, 64, 57–80.
- Davies, L.C.; Jenkins, S.J.; Allen, J.E.; Taylor, P.R. Tissue-resident macrophages. Nat. Immunol. 2013, 14, 986–995.
- Yang, J.; Zhang, L.; Yu, C.; Yang, X.-F.; Wang, H. Monocyte and macrophage differentiation: Circulation inflammatory monocyte as biomarker for inflammatory diseases. Biomark. Res. 2014, 2, 1.
- Molteni, M.; Gemma, S.; Rossetti, C. The Role of Toll-Like Receptor 4 in Infectious and Noninfectious Inflammation. Mediat. Inflamm. 2016, 2016, 6978936.
- Rayees, S.; Rochford, I.; Joshi, J.C.; Joshi, B.; Banerjee, S.; Mehta, D. Macrophage TLR4 and PAR2 Signaling: Role in Regulating Vascular Inflammatory Injury and Repair. Front. Immunol. 2020, 11, 2091.
- Garlet, G.P.; Giannobile, W.V. Macrophages: The Bridge between Inflammation Resolution and Tissue Repair? J. Dent. Res. 2018, 97, 1079–1081.
- House, I.G.; Savas, P.; Lai, J.; Chen, A.X.Y.; Oliver, A.J.; Teo, Z.L.; Todd, K.L.; Henderson, M.A.; Giuffrida, L.; Petley, E.V.; et al. Macrophage-Derived CXCL9 and CXCL10 Are Required for Antitumor Immune Responses Following Immune Checkpoint Blockade. Clin. Cancer Res. 2020, 26, 487–504.
- Yao, Y.; Cai, X.; Ren, F.; Ye, Y.; Wang, F.; Zheng, C.; Qian, Y.; Zhang, M. The Macrophage-Osteoclast Axis in Osteoimmunity and Osteo-Related Diseases. Front. Immunol. 2021, 12, 664871.
- Italiani, P.; Boraschi, D. From Monocytes to M1/M2 Macrophages: Phenotypical vs. Functional Differentiation. Front. Immunol. 2014, 5, 514.
- Lappin, D.F.; Macleod, C.P.; Kerr, A.; Mitchell, T.J.; Kinane, D.F. Anti-inflammatory cytokine IL-10 and T cell cytokine profile in periodontitis granulation tissue. Clin. Exp. Immunol. 2001, 123, 294–300.
- Zhu, L.; Hua, F.; Ding, W.; Ding, K.; Zhang, Y.; Xu, C. The correlation between the Th17/Treg cell balance and bone health. Immun. Ageing 2020, 17, 30.
- Stern, M.H.; Dreizen, S.; Mackler, B.F.; Selbst, A.G.; Levy, B.M. Quantitative analysis of cellular composition of human periapical granuloma. J. Endod. 1981, 7, 117–122.
- Shapouri-Moghaddam, A.; Mohammadian, S.; Vazini, H.; Taghadosi, M.; Esmaeili, S.-A.; Mardani, F.; Seifi, B.; Mohammadi, A.; Afshari, J.T.; Sahebkar, A. Macrophage plasticity, polarization, and function in health and disease. J. Cell. Physiol. 2018, 233, 6425–6440.
- Kawai, T.; Matsuyama, T.; Hosokawa, Y.; Makihira, S.; Seki, M.; Karimbux, N.Y.; Goncalves, R.B.; Valverde, P.; Dibart, S.; Li, Y.-P.; et al. B and T lymphocytes are the primary sources of RANKL in the bone resorptive lesion of periodontal disease. Am. J. Pathol. 2006, 169, 987–998.
- Dallas, S.L.; Bonewald, L.F. Dynamics of the transition from osteoblast to osteocyte. Ann. N. Y. Acad. Sci. 2010, 1192, 437–443.
- Pérez-Sayáns, M.; Somoza-Martín, J.M.; Barros-Angueira, F.; Rey, J.M.G.; García-García, A. RANK/RANKL/OPG role in distraction osteogenesis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 679–686.
- Wada, T.; Nakashima, T.; Hiroshi, N.; Penninger, J.M. RANKL–RANK signaling in osteoclastogenesis and bone disease. Trends Mol. Med. 2006, 12, 17–25.
- Boyce, B.F.; Xing, L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 473, 139–146.
- Ushach, I.; Zlotnik, A. Biological role of granulocyte macrophage colony-stimulating factor (GM-CSF) and macrophage colony-stimulating factor (M-CSF) on cells of the myeloid lineage. J. Leukoc. Biol. 2016, 100, 481–489.
- Lee, M.S.; Kim, H.S.; Yeon, J.-T.; Choi, S.-W.; Chun, C.H.; Kwak, H.B.; Oh, J. GM-CSF Regulates Fusion of Mononuclear Osteoclasts into Bone-Resorbing Osteoclasts by Activating the Ras/ERK Pathway1. J. Immunol. 2009, 183, 3390–3399.
- Willis, R.D.; DiCosimo, C.J. The absence of proprioceptive nerve endings in the human periodontal ligament: The role of periodontal mechanoreceptors in the reflex control of mastication. Oral Surg. Oral Med. Oral Pathol. 1979, 48, 108–115.
- Byers, M.R. Sensory innervation of periodontal ligament of rat molars consists of unencapsulated Ruffini-like mechanoreceptors and free nerve endings. J. Comp. Neurol. 1985, 231, 500–518.
- Byers, M.R. Segregation of NGF receptor in sensory receptors, nerves and local cells of teeth and periodontium demonstrated by EM immunocytochemistry. J. Neurocytol. 1990, 19, 765–775.
- Lambrichts, I.; Creemers, J.; van Steenberghe, D. Morphology of neural endings in the human periodontal ligament: An electron microscopic study. J. Periodontal Res. 1992, 27, 191–196.
- Tabata, T.; Karita, K. Response properties of periodontal mechanosensitive fibers in the superior dental nerve of the cat. Exp. Neurol. 1986, 94, 469–478.
- Karita, K.; Tabata, T. Response fields of the periodontal mechanosensitive units in the superior alveolar nerve of the cat. Exp. Neurol. 1985, 90, 558–565.
- Tender, G.C.; Li, Y.-Y.; Cui, J.-G. Vanilloid receptor 1-positive neurons mediate thermal hyperalgesia and tactile allodynia. Spine J. 2008, 8, 351–358.
- Christine, W.; Michael, G.H. Neuroanatomy, Touch Receptor; StatPearls Publishing: St. Petersburg, FL, USA, 2023.
- Mengel, M.K.C.; Jyväsjärvi, E.; Kniffki, K.-D. Identification and characterization of afferent periodontal C fibres in the cat. PAIN 1992, 48, 413–420.
- Bender, I.B. Pulpal Pain Diagnosis—A Review. J. Endod. 2000, 26, 175–179.
- Toledo Mauriño, J.J.; Fonseca-Camarillo, G.; Furuzawa-Carballeda, J.; Barreto-Zuñiga, R.; Martínez Benítez, B.; Granados, J.; Yamamoto-Furusho, J.K. TRPV Subfamily (TRPV2, TRPV3, TRPV4, TRPV5, and TRPV6) Gene and Protein Expression in Patients with Ulcerative Colitis. J. Immunol. Res. 2020, 2020, 2906845.
- Jara-Oseguera, A.; Simon, A.S.; Rosenbaum, T. TRPV1: On the Road to Pain Relief. Curr. Mol. Pharmacol. 2008, 1, 255–269.
- Samanta, A.; Hughes, T.E.T.; Moiseenkova-Bell, V.Y. Transient Receptor Potential (TRP) Channels. In Membrane Protein Complexes: Structure and Function; Harris, J.R., Boekema, E.J., Eds.; Springer: Singapore, 2018; pp. 141–165.
- Zygmunt, P.M.; Högestätt, E.D. TRPA1. In Mammalian Transient Receptor Potential (TRP) Cation Channels: Volume I; Nilius, B., Flockerzi, V., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 583–630.
- Cao, E.; Liao, M.; Cheng, Y.; Julius, D. TRPV1 structures in distinct conformations reveal activation mechanisms. Nature 2013, 504, 113–118.
- Liao, M.; Cao, E.; Julius, D.; Cheng, Y. Structure of the TRPV1 ion channel determined by electron cryo-microscopy. Nature 2013, 504, 107–112.
- Helley, M.P.; Abate, W.; Jackson, S.K.; Bennett, J.H.; Thompson, S.W.N. The expression of Toll-like receptor 4, 7 and co-receptors in neurochemical sub-populations of rat trigeminal ganglion sensory neurons. Neuroscience 2015, 310, 686–698.
- Wadachi, R.; Hargreaves, K. Trigeminal nociceptors express TLR-4 and CD14: A mechanism for pain due to infection. J. Dent. Res. 2006, 85, 49–53.
- Diogenes, A.; Ferraz, C.C.R.; Akopian, A.N.; Henry, M.A.; Hargreaves, K.M. LPS Sensitizes TRPV1 via Activation of TLR4 in Trigeminal Sensory Neurons. J. Dent. Res. 2011, 90, 759–764.
- Meseguer, V.; Alpizar, Y.A.; Luis, E.; Tajada, S.; Denlinger, B.; Fajardo, O.; Manenschijn, J.-A.; Fernández-Peña, C.; Talavera, A.; Kichko, T.; et al. TRPA1 channels mediate acute neurogenic inflammation and pain produced by bacterial endotoxins. Nat. Commun. 2014, 5, 3125.
- Ferraz, C.C.R.; Henry, M.A.; Hargreaves, K.M.; Diogenes, A. Lipopolysaccharide From Porphyromonas gingivalis Sensitizes Capsaicin-Sensitive Nociceptors. J. Endod. 2011, 37, 45–48.
- Amara, S.G.; Jonas, V.; Rosenfeld, M.G.; Ong, E.S.; Evans, R.M. Alternative RNA processing in calcitonin gene expression generates mRNAs encoding different polypeptide products. Nature 1982, 298, 240–244.
- Fisher, L.A.; Kikkawa, D.O.; Rivier, J.E.; Amara, S.G.; Evans, R.M.; Rosenfeld, M.G.; Vale, W.W.; Brown, M.R. Stimulation of noradrenergic sympathetic outflow by calcitonin gene-related peptide. Nature 1983, 305, 534–536.
- Russell, F.A.; King, R.; Smillie, S.-J.; Kodji, X.; Brain, S.D. Calcitonin Gene-Related Peptide: Physiology and Pathophysiology. Physiol. Rev. 2014, 94, 1099–1142.
- v. Euler, U.S.; Gaddum, J.H. An unidentified depressor substance in certain tissue extracts. J. Physiol. 1931, 72, 74–87.
- Krause, J.E.; Takeda, Y.; Hershey, A.D. Structure, Functions, and Mechanisms of Substance P Receptor Action. J. Investig. Dermatol. 1992, 98, S2–S7.
- Mashaghi, A.; Marmalidou, A.; Tehrani, M.; Grace, P.M.; Pothoulakis, C.; Dana, R. Neuropeptide substance P and the immune response. Cell. Mol. Life Sci. 2016, 73, 4249–4264.
- Arslan, H.; Yıldız, E.D.; Köseoğlu, S. Effects of endodontic treatment on salivary levels of CGRP and substance P: A pilot study. Restor. Dent. Endod. 2020, 45, e40.
- Wakisaka, S. Neuropeptides in the dental pulp: Distribution, origins, and correlation. J. Endod. 1990, 16, 67–69.
- Caviedes-Bucheli, J.; Muñoz, H.R.; Azuero-Holguín, M.M.; Ulate, E. Neuropeptides in Dental Pulp: The Silent Protagonists. J. Endod. 2008, 34, 773–788.
- Kato, J.; Wakisaka, S.; Kurisu, K. Immunohistochemical Changes in the Distribution of Nerve Fibers in the Periodontal Ligament during an Experimental Tooth Movement of the Rat Molar. Acta Anat. 2008, 157, 53–62.
- Caviedes-Bucheli, J.; Castellanos, F.; Vasquez, N.; Ulate, E.; Munoz, H.R. The influence of two reciprocating single-file and two rotary-file systems on the apical extrusion of debris and its biological relationship with symptomatic apical periodontitis. A systematic review and meta-analysis. Int. Endod. J. 2016, 49, 255–270.
- Pradeep, A.R.; Raj, S.; Aruna, G.; Chowdhry, S. Gingival crevicular fluid and plasma levels of neuropeptide Substance-P in periodontal health, disease and after nonsurgical therapy. J. Periodontal Res. 2009, 44, 232–237.
- Lundy, F.T.; Mullally, B.H.; Burden, D.J.; Lamey, P.-J.; Shaw, C.; Linden, G.J. Changes in substance P and neurokinin A in gingival crevicular fluid in response to periodontal treatment. J. Clin. Periodontol. 2000, 27, 526–530.
- Burgener, B.; Ford, A.R.; Situ, H.; Fayad, M.I.; Hao, J.J.; Wenckus, C.S.; Johnson, B.R.; BeGole, E.A.; George, A. Biologic Markers for Odontogenic Periradicular Periodontitis. J. Endod. 2010, 36, 1307–1310.
- Sacerdote, P.; Levrini, L. Peripheral Mechanisms of Dental Pain: The Role of Substance P. Mediat. Inflamm. 2012, 2012, 951920.
- Takahashi, N.; Matsuda, Y.; Sato, K.; de Jong, P.R.; Bertin, S.; Tabeta, K.; Yamazaki, K. Neuronal TRPV1 activation regulates alveolar bone resorption by suppressing osteoclastogenesis via CGRP. Sci. Rep. 2016, 6, 29294.
- Stashenko, P.; Teles, R.; d’Souza, R. Periapical inflammatory responses and their modulation. Crit. Rev. Oral Biol. Med. 1998, 9, 498–521.
- Kim, S.; Dorscher-Kim, J. Effects of Substance P on Blood Flow of the Dental Pulp in Dogs. In Proceedings of the Substance P and Neurokinins; Springer-Verlag New York Inc.: New York, NY, USA, 1987; pp. 197–199.
- Takeda, K.; Akira, S. Toll-Like Receptors. Curr. Protoc. Immunol. 2007, 77, 14.12.11–14.12.13.
- Ma, W.; Dumont, Y.; Vercauteren, F.; Quirion, R. Lipopolysaccharide induces calcitonin gene-related peptide in the RAW264. 7 macrophage cell line. Immunology 2010, 130, 399–409.
- Lai, J.-P.; Ho, W.Z.; Kilpatrick, L.E.; Wang, X.; Tuluc, F.; Korchak, H.M.; Douglas, S.D. Full-length and truncated neurokinin-1 receptor expression and function during monocyte/macrophage differentiation. Proc. Natl. Acad. Sci. USA 2006, 103, 7771–7776.
- Marriott, I.; Bost, K.L. IL-4 and IFN-γ Up-Regulate Substance P Receptor Expression in Murine Peritoneal Macrophages1. J. Immunol. 2000, 165, 182–191.
- Simeonidis, S.; Castagliuolo, I.; Pan, A.; Liu, J.; Wang, C.-C.; Mykoniatis, A.; Pasha, A.; Valenick, L.; Sougioultzis, S.; Zhao, D.; et al. Regulation of the NK-1 receptor gene expression in human macrophage cells via an NF-κB site on its promoter. Proc. Natl. Acad. Sci. USA 2003, 100, 2957–2962.
- Goldman, R.; Bar-Shavit, Z.; Shezen, E.; Terry, S.; Blumberg, S. Enhancement of Phagocytosis by Neurotensin, a Newly Found Biological Activity of the Neuropeptide. In Macrophages and Natural Killer Cells: Regulation and Function; Normann, S.J., Sorkin, E., Eds.; Springer US: Boston, MA, USA, 1982; pp. 133–141.
- Hartung, H.-P. Activation of macrophages by neuropeptides. Brain Behav. Immun. 1988, 2, 275–281.
- Ruff, M.R.; Wahl, S.M.; Pert, C.B. Substance P receptor-mediated chemotaxis of human monocytes. Peptides 1985, 6, 107–111.
- Hartung, H.-P.; Toyka, K.V. Substance P, the Immune System and Inflammation. Int. Rev. Immunol. 1989, 4, 229–249.
- Cozens, P.J.; Rowe, F.M. Substance-P is a potent inducer of tnf and IL-1 secretion by macrophages—A potential role for tnf in the pathogenesis of asthma. Immunobiology 1987, 175, 7.
- Saito, I.; Ishii, K.; Hanada, K.; Sato, O.; Maeda, T. Responses of calcitonin gene-related peptide-immunopositive nerve fibres in the periodontal ligament of rat molars to experimental tooth movement. Arch. Oral Biol. 1991, 36, 689–692.
- Wakisaka, S.; Nishikawa, S.; Ichikawa, H.; Matsuo, S.; Takano, Y.; Akai, M. The distribution and origin of substance P-like immunoreactivity in the rat molar pulp and periodontal tissues. Arch. Oral Biol. 1985, 30, 813–818.
- Heyeraas, K.J.; Kvinnsland, I.; Byers, M.R.; Jacobsen, E.B. Nerve fibers immunoreactive to protein gene product 9.5, calcitonin gene-related peptide, substance P, and neuropeptide Y in the dental pulp, periodontal ligament, and gingiva in cats. Acta Odontol. Scand. 1993, 51, 207–221.
- Gašperšič, R.; Kovačič, U.; Cör, A.; Skalerič, U. Unilateral ligature-induced periodontitis influences the expression of neuropeptides in the ipsilateral and contralateral trigeminal ganglion in rats. Arch. Oral Biol. 2008, 53, 659–665.
- Kabashima, H.; Nagata, K.; Maeda, K.; Iijima, T. Involvement of substance P, mast cells, TNF-α and ICAM-1 in the infiltration of inflammatory cells in human periapical granulomas. J. Oral Pathol. Med. 2002, 31, 175–180.
- de Avila, E.D.; de Molon, R.S.; de Godoi Gonçalves, D.A.; Camparis, C.M. Relationship between levels of neuropeptide Substance P in periodontal disease and chronic pain: A literature review. J. Investig. Clin. Dent. 2014, 5, 91–97.
- Ferrin, J.; Kirakodu, S.; Jensen, D.; Al-Attar, A.; Peyyala, R.; Novak, M.J.; Dawson, D.; Al-Sabbagh, M.; Stromberg, A.J.; Orraca, L.; et al. Gene expression analysis of neuropeptides in oral mucosa during periodontal disease in non-human primates. J. Periodontol. 2018, 89, 858–866.
- Owan, I.; Ibaraki, K. The role of calcitonin gene-related peptide (CGRP) in macrophages: The presence of functional receptors and effects on proliferation and differentiation into osteoclast-like cells. Bone Miner. 1994, 24, 151–164.
- Fernandez, S.; Knopf, M.A.; Bjork, S.K.; McGillis, J.P. Bone Marrow-Derived Macrophages Express Functional CGRP Receptors and Respond to CGRP by Increasing Transcription of c-fos and IL-6 mRNA. Cell. Immunol. 2001, 209, 140–148.
- Ma, W.; Quirion, R. Increased calcitonin gene-related peptide in neuroma and invading macrophages is involved in the up-regulation of interleukin-6 and thermal hyperalgesia in a rat model of mononeuropathy. J. Neurochem. 2006, 98, 180–192.
- Frielingsdorf, H.; Simpson, D.R.; Thal, L.J.; Pizzo, D.P. Nerve growth factor promotes survival of new neurons in the adult hippocampus. Neurobiol. Dis. 2007, 26, 47–55.
- Ulupinar, E.; Jacquin, M.F.; Erzurumlu, R.S. Differential effects of NGF and NT-3 on embryonic trigeminal axon growth patterns. J. Comp. Neurol. 2000, 425, 202–218.
- Minnone, G.; De Benedetti, F.; Bracci-Laudiero, L. NGF and Its Receptors in the Regulation of Inflammatory Response. Int. J. Mol. Sci. 2017, 18, 1028.
- Salio, C.; Averill, S.; Priestley, J.V.; Merighi, A. Costorage of BDNF and neuropeptides within individual dense-core vesicles in central and peripheral neurons. Dev. Neurobiol. 2007, 67, 326–338.
- Ehrhard, P.B.; Ganter, U.; Stalder, A.; Bauer, J.; Otten, U. Expression of functional trk protooncogene in human monocytes. Proc. Natl. Acad. Sci. USA 1993, 90, 5423–5427.
- Sun, J.; Ramnath, R.D.; Zhi, L.; Tamizhselvi, R.; Bhatia, M. Substance P enhances NF-κB transactivation and chemokine response in murine macrophages via ERK1/2 and p38 MAPK signaling pathways. Am. J. Physiol. Cell Physiol. 2008, 294, C1586–C1596.
- Lee, S.-K.; Pi, S.-H.; Kim, S.-H.; Min, K.-S.; Lee, H.-J.; Chang, H.-S.; Kang, K.-H.; Kim, H.-R.; Shin, H.-I.; Kim, E.-C. Substance P regulates macrophage inflammatory protein 3α/chemokine C-C ligand 20 (CCL20) with heme oxygenase-1 in human periodontal ligament cells. Clin. Exp. Immunol. 2007, 150, 567–575.
- Keane, M.P.; Strieter, R.M.; Belperio, J.A. Macrophage inflammatory protein. In Encyclopedia of Respiratory Medicine; Laurent, G.J., Shapiro, S.D., Eds.; Academic Press: Oxford, UK, 2006; pp. 1–5.
- Deshmane, S.L.; Kremlev, S.; Amini, S.; Sawaya, B.E. Monocyte Chemoattractant Protein-1 (MCP-1): An Overview. J. Interferon Cytokine Res. 2009, 29, 313–326.
- Jiang, M.H.; Chung, E.; Chi, G.F.; Ahn, W.; Lim, J.E.; Hong, H.S.; Kim, D.W.; Choi, H.; Kim, J.; Son, Y. Substance P induces M2-type macrophages after spinal cord injury. Neuroreport 2012, 23, 786–792.
- Hong, H.S.; Son, Y. Substance P ameliorates collagen II-induced arthritis in mice via suppression of the inflammatory response. Biochem. Biophys. Res. Commun. 2014, 453, 179–184.
- Pinho-Ribeiro, F.A.; Verri, W.A.; Chiu, I.M. Nociceptor Sensory Neuron–Immune Interactions in Pain and Inflammation. Trends Immunol. 2017, 38, 5–19.
- Rechenberg, D.K.; Munir, A.; Zehnder, M. Correlation between the clinically diagnosed inflammatory process and periapical index scores in severely painful endodontically involved teeth. Int. Endod. J. 2021, 54, 172–180.
- Wideman, T.H.; Edwards, R.R.; Walton, D.M.; Martel, M.O.; Hudon, A.; Seminowicz, D.A. The Multimodal Assessment Model of Pain: A Novel Framework for Further Integrating the Subjective Pain Experience Within Research and Practice. Clin. J. Pain 2019, 35, 212.
- Wilcox, C.E.; Mayer, A.R.; Teshiba, T.M.; Ling, J.; Smith, B.W.; Wilcox, G.L.; Mullins, P.G. The Subjective Experience of Pain: An FMRI Study of Percept-Related Models and Functional Connectivity. Pain Med. 2015, 16, 2121–2133.
- Tarnawski, L.; Olofsson, P.S. Inflammation neuroscience: Neuro-immune crosstalk and interfaces. Clin. Transl. Immunol. 2021, 10, e1352.


