Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | khatereh zarkesh | -- | 2391 | 2023-07-14 11:07:08 | | | |
| 2 | Rita Xu | -59 word(s) | 2332 | 2023-07-14 11:46:31 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Zarkesh, K.; Akbarian, M.; Tayebi, L.; Uversky, V.N.; Rubio-Casillas, A.; Redwan, E.M. SARS-CoV-2 Peptide Vaccines. Encyclopedia. Available online: https://encyclopedia.pub/entry/46810 (accessed on 28 June 2026).
Zarkesh K, Akbarian M, Tayebi L, Uversky VN, Rubio-Casillas A, Redwan EM. SARS-CoV-2 Peptide Vaccines. Encyclopedia. Available at: https://encyclopedia.pub/entry/46810. Accessed June 28, 2026.
Zarkesh, Khatereh, Mohsen Akbarian, Lobat Tayebi, Vladimir N. Uversky, Alberto Rubio-Casillas, Elrashdy M. Redwan. "SARS-CoV-2 Peptide Vaccines" Encyclopedia, https://encyclopedia.pub/entry/46810 (accessed June 28, 2026).
Zarkesh, K., Akbarian, M., Tayebi, L., Uversky, V.N., Rubio-Casillas, A., & Redwan, E.M. (2023, July 14). SARS-CoV-2 Peptide Vaccines. In Encyclopedia. https://encyclopedia.pub/entry/46810
Zarkesh, Khatereh, et al. "SARS-CoV-2 Peptide Vaccines." Encyclopedia. Web. 14 July, 2023.
Copy Citation
Several times during the past two decades, epidemic viral diseases created global challenges. Although many solutions have been proposed to deal with this tight spot, it is still believed that public vaccination represents the most effective strategy to handle it. So far, various kinds of vaccines including protein subunits, virus-like particles, inactivated, live attenuated, viral vectors, RNA, and DNA vaccines have been used in the prevention of COVID-19. Among the various categories of vaccines, peptide vaccines have created a new hope for quick and trustworthy access due to the development of proteomics equipment.
SARS-CoV-2
peptide vaccines
COVID-19 vaccination
1. Introduction
Looking through the historical lens, every few decades human health has faced epidemic diseases that seriously endanger human life [1]. Viral infection on a population scale is one of the oldest risks that always emerge with new faces. The infections can spread rapidly through the public, particularly in areas with a high population density. The transmission of a virus usually depends on factors, such as the mode of transmission, the virulence of the virus, and the vulnerability of the population. Some viral infections, such as the common cold or flu, are relatively mild and are typically self-limiting. However, other viral infections such as the coronavirus family can be much more severe and may lead to serious health consequences and/or death. When a viral infection spreads through a population, it can quickly lead to an outbreak or epidemic. In some cases, the infection may continue to spread and become a pandemic, affecting populations across multiple countries or continents [1][2].
The SARS-CoV-2 belongs to the Coronaviridae family. This is an enveloped positive-stranded RNA (ribonucleic acid) virus, which has the largest viral genome (26–33 kilobases) among the RNA viruses [3]. According to the phylogenetic classification, Coronavirinae can be further divided into four groups; alpha, beta, gamma, and delta. This subfamily has been identified to infect mammals and birds, including bats, mice, pigs, dogs, cows, chickens, horses, and humans [4]. Few studies are showing that bats can host many types of coronaviruses, which vary dramatically depending on the living area and the type of bat. It seems that these animals are the natural reservoir of this subfamily.
Human coronaviruses (HCoVs) are related to numerous respiratory diseases of varying severity, including pneumonia and bronchitis. Today, the human coronavirus is known as one of the fastest-changing viruses due to the high speed of genomic nucleotide exchange and recombination [5]. Viruses associated with severe acute respiratory syndrome (SARS) and Middle East acute respiratory syndrome (MERS) are among the types of pathogens related to Coronavirinae, which are common between humans and animals and can cause severe respiratory disease in humans [6]. SARS coronavirus (SARS-CoV) first appeared in China in 2002. The outbreak of SARS-CoV lasted for eight months, almost 10 years after the emergence of SARS-CoV (also known as SARS-CoV-1), a highly pathogenic human coronavirus with the name MERS coronavirus (MERS-CoV) appeared in Saudi Arabia. SARS-CoV-2, another type of coronavirus originally named “novel coronavirus” was identified in Wuhan, China in December 2019. Based on the different analyses, the stable mutation in the nonstructural protein 2 (nsp2) has led to SARS-CoV-2 being more contagious than SARS-CoV-1 [7].
SARS-CoV-2 as an RNA virus is genetically located in the beta coronavirus category and uses a glycoprotein (spike protein) to bind to the angiotensin-converting enzyme 2 (ACE2) receptor [8]. Following SARS-CoV-2 infection, some infected people may remain asymptomatic or have only mild symptoms, whereas others develop pneumonia and acute respiratory distress syndrome (ARDS) that require intubation in special care units and often causes complications with unfavorable results. Mortality is associated with age, the presence of underlying (background) diseases, the severity of the disease, increased respiratory failure, a low number of lymphocytes, and previous infection [9]. The transmission of SARS-CoV-2 is through respiratory droplets. According to some studies, the virus may be transferable in some people 5 to 13 days after discharge and partial recovery of the disease; therefore, it is necessary to take precautions for the patients during the recovery phase. As mentioned, ACE2 acts as a receptor for the entry of the SARS-CoV-2 virus [10]. Widespread expression of the receptor in various cells, such as alveolar type II (AT2) cells of the lung, upper esophagus, epithelial cells, absorptive enterocytes of the ileum and large intestine may play a significant role in the infection pathways associated with SARS-CoV-2 virus [11].
When designing a vaccine, researchers must first have complete information regarding the characteristics of the antigen, adjuvant, vaccine manufacturing, and delivery system. Due to the rapid availability of genomic and structural information on the SARS-CoV-2 virus for researchers, the efficient production of recombinant vaccines was faster than the production of weakened and inactivated live vaccines [12]. Also, the available information on the production of vaccines against SARS/MERS has been helpful for the development of vaccines against SARS-CoV-2. The use of nanotechnology systems has provided great acceleration in the production of new and efficient vaccines and has helped a lot in the development of new vaccines [13].
2. Methodological Routes to Discover and Finalize a Peptide as a Protective Agent
The idea of using peptides to stimulate the immune system has a very long history. However, the entry of this concept into the field of modern medicine is due to the studies of William Bradley Coley (1862–1936). Studies show that the peptides as vaccine candidates against SARS-CoV-2 are generally synthetic [14]. It is expected that the sequence of a peptide vaccine (which is between 20 and 30 amino acids) must be immunogenic or able to disrupt a stage of the virus’s path of pathogenesis. When it comes to the synthesis of peptide vaccines, it is expected that their production process will be carried out with higher precision and reproducibility, which will guarantee the quality of vaccination, as well as the speed of their industrialization [15]. However, studies on some of these types of peptides show that due to the not enough strong immune response they create, the presence of adjuvants is always needed to obtain an adequate response [14]. Another challenge that has been observed is their vulnerability to proteases in the body’s environment. As a result, most peptide vaccines do not have much resistance against proteases. However, it is suggested that the challenge can be overcome by inserting the vaccines into liposomes, conjugation on the surface of other carrier proteins, or connecting them to the surfaces of nanoparticles [16]. In this section, according to Figure 1, the methodological ways by which peptide vaccines can be proposed are presented.
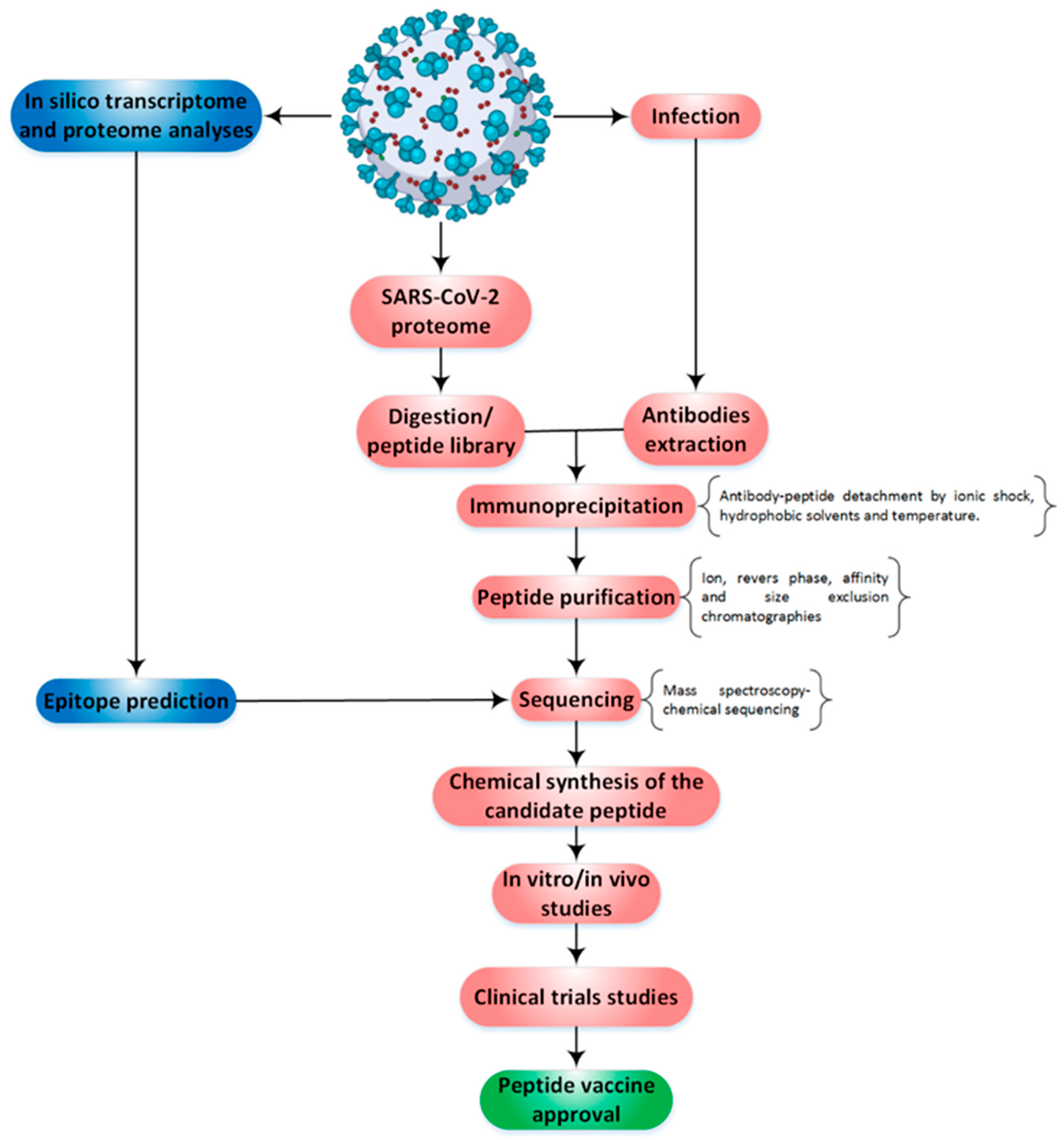
Figure 1. The steps are taken to obtain a final vaccine peptide. The path to reach the peptide vaccine is from either top to bottom or vice versa. In the scheme, in the pink part: first different peptides are extracted from SARS-CoV-2, and then the final peptide sequence is achieved by performing other steps. In another path (blue), a specific sequence is obtained from the beginning according to the considerations of different in silico studies, and then an attempt is made to confirm the function of the proposed peptide with its chemical synthesis. It is believed that the first path is associated with more effort and higher confidence, while the second path, although the result is less certain, takes less time. Sometimes a mix of both routes is adopted to go through the peptide vaccine approval process.
Depending on the aim of the research, it is possible to extract the proteome of SARS-CoV-2 from the entire viral proteome or a part of the virus structure; e.g., the membrane. For the virus, it has been stated that reverse transcription-polymerase chain reaction is the most useful way to reach the virus genome in infected patients [17]. However, although this path is well explained and implemented, it has dark spots that cast a shadow on the accuracy of the extracted outputs. For example, the presence of some mutations on the path from gene to protein may cause the final prediction of the protein sequence from the gene with a percentage of error [18]. Therefore, although the direct examination of the viral proteome is a time-consuming and long process, the obtained data are more trustable. In general, it has been seen that there are gene sequences for 28 proteins in SARS-CoV, of which only 16 proteins have been structurally characterized [19]. Utilization of the mass spectroscopic techniques in combination with the computer-aided analyses of data allowed for the characterization of the interactions between the known proteome in SARS-CoV-1 and -2 with host cellular proteins and revealed that there are a total of 1484 interactions between them [20][21]. This sequencing process is highly accurate for peptides that are obtained from enzymatic digestion in vitro, however, for peptides that are obtained in antigen-presenting cells (in vivo digestion), it doesn’t show high accuracy. As a result, whether the viral proteome originated from antigen-presenting cells or directly prepared from viral enzymatic digestion will be a decisive turn point in the accuracy of the information obtained by mass spectrometry sequencing [21].
3. Landscape of SARS-CoV-2 Peptide Vaccines on Clinical Trials
Based on the document published by the World Health Organization (WHO) [22], by February 2022, 146 vaccines are being developed to the clinical stage, and 159 vaccines are currently under investigation in the pre-clinical phase [23][24]. The subunit protein platform comprises 33% of all vaccines in the clinical phase (see Figure 2).
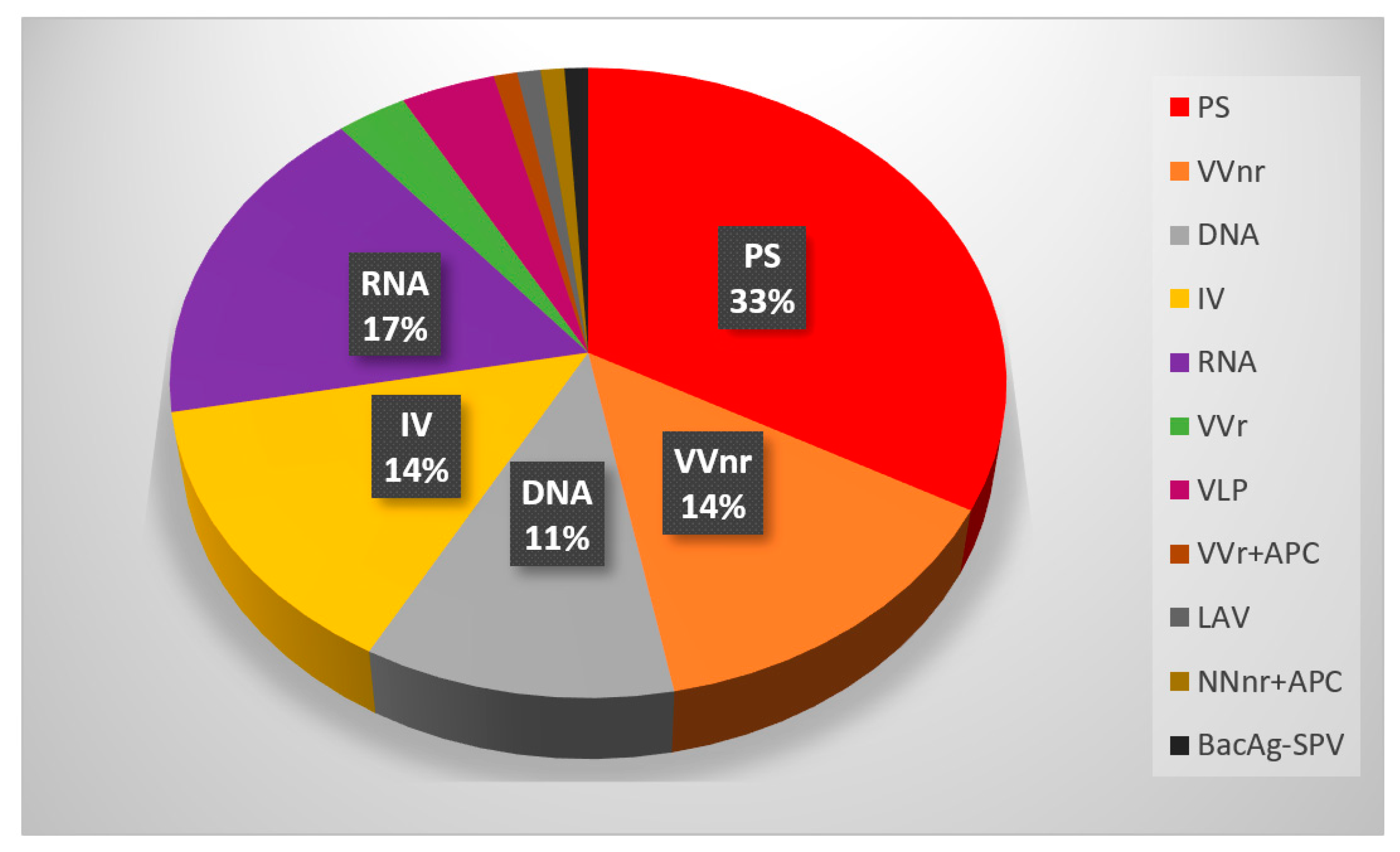
Figure 2. Candidates in the clinical phase, protein subunit vaccine includes the greatest percentage among vaccines in the clinical trial phase. The most candidate for the COVID-19 vaccine in the clinical trial phase is the Protein subunit (ps). After that, RNA, Viral Vector (non-replicating, Inactivated Virus (IV), and DNA vaccines have a higher portion of clinical trial phase vaccines. Protein subunit (ps), Viral Vector (non-replicating) (VVnr), Inactivated Virus (IV), Viral Vector (replicating) (VVr), Virus Like Particle (VLP), VVr + Antigen Presenting Cell (VVr + APC), Live Attenuated Virus (LAV), VVnr + Antigen Presenting Cell (NNnr + APC), Bacterial antigen-spore expression vector (BacAg-SPV).
CoVepiT (OSE-13E) is a multivariate vaccine candidate versus SARS-CoV-2 in clinical stage 1. This peptides-based vaccine represents CD8+T-cell-mediated immune response against 11 different proteins of the SARS-CoV-2 virus including Spike, Membrane, Nucleocapsid, and several non-structural proteins. 48 non-COVID-19 volunteers received one single dose or two doses separated by 21 days and the safety and Immunogenicity of the vaccine were evaluated. CD8+ T cells responding to wild-type SARS-CoV-2 epitopes remarkably increased after 22 days, 3, and 6 months of vaccination. the study was estimated in March 2022, but no other results have yet been published [25].
Enrollments were selected among those who have received 2 doses of Vero cell (Inactivated COVID-19 vaccine). A dose of the recombinant COVID-19 vaccine will be administered in different time schedules (4–6 months, 7–9 months, and more than 9 months). In total, 3580 enrollment precipitated phases 1 and 2 in China. Following the results, phase 3 is going on 1848 enrollment in the United Arab Emirates. Furthermore, a study on Subject who has been vaccinated intramuscularly with three doses of the Recombinant COVID-19 vaccine (0, 30, and 60 days) is going [26]. The study is scheduled to be finished in February 2024.
COVAC-1 is a vaccine designed by the University of Saskatchewan against a specific portion of the spike protein of SARS-CoV-2 (S1 protein) spike protein. In addition, it contains three different TriAds adjuvants that can enhance the immune response. A multi-national and Phase 1 trial on the Safety and immunogenicity is ongoing in different doses of S1 protein (25 and 50 µg) administered twice (4 weeks apart) in healthy adults. Although the promising safety and immunogenicity results of phase 1 of the vaccine were published in the journal Nature in November 2021 [17], they decided not to move forward with the study design (Withdrawn) [27].
Another phase 1 and phase 2 clinical trial study by the Beijing Institute of Microbiology and Epidemiology (Beijing, China) and Zhongyianke Biotech Co., Ltd. (Tianjin, China) was accomplished. 216 volunteers who received three doses of 40 μg SCoK (NCT04636333) showed appropriate safety and immunogenicity. SCoK is a recombinant SARS-CoV-2 vaccine (CHO cell). No severe local and systemic adverse effects in participating groups. The phase 3 clinical trial is under consideration on safety and antibody titer against the live virus [28].
The efficacy and safety of SCB-2019 (NCT04405908), a protein subunit vaccine, was evaluated in 216 healthy volunteers who received 2 doses of 3 μg to 30 μg vaccine. Also, the role of two different adjuvants in the immunogenicity of the vaccine, including CpG 1018 adjuvant plus Alum adjuvant and AS03 was investigated [29]. S-Trimer protein with both adjuvants demonstrated remarkable humoral and cellular immune responses against COVID-19. 30 microgram (μg) CpG 1018/Alum-adjuvanted SCB-2019 vaccine was selected as a suitable vaccine for phase 2 and 3 studies. The vaccine is administered as a booster dose after 4 months with a second injection. However, the study is active; results have not yet been published [30].
In a parallel study in Colombia, the safety of candidate SCB-2019 on 3820 <18 years old participants will accomplish. The study is a dose-finding and phase 2/3. The study is estimated to finish in July 2024 [31].
Another protein subunit vaccine is COVAX19 (Spikogen®) which Vaxine Pty Ltd. sponsors. The healthy volunteer received one dose of (25 μg) Spike antigen plus 15 mg Advax-CpG55.2™ adjuvant. The vaccine could make neutralizing antibodies against SARS-CoV-2. Following the appropriate finds of phases 1 and 2, Spikogen® was administered as a booster dose to assess the safety and titer of neutralizing antibodies [32]). No extreme adverse reaction was observed. The remarkable result is that the immune response was established against severe variants such as Omicron and Delta [33]. Another protein subunit vaccine is NVX-CoV2373, a recombinant spike protein of SARS-CoV-2. A Phase 1/2 and dose-finding study were assessed for safety and reactogenicity of alone NVX-CoV2373 vaccine and with Matrix-M1 adjuvant [34]. The finding showed all participants indicated high tolerated and immunogenicity with a 2-dose of 5 μg vaccine. Following the results, 1610 participants showed a gradual immune response, when administered as a booster dose of NVX-CoV2373 [35]. Figure 3 shows the schematic of the EpiVaCcorona vaccine, which is based on a peptide produced in Russia.
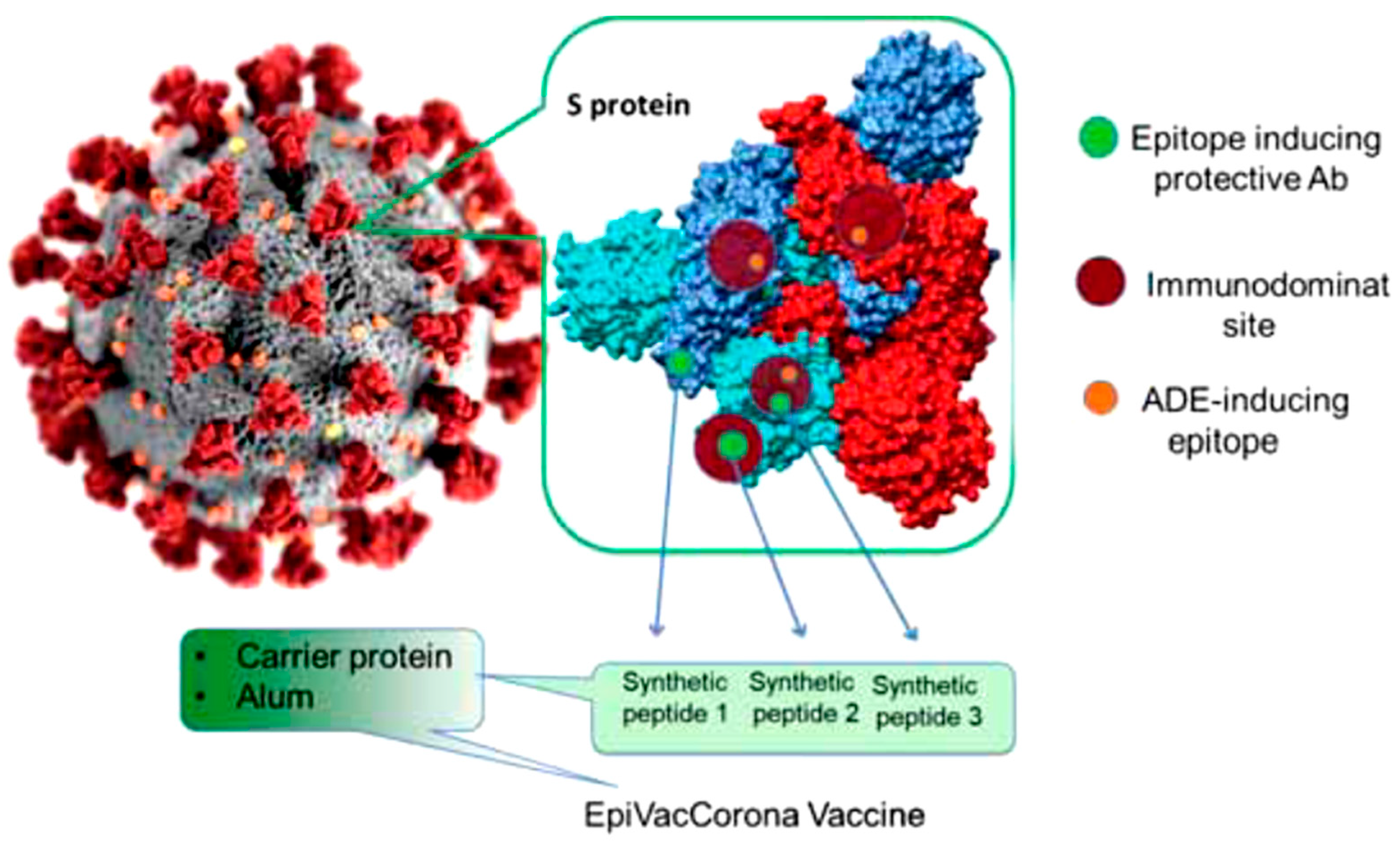
Figure 3. Schematic of EpiVacCorona (EpiVacCorona vaccine based on peptide antigens for the prevention of COVID-19). B cell epitopes (red circle) located on the virus s protein were selected using computer simulation methods. The immunogenic epitopes which lead to severe infection were excluded. From the 3 selected epitopes (green circle), peptides containing 20–31 amino acids were designed and synthesized. This platform contains three synthetic peptides similar to the s protein of SARS-2 conjugated to a chimeric recombinant protein carrier.
References
- Burrell, C.J.; Howard, C.R.; Murphy, F.A. Epidemiology of viral infections. Fenner White’s Med. Virol. 2017, 185–203.
- Zarkesh, K.; Entezar-Almahdi, E.; Ghasemiyeh, P.; Akbarian, M.; Bahmani, M.; Roudaki, S.; Fazlinejad, R.; Mohammadi-Samani, S.; Firouzabadi, N.; Hosseini, M.; et al. Drug-based therapeutic strategies for COVID-19-infected patients and their challenges. Future Microbiol. 2021, 16, 1415–1451.
- Fehr, A.R.; Perlman, S. Coronaviruses: An overview of their replication and pathogenesis. Coronaviruses Methods Protoc. 2015, 1–23.
- Zhang, S.F.; Tuo, J.L.; Huang, X.B.; Zhu, X.; Zhang, D.M.; Zhou, K.; Yuan, L.; Luo, H.J.; Zheng, B.J.; Yuen, K.Y.; et al. Epidemiology characteristics of human coronaviruses in patients with respiratory infection symptoms and phylogenetic analysis of HCoV-OC43 during 2010–2015 in Guangzhou. PLoS ONE 2018, 13, e0191789.
- Fung, T.S.; Liu, D.X. Human coronavirus: Host-pathogen interaction. Annu. Rev. Microbiol. 2019, 73, 529–557.
- Peiris, M.; Poon, L.L.M. Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) (Coronaviridae). Encycl. Virol. 2021, 814–824.
- World Health Organization. Coronavirus 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 4 July 2020).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733.
- Matricardi, P.M.; Dal Negro, R.W.; Nisini, R. The first, holistic immunological model of COVID-19: Implications for prevention, diagnosis, and public health measures. Pediatr. Allergy Immunol. 2020, 31, 454–470.
- Shang, J.; Ye, G.; Shi, K.; Wan, Y.; Luo, C.; Aihara, H.; Li, F. Structural basis of receptor recognition by SARS-CoV-2. Nature 2020, 581, 221–224.
- Dong, M.; Zhang, J.; Ma, X.; Tan, J.; Chen, L.; Liu, S.; Xin, Y.; Zhuang, L. ACE2, TMPRSS2 distribution and extrapulmonary organ injury in patients with COVID-19. Biomed. Pharmacother. 2020, 131, 110678.
- Lucchese, G. Epitopes for a 2019-nCoV vaccine. Cell. Mol. Immunol. 2020, 17, 539–540.
- Song, Z.; Xu, Y.; Bao, L.; Zhang, L.; Yu, P.; Qu, Y.; Zhu, H.; Zhao, W.; Han, Y.; Qin, C. From SARS to MERS, thrusting coronaviruses into the spotlight. Viruses 2019, 11, 59.
- Purcell, A.W.; McCluskey, J.; Rossjohn, J. More than one reason to rethink the use of peptides in vaccine design. Nat. Rev. Drug Discov. 2007, 6, 404–414.
- Nelde, A.; Rammensee, H.G.; Walz, J.S. The peptide vaccine of the future. Mol. Cell. Proteom. 2021, 20, 100022.
- Kianpour, M.; Akbarian, M.; Uversky, V.N. Nanoparticles for coronavirus control. Nanomaterials 2022, 12, 1602.
- Heitmann, J.S.; Bilich, T.; Tandler, C.; Nelde, A.; Maringer, Y.; Marconato, M.; Reusch, J.; Jäger, S.; Denk, M.; Richter, M.; et al. A COVID-19 peptide vaccine for the induction of SARS-CoV-2 T cell immunity. Nature 2022, 601, 617–622.
- Akbarian, M.; Lundstrom, K.; Redwan, E.M.; Uversky, V.N. Vaccine Development Strategies and the Current Status of COVID-19 Vaccines. In COVID-19: From Bench to Bedside; CRC Press: Boca Raton, FL, USA, 2022.
- Bartlam, M.; Xu, Y.; Rao, Z. Structural proteomics of the SARS coronavirus: A model response to emerging infectious diseases. J. Struct. Funct. Genom. 2007, 8, 85–97.
- Stukalov, A.; Girault, V.; Grass, V.; Bergant, V.; Karayel, O.; Urban, C.; Haas, D.A.; Huang, Y.; Oubraham, L.; Wang, A.; et al. Multi-level proteomics reveals host-perturbation strategies of SARS-CoV-2 and SARS-CoV. bioRxiv 2020, 1, 1.
- Dudek, N.L.; Croft, N.P.; Schittenhelm, R.B.; Ramarathinam, S.H.; Purcell, A.W. A systems approach to understand antigen presentation and the immune response. Proteom. Syst. Biol. Methods Protoc. 2016, 1394, 189–209.
- Worl Health Organization. Draft Landscape of COVID-19 Candidate Vaccines. 2 July 2020. Available online: https://www.who.int/publications/m/item/draft-landscape-of-COVID-19-candidate-vaccines (accessed on 4 July 2020).
- Fares, S.; Elmnyer, M.M.; Mohamed, S.S.; Elsayed, R. COVID-19 vaccination perception and attitude among healthcare workers in Egypt. J. Prim. Care Community Health 2021, 12, 21501327211013303.
- Yan, Z.P.; Yang, M.; Lai, C.L. COVID-19 vaccines: A review of the safety and efficacy of current clinical trials. Pharmaceuticals 2021, 14, 406.
- OSE Immunotherapeutics. A Randomized, Open Label, Phase 1 Study to Evaluate the Safety, Reactogenicity and Immunogenicity of OSE-13E, a Multiepitope-Based Vaccine Candidate against COVID-19, in Healthy Adults (COVEPIT-3). Clinical Trial Registration NCT04885361. 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04885361 (accessed on 26 June 2023).
- Belayachi, J.; Obtel, M.; Mhayi, A.; Razine, R.; Abouqal, R. Long term effectiveness of inactivated vaccine BBIBP-CorV (Vero Cells) against COVID-19 associated severe and critical hospitalization in Morocco. PLoS ONE 2022, 17, e0278546.
- Garnett, L.; Tran, K.; Chan, M.; Tierney, K.; Schiffman, Z.; Audet, J.; Lew, J.; Meilleur, C.; Chan, M.; Manguiat, K.; et al. An S1 subunit vaccine and combination adjuvant (COVAC-1) elicits robust protection against SARS-CoV-2 challenge in African green monkeys. bioRxiv 2022, 6.
- Luo, D.; Pan, H.; He, P.; Yang, X.; Li, T.; Ning, N.; Fang, X.; Yu, W.; Wei, M.; Gao, H. A randomized, double-blind, placebo-controlled phase 1 and phase 2 clinical trial to evaluate efficacy and safety of a SARS-CoV-2 vaccine SCoK in adults. Clin. Transl. Med. 2022, 12, e1016.
- Richmond, P.; Hatchuel, L.; Dong, M.; Ma, B.; Hu, B.; Smolenov, I.; Li, P.; Liang, P.; Han, H.H.; Liang, J.; et al. Safety and immunogenicity of S-Trimer (SCB-2019), a protein subunit vaccine candidate for COVID-19 in healthy adults: A phase 1, randomised, double-blind, placebo-controlled trial. Lancet 2021, 397, 682–694.
- A Controlled Phase 2/3 Study of Adjuvanted Recombinant SARS-CoV-2 Trimeric S-protein Vaccine (SCB-2019) for the Prevention of COVID-19. NCT04672395. Available online: www.ClinicalTrials.gov (accessed on 26 June 2023).
- Lopez, P.; Bravo, L.; Buntinx, E.; Borja-Tabora, C.; Velasquez, H.; Rodriguez, E.J.; Rodriguez, C.A.; Carlos, J.; Montellano, M.E.; Alberto, E.R. Safety and immunogenicity of SCB-2019, an adjuvanted, recombinant SARS-CoV-2 trimeric S-protein subunit COVID-19 vaccine in healthy 12–17 year-old adolescents. medRxiv 2023, 2, 23286317.
- Tabarsi, P.; Anjidani, N.; Shahpari, R.; Roshanzamir, K.; Fallah, N.; Andre, G.; Petrovsky, N.; Barati, S. Immunogenicity and safety of SpikoGen®, an adjuvanted recombinant SARS-CoV-2 spike protein vaccine as a homologous and heterologous booster vaccination: A randomized placebo-controlled trial. Immunology 2022, 167, 340–353.
- Tabarsi, P.; Anjidani, N.; Shahpari, R.; Mardani, M.; Sabzvari, A.; Yazdani, B.; Kafi, H.; Fallah, N.; Ebrahimi, A.; Taheri, A.; et al. Evaluating the efficacy and safety of SpikoGen®, an Advax-CpG55. 2–adjuvanted severe acute respiratory syndrome coronavirus 2 spike protein vaccine: A phase 3 randomized placebo-controlled trial. Clin. Microbiol. Infect. 2023, 29, 215–220.
- Mallory, R.M.; Formica, N.; Pfeiffer, S.; Wilkinson, B.; Marcheschi, A.; Albert, G.; McFall, H.; Robinson, M.; Plested, J.S.; Zhu, M.; et al. Safety and immunogenicity following a homologous booster dose of a SARS-CoV-2 recombinant spike protein vaccine (NVX-CoV2373): A secondary analysis of a randomised, placebo-controlled, phase 2 trial. Lancet Infect. Dis. 2022, 22, 1565–1576.
- Medicine UNLo. Evaluation of the Safety and Immunogenicity of a SARS-CoV-2 rS (COVID-19) Nanoparticle Vaccine with/without Matrix-M. Adjuvant. Available online: https://clinicaltrials.gov/ct2/show/NCT04368988 (accessed on 26 June 2023).
More
Information
Subjects:
Pharmacology & Pharmacy
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
755
Revisions:
2 times
(View History)
Update Date:
14 Jul 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No