Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Andrea Gabai | -- | 1207 | 2023-07-12 15:38:09 | | | |
| 2 | Jason Zhu | -1 word(s) | 1206 | 2023-07-13 03:59:12 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Gabai, A.; Zeppieri, M.; Finocchio, L.; Salati, C. Ocular Barriers. Encyclopedia. Available online: https://encyclopedia.pub/entry/46711 (accessed on 23 July 2026).
Gabai A, Zeppieri M, Finocchio L, Salati C. Ocular Barriers. Encyclopedia. Available at: https://encyclopedia.pub/entry/46711. Accessed July 23, 2026.
Gabai, Andrea, Marco Zeppieri, Lucia Finocchio, Carlo Salati. "Ocular Barriers" Encyclopedia, https://encyclopedia.pub/entry/46711 (accessed July 23, 2026).
Gabai, A., Zeppieri, M., Finocchio, L., & Salati, C. (2023, July 12). Ocular Barriers. In Encyclopedia. https://encyclopedia.pub/entry/46711
Gabai, Andrea, et al. "Ocular Barriers." Encyclopedia. Web. 12 July, 2023.
Copy Citation
Innovative and new drug delivery systems (DDSs) have been developed to vehicle treatments and drugs to the ocular posterior segment and the retina. New formulations and technological developments, such as nanotechnology, novel matrices, and non-traditional treatment strategies, open new perspectives in this field.
drug delivery systems (DDSs)
nanotechnology
matrices
ocular posterior segment
1. Introduction
New drug delivery methods to target specific ocular tissues and treat debilitating ocular diseases have been proposed in the past decade. Of all ocular diseases, 55% originate from the posterior segment [1]. Retinal diseases, such as age-related macular degeneration (AMD), diabetic retinopathy (DR), diabetic macular edema (DME), endophthalmitis, viral retinitis, proliferative vitreoretinopathy (PVR), posterior uveitis, retinal vascular occlusions, retinitis pigmentosa (RP), and inherited retinal diseases (IRDs), represent the leading cause of vision impairment [2][3].
The presence of static barriers (different layers of the cornea, sclera, retina, blood–aqueous (BAB) and (BRB) blood–retinal barriers) (Figure 1) and dynamic barriers (conjunctival and choroidal blood flow, tear turnover, and lymphatic clearance) represent an obstacle to the delivery of a drug to a particular ocular tissue and to treating these retinal diseases [4]. The research field based on ocular “drug delivery”, which refers to numerous innovative techniques to target retinal tissue and overcome ocular barriers, has witnessed huge growth in recent years.
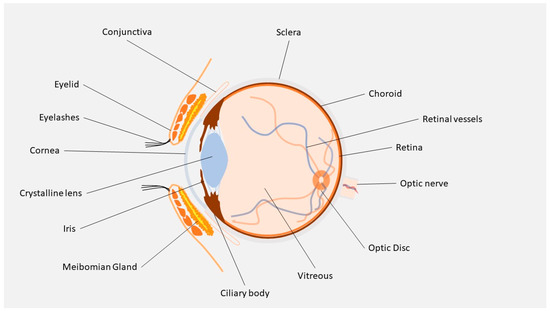
Figure 1. Ocular anatomy.
Depending on disease type, drug property, and target site, drugs can be administered through different routes, including topical, intravitreal, periocular, and systemic. Several types of ophthalmic drug delivery systems (DDSs) are currently available on the market, and range from eyedrops, eye ointments, gels, and ocular inserts, such as eye dosage formulations that are created to increase the holding time of drugs in the eye. Topical drug instillation on the ocular surface is a common and non-invasive application method for the treatment modalities of eye disorders. This route, however, offers suboptimal ocular bioavailability. Studies have shown that 90% of eyedrops available on the market only provide 5% of drug bioavailability, while the rest of the drug gets washed away through different elimination routes, such as tear fluid, nasolacrimal secretion, protein binding, enzymatic degradation, or metabolism by protease and esterase enzyme [5]. Despite the limits of topical treatments, current studies have reported promising results for substances delivered to the retina, which suggests that topical treatment of retinal diseases might be possible in the future [6][7].
Injection into the globe is very often recommended for drug delivery into the posterior region, but it is painful, causes patient non-compliance, has risks of infection, and is associated with various side effects. Over the past decade, thanks to advances in nanotechnology and the development of many drug delivery systems, such as implants, in situ gel, contact lenses, microneedles, liposomes, nanomicelles, dendrimers, and other nanoparticles (NPs), numerous drug-delivery solutions have been proposed. The polymeric nature of these various technologies includes the distinction between microparticles, which are polymeric systems larger than 1 µm, and nanoparticles that have a smaller diameter. Structurally, these particles can be broadly described as micro/nanospheres, when the loaded drug is integrated in the matrix and nano/microcapsules, when the drug is enclosed in a polymeric shell. Although most of the studies in this field are still in the preclinical stages, micro/nanotechnology-based DDSs possess great potential to solve the shortcomings of currently available drug delivery systems. These new strategies can potentially allow safe and effective drug administration to the ocular posterior segment and retina [8][9][10][11].
2. Ocular Barriers
Pharmaceutical formulations via the anterior segment, mostly liquid solutions, or suspensions, are the most common treatment used in ophthalmology. These locally administered drops include a broad range of molecules, such as antibiotics, anti-inflammatory agents, anti-glaucomatous drops, lubricants, and diagnostic agents. Topical formulations tend to be used for the ocular surface and do not allow topical drugs to reach therapeutic concentrations in the posterior ocular segment (vitreous, retina, choroid) due to several anatomical and functional barriers.
2.1. Lacrimal Wash-Out and Mucosal Capillary Circulation
The first and most important factor that decreases topic drop efficacy in the posterior segment is the continuous lacrimal wash-out of the ocular surface. This shortens the contact between eyedrops and the ocular surface so that an instilled volume of topical drug is usually drained via the nasolacrimal duct in approximately 2 min [12]. Capillary vessels, both in the nasal mucosa and conjunctiva, also prevent a portion of the active drug from reaching therapeutic concentration within the eye by dispersing molecules in the systemic blood flow [13].
2.2. Cornea
The epithelium of the cornea is the principal barrier of this multilayered bio-membrane. Epithelial cells are lipophilic, tightly interconnected, organized in a 3 to 6 layer structure, and continuously replaced with newer cells migrating from the limbus to the corneal apex. The intercellular tight junctions limit the paracellular passage of hydrophilic molecules and ions, making the cornea much more permeable to lipophilic drugs, and capable of transcellular passage. The corneal stroma, which is rich in collagen fibrils and glycosaminoglycan, is hydrophilic, thus limiting the absorption rate of lipophilic molecules crossing the epithelium. The endothelium, with its monolayer structure, seems to offer little resistance to lipophilic substances. For these reasons, corneal permeation is currently the preferred way to deliver lipophilic drugs with a small molecular weight in the anterior chamber [14][15].
2.3. Conjunctiva
Studies have reported that the conjunctiva is approximately 20 times more permeable than the cornea, and that allows for the absorption of more hydrophilic and larger molecules, thus offering a potential route of administration for new therapeutic proteins and peptides [16][17][18].
2.4. Sclera
The sclera is composed of collagen fibers embedded in mucopolysaccharides, thus making it more permeable to drugs than the cornea and less than the conjunctiva. It is important to remember that the conjunctiva is the most vascularized and porous structure of the ocular surface [19]. Scleral permeation mostly occurs through passive diffusion, with a permeability coefficient inversely related to the molecular weight of the permeating substances [16][20].
2.5. BAB and BRB
Systemic drug administration provides low ocular bioavailability (<5%) due to the limited fraction of the entire blood reaching the eye and the presence of the BAB and BRB, which render systemic administration effective only for drugs with high therapeutic index, and for treatments given in high doses, such as antibiotics and antiviral agents [13][21].
Non-pigmented ciliary cells and endothelial cells of the irideal vessels are the main elements of the BAB. The tight intersections of this structure render the wall of the capillaries impermeable to the plasma albumin, thus avoiding access to the aqueous humor and limiting the passage of hydrophilic drugs from the systemic circulation to the anterior chamber. The disruption of BAB in inflammatory conditions can allow systemic drugs to freely distribute to the anterior chamber [13].
The blood flow through the choroidal vasculature passively contributes to the clearance of systemic drugs, preventing penetration into the eye. The choroidal vessel walls, however, are rather permeable, so blood and drugs can easily leak through. A more active barrier to penetration is represented by the retinal pigment epithelium (RPE) and Bruch’s membrane, which constitute the outer part of the BRB. Retinal vessel endothelium and intertwining connections also block drug passage from systemic circulation to the retina and vitreous, constituting the inner part of the BRB [13][22][23]. The metabolic, molecular, and pharmacokinetic characteristics of blood–ocular barriers are not completely known; future histological and molecular pathologic studies are needed to better understand the underlying mechanisms involved in these structures.
References
- Edelhauser, H.F.; Rowe-Rendleman, C.L.; Robinson, M.R.; Dawson, D.G.; Chader, G.J.; Grossniklaus, H.E.; Rittenhouse, K.D.; Wilson, C.G.; Weber, D.A.; Kuppermann, B.D.; et al. Ophthalmic Drug Delivery Systems for the Treatment of Retinal Diseases: Basic Research to Clinical Applications. Investig. Opthalmology Vis. Sci. 2010, 51, 5403–5420.
- Thrimawithana, T.R.; Young, S.; Bunt, C.R.; Green, C.; Alany, R.G. Drug delivery to the posterior segment of the eye. Drug Discov. Today 2011, 16, 270–277.
- Bansal, P.; Garg, S.; Sharma, Y.; Venkatesh, P. Posterior Segment Drug Delivery Devices: Current and Novel Therapies in Development. J. Ocul. Pharmacol. Ther. 2016, 32, 135–144.
- Awwad, S.; Ahmed, A.H.M.; Sharma, G.; Heng, J.S.; Khaw, P.T.; Brocchini, S.; Lockwood, A. Principles of pharmacology in the eye. Br. J. Pharmacol. 2017, 174, 4205–4223.
- Gholizadeh, S.; Wang, Z.; Chen, X.; Dana, R.; Annabi, N. Advanced nanodelivery platforms for topical ophthalmic drug delivery. Drug Discov. Today 2021, 26, 1437–1449.
- Löscher, M.; Seiz, C.; Hurst, J.; Schnichels, S. Topical Drug Delivery to the Posterior Segment of the Eye. Pharmaceutics 2022, 14, 134.
- Kang-Mieler, J.J.; Rudeen, K.M.; Liu, W.; Mieler, W.F. Advances in ocular drug delivery systems. Eye 2020, 34, 1371–1379.
- Yadav, D.; Varma, L.T.; Yadav, K. Drug delivery to posterior segment of the eye: Conventional delivery strategies their barriers and restrictions. In Drug Delivery for the Retina and Posterior Segment Disease; Patel, J.K., Sutariya, V., Kanwar, J.R., Pathak, Y.V., Eds.; Springer: Cham, Switzerland, 2018; pp. 51–67.
- Akhter, M.H.; Ahmad, I.; Alshahrani, M.Y.; Al-Harbi, A.I.; Khalilullah, H.; Afzal, O.; Altamimi, A.S.A.; Najib Ullah, S.N.M.; Ojha, A.; Karim, S. Drug Delivery Challenges and Current Progress in Nanocarrier-Based Ocular Therapeutic System. Gels 2022, 8, 82.
- Wang, R.; Gao, Y.; Liu, A.; Zhai, G. A review of nanocarrier-mediated drug delivery systems for posterior segment eye disease: Challenges analysis and recent advances. J. Drug Target. 2021, 29, 687–702.
- Joseph, R.R.; Venkatraman, S.S. Drug delivery to the eye: What benefits do nanocarriers offer? Nanomedicine 2017, 12, 683–702.
- Urtti, A.; Salminen, L. Minimizing systemic absorption of topically administered ophthalmic drugs. Surv. Ophthalmol. 1993, 37, 435–456.
- Urtti, A. Challenges and obstacles of ocular pharmacokinetics and drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1131–1135.
- Maurice, D.M.; Mishima, S. Ocular pharmacokinetics. In Handbook of Experimental Pharmacology; Sears, M.L., Ed.; Springer: Berlin/Heidelberg, Germany, 1984; Volume 69, pp. 16–119.
- Hornof, M.; Toropainen, E.; Urtti, A. Cell culture models of the ocular barriers. Eur. J. Pharm. Biopharm. 2005, 60, 207–225.
- Prausnitz, M.R.; Noonan, J.S. Permeability of cornea, sclera, and conjunctiva: A literature analysis for drug delivery to the eye. J. Pharm. Sci. 1998, 87, 1479–1488.
- Hämäläinen, K.M.; Kontturi, K.; Murtomäki, L.; Auriola, S.; Urtti, A. Estimation of pore size and porosity of biomembranes from permeability measurements of polyethylene glycols using an effusion-like approach. J. Control. Release 1997, 49, 97–104.
- Geroski, D.H.; Edelhauser, H.F. Transscleral drug delivery for posterior segment disease. Adv. Drug Deliv. Rev. 2001, 52, 37–48.
- Hämäläinen, K.M.; Kananen, K.; Auriola, S.; Kontturi, K.; Urtti, A. Characterization of paracellular aqueous penetration routes in cornea conjunctiva sclera. Investig. Ophthalmol. Vis. Sci. 1997, 38, 627–634.
- Raghava, S.; Hammond, M.; Kompella, U.B. Periocular routes for retinal drug delivery. Exp. Opin. Drug Deliv. 2004, 1, 99–114.
- Loftsson, T.; Sigurdsson, H.H.; Konrádsdóttir, F.; Gísladóttir, S.; Jansook, P.; Stefánsson, E. Topical drug delivery to the posterior segment of the eye: Anatomical and physiological considerations. Pharmazie 2008, 63, 171–179.
- Tawfik, M.; Chen, F.; Goldberg, J.L.; Sabel, B.A. Nanomedicine and drug delivery to the retina: Current status and implications for gene therapy. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2022, 395, 1477–1507.
- Cunha-Vaz, J.G. The blood-retinal barriers. Doc. Ophthalmol. 1976, 41, 287–327.
More
Information
Subjects:
Ophthalmology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.1K
Revisions:
2 times
(View History)
Update Date:
13 Jul 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No