 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Jacobo Porto Álvarez | -- | 2186 | 2023-09-13 17:12:06 | | | |
| 2 | Lindsay Dong | Meta information modification | 2186 | 2023-09-15 03:00:39 | | |
Video Upload Options
Acute ischemic stroke (AIS) is the loss of neurological function due to a sudden reduction in cerebral blood flow and is a leading cause of disability and death worldwide. The field of radiological imaging has experienced growth in recent years, which could be boosted by the advent of artificial intelligence. One of the latest innovations in artificial intelligence is radiomics, which is based on the fact that a large amount of quantitative data can be extracted from radiological images, from which patterns can be identified and associated with specific pathologies. Since its inception, radiomics has been particularly associated with the field of oncology and has shown promising results in a wide range of clinical situations. The performance of radiomics in non-tumour pathologies has been increasingly explored in recent years, and the results continue to be promising.
1. Introduction
2. Radiomics
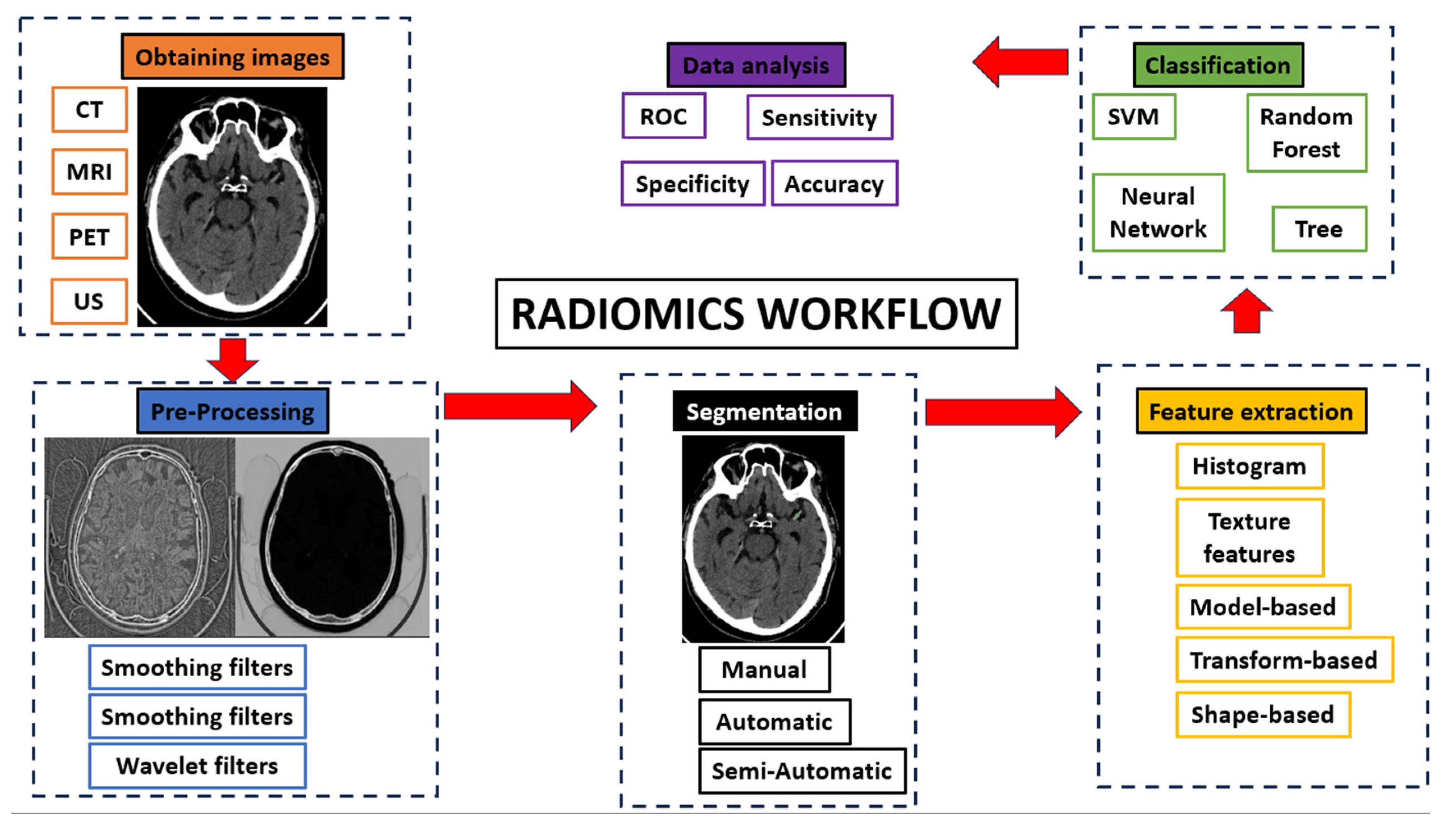
2.1. Radiomics Workflow
-
Obtaining images: Radiomics can be applied to all types of medical imaging. There are published articles on the performance of radiomics in ultrasound, Non-Contrast Enhancement-CT (NCECT), Computed Tomography Angiography (CTA), MRI and PET. In this step, there can be a great deal of heterogeneity when using images acquired in different hospitals or even on different machines within the same hospital.
-
Pre-processing: The quality of the images can be improved by using the pre-processing tools. In this step, some image filters are used to reduce noise. The aim is to increase the predictive power of the classifiers [15].
-
Segmentation: In this step, the region of interest is selected in the radiological image. The segmentation of this region can be performed in three ways: manual, semi-automatic and automatic. Manual segmentation is the gold standard and the most commonly used method in the studies. The main advantage of this model is the intervention of an expert radiologist in its performance. The main disadvantage of this model is the time required to manually segment the entire region of interest [16]. Automatic segmentation is based on automatic detection of the region of interest without human intervention. Finally, semi-automatic segmentation is performed under the supervision of an expert radiologist who can edit an initial automatic pre-segmentation. The advantage of this method is the speed of the segmentation and the fact that the human component remains [17]. With today’s increasingly sophisticated segmentation software, semi-automatic 3D segmentation of an area of interest can be performed quickly and comfortably for the radiologist.
-
Feature extraction and classification: There is a wealth of numerical data that can be extracted from medical images, known as radiomic features. There are several classes of radiomic features: Histogram features (grey level mean, maximum, minimum, variance and percentiles), texture features (absolute gradient, grey level co-occurrence matrix—GLCM—, grey level run length matrix—GLRLM—, grey level size zone matrix—GLSZM—, grey level distance zone matrix—GLDZM—, Neighborhood Grey Level Difference Matrix—NGTDM—, and Neighborhood Grey Level Dependence Matrix—NGLDM—), model-based features, transform-based features (Fourier, Garbor and Wavelet) and shape-based features (geometric properties of ROIs) [18]. These numerical data are classified by automatic classifiers. These classifiers are capable of recognizing different groups of patterns depending on the objective we set for them.
-
Data analysis.
2.2. Radiomics in AIS
2.3. Prognostic Prediction
2.4. Detection of Ischemic Stroke
2.5. Treatment Predictions
2.6. Prediction of Complications after AIS
2.7. Etiology Prediction
2.8. Time since Stroke Prediction
2.9. Differentiation Hemorrhage from Iodinated Contrast Extravasation after Thrombectomy
3. Conclusions
References
- Phipps, M.S.; Cronin, C.A. Management of acute ischemic stroke. BMJ 2020, 368, l6983.
- World Health Organization. Global Health Estimates. Available online: https://www.who.int/data/global-health-estimates (accessed on 9 December 2020).
- Saini, V.; Guada, L.; Yavagal, D.R. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions. Neurology 2021, 97 (Suppl. S2), S6–S16.
- Broderick, J.P.; Palesch, Y.Y.; Demchuk, A.M.; Yeatts, S.D.; Khatri, P.; Hill, M.D.; Jauch, E.C.; Jovin, T.G.; Yan, B.; Silver, F.L.; et al. Endovascular Therapy after Intravenous t-PA versus t-PA Alone for Stroke. N. Engl. J. Med. 2013, 368, 893–903, Erratum in N. Engl. J. Med. 2013, 368, 893–903.
- Kidwell, C.S.; Jahan, R.; Gornbein, J.; Alger, J.R.; Nenov, V.; Ajani, Z.; Feng, L.; Meyer, B.C.; Olson, S.; Schwamm, L.H.; et al. A Trial of Imaging Selection and Endovascular Treatment for Ischemic Stroke. N. Engl. J. Med. 2013, 368, 914–923.
- Fargen, K.M.; Singla, A.; Mocco, J. The New England Journal of Medicine Stroke Trials: What Do They Really Mean? Neurosurgery 2015, 62, 137–140.
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577.
- Porto-Álvarez, J.; Barnes, G.T.; Villanueva, A.; García-Figueiras, R.; Baleato-González, S.; Zapico, E.H.; Souto-Bayarri, M. Digital Medical X-ray Imaging, CAD in Lung Cancer and Radiomics in Colorectal Cancer: Past, Present and Future. Appl. Sci. 2023, 13, 2218.
- Singh, G.; Manjila, S.; Sakla, N.; True, A.; Wardeh, A.H.; Beig, N.; Vaysberg, A.; Matthews, J.; Prasanna, P.; Spektor, V. Radiomics and radiogenomics in gliomas: A contemporary update. Br. J. Cancer 2021, 125, 641–657.
- Anagnostopoulos, A.K.; Gaitanis, A.; Gkiozos, I.; Athanasiadis, E.I.; Chatziioannou, S.N.; Syrigos, K.N.; Thanos, D.; Chatziioannou, A.N.; Papanikolaou, N. Radiomics/Radiogenomics in Lung Cancer: Basic Principles and Initial Clinical Results. Cancers 2022, 14, 1657.
- Porto-Álvarez, J.; Cernadas, E.; Martínez, R.A.; Fernández-Delgado, M.; Zapico, E.H.; González-Castro, V.; Baleato-González, S.; García-Figueiras, R.; Antúnez-López, J.R.; Souto-Bayarri, M. CT-Based Radiomics to Predict KRAS Mutation in CRC Patients Using a Machine Learning Algorithm: A Retrospective Study. Biomedicines 2023, 11, 2144.
- Chen, Q.; Xia, T.; Zhang, M.; Xia, N.; Liu, J.; Yang, Y. Radiomics in Stroke Neuroimaging: Techniques, Applications, and Challenges. Aging Dis. 2021, 12, 143–154.
- Jain, M.; Rai, C.S.; Jain, J. A Novel Method for Differential Prognosis of Brain Degenerative Diseases Using Radiomics-Based Textural Analysis and Ensemble Learning Classifiers. Comput. Math. Methods Med. 2021, 2021, 7965677.
- Alwalid, O.; Long, X.; Xie, M.; Yang, J.; Cen, C.; Liu, H.; Han, P. CT Angiography-Based Radiomics for Classification of Intracranial Aneurysm Rupture. Front. Neurol. 2021, 12, 619864.
- Demircioğlu, A. The effect of preprocessing filters on predictive performance in radiomics. Eur. Radiol. Exp. 2022, 6, 40.
- Van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging-”how-to” guide and critical reflection. Insights Imaging 2020, 11, 91.
- Parmar, C.; Velazquez, E.R.; Leijenaar, R.; Jermoumi, M.; Carvalho, S.; Mak, R.H.; Mitra, S.; Shankar, B.U.; Kikinis, R.; Haibe-Kains, B.; et al. Robust Radiomics Feature Quantification Using Semiautomatic Volumetric Segmentation. PLoS ONE 2014, 9, e102107.
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495.
- Guan, Y.; Wang, P.; Wang, Q.; Li, P.; Zeng, J.; Qin, P.; Meng, Y. Separability of Acute Cerebral Infarction Lesions in CT Based Radiomics: Toward Artificial Intelligence-Assisted Diagnosis. BioMed Res. Int. 2020, 2020, 8864756.
- Guo, Y.; Yang, Y.; Cao, F.; Wang, M.; Luo, Y.; Guo, J.; Liu, Y.; Zeng, X.; Miu, X.; Zaman, A.; et al. A Focus on the Role of DSC-PWI Dynamic Radiomics Features in Diagnosis and Outcome Prediction of Ischemic Stroke. J. Clin. Med. 2022, 11, 5364.
- Su, J.-H.; Meng, L.-W.; Dong, D.; Zhuo, W.-Y.; Wang, J.-M.; Liu, L.-B.; Qin, Y.; Tian, Y.; Tian, J.; Li, Z.-H. Noninvasive model for predicting future ischemic strokes in patients with silent lacunar infarction using radiomics. BMC Med. Imaging 2020, 20, 77.
- Hofmeister, J.; Bernava, G.; Rosi, A.; Vargas, M.I.; Carrera, E.; Montet, X.; Burgermeister, S.; Poletti, P.-A.; Platon, A.; Lovblad, K.-O.; et al. Clot-Based Radiomics Predict a Mechanical Thrombectomy Strategy for Successful Recanalization in Acute Ischemic Stroke. Stroke 2020, 51, 2488–2494.
- Zhang, H.; Polson, J.; Nael, K.; Salamon, N.; Yoo, B.; Speier, W.; Arnold, C. A Machine Learning Approach to Predict Acute Ischemic Stroke Thrombectomy Reperfusion using Discriminative MR Image Features. In Proceedings of the 2021 IEEE EMBS International Conference on Biomedical and Health Informatics (BHI), Virtual, 27–30 July 2021.
- Qiu, W.; Kuang, H.; Nair, J.; Assis, Z.; Najm, M.; McDougall, C.; McDougall, B.; Chung, K.; Wilson, A.; Goyal, M.; et al. Radiomics-Based Intracranial Thrombus Features on CT and CTA Predict Recanalization with Intravenous Alteplase in Patients with Acute Ischemic Stroke. Am. J. Neuroradiol. 2019, 40, 39–44.
- Fu, B.; Qi, S.; Tao, L.; Xu, H.; Kang, Y.; Yao, Y.; Yang, B.; Duan, Y.; Chen, H. Image Patch-Based Net Water Uptake and Radiomics Models Predict Malignant Cerebral Edema After Ischemic Stroke. Front. Neurol. 2020, 11, 609747.
- Jiang, L.; Zhang, C.; Wang, S.; Ai, Z.; Shen, T.; Zhang, H.; Duan, S.; Yin, X.; Chen, Y.-C. MRI Radiomics Features From Infarction and Cerebrospinal Fluid for Prediction of Cerebral Edema after Acute Ischemic Stroke. Front. Aging Neurosci. 2022, 14, 782036.
- Meng, Y.; Wang, H.; Wu, C.; Liu, X.; Qu, L.; Shi, Y. Prediction Model of Hemorrhage Transformation in Patient with Acute Ischemic Stroke Based on Multiparametric MRI Radiomics and Machine Learning. Brain Sci. 2022, 12, 858.
- Chen, Y.; He, Y.; Jiang, Z.; Xie, Y.; Nie, S. Ischemic stroke subtyping method combining convolutional neural network and radiomics. J. X-ray Sci. Technol. 2022, 31, 223–235.
- Cheng, Y.; Wan, S.; Wu, W.; Chen, F.; Jiang, J.; Cai, D.; Bao, Z.; Li, Y.; Zhang, L. Computed Tomography Angiography-Based Thrombus Radiomics for Predicting the Time Since Stroke Onset. Acad. Radiol. 2023, 36697269.
- Chen, X.; Li, Y.; Zhou, Y.; Yang, Y.; Yang, J.; Pang, P.; Wang, Y.; Cheng, J.; Chen, H.; Guo, Y. CT-based radiomics for differentiating intracranial contrast extravasation from intraparenchymal haemorrhage after mechanical thrombectomy. Eur. Radiol. 2022, 32, 4771–4779.

