Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Bogdan Amuzescu | -- | 2423 | 2023-09-13 10:41:33 | | | |
| 2 | Peter Tang | Meta information modification | 2423 | 2023-09-13 15:01:23 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Shaher, S.A.A.; Mihailescu, D.F.; Amuzescu, B. Aspartame Safety as a Food Sweetener. Encyclopedia. Available online: https://encyclopedia.pub/entry/49102 (accessed on 11 August 2026).
Shaher SAA, Mihailescu DF, Amuzescu B. Aspartame Safety as a Food Sweetener. Encyclopedia. Available at: https://encyclopedia.pub/entry/49102. Accessed August 11, 2026.
Shaher, Shurooq Asaad Abdulameer, Dan Florin Mihailescu, Bogdan Amuzescu. "Aspartame Safety as a Food Sweetener" Encyclopedia, https://encyclopedia.pub/entry/49102 (accessed August 11, 2026).
Shaher, S.A.A., Mihailescu, D.F., & Amuzescu, B. (2023, September 13). Aspartame Safety as a Food Sweetener. In Encyclopedia. https://encyclopedia.pub/entry/49102
Shaher, Shurooq Asaad Abdulameer, et al. "Aspartame Safety as a Food Sweetener." Encyclopedia. Web. 13 September, 2023.
Copy Citation
Aspartame is the methyl-ester of the aspartate-phenylalanine dipeptide. Over time, it has become a very popular artificial sweetener. However, since its approval by the main food safety agencies, several concerns have been raised related to neuropsychiatric effects and neurotoxicity due to its ability to activate glutamate receptors, as well as carcinogenic risks due to the increased production of reactive oxygen species.
aspartame
artificial sweetener
excitotoxicity
neuropsychiatric symptoms
reactive oxygen species
carcinogenic risk
1. Introduction
Due to decreased sugar production throughout the two world wars as well as an increased prevalence of nutrition disorders, particularly diabetes mellitus, in post-war industrialized societies, artificial sweeteners, also known as non-nutritive sweeteners, gained popularity [1]. Some non-nutritive, low-calorie sweeteners provide a similar taste while bringing 200–300 times fewer calories than sugar [2]. Saccharin, discovered and used since 1879, was widely regarded at the time as a sugar substitute. James Schlatter, while doing biochemical synthesis experiments with Robert Mazur, accidentally discovered aspartame in 1965, and his employer G.D. Searle immediately started testing the substance in the hope of producing and commercializing it on a wide scale [3][4] (Figure 1). Aspartame is the methyl ester of the dipeptide formed by L-aspartic acid and L-phenylalanine [5]. It has been found to be 188 times sweeter than sugar while having the same calorie contents per weight unit [6].
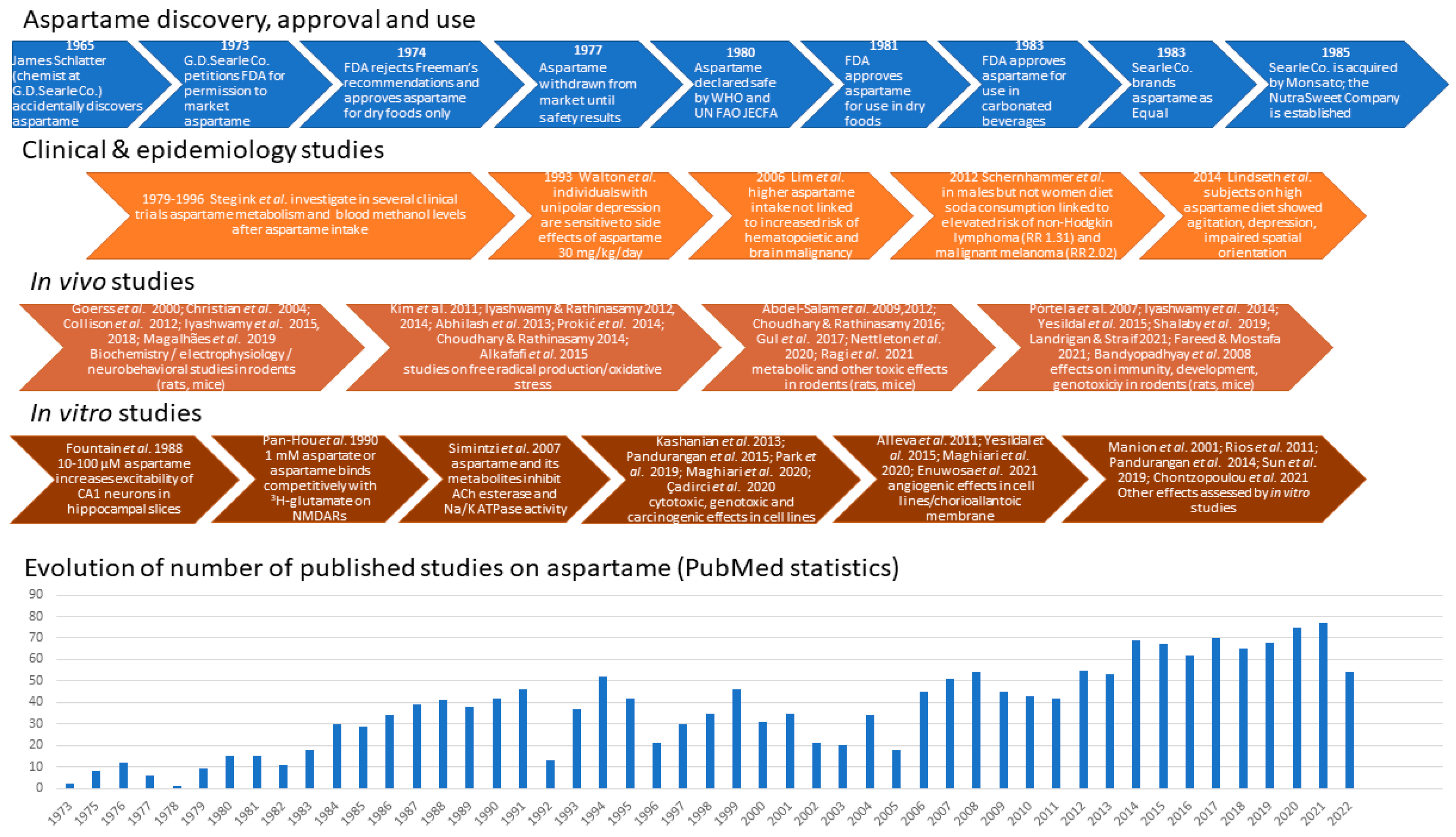
Figure 1. Main steps related to aspartame discovery, approval, development, and use, along with some of the clinical trials, in vivo and in vitro studies evidencing its biological effects, and the dynamics of publications describing them [7][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48][49][50][51][52][53][54][55][56][57][58][59].
In 1973, D. Searle requested from the Food and Drug Administration (FDA) an initial clearance for aspartame. The FDA stated that the maximum daily dosage of aspartame for humans should be 50 mg/kg body weight/day in the United States; in Europe, a maximal acceptable daily intake (ADI) of 40 mg/kg body weight/day was adopted [60]. However, some chronic exposure and carcinogenesis studies [61][62] found—even in female rats exposed to relatively low doses of aspartame (4 or 20 mg/kg body weight/day)—exposures that are close to the current ADI in the European Union (40 mg/kg body weight/day) bring an increased incidence of malignant tumors.
By 1983, the Equal® brand of aspartame sugar replacement ruled the tabletop non-nutritive sweetener industry. Aspartame appealed to diabetics because its dipeptide composition did not require insulin to be metabolized, and it featured a better sweet taste devoid of bitterness and presumably fewer side effects compared to earlier sugar substitutes, such as saccharin and cyclamate. Large soft drinks companies, such as Coca-Cola® and Royal Crown®, declared they would combine two artificial sweeteners, e.g., aspartame and acesulfame K, in their low-calorie diet soda products in order to minimize the side effects of each of them [1][7][63], a guideline followed so far. One year after full approval was obtained, in 1984, NutraSweet® quickly developed into a very lucrative division of G.D. Searle, and the number of customers grew less affected by safety concerns [64]. Thus, nowadays, aspartame is a common component in over 6000 food products and beverages.
Aspartame is present in soft drinks, dessert mixes, yogurt, chewable multivitamins, and morning cereals. Millions of people throughout the world ingest it because it is also present in 600 different types of medicines [65]. The production of low-calorie beverages, which are widely consumed by youngsters and pregnant people, is a crucial use in the United States [66][67]. Although some early studies estimated that the amount of methanol intake resulting from diet soda drinking in a hot environment could reach 250 mg/day or 32 times the Environmental Protection Agency’s daily limit suggestion [68], a more realistic estimate places the methanol intake resulting from daily aspartame consumption in the highest 90% as being 25 times lower than the maximal safe level of methanol intake of 7.1–8.4 mg/kg/day established by FDA, and much lower than the methanol intake resulting from other natural sources, such as pectin, fruits, vegetables, and alcoholic beverages [69]. A substantial body of the literature shows that young animals are more vulnerable than older animals to a variety of chemical and physical carcinogens, particularly during the prenatal period [70]. A re-examination of histopathology data from large groups of animals fed on aspartame-containing diets within studies performed at the Ramazzini Institute in Bologna confirmed that aspartame exposure during pregnancy raises the risk of cancer in rodent offspring [8]. Additional research into associations between aspartame and conditions, like brain tumors, brain lesions, and lymphoma, has also been advised by several researchers [61][71]. The Food Additives and Nutrient Sources Added to Food Panel evaluated the potential risks of aspartame for pregnant women by assessing the plasma concentrations of the breakdown product phenylalanine following the consumption of aspartame-containing products [60][72] (Figure 2).
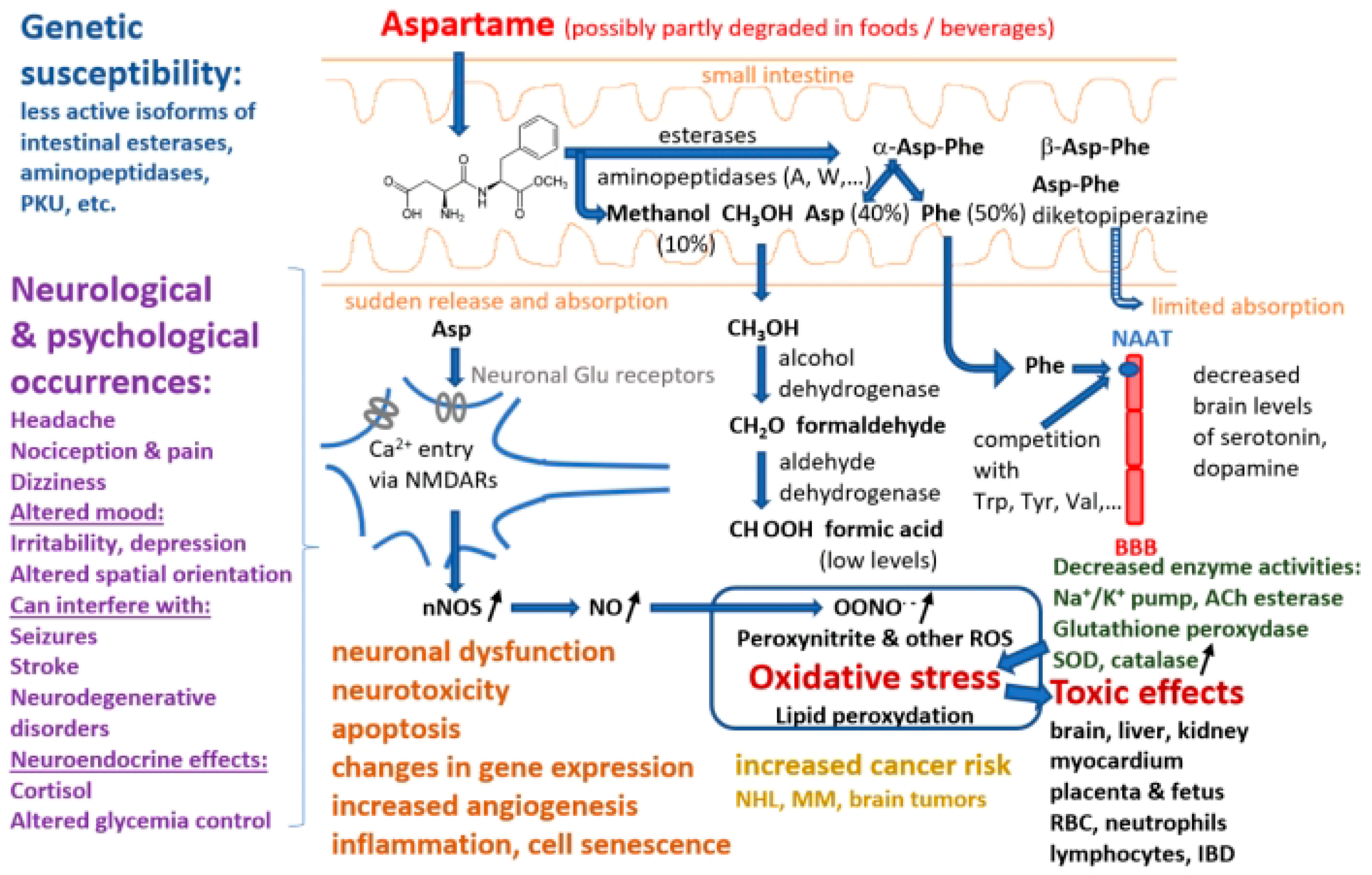
Figure 2. Summary of pathways involved in aspartame decomposition, kinetics, metabolism, potential adverse effects at cell level, side effects, and relationships with different disorders (abbreviations: PKU—phenylketonuria, NAAT—large neutral amino acids transporter, BBB—blood–brain barrier, NMDARs—N-methyl-D-aspartate receptors, nNOS—neuronal nitric oxide synthase, NO—nitric oxide, ROS—reactive oxygen species, ACh—acetylcholine, SOD—superoxide dismutase, RBC—red blood cell, IBD—inflammatory bowel diseases, NHL—non-Hodgkin lymphoma, MM—multiple myeloma).
2. Chemical Structure, Digestion, and Metabolism
Aspartame is the methyl ester of a dipeptide composed of a hydrophilic and a hydrophobic amino acid residue, aspartic acid (Asp) and phenylalanine (Phe), respectively, giving it some unique qualities [73][74]. Aspartame in purified solid form is a white crystalline powder that may be stored at temperatures between 30 and 80 °C and is extremely stable under dry conditions [75]. At room temperature, its aqueous solution has a half-life of approximately 300 days and reaches the highest stability at a pH of 4.3, which is common for diet sodas. The peptide bonds are hydrolyzed in certain conditions, such as high temperature or basic pH [1].
Aspartame stability in soft drinks has been studied intensively. Thus, it was found that after 50 weeks storage at room temperature of a diet soda, 20% of its aspartame content was de-esterified to α-Asp-Phe, 15% was converted to β-Asp-Phe and β-aspartame, and another 20% was converted into a cyclic dipeptide known as aspartame diketopiperazine (3-carboxyl-methyl-6 benzyl-2.5 diketo-piperazine) [75][76]. Aspartame produces methanol by hydrolysis in highly acidic or alkaline environments. The peptide bonds are also hydrolyzed in more extreme circumstances, releasing the free amino acids. Upon consumption, aspartame is split by several digestive enzymes, such as esterases and peptidases, into a number of chemical components, including aspartic acid, phenylalanine, and methanol, the latter being further decomposed into formaldehyde and formic acid [77]. Studies with human and pig intestinal microvilli preparations and specific inhibitors showed that aminopeptidases A and W are the most active in decomposing the α-Asp-Phe dipeptide [78]. Another pioneering study proved that Asp-Phe is hydrolyzed by three of four brush border peptidases and by a cytosolic peptidase different from the seven known isoforms [5]. Similarly, amino acids and dipeptide intestinal absorption studies [79] showed that, although dipeptide absorption mechanisms are present, particularly in the jejunum and ileum [80], α-aspartame is almost entirely decomposed in the intestinal lumen and passes into circulation as Asp (40%), Phe (50%), and methanol (10%) [69][76]. The rates of intestinal absorption of β-Asp-Phe and aspartame diketopiperazine are small [76]. The group of Lewis Stegink was particularly active and performed a number of clinical studies on adults, children, and infants, involving acute (single-dose or repeated doses over less than 1 day) or prolonged (e.g., daily for 13 consecutive weeks) intake of aspartame doses, sometimes higher than the ADI (up to 200 mg/kg body weight) to assess the pharmacokinetics and demonstrate the lack of toxicity of aspartame decomposition products [9][10][11][12][13][14][15][16][81], except for subjects with genetic traits resulting in low plasma α-Asp-Phe hydrolase activity [17]. However, other clinical studies reached different conclusions, showing adverse effects of aspartame, particularly in subjects with neurological or psychiatric conditions, such as migraines [82][83], other headaches [84][85], or unipolar depression [18]. Part of these differences may result from the fact that aspartame was administered in some studies, e.g., [18], as powder included in enteric-soluble capsules, which can release very high concentrations of aspartame over limited areas of the intestinal mucosa, in contrast to administration in a pre-dissolved form in water or beverages.
While phenylalanine is turned into tyrosine and phenylethylamine, and methanol is converted into formaldehyde, which then undergoes an oxidation reaction to formic acid, aspartic acid is converted to alanine and oxaloacetate [86]. Each of these compounds is metabolized according to a natural metabolic route in the same manner as those originating from foods and other dietary sources. As demonstrated in animals, methanol from aspartame enters the portal circulation and is promptly converted by alcohol dehydrogenase to formaldehyde, which is further transformed into formate by aldehyde dehydrogenase [65]. Early pharmacokinetics and metabolism studies in humans have shown that upon acute ingestion of 50 mg/kg aspartame, blood methanol levels increased to 0.34 ± 0.12 mg/dL (mean ± SEM, n = 6) in adults 30–90 min after intake, and to 0.30 ± 0.10 mg/dL in infants; higher aspartame doses produced proportionally higher peak blood methanol levels [9][10]. However, several researchers have pointed out that methanol levels resulting from aspartame intake are several times smaller than those produced by consumption of other common foods and drinks, like fruit or vegetable juices and fermented distilled beverages, due to enzyme-driven breakdown of methoxyl groups of polysaccharides, such as pectin [9][69]. Therefore, aspartame side effects are more likely due to the two amino acids released by its decomposition, phenylalanine, and aspartate. Thus, a clinical study on children fed with aspartame 34 mg/kg/day for two weeks proved increased phenyalanine and tyrosine plasma levels compared to a placebo group [87].
The increased phenylalanine concentrations are linked to lower levels of catecholamines, serotonin, and dopamine [88]. Phenylalanine is a large neutral amino acid that competes with other amino acids for binding on the large neutral amino acid transporter [89]. Phenylalanine released from aspartame may theoretically mediate neurologic effects since it has neurotoxic potential and influences the production of monoamine neurotransmitters. When pentylenetetrazole, an epileptogenic drug, is administered to mice after aspartame administration, the frequency of seizures that follow is increased [90]. This is because aspartame causes plasma phenylalanine levels to rise more than those of tyrosine (which likely happens after any aspartame dose in humans). Phenylalanine prevents dopamine release in the striatum, whereas valine, which competes with phenylalanine for passage across the blood–brain barrier, can alleviate its proepileptogenic effect [91]. The reduced levels of dopamine and serotonin are a result of the excess phenylalanine blocking the transport of crucial amino acids to the brain. In addition to being employed in protein synthesis, phenylalanine can also be converted into the highly concentrated phenylpyruvic acid in phenylketonuria patients [19][92]. By competing for neutral amino acid transporters, phenylalanine can directly affect the entry of other critical amino acids into the CNS. As a result, it indirectly influences neurotransmitter deficiencies that result in functional problems [93].
On the other hand, aspartate, the carboxylate anion of aspartic acid, undergoes transamination in enterocytes to become oxaloacetate before reaching the portal circulation [69]. The urea cycle and gluconeogenesis can be affected by the body’s conversion of oxaloacetate and aspartate [2]. Aspartate and other related amino acids, such as asparagine, glutamate, and glutamine, did not significantly change their plasma levels in healthy people after taking aspartame doses of 34–50 mg/kg [14]. Aspartic acid residues are frequently found in proteins. The body may convert aspartic acid into the neurotransmitter glutamate, which at very high levels, can have harmful effects on the nervous system. In addition, high doses of aspartate can directly activate N-methyl-D-aspartate (NMDA) receptors, exerting excitotoxicity and other central nervous system adverse effects. However, the European Food Safety Authority’s experts did not see any evidence of neurotoxicity associated with aspartame and therefore concluded that aspartic acid derived from aspartame does not raise any safety concerns for consumers [60].
3. Mechanisms of Toxicity of Aspartame Metabolism Products
The fundamental tenet of toxicology is that all substances are harmful at some concentration. As a result, it is not surprising that aspartame or its components have negative effects on sensitive animal species when consumed at very high doses. Upon testing the effects of various aspartame doses on blood levels of aspartate, phenylalanine, and methanol, several studies proved that these levels were well below those associated with adverse effects in animal species, raising the important question of whether aspartame ingestion is potentially harmful to humans during normal use or abuse, in spite of the fact that the dietary exposure of consumers to these compounds is higher than that resulting from aspartame intake [12]. Although FDA and other regulatory agencies have established permissible daily intake guidelines for aspartame ingestion, there are many questions about its safety today.
Frequent high-dose aspartame intake may have nephrotoxic effects. Thus, according to experimental data from different animal species, long-term consumption of aspartame caused a dose-dependent increased production of free radicals in renal tissues as well as kidney injury, as proved by a search of several literature databases for publications on the adverse effects of aspartame on the kidney function from 1980 to 2016 [94]. Additionally, recent cohort studies showed a link between excessive aspartame use and an elevated risk for cardiovascular disorders [95]. The administration of aspartame caused oxidative stress and markedly reduced the activity of antioxidant enzymes, such as superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase in both rat liver and renal tissues [96]. Increased pro-oxidant levels, such as reactive oxygen and nitrogen species (ROS/RNS), or decreased antioxidant levels, which could cause cell malfunction and disintegration, are indicators of oxidative stress [97].
4. Neurological and Cytotoxic Effects by Activation of NMDA and Other Glutamate Receptors by Aspartame or Its Metabolites
Glutamate represents the main excitatory neurotransmitter in the central nervous system. Glutamate receptors are divided into the following two groups: metabotropic glutamate receptors (mGluRs), with seven transmembrane α-helical segments accommodating the ligand molecule at the center, similar to rhodopsin, and ionotropic glutamate receptors (iGluRs), tetrameric ligand-gated ion channels with large extracellular domains featuring multiple ligand-binding sites and four transmembrane α-helical segments per subunit. The three types of ionotropic glutamate receptors—NMDA, AMPA, and kainate receptors—are distinguished by varying ion selectivity, activating agents, and pharmacological agonists and inhibitors [98]. The N-methyl-D-aspartate receptors (NMDAR) are crucial molecular components of learning and memory via the complex phenomenon of long-term potentiation (LTP), which involves receptor phosphorylation triggered by calcium influx upon repeated stimulation [99]. However, several pathological conditions, such as ischemic stroke or neurodegenerative diseases, may lead to excitotoxicity, consisting of excessive synaptic glutamate release and NMDAR overactivation with massive Ca2+ inflow, resulting in neuronal cell death [100]. The same author pointed out that the developing human brain is exposed to excitotoxic compounds, such as those present in foods, to a much larger extent compared to the adult brain due to an immature blood–brain barrier [101]. Therefore, it seemed logical to express similar concerns over the use of aspartame since the compound itself and its decomposition product aspartate may effectively activate NMDARs [102], in addition to neurotransmitter imbalances caused by aspartate and phenylalanine [88][91].
References
- Chattopadhyay, S.; Raychaudhuri, U.; Chakraborty, R. Artificial sweeteners—A review. J. Food Sci. Technol. 2014, 51, 611–621.
- Marinovich, M.; Galli, C.L.; Bosetti, C.; Gallus, S.; La Vecchia, C. Aspartame, low-calorie sweeteners and disease: Regulatory safety and epidemiological issues. Food Chem. Toxicol. 2013, 60, 109–115.
- Mazur, R.H. Discovery of aspartame. In Aspartame: Physiology and Biochemistry; Stegink, L.D., Filer, L.J.J., Eds.; Marcel Dekker: New York, NY, USA, 1984; pp. 3–9.
- Mazur, R.H.; Schlatter, J.M.; Goldkamp, A.H. Structure-taste relationships of some dipeptides. J. Am. Chem. Soc. 1969, 91, 2684–2691.
- Tobey, N.A.; Heizer, W.D. Intestinal hydrolysis of aspartylphenylalanine—The metabolic product of aspartame. Gastroenterology 1986, 91, 931–937.
- Barceloux, D.G.; Bond, G.R.; Krenzelok, E.P.; Cooper, H.; Vale, J.A. American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J. Toxicol. Clin. Toxicol. 2002, 40, 415–446.
- Ragi, M.E.; El-Haber, R.; El-Masri, F.; Obeid, O.A. The effect of aspartame and sucralose intake on body weight measures and blood metabolites: Role of their form (solid and/or liquid) of ingestion. Br. J. Nutr. 2021, 128, 352–360.
- Landrigan, P.J.; Straif, K. Aspartame and cancer—New evidence for causation. Environ. Health 2021, 20, 42.
- Stegink, L.D.; Brummel, M.C.; Filer, L.J., Jr.; Baker, G.L. Blood methanol concentrations in one-year-old infants administered graded doses of aspartame. J. Nutr. 1983, 113, 1600–1606.
- Stegink, L.D.; Brummel, M.C.; McMartin, K.; Martin-Amat, G.; Filer, L.J., Jr.; Baker, G.L.; Tephly, T.R. Blood methanol concentrations in normal adult subjects administered abuse doses of aspartame. J. Toxicol. Environ. Health 1981, 7, 281–290.
- Stegink, L.D.; Filer, L., Jr. Effects of Aspartame Ingestion on Plasma Aspartate, Phenylalanine and Methanol Concentrations in Potentially Sensitive Populations. In The Clinical Evaluation of a Food Additive: Assessment of Aspartame; Tschanz, C., Butchko, H.H., Stargel, W., Kotsonis, F.N., Eds.; CRC Press: Boca Raton, FL, USA, 1996; pp. 87–113.
- Stegink, L.D.; Filer, L.J., Jr.; Baker, G.L. Plasma amino acid concentrations in normal adults ingesting aspartame and monosodium L-glutamate as part of a soup/beverage meal. Metabolism 1987, 36, 1073–1079.
- Stegink, L.D.; Filer, L.J., Jr.; Baker, G.L. Repeated ingestion of aspartame-sweetened beverage: Effect on plasma amino acid concentrations in normal adults. Metabolism 1988, 37, 246–251.
- Stegink, L.D.; Filer, L.J., Jr.; Baker, G.L.; Brummel, M.C. Plasma and erythrocyte amino acid levels of adult humans given 100 mg/kg body weight aspartame. Toxicology 1979, 14, 131–140.
- Stegink, L.D.; Filer, L.J., Jr.; Baker, G.L.; McDonnell, J.E. Effect of an abuse dose of aspartame upon plasma and erythrocyte levels of amino acids in phenylketonuric heterozygous and normal adults. J. Nutr. 1980, 110, 2216–2224.
- Stegink, L.D.; Filer, L.J., Jr.; Bell, E.F.; Ziegler, E.E.; Tephly, T.R. Effect of repeated ingestion of aspartame-sweetened beverage on plasma amino acid, blood methanol, and blood formate concentrations in normal adults. Metabolism 1989, 38, 357–363.
- Stegink, L.D.; Lindgren, S.D.; Brummel, M.C.; Stumbo, P.J.; Wolraich, M.L. Erythrocyte L-aspartyl-L-phenylalanine hydrolase activity and plasma phenylalanine and aspartate concentrations in children consuming diets high in aspartame. Am. J. Clin. Nutr. 1995, 62, 1206–1211.
- Walton, R.G.; Hudak, R.; Green-Waite, R.J. Adverse reactions to aspartame: Double-blind challenge in patients from a vulnerable population. Biol. Psychiatry 1993, 34, 13–17.
- Iyaswamy, A.; Kammella, A.K.; Thavasimuthu, C.; Wankupar, W.; Dapkupar, W.; Shanmugam, S.; Rajan, R.; Rathinasamy, S. Oxidative stress evoked damages leading to attenuated memory and inhibition of NMDAR-CaMKII-ERK/CREB signalling on consumption of aspartame in rat model. J. Food Drug Anal. 2018, 26, 903–916.
- Prokić, M.D.; Paunović, M.G.; Matić, M.M.; Djordjević, N.Z.; Ognjanović, B.I.; Štajn, A.S.; Saičić, Z.S. Prooxidative effects of aspartame on antioxidant defense status in erythrocytes of rats. J. Biosci. 2014, 39, 859–866.
- Schernhammer, E.S.; Bertrand, K.A.; Birmann, B.M.; Sampson, L.; Willett, W.C.; Feskanich, D. Consumption of artificial sweetener- and sugar-containing soda and risk of lymphoma and leukemia in men and women. Am. J. Clin. Nutr. 2012, 96, 1419–1428.
- Maghiari, A.L.; Coricovac, D.; Pinzaru, I.A.; Macașoi, I.G.; Marcovici, I.; Simu, S.; Navolan, D.; Dehelean, C. High Concentrations of Aspartame Induce Pro-Angiogenic Effects in Ovo and Cytotoxic Effects in HT-29 Human Colorectal Carcinoma Cells. Nutrients 2020, 12, 3600.
- Alleva, R.; Borghi, B.; Santarelli, L.; Strafella, E.; Carbonari, D.; Bracci, M.; Tomasetti, M. In vitro effect of aspartame in angiogenesis induction. Toxicol. Vitr. 2011, 25, 286–293.
- Enuwosa, E.; Gautam, L.; King, L.; Chichger, H. Saccharin and sucralose protect the glomerular microvasculature in vitro against VEGF-induced permeability. Nutrients 2021, 13, 2746.
- Yesildal, F.; Aydin, F.N.; Deveci, S.; Tekin, S.; Aydin, I.; Mammadov, R.; Fermanli, O.; Avcu, F.; Acikel, C.H.; Ozgurtas, T. Aspartame induces angiogenesis in vitro and in vivo models. Hum. Exp. Toxicol. 2015, 34, 260–265.
- Choudhary, A.K.; Rathinasamy, S. Effect of aspartame in spinal cord and motor behavior in Wistar albino rats. J. Behav. Health 2014, 3, 107–111.
- Pandurangan, M.; Enkhtaivan, G.; Mistry, B.; Chandrasekaran, M.; Noorzai, R.; Kim, D.H. Investigation of role of aspartame on apoptosis process in HeLa cells -->. Saudi J. Biol. Sci. 2016, 23, 503–506.
- Pórtela, G.S.; Azoubel, R.; Batigália, F. Effects of aspartame on maternal-fetal and placental weights, length of umbilical cord and fetal liver: A kariometric experimental study. Int. J. Morphol. 2007, 25, 549–554.
- Shalaby, A.M.; Ibrahim, M.; Aboregela, A.M. Effect of aspartame on the placenta of adult albino rat. A histological and immunohistochemical study. Ann. Anat. 2019, 224, 133–141.
- Pan-Hou, H.; Suda, Y.; Ohe, Y.; Sumi, M.; Yoshioka, M. Effect of aspartame on N-methyl-D-aspartate-sensitive L- glutamate binding sites in rat brain synaptic membranes. Brain Res. 1990, 520, 351–353.
- Abdel-Salam, O.M.; Salem, N.A.; Hussein, J.S. Effect of aspartame on oxidative stress and monoamine neurotransmitter levels in lipopolysaccharide-treated mice. Neurotox. Res. 2012, 21, 245–255.
- Abhilash, M.; Sauganth Paul, M.; Varghese, M.V.; Nair, R.H. Long-term consumption of aspartame and brain antioxidant defense status. Drug Chem. Toxicol. 2013, 36, 135–140.
- Alkafafy, M.E.-S.; Ibrahim, Z.S.; Ahmed, M.M.; El-Shazly, S.A. Impact of aspartame and saccharin on the rat liver: Biochemical, molecular, and histological approach. Int. J. Immunopathol. Pharmacol. 2015, 28, 247–255.
- Iyaswamy, A.; Rathinasamy, S. Effect of chronic exposure to aspartame on oxidative stress in the brain of albino rats. J. Biosci. 2012, 37, 679–688.
- Iyaswamy, A.; Rathinasamy, S. Biochemical responses and mitochondrial mediated activation of apoptosis on long-term effect of aspartame in rat brain. Redox Biol. 2014, 2, 820–831.
- Christian, B.; McConnaughey, K.; Bethea, E.; Brantley, S.; Coffey, A.; Hammond, L.; Harrell, S.; Metcalf, K.; Muehlenbein, D.; Spruill, W. Chronic aspartame affects T-maze performance, brain cholinergic receptors and Na+, K+-ATPase in rats. Pharmacol. Biochem. Behav. 2004, 78, 121–127.
- Simintzi, I.; Schulpis, K.H.; Angelogianni, P.; Liapi, C.; Tsakiris, S. L-Cysteine and glutathione restore the reduction of rat hippocampal Na+, K+-ATPase activity induced by aspartame metabolites. Toxicology 2007, 237, 177–183.
- Iyaswamy, A.; Rathinasamy, S. Neurobehavioral changes and activation of neurodegenerative apoptosis on long-term consumption of aspartame in the rat brain. J. Nutr. Intermed. Metabol. 2015, 2, 76–85.
- Collison, K.S.; Makhoul, N.J.; Zaidi, M.Z.; Saleh, S.M.; Andres, B.; Inglis, A.; Al-Rabiah, R.; Al-Mohanna, F.A. Gender dimorphism in aspartame-induced impairment of spatial cognition and insulin sensitivity. PLoS ONE 2012, 7, e31570.
- Magalhães, P.C.G.; Abadie-Guedes, R.; da Costa Mendonça, M.A.B.; de Souza, A.D.; Guedes, R.C.A. Behavioral and electrophysiological brain effects of aspartame on well-nourished and malnourished rats. Metab. Brain Dis. 2019, 34, 651–658.
- Goerss, A.L.; Wagner, G.C.; Hill, W.L. Acute effects of aspartame on aggression and neurochemistry of rats. Life Sci. 2000, 67, 1325–1329.
- Lindseth, G.N.; Coolahan, S.E.; Petros, T.V.; Lindseth, P.D. Neurobehavioral effects of aspartame consumption. Res. Nurs. Health 2014, 37, 185–193.
- Lim, U.; Subar, A.F.; Mouw, T.; Hartge, P.; Morton, L.M.; Stolzenberg-Solomon, R.; Campbell, D.; Hollenbeck, A.R.; Schatzkin, A. Consumption of aspartame-containing beverages and incidence of hematopoietic and brain malignancies. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1654–1659.
- Abdel Salam, O.M.; Shaffie, N.M.; Sleem, A.A. Hepatoprotective effects of citric acid and aspartame on carbon tetrachloride-induced hepatic damage in rats. EXCLI J. 2009, 8, 41–49.
- Kim, J.Y.; Seo, J.; Cho, K.H. Aspartame-fed zebrafish exhibit acute deaths with swimming defects and saccharin-fed zebrafish have elevation of cholesteryl ester transfer protein activity in hypercholesterolemia. Food Chem. Toxicol. 2011, 49, 2899–2905.
- Choudhary, A.K.; Rathinasamy, S. Effects of aspartame on hsp70, bcl-2 and bax expression in immune organs of Wistar albino rats. J. Biomed. Res. 2016, 30, 427–435.
- Gul, S.S.; Hamilton, A.R.; Munoz, A.R.; Phupitakphol, T.; Liu, W.; Hyoju, S.K.; Economopoulos, K.P.; Morrison, S.; Hu, D.; Zhang, W.; et al. Inhibition of the gut enzyme intestinal alkaline phosphatase may explain how aspartame promotes glucose intolerance and obesity in mice. Appl. Physiol. Nutr. Metab. 2017, 42, 77–83.
- Nettleton, J.E.; Cho, N.A.; Klancic, T.; Nicolucci, A.C.; Shearer, J.; Borgland, S.L.; Johnston, L.A.; Ramay, H.R.; Noye Tuplin, E.; Chleilat, F.; et al. Maternal low-dose aspartame and stevia consumption with an obesogenic diet alters metabolism, gut microbiota and mesolimbic reward system in rat dams and their offspring. Gut 2020, 69, 1807–1817.
- Fareed, S.A.; Mostafa, H.E. Could aspartame exacerbate caffeine effects on renal maturation in rat’s offspring? A biochemical and histological study. Birth Defects Res. 2021, 113, 90–107.
- Bandyopadhyay, A.; Ghoshal, S.; Mukherjee, A. Genotoxicity testing of low-calorie sweeteners: Aspartame, acesulfame-K, and saccharin. Drug Chem. Toxicol. 2008, 31, 447–457.
- Fountain, S.B.; Hennes, S.K.; Teyler, T.J. Aspartame exposure and in vitro hippocampal slice excitability and plasticity. Fundam. Appl. Toxicol. 1988, 11, 221–228.
- Simintzi, I.; Schulpis, K.H.; Angelogianni, P.; Liapi, C.; Tsakiris, S. The effect of aspartame on acetylcholinesterase activity in hippocampal homogenates of suckling rats. Pharmacol. Res. 2007, 56, 155–159.
- Kashanian, S.; Khodaei, M.M.; Kheirdoosh, F. In vitro DNA binding studies of Aspartame, an artificial sweetener. J. Photochem. Photobiol. B 2013, 120, 104–110.
- Çadirci, K.; Tozlu, Ö.Ö.; Türkez, H.; Mardinoğlu, A. The in vitro cytotoxic, genotoxic, and oxidative damage potentials of the oral artificialsweetener aspartame on cultured human blood cells. Turk. J. Med. Sci. 2020, 50, 448–454.
- Manion, C.V.; Howard, J.; Ogle, B.; Parkhurst, J.; Edmundson, A. Aspartame effect in sickle cell anemia. Clin. Pharmacol. Ther. 2001, 69, 346–355.
- Rios, D.; Ionta, F.Q.; Rebelato, R.; Jordão, M.C.; Wang, L.; Magalhães, A.C.; Honório, H.M. The effect of aspartame and pH changes on the erosive potential of cola drinks in bovine enamel: An in vitro study. J. Clin. Exp. Dent. 2018, 10, e933–e937.
- Pandurangan, M.; Park, J.; Kim, E. Aspartame downregulates 3T3-L1 differentiation. Vitr. Cell. Dev. Biol. Anim. 2014, 50, 851–857.
- Sun, D.; Liu, L.; Mao, S.; Zhu, W.; Liu, J. Aspartame supplementation in starter accelerates small intestinal epithelial cell cycle and stimulates secretion of glucagon-like peptide-2 in pre-weaned lambs. J. Anim. Physiol. Anim. Nutr. 2019, 103, 1338–1350.
- Chontzopoulou, E.; Papaemmanouil, C.D.; Chatziathanasiadou, M.V.; Kolokouris, D.; Kiriakidi, S.; Konstantinidi, A.; Gerogianni, I.; Tselios, T.; Kostakis, I.K.; Chrysina, E.D.; et al. Molecular investigation of artificial and natural sweeteners as potential anti-inflammatory agents. J. Biomol. Struct. Dyn. 2022, 40, 12608–12620.
- EFSA Panel on Food Additives Nutrient Sources added to Food. Scientific Opinion on the re-evaluation of aspartame (E 951) as a food additive. EFSA J. 2013, 12, 3696.
- Soffritti, M.; Belpoggi, F.; Degli Esposti, D.; Lambertini, L.; Tibaldi, E.; Rigano, A. First experimental demonstration of the multipotential carcinogenic effects of aspartame administered in the feed to Sprague-Dawley rats. Environ. Health Perspect. 2006, 114, 379–385.
- Soffritti, M.; Belpoggi, F.; Tibaldi, E.; Esposti, D.D.; Lauriola, M. Life-span exposure to low doses of aspartame beginning during prenatal life increases cancer effects in rats. Environ. Health Perspect. 2007, 115, 1293–1297.
- Collison, K.S.; Inglis, A.; Shibin, S.; Andres, B.; Ubungen, R.; Thiam, J.; Mata, P.; Al-Mohanna, F.A. Differential effects of early-life NMDA receptor antagonism on aspartame-impaired insulin tolerance and behavior. Physiol. Behav. 2016, 167, 209–221.
- Sykes, M. The Aspartame Controversy of 1981, The Hidden Truth Behind the Not-So-Sweet Artificial Sweetner. Va. Tech Undergrad. Hist. Rev. 2015, 4.
- Butchko, H.; Stargel, W.; Comer, C.; Mayhew, D.; Benninger, C.; Blackburn, G.; De Sonneville, L.; Geha, R.; Hertelendy, Z.; Kostner, A. Intake of aspartame vs the acceptable daily intake. Regul. Toxicol. Pharmacol. 2002, 35, S13–S16.
- Fatibello-Filho, O.; Marcolino-Junior, L.H.; Pereira, A.V. Solid-phase reactor with copper (II) phosphate for flow-injection spectrophotometric determination of aspartame in tabletop sweeteners. Anal. Chim. Acta 1999, 384, 167–174.
- Fitch, C.; Keim, K. Position of the academy of nutrition and dietetics: Use of nutritive and nonnutritive sweetener. J. Acad. Nutr. Diet. 2012, 112, 739–758.
- Monte, W.C. Aspartame: Methanol and the public health. J. Appl. Nutr. 1984, 36, 42–53.
- Magnuson, B.A.; Burdock, G.A.; Doull, J.; Kroes, R.M.; Marsh, G.M.; Pariza, M.W.; Spencer, P.S.; Waddell, W.J.; Walker, R.; Williams, G.M. Aspartame: A safety evaluation based on current use levels, regulations, and toxicological and epidemiological studies. Crit. Rev. Toxicol. 2007, 37, 629–727.
- National Research Council. Pesticides in the Diets of Infants and Children; The National Academies Press: Washington, DC, USA, 1993.
- Olney, J.W.; Farber, N.B.; Spitznagel, E.; Robins, L.N. Increasing brain tumor rates: Is there a link to aspartame? J. Neuropathol. Exp. Neurol. 1996, 55, 1115–1123.
- Czarnecka, K.; Pilarz, A.; Rogut, A.; Maj, P.; Szymańska, J.; Olejnik, Ł.; Szymański, P. Aspartame-True or False? Narrative Review of Safety Analysis of General Use in Products. Nutrients 2021, 13, 1957.
- Amchra, F.Z.; Al Faiz, C.; Chaouqi, S.; Khiraoui, A.; Benhmimou, A.; Guedira, T. Effect of Stevia rebaudiana, sucrose and aspartame on human health: A comprehensive review. J. Med. Plants Stud. 2018, 6, 102–108.
- Singh, M.; Kumar, A.; Tarannum, N. Water-compatible ‘aspartame’-imprinted polymer grafted on silica surface for selective recognition in aqueous solution. Anal. Bioanal. Chem. 2013, 405, 4245–4252.
- Bell, L.N.; Labuza, T.P. Aspartame degradation kinetics as affected by pH in intermediate and low moisture food systems. J. Food Sci. 1991, 56, 17–20.
- Lipton, W.E.; Li, Y.N.; Younoszai, M.K.; Stegink, L.D. Intestinal absorption of aspartame decomposition products in adult rats. Metabolism 1991, 40, 1337–1345.
- Magnuson, B.A.; Carakostas, M.C.; Moore, N.H.; Poulos, S.P.; Renwick, A.G. Biological fate of low-calorie sweeteners. Nutr. Rev. 2016, 74, 670–689.
- Hooper, N.M.; Hesp, R.J.; Tieku, S. Metabolism of aspartame by human and pig intestinal microvillar peptidases. Biochem. J. 1994, 298, 635–639.
- Li, D.; Zhao, X.H.; Yang, T.B.; Johnson, E.W.; Thacker, P.A. A comparison of the intestinal absorption of amino acids in piglets when provided in free form or as a dipeptide. Asian-Australas. J. Anim. Sci. 1999, 12, 939–943.
- Adibi, S.A. Intestinal transport of dipeptides in man: Relative importance of hydrolysis and intact absorption. J. Clin. Investig. 1971, 50, 2266–2275.
- Stegink, L.D. The aspartame story: A model for the clinical testing of a food additive. Am. J. Clin. Nutr. 1987, 46, 204–215.
- Koehler, S.M.; Glaros, A. The effect of aspartame on migraine headache. Headache 1988, 28, 10–14.
- Newman, L.C.; Lipton, R.B. Migraine MLT-down: An unusual presentation of migraine in patients with aspartame-triggered headaches. Headache 2001, 41, 899–901.
- Schiffman, S.S.; Buckley, C.E., 3rd; Sampson, H.A.; Massey, E.W.; Baraniuk, J.N.; Follett, J.V.; Warwick, Z.S. Aspartame and susceptibility to headache. N. Engl. J. Med. 1987, 317, 1181–1185.
- Van den Eeden, S.K.; Koepsell, T.D.; Longstreth, W.T., Jr.; van Belle, G.; Daling, J.R.; McKnight, B. Aspartame ingestion and headaches: A randomized crossover trial. Neurology 1994, 44, 1787–1793.
- Ranney, R.E.; Oppermann, J.A. A review of the metabolism of the aspartyl moiety of aspartame in experimental animals and man. J. Environ. Pathol. Toxicol. 1979, 2, 979–985.
- Shaywitz, B.A.; Sullivan, C.M.; Anderson, G.M.; Gillespie, S.M.; Sullivan, B.; Shaywitz, S.E. Aspartame, behavior, and cognitive function in children with attention deficit disorder. Pediatrics 1994, 93, 70–75.
- Choudhary, A.K.; Lee, Y.Y. The debate over neurotransmitter interaction in aspartame usage. J. Clin. Neurosci. 2018, 56, 7–15.
- Humphries, P.; Pretorius, E.; Naudé, H. Direct and indirect cellular effects of aspartame on the brain. Eur. J. Clin. Nutr. 2008, 62, 451–462.
- Reinhard, J.F.; Reinhard, J.F.J. Experimental evaluation of anticonvulsants. In Anticonvulsants; Vida, J.A., Ed.; Academic Press: New York, NY, USA, 1972; pp. 58–110.
- Maher, T.J.; Wurtman, R.J. Possible neurologic effects of aspartame, a widely used food additive. Environ. Health Perspect. 1987, 75, 53–57.
- Nelson, D.L.; Cox, M.M. Lehninger Principles of Biochemistry, 5th ed.; WH Freeman & Co.: New York, NY, USA, 2008.
- Rycerz, K.; Jaworska-Adamu, J.E. Effects of aspartame metabolites on astrocytes and neurons. Folia Neuropathol. 2013, 51, 10–17.
- Ardalan, M.R.; Tabibi, H.; Attari, V.E.; Mahdavi, A.M. Nephrotoxic effect of aspartame as an artificial sweetener: A brief review. Iran. J. Kidney Dis. 2017, 11, 339.
- Debras, C.; Chazelas, E.; Sellem, L.; Porcher, R.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, S.F.; Agaësse, C.; De Sa, A.; Lutchia, R.; et al. Artificial sweeteners and risk of cardiovascular diseases: Results from the prospective NutriNet-Santé cohort. BMJ 2022, 378, e071204.
- Alwaleedi, S.A. Alterations in antioxidant defense system in hepatic and renal tissues of rats following aspartame intake. J. Appl. Biol. Biotechnol. 2016, 4, 046–052.
- Halliwell, B.; Gutteridge, J.M.C. Free Radicals in Biology and Medicine, 5th ed.; Oxford University Press: New York, NY, USA, 2015; p. 896.
- Reiner, A.; Levitz, J. Glutamatergic Signaling in the Central Nervous System: Ionotropic and Metabotropic Receptors in Concert. Neuron 2018, 98, 1080–1098.
- Polizzi, S.; Pira, E.; Ferrara, M.; Bugiani, M.; Papaleo, A.; Albera, R.; Palmi, S. Neurotoxic effects of aluminium among foundry workers and Alzheimer’s disease. Neurotoxicology 2002, 23, 761–774.
- Olney, J.W. Brain lesions, obesity, and other disturbances in mice treated with monosodium glutamate. Science 1969, 164, 719–721.
- Olney, J.W. Excitotoxic food additives—Relevance of animal studies to human safety. Neurobehav. Toxicol. Teratol. 1984, 6, 455–462.
- Choudhary, A.K.; Lee, Y.Y. Neurophysiological symptoms and aspartame: What is the connection? Nutr. Neurosci. 2017, 21, 306–316.
More
Information
Subjects:
Food Science & Technology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.6K
Revisions:
2 times
(View History)
Update Date:
13 Sep 2023
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No