 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Narmeen Jamal AL-Awwad | -- | 3160 | 2023-07-15 17:22:55 | | | |
| 2 | Jessie Wu | -2 word(s) | 3158 | 2023-07-17 05:33:55 | | |
Video Upload Options
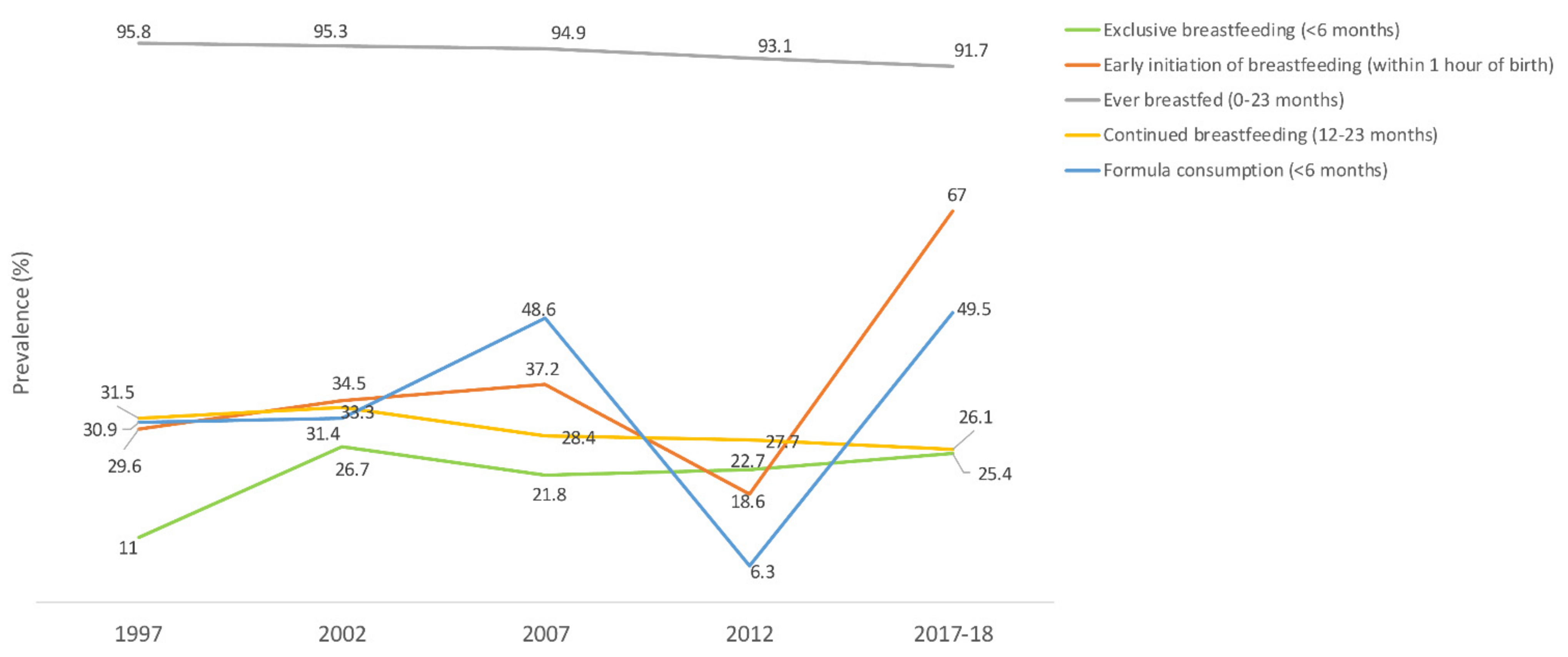
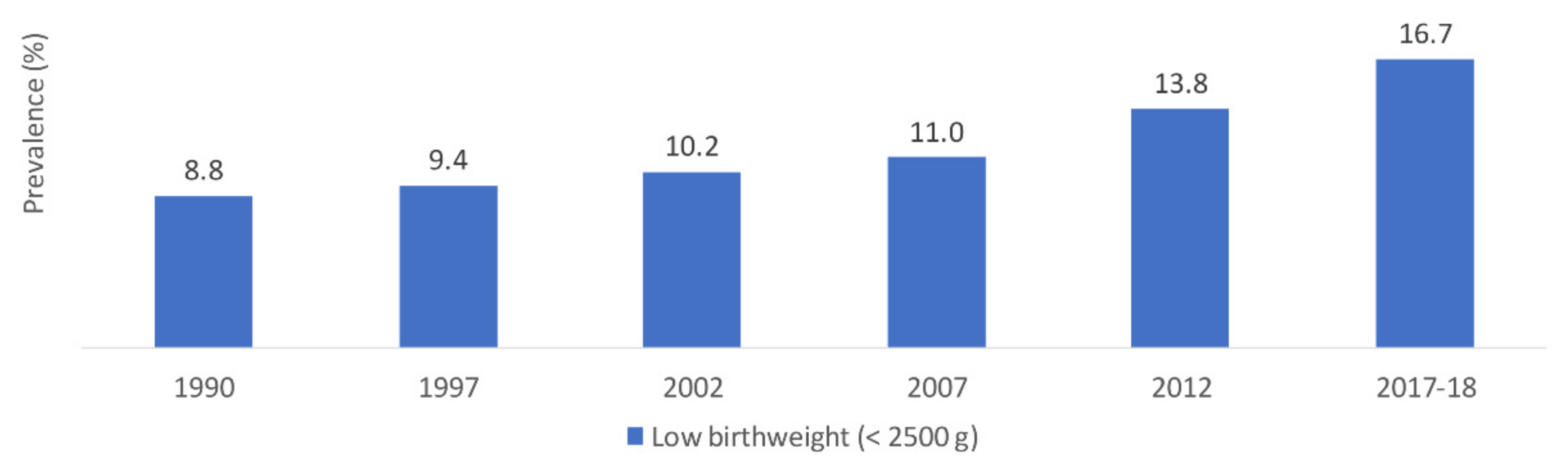
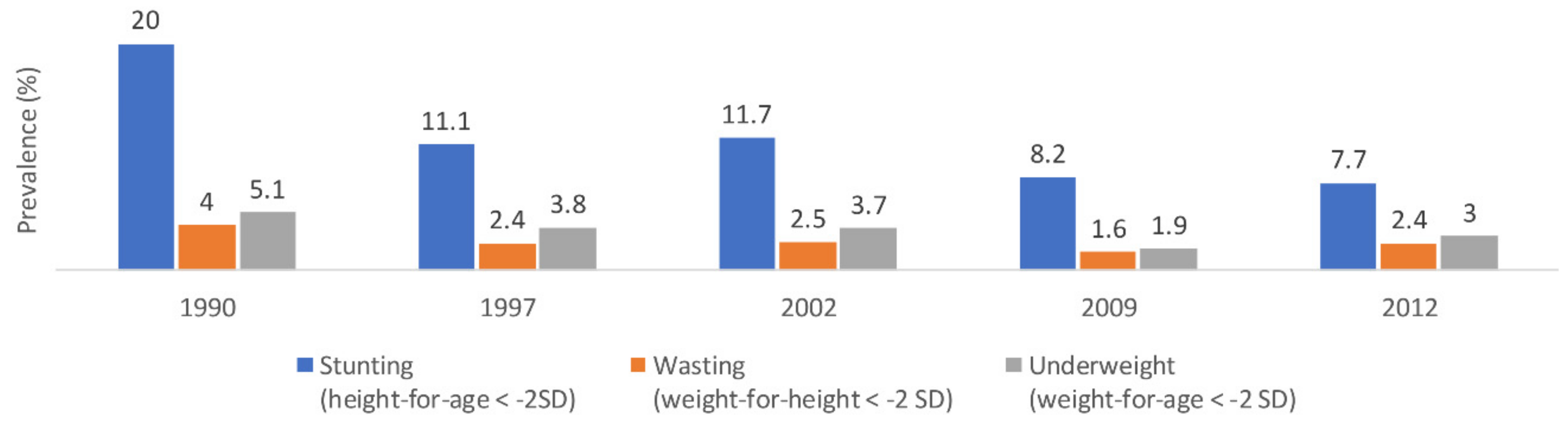
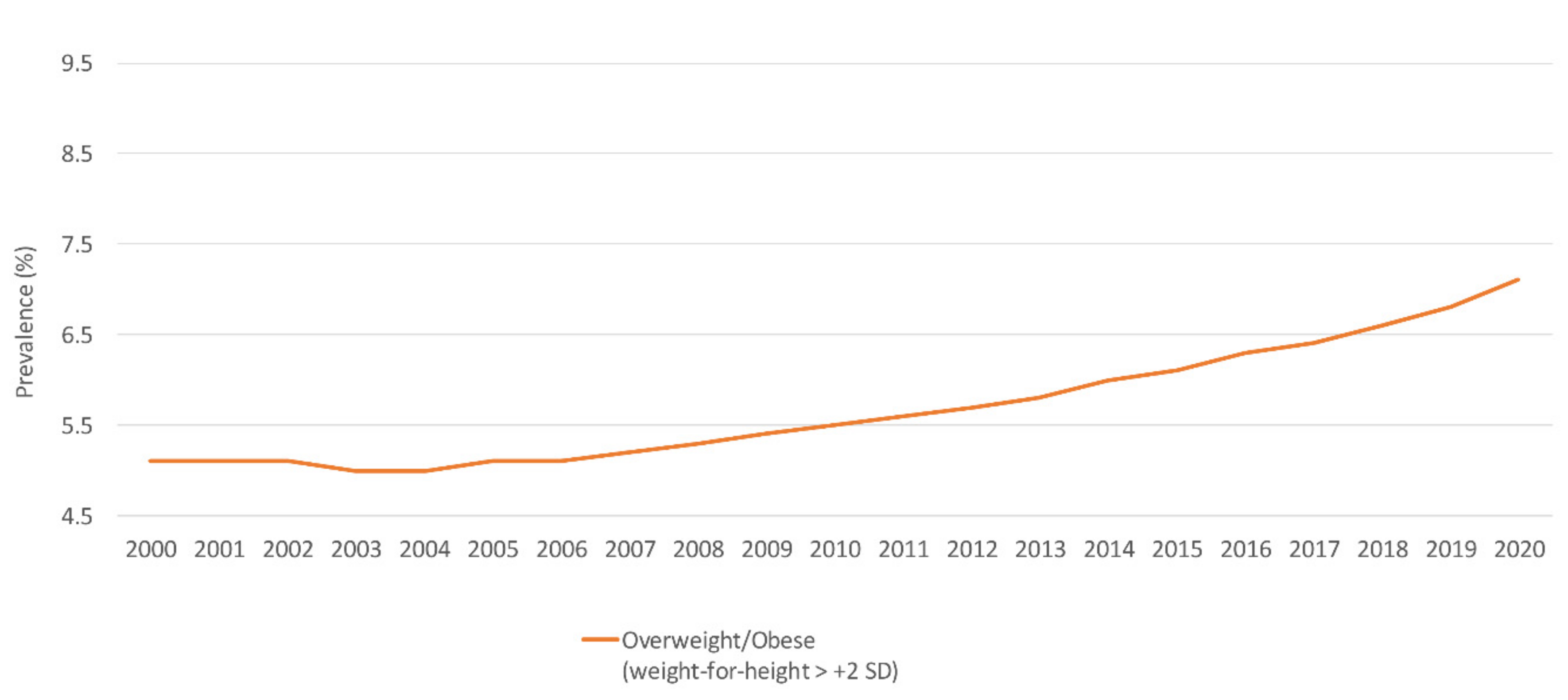
Jordan is witnessing an escalating pace of nutrition transition, which may be associated with an increased burden of malnutrition and related non-communicable diseases. The nutrition situation in Jordan is analyzed by exploring specific nutrition indicators, namely infant and young child feeding, low birthweight, micronutrient deficiencies, anthropometric indicators, and food consumption patterns. Results showed that although most children were ever breastfed and early initiation of breastfeeding had a two-fold increasing trend, rates of exclusive breastfeeding below 6 months of age and continued breastfeeding until two years of age were low. Complementary feeding indicators, particularly minimum diet diversity and minimum acceptable diet standards, were suboptimal. An overall low burden of stunting, wasting, and underweight among children under 5 years and remarkable progress in optimizing iodine status among school-aged children were reported. Conversely, the burden of low birthweight and overweight/obesity exacerbated, coexisting with anemia, vitamin A deficiency, and vitamin D deficiency. Overall, fruit and vegetable consumption were inadequate. The consumption of soft drinks and salt on the other hand was higher than recommended. The double burden of malnutrition in Jordan is acknowledged and recommends the prioritization and evaluation of interventions towards improving the population’s nutritional status and achieving nutrition targets.
1. Introduction
2. Breastfeeding Indicators
3. Complementary Feeding Indicators
3.1. Low Birthweight
3.2. Stunting, Wasting and Underweight among Children under 5 Years
4. Micronutrient Deficiencies
4.1. Anemia
Children under 5 Years
Women of Reproductive Age
4.2. Vitamin A Deficiency
Children under 5 Years
Women of Reproductive Age
4.3. Vitamin D Deficiency
Children under 5 Years
Adults and Women of Reproductive Age
4.4. Iodine Deficiency
5. Overweight and Obesity
5.1. Children under 5 Years
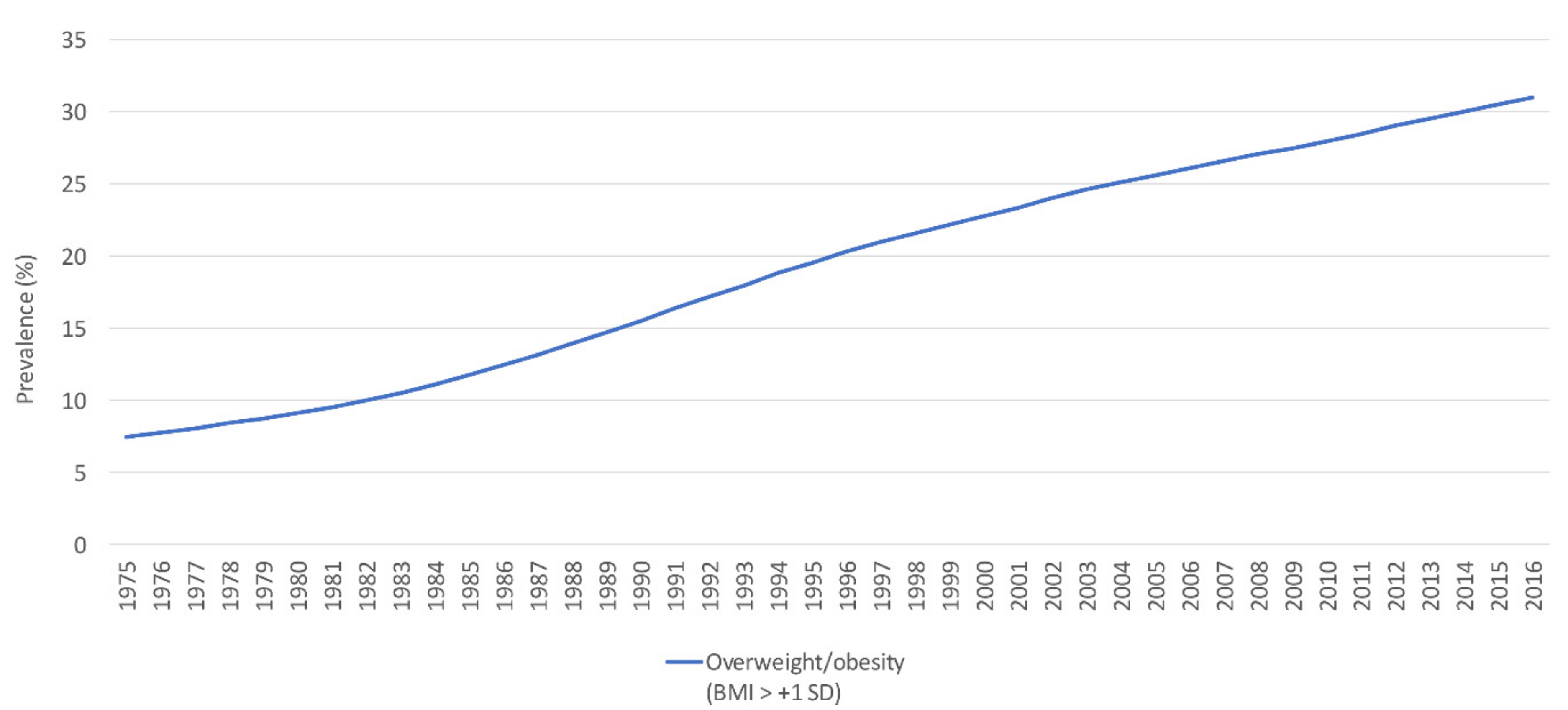
5.2. School-Aged Children and Adolescents
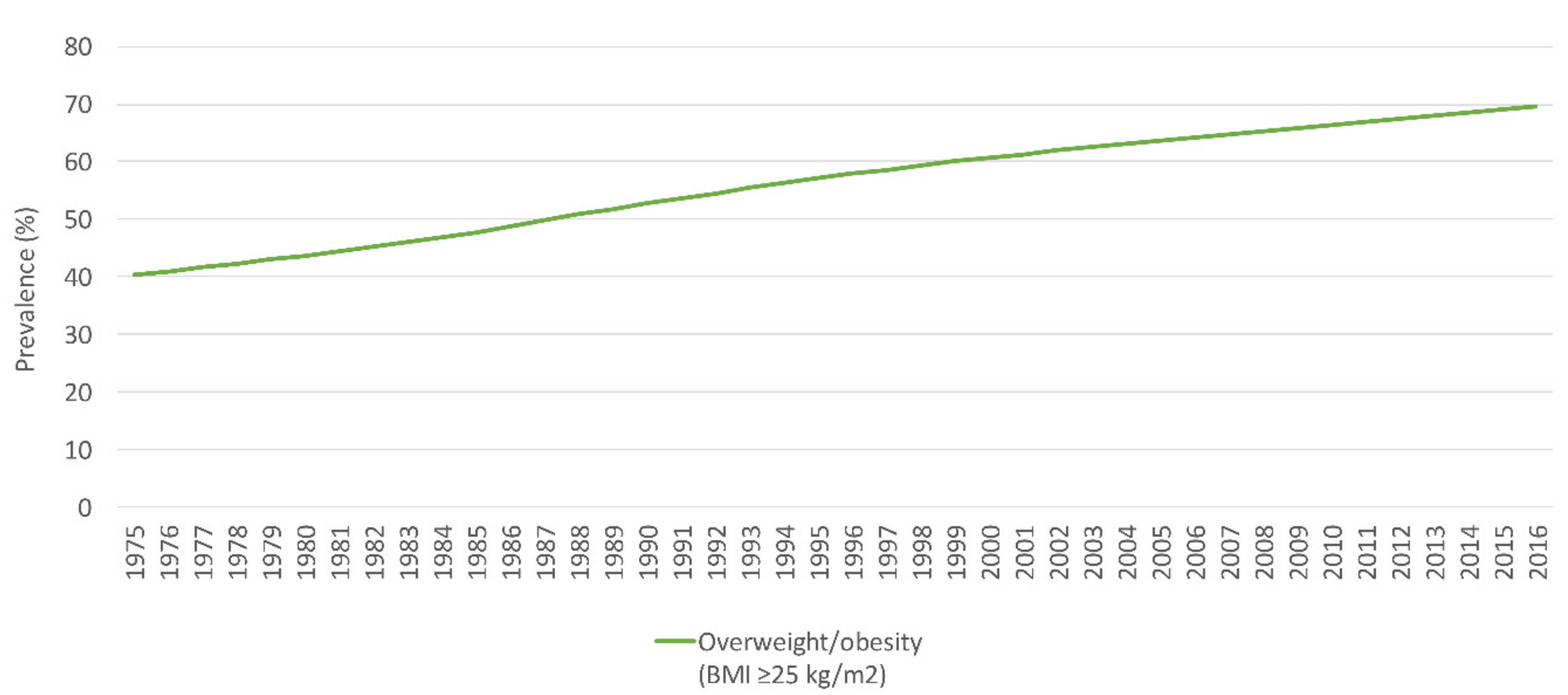
5.3. Adults and Women of Reproductive Age
6. Food Consumption Patterns
6.1. Children under 5 Years and Adolescents
6.2. Adults and Women of Reproductive Age
7. National Nutrition Policies and Strategies in Jordan
7.1. The Baby Friendly Hospital Initiative (BFHI) and the International Code of Marketing of Breast-Milk Substitutes
7.2. Food Fortification and Micronutrient Supplementation
7.3. Multisectoral Coordination to Tackle Obesity
References
- World Health Organization. Malnutrition. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 2 October 2021).
- Global Nutrition Report. 2020 Global Nutrition Report: Action on Equity to End Malnutrition; Development Initiatives: Bristol, UK, 2020; Available online: https://globalnutritionreport.org/reports/2020-global-nutrition-report/ (accessed on 4 October 2021).
- Nasreddine, L.; Ayoub, J.; Al Jawaldeh, A. Review of the nutrition situation in the Eastern Mediterranean Region. East. Mediterr. Health J. 2018, 24, 77–92.
- World Health Organization Regional Office for the Eastern Mediterranean. Strategy on Nutrition for the Eastern Mediterranean Region 2020–2030. World Health Organization. Regional Office for the Eastern Mediterranean. License: CC BY-NC-SA 3.0 IGO. 2019. Available online: https://apps.who.int/iris/handle/10665/330059 (accessed on 3 October 2021).
- World Health Organization Regional Office for the Eastern Mediterranean. Nutrition: Malnutrition. Malnutrition in All Its Forms. 2021. Available online: http://www.emro.who.int/nutrition/double-burden-of-nutrition/index.html (accessed on 5 October 2021).
- Groce, N.; Challenger, E.; Berman-Bieler, R.; Farkas, A.; Yilmaz, N.; Schultink, W.; Clark, D.; Kaplan, C.; Kerac, M. Malnutrition and disability: Unexplored opportunities for collaboration. Paediatr. Int. Child. Health 2014, 34, 308–314.
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451.
- Itoh, H.; Kanayama, N. Nutritional conditions in early life and risk of non-communicable diseases (NCDs) from the perspective of preemptive medicine in perinatal care. Hypertens Res. Pregnancy 2015, 3, 1–12.
- World Health Organization. Comprehensive Implementation Plan on Maternal, Infant and Young Child Nutrition. 2014. Available online: https://apps.who.int/iris/bitstream/handle/10665/113048/WHO_NMH_NHD_14.1_eng.pdf (accessed on 27 September 2021).
- World Health Organization. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 October 2021).
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.-P.; Bentham, J. The epidemiological burden of obesity in childhood: A worldwide epidemic requiring urgent action. BMC Med. 2019, 17, 212.
- Hu, F.B. Overweight and obesity in women: Health risks and consequences. J. Women’s Health 2003, 12, 163–172.
- The World Bank. World Bank Country and Lending Groups. 2021. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519 (accessed on 5 October 2021).
- Nasreddine, L.M.; Kassis, A.N.; Ayoub, J.J.; Naja, F.A.; Hwalla, N.C. Nutritional status and dietary intakes of children amid the nutrition transition: The case of the Eastern Mediterranean Region. Nutr. Res. 2018, 57, 12–27.
- Department of Statistics (DOS) and ICF. Jordan Population and Family Health Survey 2017–2018; DOS and ICF: Amman, Jordan; Rockville, MD, USA, 2019.
- Neves, P.A.; Vaz, J.S.; Maia, F.S.; Baker, P.; Gatica-Domínguez, G.; Piwoz, E.; Rollins, N.; Victora, C.G. Rates and time trends in the consumption of breastmilk, formula, and animal milk by children younger than 2 years from 2000 to 2019: Analysis of 113 countries. Lancet Child. Adolesc. Health 2021, 5, 619–630.
- UNICEF. Infant and Young Child Feeding. 2021. Available online: https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/ (accessed on 7 August 2021).
- Islam, M.M.; Ababneh, F.; Akter, T.; Khan, H.R. Prevalence and risk factors for low birth weight in Jordan and its association with under-five mortality: A population-based analysis. East. Mediterr. Health J. 2020, 26, 1273–1284.
- Department of Statistics (DOS) and ICF International. Jordan Population and Family Health Survey 2012; Department of Statistics and ICF International: Calverton, MD, USA, 2013.
- Department of Statistics (DOS) and Macro International Inc. Jordan Population and Family Health Survey 2007; Department of Statistics and Macro International Inc.: Calverton, MD, USA, 2008.
- Department of Statistics (DOS) and ORC Macro. Jordan Population and Family Health Survey 2002; Department of Statistics & ORC Macro: Calverton, MD, USA, 2003.
- Department of Statistics (DOS) and Macro International Inc. Jordan Population and Family Health Survey 1997; Department of Statistics & Macro International: Calverton, MD, USA, 1998.
- Department of Statistics (DOS) and IRD/Macro International. Jordan Population and Family Health Survey 1990; Department of Statistics & IRD/Macro International: Calverton, MD, USA, 1992.
- UNICEF. Malnutrition. 2021. Available online: https://data.unicef.org/topic/nutrition/malnutrition/ (accessed on 10 August 2021).
- World Health Organization. Global Health Observatory Data Repository. Child Malnutrition by Country. Available online: https://apps.who.int/gho/data/node.main.CHILDMALNUTRITION?lang=en (accessed on 14 August 2021).
- UNICEF. Malnutrition Data. 2021. Available online: https://data.unicef.org/resources/dataset/malnutrition-data/ (accessed on 10 August 2021).
- FAO. Food and Nutrition Profile, Jordan. 2011. Available online: http://www.fao.org/3/aq039e/aq039e.pdf (accessed on 18 September 2021).
- Ministry of Health-Jordan; Global Alliance for Improved Nutrition (GAIN); United States Center for Disease Control and Prevention (CDC); United Nation Children’s Fund (UNICEF). National Micronutrient Survey-Jordan 2010; Ministry of Health: Amman, Jordan, 2011.
- Serdula, M.; Nichols, E.; Aburto, N.; Masa’d, H.; Obaid, B.; Wirth, J.; Tarawneh, M.; Barham, R.; Hijawi, B.; Sullivan, K. Micronutrient status in Jordan: 2002 and 2010. Eur. J. Clin. Nutr. 2014, 68, 1124–1128.
- World Health Organization. Global Health Observatory Data Repository. Anaemia in Children <5 Years: Estimates by Country. 2021. Available online: https://apps.who.int/gho/data/view.main.ANEMIACHILDRENv?lang=en (accessed on 18 August 2021).
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System. Geneva, World Health Organization (WHO/NMH/NHD/MNM/11.1). 2011. Available online: https://www.who.int/vmnis/indicators/haemoglobin.pdf (accessed on 4 October 2021).
- World Health Organization. Vitamin and Mineral Nutrition Information System (VMNIS). WHO Global Database on Vitamin A Deficiency. The Vitamin A Deficiency Database Includes Data by Country Based on Xerophthalmia and/or Serum or Plasma retinol Concentration. 2006. Available online: https://www.who.int/vmnis/vitamina/data/database/countries/jor_vita.pdf (accessed on 4 September 2021).
- Nichols, E.K.; Khatib, I.M.D.; Aburto, N.J.; Serdula, M.K.; Scanlon, K.S.; Wirth, J.P.; Sullivan, K.M. Vitamin D status and associated factors of deficiency among Jordanian children of preschool age. Eur. J. Clin. Nutr. 2015, 69, 90–95.
- El-Khateeb, M.; Khader, Y.; Batieha, A.; Jaddou, H.; Hyassat, D.; Khawaja, N.; Abujbara, M.; Ajlouni, K. Vitamin D deficiency and associated factors in Jordan. SAGE Open Med. 2019, 7, 2050312119876151.
- Batieha, A.; Khader, Y.; Jaddou, H.; Hyassat, D.; Batieha, Z.; Khateeb, M.; Belbisi, A.; Ajlouni, K. Vitamin D status in Jordan: Dress style and gender discrepancies. Annu. Nutr. Metab. 2011, 58, 10–18.
- Nichols, E.; Khatib, I.; Aburto, N.; Sullivan, K.; Scanlon, K.; Wirth, J.; Serdula, M. Vitamin D status and determinants of deficiency among non-pregnant Jordanian women of reproductive age. Eur. J. Clin. Nutr. 2012, 66, 751–756.
- WHO Regional Office for the Eastern Mediterranean. Wheat Flour Fortification in the Eastern Mediterranean Region. License: CC BY-NC-SA 3.0 IGO. 2019. Available online: https://apps.who.int/iris/handle/10665/311730?locale-attribute=fr& (accessed on 18 September 2021).
- Massa’d, H.; Barham, R. National Survey to Assess Iodine Deficiency Disorders (IDD) among Jordanian Children—2010; Jordan Ministry of Health Nutrition Department, World Health Organization Non-Communicable Disease Department: Amman, Jordan, 2011.
- World Health Organization. Vitamin and Mineral Nutrition Information System (VMNIS). WHO Global Database on Iodine Deficiency: The Database on Iodine Deficiency Includes Data by Country on Goitre Prevalence and/or Urinary Iodine Concentration. 2006. Available online: https://www.who.int/vmnis/iodine/data/database/countries/per_idd.pdf (accessed on 4 September 2021).
- Zayed, A.A.; Beano, A.M.; Haddadin, F.I.; Radwan, S.S.; Allauzy, S.A.; Alkhayyat, M.M.; Al-Dahabrah, Z.A.; Al-Hasan, Y.G.; Yousef, A.-M.F. Prevalence of short stature, underweight, overweight, and obesity among school children in Jordan. BMC Public Health 2016, 16, 1040.
- Al Qaseer, B.M.; Batarseh, S.; Asaad, A. Global School-Based Student Health Survey; MoH Jordan, CDC and WHO: Amman, Jordan, 2007; Available online: https://www.who.int/ncds/surveillance/gshs/GSHS_Country_Report_Jordan_2007.pdf (accessed on 17 August 2021).
- Al Qaseer, B.M.; Al Jawhari, N.M.; Kharabsheh, S.H. Global School-Based Student Health Survey; MoH Jordan, CDC and WHO: Amman, Jordan, 2004; Available online: https://www.who.int/ncds/surveillance/gshs/final%20copy%20of%20GSHS%20Country%20Report%20of%20Jordan.pdf (accessed on 17 August 2021).
- World Health Organization. The Global Health Observatory: Explore a World of Health Data. Prevalence of Overweight among Children and Adolescents, BMI > +1 Standard Deviations above the Median (Crude Estimate) (%). 2021. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-overweight-among-children-and-adolescents-bmi-1-standard-deviations-above-the-median-(crude-estimate)-(-) (accessed on 14 August 2021).
- MOH. Jordan National Stepwise Survey (STEPs) for Noncommunicable Diseases Risk Factors 2019. The Ministry of Health, Jordan, WHO. 2020. Available online: https://www.who.int/publications/m/item/2019-steps-country-report-jordan (accessed on 15 August 2021).
- MOH. Jordan National Stepwise Survey (STEPs) for Noncommunicable Diseases Risk Factors 2004. The Ministry of Health, Jordan, WHO. 2004. Available online: https://www.who.int/publications/m/item/2004-steps-country-report-jordan (accessed on 18 August 2021).
- MOH. Jordan National Stepwise Survey (STEPs) for Noncommunicable Diseases Risk Factors 2007. The Ministry of Health, Jordan, WHO. 2007. Available online: https://www.who.int/publications/m/item/2007-steps-country-report-jordan (accessed on 21 August 2021).
- World Health Organization. Growth Reference Data for 5–19 Years. Indicators: BMI-for-Age (5–19 Years). 2021. Available online: https://www.who.int/toolkits/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed on 17 August 2021).
- World Health Organization. The Global Health Observatory: Explore a World of Health Data. Prevalence of Anaemia in Children Aged 6–59 Months (%). 2021. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-anaemia-in-children-under-5-years-(-) (accessed on 25 August 2021).
- Hasan, M.M.; Ahmed, S.; Magalhaes, R.J.S.; Fatima, Y.; Biswas, T.; Mamun, A.A. Double burden of malnutrition among women of reproductive age in 55 low-and middle-income countries: Progress achieved and opportunities for meeting the global target. Eur. J. Clin. Nutr. 2021.
- World Health Organization. Jordan STEPS Survey 2007 Fact Sheet. 2007. Available online: https://cdn.who.int/media/docs/default-source/ncds/ncd-surveillance/data-reporting/jordan/steps/2007-fact-sheet-jordan.pdf?sfvrsn=df1a70ea_2&download=true (accessed on 4 October 2021).
- World Health Organization. Policy-Nutrition in Jordan Update and Plan of Action. 2006. Available online: https://extranet.who.int/nutrition/gina/en/node/23541 (accessed on 22 October 2021).
- World Health Organization. Implementation Guidance: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services-the Revised Baby-Friendly Hospital Initiative; License: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2018.
- Abul-Fadl, A.; Farghaly, N.F.; Alsumaie, M.A.; Bozo, M.; Al-Jawaldeh, A. Satisfaction with code implementation and Baby-friendly practices in the Eastern Mediterranean region: Health professional perspectives from 15 countries. Indian J. Child. Health 2021, 8, 60–69.
- Al-Jawaldeh, A.; Abul-Fadl, A.; Farghaly, N.F. Enacting the Code by effective national laws influence trends in exclusive breastfeeding: An analytical study from the Eastern Mediterranean Region. Indian J. Child. Health 2021, 8, 12–19.
- Al-Jawaldeh, A.; Abul-Fadl, A. Assessment of the baby friendly hospital initiative implementation in the Eastern Mediterranean Region. Children 2018, 5, 41.
- Al-Jawaldeh, A.; Taktouk, M.; Doggui, R.; Abdollahi, Z.; Achakzai, B.; Aguenaou, H.; Al-Halaika, M.; Almamary, S.; Barham, R.; Coulibaly-Zerbo, F. Are Countries of the Eastern Mediterranean Region on Track towards Meeting the World Health Assembly Target for Anemia? A Review of Evidence. Int. J. Environ. Res. Public Health 2021, 18, 2449.
- World Health Organization Regional Office for the Eastern Mediterranean. Nutrition: Publications. Success Stories. 2021. Available online: http://www.emro.who.int/nutrition/resources/success-stories.html (accessed on 5 October 2021).

