Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Marta Cvijić | -- | 1812 | 2023-06-26 19:09:50 | | | |
| 2 | Fanny Huang | Meta information modification | 1812 | 2023-06-28 08:55:20 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Škafar, M.; Ambrožič, J.; Toplišek, J.; Cvijić, M. Role of Exercise Stress Echocardiography in Pulmonary Hypertension. Encyclopedia. Available online: https://encyclopedia.pub/entry/46076 (accessed on 25 July 2026).
Škafar M, Ambrožič J, Toplišek J, Cvijić M. Role of Exercise Stress Echocardiography in Pulmonary Hypertension. Encyclopedia. Available at: https://encyclopedia.pub/entry/46076. Accessed July 25, 2026.
Škafar, Mojca, Jana Ambrožič, Janez Toplišek, Marta Cvijić. "Role of Exercise Stress Echocardiography in Pulmonary Hypertension" Encyclopedia, https://encyclopedia.pub/entry/46076 (accessed July 25, 2026).
Škafar, M., Ambrožič, J., Toplišek, J., & Cvijić, M. (2023, June 26). Role of Exercise Stress Echocardiography in Pulmonary Hypertension. In Encyclopedia. https://encyclopedia.pub/entry/46076
Škafar, Mojca, et al. "Role of Exercise Stress Echocardiography in Pulmonary Hypertension." Encyclopedia. Web. 26 June, 2023.
Copy Citation
Pulmonary hypertension (PH) is a pathophysiological disorder that may involve various clinical conditions and may be associated with numerous respiratory and/or cardiovascular diseases. Exercise echocardiography can unmask exercise PH, detect the early stages of left ventricular diastolic dysfunction, and, therefore, differentiate between pre- and post-capillary PH. Regardless of the underlying aetiology, a developed PH is associated with increased mortality. Parameters of overt right ventricle (RV) dysfunction, including RV dilation, reduced RV ejection fraction, and elevated right-sided filling pressures, are detectable with resting echocardiography and are associated with worse outcome.
pulmonary hypertension
exercise stress echocardiography
pulmonary arterial pressure
1. Diagnostic Role
In patients with exertional dyspnoea and suspected PH due to HFpEF, there is a possibility to unmask early stages of LV diastolic dysfunction to detect increased LV filling pressures during exercise and, therefore, to differentiate between pre- and post-capillary PH.
As in resting echocardiography, the increase in the E/e′ ratio during exercise is suggestive of elevated LV filling pressures. However, studies comparing haemodynamic data acquired by echocardiography and by RHC during exercise are limited [1][2]. Even though the E/e′ ratio during exercise had only a moderate correlation with directly invasively measured PAWP (r = 0.57; p < 0.001), adding the peak exercise E/e′ ratio to the ESC proposed algorithm of diastolic dysfunction improved sensitivity (up to 90%) and can be used to rule out post-capillary PH [3]. Using low-level exercise (20 W) seems to be a good alternative, as E/e′ at 20 W could reliably predict normal PAWP during exercise (AUC: 0.77; p < 0.01) [4]. The authors proposed a cut-off of 12.4 for E/e′ at 20 W (specificity 83%, sensitivity 75%). However, these studies comprised only healthy controls and patients with HFpEF. There is only one study that tested the echocardiographic mPAP/CO ratio to identify patients with abnormal pulmonary vascular response to exercise [5]. In a study group of healthy subjects and mainly patients with chronic thromboembolic pulmonary hypertension, mPAP/CO via exercise stress echocardiography of 3.2 mmHg/L/min was identified as the most favourable threshold. Of note, this cut-off is perfectly in line with the proposed cut-off obtained by RHC.
In spite of the above-mentioned data, the diagnostic value of the stress tests during echocardiography to distinguish between PH subtypes is currently uncertain due to the lack of prospective data, especially regarding its use to identify cases of combined post- and pre-capillary PH. Based on the data from the literature, exercise echocardiography is considered abnormal if the average E/e′ ratio at peak stress increases to ≥15, with or without a peak TR velocity >3.4 m/s (Figure 1) [3][6][7]. An increase in TR velocity only should not be used to diagnose post-capillary PH because it might be a normal hyperdynamic response to exercise with increased pulmonary blood flow in the absence of LV diastolic dysfunction [8].
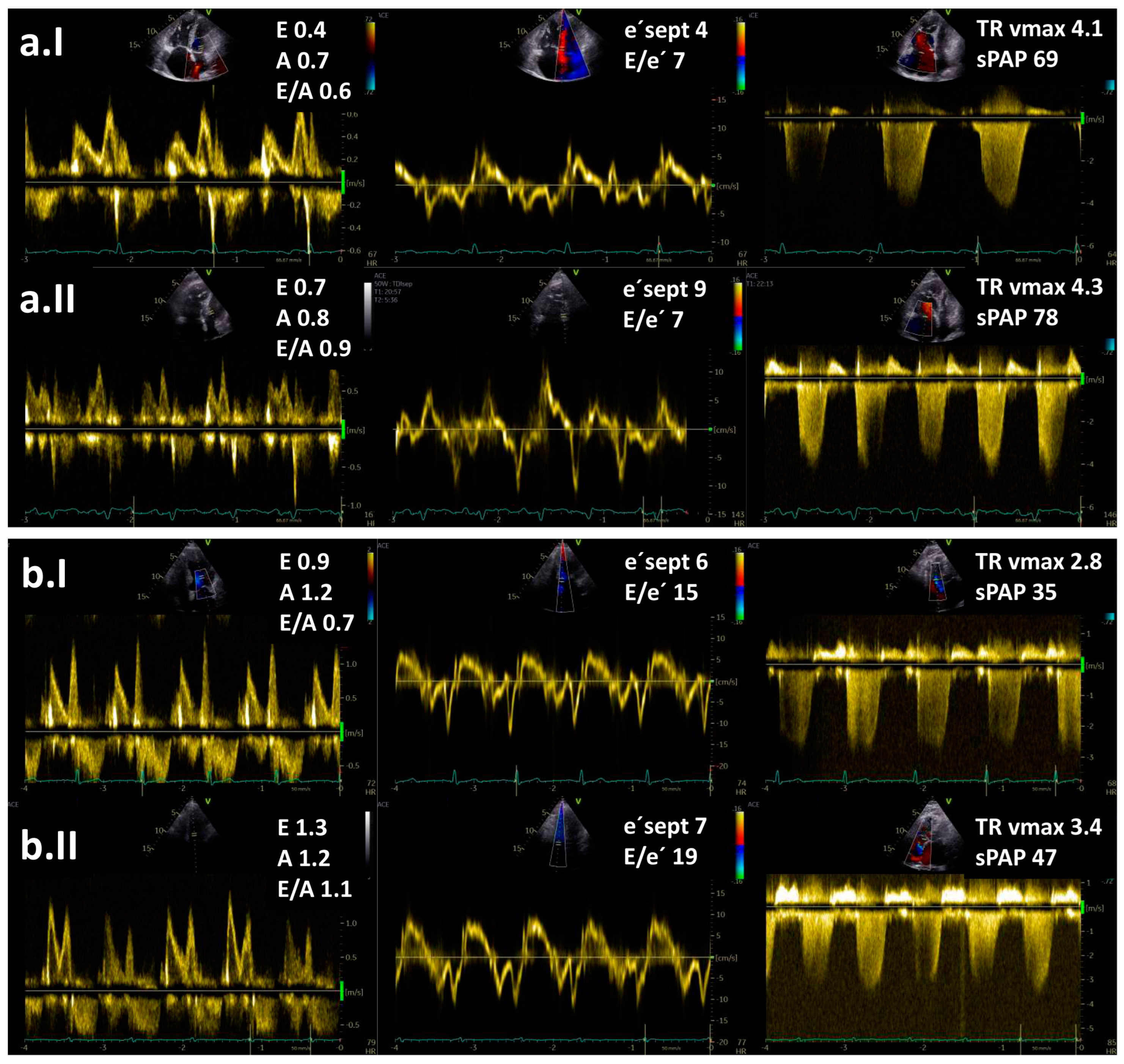
Figure 1. Resting (I) and exercise stress echocardiography (II) in two patients with pulmonary hypertension (PH): (a) a patient with pre-capillary PH and (b) a patient with post-capillary PH. Maximal tricuspid regurgitation velocity (TR vmax) is elevated in both patients. Note an increase in E/e′ ratio at low-level exercise from 15 to 19 in a patient with post-capillary PH but no increase in a patient with pre-capillary PH. Legend: sPAP—systolic pulmonary arterial pressure.
Exercise stress echocardiography could be extremely useful as an effective gatekeeper to the RHC for patients with exertional dyspnoea of unknown aetiology and normal resting echocardiographic results and also for identifying patients with a high risk for developing PH. It has been demonstrated that exercise stress echocardiography can distinguish between noncardiac and cardiac causes of unexplained dyspnoea [3][9]. The diagnostic value of exercise stress echocardiography was also evaluated in asymptomatic relatives of patients with idiopathic and familial PAH [10]. Hypertensive response to exercise, defined by TR velocity > 3.1 m/s, was more often present in relatives of PAH patients than in control subjects. Additionally, exercise stress echocardiography is considered to be reasonable, especially in patients with connective tissue disease [11]. It has been reported that up to 50% of this patient population with normal resting mPAP had an abnormal increase in mPAP during exercise. In patients with systemic sclerosis, PH was confirmed by RHC in 81% of patients with positive exercise stress echocardiography [12]. Moreover, exercise stress echocardiography could unmask exercise PH in patients with systemic sclerosis and baseline echocardiographic PAP within the grey zone [13]. It is important to note that in both studies, authors used a definition of exercise PH, which is not in line with nowadays valid definition (an increase of 20 mmHg over the resting sPAP or sPAP > 50 mmHg was considered as a positive test result). However, the clinical value of exercise PH identified by exercise stress echocardiography remains uncertain because of the lack of validated criteria and prospective confirmatory data [14]. Therefore, data from exercise stress echocardiography are not sufficient to be a substitute for invasive haemodynamic data under all circumstances, especially if a therapeutic decision depends on the results [15].
2. Prognostic Role
Regardless of the underlying aetiology, the developed PH is associated with worsening symptoms and substantially increased mortality [16]. Even though the detection of exercise PH via exercise stress echocardiography is considered an early and mild phase of PAH [17], patients with exercise PH already had worse outcomes than subjects without exercise PH [18].
The survival of PH patients depends on the capability of the RV to adapt to chronically elevated PAP [19]. Over time, adaptive concentric RV hypertrophy with preserved RV function can evolve into RV dilatation and systolic dysfunction [20][21]. RV function is a major determinant of functional capacity and prognosis when RV afterload is elevated [22][23][24]. Echocardiographic measures of RV function that are independent predictors of mortality in PH include the tricuspid annular plane systolic excursion (TAPSE < 18 mm [25][26][27]), RV fractional area change (FAC < 35% [28][29]), peak systolic tricuspid lateral annular velocity (S’ < 9.7 cm/s [30]) and Tei index (>0.40 by pulse Doppler or >0.55 by tissue Doppler [31]). Conventional 2-dimensional echocardiographic evaluation of the RV is difficult due to the complex 3-dimensional (3D) anatomical shape of the RV. This limitation can be overcome with 3D echocardiography and/or cardiac magnetic resonance [32][33] and recently, an increased 3D RVESVi has been shown to correlate with increased mortality [34].
However, these parameters all fail to identify occult RV dysfunction in patients with PH [35] as they reflect already established RV dysfunction. Subtle RV dysfunction could possibly be recognised by the use of advanced echocardiographic techniques, such as strain/myocardial deformation and myocardial work [36][37][38]. Previous studies demonstrated that RV longitudinal strain was a powerful predictor of survival in patients with PH and provided incremental prognostic value over conventional clinical and echocardiographic variables [39][40].
Additionally, the assessment of RV contractile reserve via RV–pulmonary arterial (PA) coupling shows promising results in detecting subclinical RV systolic dysfunction [35][41][42][43][44][45]. Gold standard measurement of RV–PA coupling involves conductance catheter measurement of “multi-beat” RV end-systolic elastance (Ees), a method that remains costly, impractical and clinically challenging [41]. However, new echocardiographic indices, such as the TAPSE/sPAP ratio [24][46][47][48] and RV free wall longitudinal strain/sPAP [38], are tightly linked to RV–PA coupling and are associated with outcomes in patients with PH.
A possible non-invasive measure of the RV contractile reserve using exercise stress echocardiography was first proposed by Grünig et al. They demonstrated that an exercise-induced increase in sPAP was a measure of the RV contractile reserve and was an independent prognostic factor in patients with pre-capillary PH [49]. A lower sPAP increase may reveal an impaired ability of the RV to adapt to pulmonary load and exercise and to further increase pressure and pulmonary blood flow. Similarly, an initial steep increment in PAP during exercise followed by a plateau with a linear pattern was associated with decreased exercise capacity and survival in patients with heart failure [50]. Echocardiographic studies focused only on the peak exercise sPAP or the peak change in sPAP [49][50]; however, it would be preferable to interpret exercise PAP pattern relative to the increase in blood flow (PAP/CO ratio). Invasively obtained haemodynamic data clearly showed that high mPAP/CO during exercise was associated with impaired survival in a heterogeneous group of different PH phenotypes [51][52]. Echocardiographic studies analysing mPAP/CO are limited, but initial results are very promising. A disproportionate increase in mPAP/CO slope during exercise was independently associated with adverse clinical outcomes in patients with HFpEF (Table 1) [53], and this parameter had an incremental value even in patients with preserved RV-PA coupling at rest.
Other authors assessed RV contractile reserve based on echocardiographic parameters of RV systolic function (e.g., change in TAPSE, change in RV FAC and change in S’) (Table 1) [54][55]. The magnitude of the increase in all three parameters was significantly lower in patients with pre-capillary PH than in healthy controls [54][55]; however, no prognostic data have been available for these parameters. Ireland et al. prospectively studied RV contractile reserve in PH patients who underwent cardiac magnetic resonance, echocardiography, and supine invasive cardiopulmonary exercise testing with concomitant RV pressure-volume catheterisation. RV contractile reserve during exercise, measured by Ees during exertion, was associated with an elevation in PAP but the preservation of RV volumes. The lack of RV reserve, on the other hand, was tightly coupled with acute RV dilation during exercise [41]. RV ejection fraction during exercise was shown to be a robust surrogate for RV contractile reserve (Table 1), and it best predicted occult RV dysfunction among a variety of resting and exercise RV measures and was also associated with clinical worsening [41]. Therefore, echocardiographic parameters of RV contractile reserve and exercise stress echocardiography could be useful for follow-up assessment, especially to identify PH patients at high risk [49].
Table 1. Non-invasive measures of the right ventricle (RV) contractile reserve during exercise stress echocardiography.
| Author | Subjects (n) | Echocardiographic Parameters | Most Relevant Findings |
|---|---|---|---|
| Grünig, 2013 [49] | 124 PH patients (PAH, CTEPH) and impaired RV systolic function | ∆sPAP | Exercise-induced sPAP increase ≤ 30 mmHg was related to the worst outcome (HR 2.84, 95% CI 1.92–6.78; p = 0.018). |
| Almeida, 2014 [55] | 14 subjects (7 controls, 7 patients with PH) | ∆S’, ∆TAPSE and ∆FAC | The magnitude of increase in ∆S’, ∆TAPSE and ∆FAC in healthy controls was higher than in patients (all p < 0.05. |
| Guo, 2019 [54] | 46 subjects (31 patients with pre-capillary PH, 15 controls) | ∆S’, ∆TAPSE and ∆FAC | Significant increase in ∆S’ (p = 0.002), ∆TAPSE (p < 0.001) and ∆FAC (p < 0.001) was noted only in healthy controls. |
| Ireland, 2021 [41] | 35 subjects with known or suspected PH | Exercise RVEF | Exercise RVEF can detect occult RV dysfunction (AUC = 0.81, cut off of exercise RVEF = 38%). Patients with exercise RVEF < 38% had an increased propensity for clinical worsening over 4 years compared to patients with RVEF > 38% (p = 0.014). |
| Saito, 2023 [53] | 345 patients (1666 HFpEF, 179 controls) | mPAP/CO slope | Patients with mPAP/CO slope > 5.2 mmHg/L/min had a higher rate of adverse events (all-cause mortality, HF events) compared to those with mPAP/CO slope < 5.2 mmHg/L/min (p = 0.0002). |
Legend: CO—cardiac output, CTEPH—chronic thromboembolic pulmonary hypertension, FAC—fractional area change, HFpEF—heart failure with preserved ejection fraction, mPAP—mean pulmonary arterial pressure, PAH—pulmonary arterial hypertension, PH—pulmonary hypertension, RVEF—right ventricular ejection fraction, sPAP—systolic pulmonary arterial pressure, S’ -Doppler-derived tricuspid lateral annular peak systolic velocity, and TAPSE—tricuspid annular plane systolic excursion.
References
- Kovacs, G.; Herve, P.; Barbera, J.A.; Chaouat, A.; Chemla, D.; Condliffe, R.; Garcia, G.; Grünig, E.; Howard, L.; Humbert, M.; et al. An official European Respiratory Society statement: Pulmonary haemodynamics during exercise. Eur. Respir. J. 2017, 50, 1700578.
- Ha, J.W.; Andersen, O.S.; Smiseth, O.A. Diastolic Stress Test: Invasive and Noninvasive Testing. JACC Cardiovasc. Imaging 2020, 13, 272–282.
- Obokata, M.; Kane, G.C.; Reddy, Y.N.V.; Olson, T.P.; Melenovsky, V.; Borlaug, B.A. Role of Diastolic Stress Testing in the Evaluation for Heart Failure with Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study. Circulation 2017, 135, 825–838.
- Effects of a dynamic handgrip exercise on left ventricular diastolic functions in diabetes mellitus patients: A preliminary clinical data Utility of E/e′ Ratio During Low-Level Exercise to Diagnose Heart Failure With Preserved. JACC Cardiovasc. Imaging 2023, 16, 145–155.
- Claessen, G.; La Gerche, A.; Voigt, J.-U.; Dymarkowski, S.; Schnell, F.; Petit, T.; Willems, R.; Claus, P.; Delcroix, M.; Heidbuchel, H. Accuracy of Echocardiography to Evaluate Pulmonary Vascular and RV Function During Exercise. JACC Cardiovasc. Imaging 2016, 9, 532–543.
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314.
- Lancellotti, P.; Pellikka, P.A.; Budts, W.; Chaudhry, F.A.; Donal, E.; Dulgheru, R.; Edvardsen, T.; Garbi, M.; Ha, J.-W.; Kane, G.C.; et al. The clinical use of stress echocardiography in non-ischaemic heart disease: Recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1191–1229.
- Nagueh, S.F.; Chang, S.M.; Nabi, F.; Shah, D.J.; Estep, J.D. Cardiac imaging in patients with heart failure and preserved ejection fraction. Circ Cardiovasc. Imaging 2017, 10, e006547.
- Talreja, D.R.; Nishimura, R.A.; Oh, J.K. Estimation of Left Ventricular Filling Pressure with Exercise by Doppler Echocardiography in Patients with Normal Systolic Function: A Simultaneous Echocardiographic-Cardiac Catheterization Study. J. Am. Soc. Echocardiogr. 2007, 20, 477–479.
- Grünig, E.; Weissmann, S.; Ehlken, N.; Fijalkowska, A.; Fischer, C.; Fourme, T.; Galié, N.; Ghofrani, A.; Harrison, R.E.; Huez, S.; et al. Stress doppler echocardiography in relatives of patients with idiopathic and familial pulmonary arterial hypertension results of a multicenter european analysis of pulmonary artery pressure response to exercise and hypoxia. Circulation 2009, 119, 1747–1757.
- Shaikh, F.; Anklesaria, Z.; Shagroni, T.; Saggar, R.; Gargani, L.; Bossone, E.; Ryan, M.; Channick, R.; Saggar, R. A review of exercise pulmonary hypertension in systemic sclerosis. J. Scleroderma Relat. Disord. 2019, 4, 225–237.
- Steen, V.; Chou, M.; Shanmugam, V.; Mathias, M.; Kuru, T.; Morrissey, R. Exercise-induced pulmonary arterial hypertension in patients with systemic sclerosis. Chest 2008, 134, 146–151.
- Rallidis, L.S.; Papangelopoulou, K.; Anthi, A.; Tsangaris, I.; Varounis, C.; Makavos, G.; Konstantonis, D.; Vlachoyiannopoulos, P.; Orfanos, S.E.; Iliodromitis, E.K. The role of exercise doppler echocardiography to unmask pulmonary arterial hypertension in selected patients with systemic sclerosis and equivocal baseline echocardiographic values for pulmonary hypertension. Diagnostics 2021, 11, 1200.
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022, 43, 3618–3731.
- Pieske, B.; Tschöpe, C.; de Boer, A.R.; Fraser, A.G.; Anker, S.D.; Donal, E.; Edelmann, F.; Fu, M.; Guazzi, M.; Lam, C.S.P.; et al. How to diagnose heart failure with preserved ejection fraction: The HFA-PEFF diagnostic algorithm: A consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Heart J. 2019, 40, 3297–3317.
- Hoeper, M.M.; Humbert, M.; Souza, R.; Idrees, M.; Kawut, S.M.; Sliwa-Hahnle, K.; Jing, Z.-C.; Gibbs, J.S.R. A global view of pulmonary hypertension. Lancet Respir. Med. 2016, 4, 306–322.
- Tolle, J.J.; Waxman, A.B.; Van Horn, T.L.; Pappagianopoulos, P.P.; Systrom, D.M. Exercise-induced pulmonary arterial hypertension. Circulation 2008, 118, 2183–2189.
- Shim, C.Y.; Kim, S.-A.; Choi, D.; Yang, W.-I.; Kim, J.-M.; Moon, S.-H.; Lee, H.-J.; Park, S.; Choi, E.-Y.; Chung, N.; et al. Clinical outcomes of exercise-induced pulmonary hypertension in subjects with preserved left ventricular ejection fraction: Implication of an increase in left ventricular filling pressure during exercise. Heart 2011, 97, 1417–1424.
- Ghio, S.; Klersy, C.; Magrini, G.; D’Armini, A.M.; Scelsi, L.; Raineri, C.; Pasotti, M.; Serio, A.; Campana, C.; Viganò, M. Prognostic relevance of the echocardiographic assessment of right ventricular function in patients with idiopathic pulmonary arterial hypertension. Int. J. Cardiol. 2010, 140, 272–278.
- Vonk-Noordegraaf, A.; Haddad, F.; Chin, K.M.; Forfia, P.R.; Kawut, S.M.; Lumens, J.; Naeije, R.; Newman, J.; Oudiz, R.J.; Provencher, S.; et al. Right Heart Adaptation to Pulmonary Arterial Hypertension. J Am Coll Cardiol. 2013, 62, D22–D33.
- Vonk Noordegraaf, A.; Westerhof, B.E.; Westerhof, N. The Relationship Between the Right Ventricle and its Load in Pulmonary Hypertension. J. Am. Coll Cardiol. 2017, 69, 236–243.
- Writing Committee Members; McLaughlin, V.V.; Archer, S.L.; Badesch, D.B.; Barst, R.J.; Farber, H.W.; Lindner, J.R.; Mathier, M.A.; McGoon, M.D.; Park, M.H.; et al. A report of the american college of cardiology foundation task force on expert consensus documents and the american heart association. Circulation 2009, 119, 2250–2294.
- D’Alonzo, G.E. Survival in Patients with Primary Pulmonary Hypertension. Ann. Intern. Med. 1991, 115, 343–349.
- Tello, K.; Dalmer, A.; Axmann, J.; Vanderpool, R.; Ghofrani, H.A.; Naeije, R.; Roller, F.; Seeger, W.; Sommer, N.; Wilhelm, J.; et al. Reserve of Right Ventricular-Arterial Coupling in the Setting of Chronic Overload. Circ. Heart Fail. 2019, 12, e005512.
- Forfia, P.R.; Fisher, M.R.; Mathai, S.C.; Housten-Harris, T.; Hemnes, A.R.; Borlaug, B.A.; Chamera, E.; Corretti, M.C.; Champion, H.C.; Abraham, T.P.; et al. Tricuspid Annular Displacement Predicts Survival in Pulmonary Hypertension. Am. J. Respir. Crit. Care Med. 2006, 174, 1034–1041.
- Burke, M.A.; Katz, D.H.; Beussink, L.; Selvaraj, S.; Gupta, D.K.; Fox, J.; Chakrabarti, S.; Sauer, A.J.; Rich, J.D.; Freed, B.H.; et al. Prognostic Importance of Pathophysiologic Markers in Patients With Heart Failure and Preserved Ejection Fraction. Circ. Heart Fail. 2014, 7, 288–299.
- Mohammed, S.F.; Hussain, I.; AbouEzzeddine, O.F.; Takahama, H.; Kwon, S.H.; Forfia, P.; Roger, V.L.; Redfield, M.M. Right Ventricular Function in Heart Failure With Preserved Ejection Fraction. Circulation 2014, 130, 2310–2320.
- Mauritz, G.-J.; Kind, T.; Marcus, J.T.; Bogaard, H.-J.; van de Veerdonk, M.; Postmus, P.E.; Boonstra, A.; Westerhof, N.; Vonk-Noordegraaf, A. Progressive Changes in Right Ventricular Geometric Shortening and Long-term Survival in Pulmonary Arterial Hypertension. Chest 2012, 141, 935–943.
- Melenovsky, V.; Hwang, S.J.; Lin, G.; Redfield, M.M.; Borlaug, B.A. Right heart dysfunction in heart failure with preserved ejection fraction. Eur. Heart J. 2014, 35, 3452–3462.
- Champion, H.C.; Michelakis, E.D.; Hassoun, P.M. Comprehensive Invasive and Noninvasive Approach to the Right Ventricle–Pulmonary Circulation Unit. Circulation 2009, 120, 992–1007.
- Yeo, T.C.; Dujardin, K.S.; Tei, C.; Mahoney, D.W.; McGoon, M.D.; Seward, J.B. Value of a Doppler-Derived Index Combining Systolic and Diastolic Time Intervals in Predicting Outcome in Primary Pulmonary Hypertension. Am. J. Cardiol. 1998, 81, 1157–1161.
- Sanz, J.; Conroy, J.; Narula, J. Imaging of the Right Ventricle. Cardiol Clin. 2012, 30, 189–203.
- Addetia, K.; Bhave, N.M.; Tabit, C.E.; Gomberg-Maitland, M.; Freed, B.H.; Dill, K.E.; Lang, R.M.; Mor-Avi, V.; Patel, A.R. Sample Size and Cost Analysis for Pulmonary Arterial Hypertension Drug Trials Using Various Imaging Modalities to Assess Right Ventricular Size and Function End Points. Circ. Cardiovasc. Imaging 2014, 7, 115–124.
- Ryo, K.; Goda, A.; Onishi, T.; Delgado-Montero, A.; Tayal, B.; Champion, H.C.; Simon, M.A.; Mathier, M.A.; Gladwin, M.T.; Gorcsan, J., 3rd. Characterization of Right Ventricular Remodeling in Pulmonary Hypertension Associated With Patient Outcomes by 3-Dimensional Wall Motion Tracking Echocardiography. Circ. Cardiovasc. Imaging 2015, 8, e003176.
- Richter, M.J.; Peters, D.; Ghofrani, H.A.; Naeije, R.; Roller, F.; Sommer, N.; Gall, H.; Grimminger, F.; Seeger, W.; Tello, K. Evaluation and prognostic relevance of right ventricular-arterial coupling in pulmonary hypertension. Am. J. Respir. Crit. Care Med. 2020, 201, 116–119.
- Carluccio, E.; Biagioli, P.; Alunni, G.; Murrone, A.; Zuchi, C.; Coiro, S.; Riccini, C.; Mengoni, A.; D’antonio, A.; Ambrosio, G. Prognostic value of right ventricular dysfunction in heart failure with reduced ejection fraction: Superiority of longitudinal strain over tricuspid annular plane systolic excursion. Circ. Cardiovasc. Imaging 2018, 11, e006894.
- Butcher, S.C.; Fortuni, F.; Montero-Cabezas, J.M.; Abou, R.; El Mahdiui, M.; Van Der Bijl, P.; Van Der Velde, E.T.; Marsan, N.A.; Bax, J.J.; Delgado, V. Right ventricular myocardial work: Proof-of-concept for non-invasive assessment of right ventricular function. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 142–152.
- Ünlü, S.; Bézy, S.; Cvijic, M.; Duchenne, J.; Delcroix, M.; Voigt, J.-U. Right ventricular strain related to pulmonary artery pressure predicts clinical outcome in patients with pulmonary arterial hypertension. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 635–642.
- Haeck, M.L.; Scherptong, R.W.; Marsan, N.A.; Holman, E.R.; Schalij, M.J.; Bax, J.J.; Vliegen, H.W.; Delgado, V. Prognostic Value of Right Ventricular Longitudinal Peak Systolic Strain in Patients With Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2012, 5, 628–636.
- Fine, N.M.; Chen, L.; Bastiansen, P.M.; Frantz, R.P.; Pellikka, P.A.; Oh, J.K.; Kane, G.C. Outcome Prediction by Quantitative Right Ventricular Function Assessment in 575 Subjects Evaluated for Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2013, 6, 711–721.
- Ireland, C.G.; Damico, R.L.; Kolb, T.M.; Mathai, S.C.; Mukherjee, M.; Zimmerman, S.L.; Shah, A.A.; Wigley, F.M.; Houston, B.A.; Hassoun, P.M.; et al. Exercise right ventricular ejection fraction predicts right ventricular contractile reserve. J. Heart Lung. Transplant. 2021, 40, 504–512.
- Hsu, S.; Houston, B.A.; Tampakakis, E.; Bacher, A.C.; Rhodes, P.S.; Mathai, S.C.; Damico, R.L.; Kolb, T.M.; Hummers, L.K.; Shah, A.A.; et al. Right ventricular functional reserve in pulmonary arterial hypertension. Circulation 2016, 133, 2413–2422.
- Hsu, S.; Kokkonen-Simon, K.M.; Kirk, J.A.; Kolb, T.M.; Damico, R.L.; Mathai, S.C.; Mukherjee, M.; Shah, A.A.; Wigley, F.M.; Margulies, K.B.; et al. Right ventricular myofilament functional differences in humans with systemic sclerosis-associated versus idiopathic pulmonary arterial hypertension. Circulation 2018, 137, 2360–2370.
- Tedford, R.J.; Mudd, J.O.; Girgis, R.E.; Mathai, S.C.; Zaiman, A.L.; Housten-Harris, T.; Boyce, D.; Kelemen, B.W.; Bacher, A.C.; Shah, A.A.; et al. Right ventricular dysfunction in systemic sclerosis-associated pulmonary arterial hypertension. Circ. Heart Fail. 2013, 6, 953–963.
- Rommel, K.-P.; von Roeder, M.; Oberueck, C.; Latuscynski, K.; Besler, C.; Blazek, S.; Stiermaier, T.; Fengler, K.; Adams, V.; Sandri, M.; et al. Load-independent systolic and diastolic right ventricular function in heart failure with preserved ejection fraction as assessed by resting and handgrip exercise pressure–volume loops. Circ. Heart Fail. 2018, 11, e004121.
- Guazzi, M.; Dixon, D.; Labate, V.; Beussink-Nelson, L.; Bandera, F.; Cuttica, M.J.; Shah, S.J. RV Contractile Function and its Coupling to Pulmonary Circulation in Heart Failure With Preserved Ejection Fraction. JACC Cardiovasc. Imaging 2017, 10, 1211–1221.
- Tello, K.; Axmann, J.; Ghofrani, H.A.; Naeije, R.; Narcin, N.; Rieth, A.; Seeger, W.; Gall, H.; Richter, M.J. Relevance of the TAPSE/PASP ratio in pulmonary arterial hypertension. Int. J. Cardiol. 2018, 266, 229–235.
- Huston, J.H.; Maron, B.A.; French, J.; Huang, S.; Thayer, T.; Farber-Eger, E.H.; Wells, Q.S.; Choudhary, G.; Hemnes, A.R.; Brittain, E.L. Association of Mild Echocardiographic Pulmonary Hypertension With Mortality and Right Ventricular Function. JAMA Cardiol. 2019, 4, 1112–1121.
- Grünig, E.; Tiede, H.; Enyimayew, E.O.; Ehlken, N.; Seyfarth, H.-J.; Bossone, E.; D’andrea, A.; Naeije, R.; Olschewski, H.; Ulrich, S.; et al. Assessment and prognostic relevance of right ventricular contractile reserve in patients with severe pulmonary hypertension. Circulation 2013, 128, 2005–2015.
- Lewis, G.D.; Murphy, R.M.; Shah, R.V.; Pappagianopoulos, P.P.; Malhotra, R.; Bloch, K.D.; Systrom, D.M.; Semigran, M.J. Pulmonary vascular response patterns during exercise in left ventricular systolic dysfunction predict exercise capacity and outcomes. Circ. Heart Fail. 2011, 4, 276–285.
- Zeder, K.; Banfi, C.; Steinrisser-Allex, G.; Maron, B.A.; Humbert, M.; Lewis, G.D.; Berghold, A.; Olschewski, H.; Kovacs, G. Diagnostic, prognostic and differential-diagnostic relevance of pulmonary haemodynamic parameters during exercise: A systematic review. Eur. Respir. J. 2022, 60, 2103181.
- Ho, J.E.; Zern, E.K.; Lau, E.S.; Wooster, L.; Bailey, C.S.; Cunningham, T.; Eisman, A.S.; Hardin, K.M.; Farrell, R.; Sbarbaro, J.A.; et al. Exercise Pulmonary Hypertension Predicts Clinical Outcomes in Patients With Dyspnea on Effort. J. Am. Coll. Cardiol. 2020, 75, 17–26.
- Saito, Y.; Obokata, M.; Harada, T.; Kagami, K.; Sorimachi, H.; Yuasa, N.; Kato, T.; Wada, N.; Okumura, Y.; Ishii, H. Disproportionate exercise-induced pulmonary hypertension in relation to cardiac output in heart failure with preserved ejection fraction: A non-invasive echocardiographic study. Eur. J. Heart Fail. 2023, Online ahead of print.
- Guo, D.-C.; Li, Y.-D.; Yang, Y.-H.; Zhu, W.-W.; Sun, L.-L.; Jiang, W.; Ye, X.; Cai, Q.-Z.; Lu, X.-Z.; Ye, X.-G. Influence of impaired right ventricular contractile reserve on exercise capacity in patients with precapillary pulmonary hypertension: A study with exercise stress echocardiography. Echocardiography 2019, 36, 671–677.
- Almeida, A.R.; Loureiro, M.J.; Lopes, L.; Cotrim, C.; Lopes, L.; Repolho, D.; Pereira, H. Echocardiographic assessment of right ventricular contractile reserve in patients with pulmonary hypertension. Rev. Port. Cardiol. 2014, 33, 155–163.
More
Information
Subjects:
Cardiac & Cardiovascular Systems
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
591
Revisions:
2 times
(View History)
Update Date:
28 Jun 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No