Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Matteo Pellegrini | -- | 1823 | 2023-05-24 20:13:27 | | | |
| 2 | Sirius Huang | -10 word(s) | 1813 | 2023-05-26 09:25:45 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Scribante, A.; Ghizzoni, M.; Pellegrini, M.; Pulicari, F.; Manfredini, M.; Poli, P.P.; Maiorana, C.; Spadari, F. Full-Digital Customized Meshes in Guided Bone Regeneration. Encyclopedia. Available online: https://encyclopedia.pub/entry/44796 (accessed on 25 June 2026).
Scribante A, Ghizzoni M, Pellegrini M, Pulicari F, Manfredini M, Poli PP, et al. Full-Digital Customized Meshes in Guided Bone Regeneration. Encyclopedia. Available at: https://encyclopedia.pub/entry/44796. Accessed June 25, 2026.
Scribante, Andrea, Martina Ghizzoni, Matteo Pellegrini, Federica Pulicari, Mattia Manfredini, Pier Paolo Poli, Carlo Maiorana, Francesco Spadari. "Full-Digital Customized Meshes in Guided Bone Regeneration" Encyclopedia, https://encyclopedia.pub/entry/44796 (accessed June 25, 2026).
Scribante, A., Ghizzoni, M., Pellegrini, M., Pulicari, F., Manfredini, M., Poli, P.P., Maiorana, C., & Spadari, F. (2023, May 24). Full-Digital Customized Meshes in Guided Bone Regeneration. In Encyclopedia. https://encyclopedia.pub/entry/44796
Scribante, Andrea, et al. "Full-Digital Customized Meshes in Guided Bone Regeneration." Encyclopedia. Web. 24 May, 2023.
Copy Citation
Meshes, especially titanium ones, are being widely applied in oral surgery. In guided bone regeneration (GBR) procedures, their use is often paired with membranes, being resorbable or non-resorbable. However, they present some limitations, such as difficulty in the treatment of severe bone defects, alongside frequent mesh exposure. Customized meshes, produced by a full-digital process, have been recently introduced in GBR procedures. The main findings in recent years of clinical trials regarding patient-specific mesh produced by CAD/CAM and 3D printing workflow, made in titanium or even PEEK, applied to GBR surgeries, are described. The purpose is to analyze their clinical management, advantages, and complications.
CAD/CAM
customized mesh
dentistry
digital workflow
GBR
guided bone regeneration
oral surgery
PEEK
titanium mesh
3D printing
1. Introduction
The alveolar bone undergoes two successive processes after extraction or loss of a dental element: resorption and atrophy. This leads to a reduction in the alveolar ridge in the first six months in the horizontal dimension and then in the vertical dimension. Therefore, the bone is often inadequate for implant placement [1][2].
The guided bone regeneration (GBR) procedure, due to its numerous advantages, such as osteogenic stability and multidirectional osteogenesis capability, appears to be one of the most used and reliable techniques to restore bone deficits in height and/or width in association with implant treatment [3][4].
Currently, the GBR technique involves the employment of membranes, resorbable or non-resorbable, combined with bone substitute materials, depending on bone defect features [5].
Bone grafts, membranes, and biological materials have been tested for their regenerative characteristics for intrabony defect treatment, as well as furcation defects, peri-implantitis sites, alveolar ridge preservation, and implant site development [6][7][8][9].
Throughout the GBR procedure, osteoblasts can favorably and selectively enter the site of the defect to stimulate and regenerate the affected bone. Indeed, barrier membranes have the purpose of inhibiting early epithelial and connective cells’ colonization of the area, while bone-filling materials direct and control osteoblastic progenitor cells’ proliferation and differentiation [5][10].
Thanks to their excellent mechanical properties, titanium meshes are broadly used in the surgical field. Stiffness and strength help the osteogenesis process, stability permits bone-filling materials to maintain their volume during healing, and elasticity may decrease oral mucosa’s compression [11][12].
Bone-augmentation techniques that require titanium mesh and implant placement can occur synchronically or delayed, as well as GBR with other bone-grafting techniques [11][13][14][15][16].
When using surgical meshes, the main complication is wound dehiscence and subsequent mesh exposure during the healing process. Mesh exposure can be classified as early exposure occurring within 4 weeks post-surgery and delayed mesh exposure occurring after 4 weeks post-surgery. Early dehiscence manifestation is related to a reduction in new bone formation and synchronic increment in fibrous tissue; when this event occurs, the grid should be quickly eliminated, and disinfection procedures carried out [17][18]. On the other hand, late mesh exposure could potentially create substitute materials’ resorption, leading to a decrease in bone dimension and inadequate quantity. However, the mesh can be left in place, as disinfection with chlorhexidine, plaque management, and smoothing of the sharp edges could solve the problem without alterations in the process of bone regeneration [19][20][21].
Standardized meshes are products with pre-determined characteristics such as thickness and width; hence they must be manually modeled to adapt to the alveolar ridge of the specific patient. This procedure presents many drawbacks, such as longer surgery, imprecise fitting, infection, pain, flap laceration, and possible future mesh exposure [22][23][24].
Therefore, recent clinical research has focused more on customized titanium mesh, thanks to the latest digitalization trends and technologies available on the market (Figure 1). Pre-operative cross-sectional imaging (cone beam computed tomography-CBCT) and 3D digital models have to be collected; thus, the patient’s alveolar ridge can be virtually reconstructed with CAD technology [25].
Custom-made titanium mesh can be produced with different protocols: CAD/CAM-3D printing or mesh-preforming on patients’ 3D jaws models [26][27].
Personalized meshes showed numerous advantages, such as quicker surgery, tailored fitting, less retention used to pin the mesh, smoother edges, and subsequent mucosal stress reduction [11][28].
In the last decade, research has concentrated on customized mesh applications in the surgical field.
The following discussion considered randomized clinical trials, observational studies, cohort studies, and case series/case reports studies. Studies that did not meet inclusion criteria were excluded. The preferred reporting items for scoping reviews (PRISMA-ScR) consensus was followed. A total of 15 studies were selected herein. Based on the studies included, the literature suggests that meshes produced by a digital process are used to restore complex and severe bone defects. Moreover, they give satisfactory aesthetic results and fit the defects, counteracting grid exposure. However, more clinical trials should be conducted to evaluate long-term results, the rate of complications, and new materials for mesh manufacturing.
2. Bone Defect Dimension
The 3D technology and additive manufacturing procedure development permitted the creation of a patient-specific grid for GBR, established on the bone defect dimension, with notable properties, being physical or biological [27][29]. Contrary to standard Ti-mesh, the 3D-printed ones have smooth margins, with the chance of reducing mucosal detriment and consequential mesh exposure, the main complication occurring after GBR surgery. Moreover, bone deficits could be reconstructed more accurately and patient-specifically [28][30].
Some studies showed that 3D precision of bone increment is not significantly related to bone deficit dimensions, being minor or major bone defects [31]. Large combined alveolar bone defects in a horizontal and vertical dimension and simultaneous implant placement could be safely and predictably treated with virtual planning and CAD/CAM patient-specific mesh manufacturing [32]. The 3D patient models used for shaping the customized mesh permit a correct fitting to the alveolar bone.
Vertical bone deficiency can be efficiently treated with up to a 90% bone regeneration rate [33][34]. In complex bone defects, patient-specific Ti-mesh has been demonstrated to potentially concur to significant bone augmentation up to 11.48 mm in horizontal and 8.90 mm in vertical dimensions, suggesting laser-sintered CAD/CAM mesh as a reliable alternative in GBR procedure related to extended atrophic alveolar ridges [35].
3. Aesthetic Aspects
Maxillary and mandibular defects, being related to traumatic, tumoral, or congenital conditions, can significantly impact functional and aesthetic aspects of patients’ lives; thus, their reconstruction is essential [36]. A key factor to consider when restoring aesthetic and functional features is the application of a grid, which permits obtaining and reinforcing 3D bone reconstruction.
Digital planning of the surgical procedure and tailored mesh permit the maintenance of bone shape. Additionally, they cooperate in the correct positioning of graft material to place implant fixtures and enhance the precision of bone augmentation and maxillary interconnection [37][38]. Regarding the anterior maxillary region, aesthetic considerations need to be conducted.
Implant placement is strictly related to an adequate volume of alveolar bone. Thus, individualized mesh seems to give promising results as far as it concerns bone augmentation and aesthetics [39].
In patients who present critical concavities of the vestibular bone, virtual bone volume augmentation and customized titanium mesh fabrication through 3D-printing technology showed a notable bone augmentation (after 6 months 3.7 mm SD ± 0.59 and after 12 months 4.3 mm (SD ± 0.83) [40].
When positioning a personalized 3D Ti-mesh, it is important to consider the chance of obtaining good soft tissue management as well as good aesthetic results with voluminous and healthy tissue characteristics without any signs of scar or fibrosis [41].
A possible solution to ensure a complex bone regeneration in the aesthetic area could be a fully digital protocol that some clinicians already apply. This combines patient-specific titanium mesh with a prosthetically guided regeneration (PGR) to achieve predictable and satisfactory outcomes (Figure 1 and Figure 2) [42].
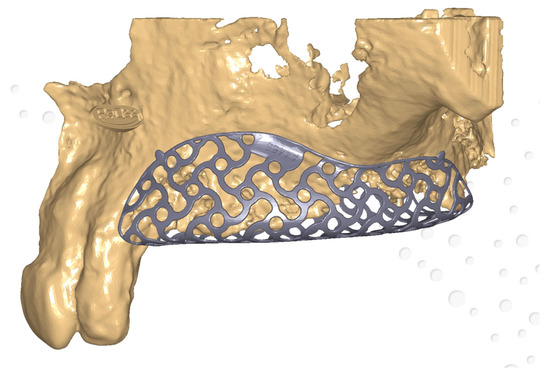
Figure 1. Customized mesh—virtual planning.
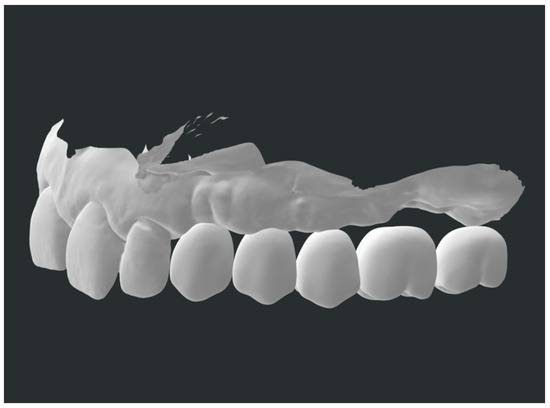
Figure 2. Prosthetically guided regeneration.
Specifically, overlaying a digital diagnostic wax-up can make the bone reconstruction procedure prophetically guided, allowing the maintenance of an adequate buccal cortical to ensure a satisfactory esthetic outcome [43][44].
4. Biological Considerations
Considering the histological characteristics of augmented alveolar bone, thanks to digital and individualized meshes, the freshly regenerated bone appeared mineralized at different stages. Close to the bone substitute materials residues in the connective tissue or medullary cavities, no signs of inflammation were noticed, leading to a newly regenerated tissue with structure, organization, vitality, and functioning processes of remodeling and assimilation of grafting materials [45].
Associated with bone regeneration, in the case of custom-made grid positioning, rapid and natural re-epithelialization under the intern portion of the mesh was noticed. This sign may be related to the initial bone augmentation with limited depletion [35].
5. Clinical Success and Complications
Virtual planning and personalized grid manufacturing associated with flap layout and its control are crucial aspects to consider in order to achieve clinical success in the GBR procedure [46]. Individualized Ti-meshes are more rigid than standard ones; thus, mesh exposure could happen eventually, even with this digital procedure [47].
This may be due to mechanical stress to the mucosal tissue’s flap, post-surgical removable prosthesis positioning, or eventually, the digital software learning curve and grid-projecting procedures [48].
Thus, a prudent approach must be adopted to ensure the clinical success of the procedure and avoid complications. Some authors showed that the application of a resorbable membrane above the customized mesh could reduce healing complication rates (13.3% vs. 33.3%) [49].
6. Early and Late Complication Management
In the case of mesh exposure, correct management can still lead to GBR success. The treatment consists of pharmacological or mechanical procedures.
Mesh exposure that occurs within 4 weeks after the surgical procedure is usually treated with chlorhexidine 0.2% (CHX) gels applied two to four times daily, followed by curettage of the interested site until tissue healing. Bone augmentation for implant positioning purposes is not limited in any way [21][50].
Alternatively, for CHX gel applications, the literature also suggests CHX mouthwashes or CHX spray with heterogeneous concentrations. However, gel preparations seem to be more effective than mouthwashes [51].
In the case of suspects of graft infection, topical antibiotic administration becomes relevant, while in the occurrence of mesh exposure, antibiotic administration is scarcely reported in the literature. This condition requires immediate mesh removal because of infection and pus. Plaque control and correct oral hygiene are also fundamental in these stages. Hence, saline washes and toothbrushes allow plaque removal [21].
For late exposure management, CHX 0.2% or, in some cases, 1% gel application two times a day until tissue healing appears to be useful and permits the maintenance of the mesh [20][52].
Mechanical smoothing of mesh edges with carbide or diamond burs for late exposure helps to create secondary healing of the wound [53][54].
7. New Materials
Despite titanium mesh being the most utilized material in guided-bone-regeneration processes, recently, the research has focused on different materials. Since PEEK material is starting to be broadly applied in the surgical field—orthopedic, traumatological, or even craniomaxillofacial—due to its inertness and biocompatibility, it could also be used in regenerative approaches [55][56].
In GBR procedures, customized PEEK grids have been applied to three-dimensional alveolar bone defects to place implant fixtures, and it has been demonstrated that there are no statistical differences (p-value = 0.2) between PEEK and pre-bent Ti-mesh, as far as it concerns bone regenerative processes [57].
References
- Hansson, S.; Halldin, A. Alveolar ridge resorption after tooth extraction: A consequence of a fundamental principle of bone physiology. J. Dent. Biomech. 2012, 3, 1758736012456543.
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23, 1–21.
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral Sci. 2017, 125, 315–337.
- Bornstein, M.M.; Halbritter, S.; Harnisch, H.; Weber, H.P.; Buser, D. A retrospective analysis of patients referred for implant placement to a specialty clinic: Indications, surgical procedures, and early failures. Int. J. Oral Maxillofac. Implant. 2008, 23, 1109–1116.
- Retzepi, M.; Donos, N. Guided Bone Regeneration: Biological principle and therapeutic applications. Clin. Oral Implant. Res. 2010, 21, 567–576.
- Ortega-Oller, I.; Padial-Molina, M.; Galindo-Moreno, P.; O’Valle, F.; Jódar-Reyes, A.B.; Peula-García, J.M. Bone Regeneration from PLGA Micro-Nanoparticles. Biomed. Res. Int. 2015, 2015, 415289.
- Padial-Molina, M.; O’Valle, F.; Lanis, A.; Mesa, F.; Dohan Ehrenfest, D.M.; Wang, H.L.; Galindo-Moreno, P. Clinical Application of Mesenchymal Stem Cells and Novel Supportive Therapies for Oral Bone Regeneration. Biomed. Res. Int. 2015, 2015, 341327.
- Gallo, S.; Pascadopoli, M.; Pellegrini, M.; Pulicari, F.; Manfredini, M.; Zampetti, P.; Spadari, F.; Maiorana, C.; Scribante, A. Latest Findings of the Regenerative Materials Application in Periodontal and Peri-Implant Surgery: A Scoping Review. Bioengineering 2022, 9, 594.
- Kormas, I.; Pedercini, A.; Alassy, H.; Wolff, L.F. The Use of Biocompatible Membranes in Oral Surgery: The Past, Present & Future Directions. A Narrative Review. Membranes 2022, 12, 841.
- Polo-Corrales, L.; Latorre-Esteves, M.; Ramirez-Vick, J.E. Scaffold design for bone regeneration. J. Nanosci. Nanotechnol. 2014, 14, 15–56.
- Jung, G.; Jeon, J.; Hwang, K.; Park, C. Preliminary evaluation of a three-dimensional, customized, and preformed titanium mesh in peri-implant alveolar bone regeneration. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 181–187.
- Badhey, A.; Kadakia, S.; Mourad, M.; Inman, J.; Ducic, Y. Calvarial Reconstruction. Semin. Plast. Surg. 2017, 31, 222–226.
- Konstantinidis, I.; Kumar, T.; Kher, U.; Stanitsas, P.D.; Hinrichs, J.E.; Kotsakis, G.A. Clinical results of implant placement in resorbed ridges using simultaneous guided bone regeneration: A multicenter case series. Clin. Oral Investig. 2015, 19, 553–559.
- Poli, P.P.; Beretta, M.; Cicciu, M.; Maiorana, C. Alveolar ridge augmentation with titanium mesh. A retrospective clinical study. Open Dent. J. 2014, 8, 148–158.
- Zhou, M.; Li, S.Y.; Terheyden, H.; Cao, S.S.; Che, Y.J.; Geng, Y.M. Particulate Coral Hydroxyapatite Sheltered by Titanium Mesh for Localized Alveolar Rehabilitation After Onlay Graft Failure: A Case Report. J. Oral Implantol. 2018, 44, 147–152.
- Maiorana, C.; Manfredini, M.; Beretta, M.; Signorino, F.; Bovio, A.; Poli, P.P. Clinical and Radiographic Evaluation of Simultaneous Alveolar Ridge Augmentation by Means of Preformed Titanium Meshes at Dehiscence-Type Peri-Implant Defects: A Prospective Pilot Study. Materials 2020, 13, 2389.
- Louis, P.J.; Gutta, R.; Said-Al-Naief, N.; Bartolucci, A.A. Reconstruction of the maxilla and mandible with particulate bone graft and titanium mesh for implant placement. J. Oral Maxillofac. Surg. 2008, 66, 235–245.
- Corinaldesi, G.; Pieri, F.; Sapigni, L.; Marchetti, C. Evaluation of survival and success rates of dental implants placed at the time of or after alveolar ridge augmentation with an autogenous mandibular bone graft and titanium mesh: A 3- to 8-year retrospective study. Int. J. Oral Maxillofac. Implant. 2009, 24, 1119–1128.
- Maiorana, C.; Santoro, F.; Rabagliati, M.; Salina, S. Evaluation of the use of iliac cancellous bone and anorganic bovine bone in the reconstruction of the atrophic maxilla with titanium mesh: A clinical and histologic investigation. Int. J. Oral Maxillofac. Implant. 2001, 16, 427–432.
- Roccuzzo, M.; Ramieri, G.; Bunino, M.; Berrone, S. Autogenous bone graft alone or associated with titanium mesh for vertical alveolar ridge augmentation: A controlled clinical trial. Clin. Oral Implant. Res. 2007, 18, 286–294.
- Poli, P.P.; Beretta, M.; Maiorana, C.; Souza, F.Á.; Bovio, A.; Manfredini, M. Therapeutic Strategies in the Management of Nonresorbable Membrane and Titanium Mesh Exposures Following Alveolar Bone Augmentation: A Systematic Scoping Review. Int. J. Oral Maxillofac. Implant. 2022, 37, 250–269.
- Benic, G.I.; Hämmerle, C.H. Horizontal bone augmentation by means of guided bone regeneration. Periodontol. 2000 2014, 66, 13–40.
- Okubo, T.; Tsukimura, N.; Taniyama, T.; Ishijima, M.; Nakhaei, K.; Rezaei, N.M.; Hirota, M.; Park, W.; Akita, D.; Tateno, A.; et al. Ultraviolet treatment restores bioactivity of titanium mesh plate degraded by contact with medical gloves. J. Oral Sci. 2018, 60, 567–573.
- Hartmann, A.; Hildebrandt, H.; Schmohl, J.U.; Kämmerer, P.W. Evaluation of risk parameters in bone regeneration using a customized titanium mesh: Results of a clinical study. Implant. Dent. 2019, 28, 543–550.
- Al-Ardah, A.J.; Alqahtani, N.; AlHelal, A.; Goodacre, B.J.; Swamidass, R.; Garbacea, A.; Lozada, J. Using Virtual Ridge Augmentation and 3-Dimensional Printing to Fabricate a Titanium Mesh Positioning Device: A Novel Technique Letter. J. Oral Implantol. 2018, 44, 293–299.
- Hartmann, A.; Seiler, M. Minimizing risk of customized titanium mesh exposures—A retrospective analysis. BMC Oral Health 2020, 20, 36.
- Inoue, K.; Nakajima, Y.; Omori, M.; Suwa, Y.; Kato-Kogoe, N.; Yamamoto, K.; Kitagaki, H.; Mori, S.; Nakano, H.; Ueno, T. Reconstruction of the Alveolar Bone Using Bone Augmentation With Selective Laser Melting Titanium Mesh Sheet: A Report of 2 Cases. Implant. Dent. 2018, 27, 602–607.
- Ciocca, L.; Fantini, M.; De Crescenzio, F.; Corinaldesi, G.; Scotti, R. Direct metal laser sintering (DMLS) of a customized titanium mesh for prosthetically guided bone regeneration of atrophic maxillary arches. Med. Biol. Eng. Comput. 2011, 49, 1347–1352.
- Kadkhodazadeh, M.; Amid, R.; Moscowchi, A. Management of extensive peri-implant defects with titanium meshes. Oral Maxillofac. Surg. 2021, 25, 561–568.
- Windisch, P.; Orban, K.; Salvi, G.E.; Sculean, A.; Molnar, B. Vertical-guided bone regeneration with a titanium-reinforced d-PTFE membrane utilizing a novel split-thickness flap design: A prospective case series. Clin. Oral Investig. 2021, 25, 2969–2980.
- Yang, W.; Chen, D.; Wang, C.; Apicella, D.; Apicella, A.; Huang, Y.; Li, L.; Zheng, L.; Ji, P.; Wang, L.; et al. The effect of bone defect size on the 3D accuracy of alveolar bone augmentation performed with additively manufactured patient-specific titanium mesh. BMC Oral Health 2022, 22, 557.
- Boogaard, M.J.; Santoro, F.; Romanos, G.E. Mesh Ridge Augmentation Using CAD/CAM Technology for Design and Printing: Two Case Reports. Compend. Contin. Educ. Dent. 2022, 43, 654–663.
- Cucchi, A.; Bettini, S.; Corinaldesi, G. A novel technique for digitalisation and customisation of reinforced polytetrafluoroethylene meshes: Preliminary results of a clinical trial. Int. J. Oral Implantol. 2022, 15, 129–146.
- Lizio, G.; Pellegrino, G.; Corinaldesi, G.; Ferri, A.; Marchetti, C.; Felice, P. Guided bone regeneration using titanium mesh to augment 3-dimensional alveolar defects prior to implant placement. A pilot study. Clin. Oral Implant. Res. 2022, 33, 607–621.
- Chiapasco, M.; Casentini, P.; Tommasato, G.; Dellavia, C.; Del Fabbro, M. Customized CAD/CAM titanium meshes for the guided bone regeneration of severe alveolar ridge defects: Preliminary results of a retrospective clinical study in humans. Clin. Oral Implant. Res. 2021, 32, 498–510.
- Cuellar, C.N.; Gil, M.C.; Delgado, J.P.; Martínez, B.G.; Sanz, J.A.; de Atalaya, J.L.; Ochandiano, S.; Vila, C.N. Reconstrucción oromandibular con colgajo libre de peroné e implantes osteointegrados. Acta Otorrinolaringol. Esp. 2003, 54, 54–64.
- Navarro Cuéllar, C.; Tousidonis Rial, M.; Antúnez-Conde, R.; Ochandiano Caicoya, S.; Navarro Cuéllar, I.; Arenas de Frutos, G.; Sada Urmeneta, Á.; García-Hidalgo Alonso, M.I.; Navarro Vila, C.; Salmerón Escobar, J.I. Virtual Surgical Planning, Stereolitographic Models and CAD/CAM Titanium Mesh for Three-Dimensional Reconstruction of Fibula Flap with Iliac Crest Graft and Dental Implants. J. Clin. Med. 2021, 10, 1922.
- Iino, M.; Fukuda, M.; Nagai, H.; Hamada, Y.; Yamada, H.; Nakaoka, K.; Mori, Y.; Chikazu, D.; Saijo, H.; Seto, I.; et al. Evaluation of 15 mandibular reconstructions with Dumbach titan mesh-system and particulate cancellous bone and marrow harvested from bilateral posterior ilia. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, e1–e8.
- Gelețu, G.L.; Burlacu, A.; Murariu, A.; Andrian, S.; Golovcencu, L.; Baciu, E.R.; Maftei, G.; Onica, N. Customized 3D-Printed Titanium Mesh Developed for an Aesthetic Zone to Regenerate a Complex Bone Defect Resulting after a Deficient Odontectomy: A Case Report. Medicina 2022, 58, 1192.
- Nickenig, H.J.; Riekert, M.; Zirk, M.; Lentzen, M.P.; Zöller, J.E.; Kreppel, M. 3D-based buccal augmentation for ideal prosthetic implant alignment-an optimized method and report on 7 cases with pronounced buccal concavities. Clin. Oral Investig. 2022, 26, 3999–4010.
- Ghanaati, S.; Al-Maawi, S.; Conrad, T.; Lorenz, J.; Rössler, R.; Sader, R. Biomaterial-based bone regeneration and soft tissue management of the individualized 3D-titanium mesh: An alternative concept to autologous transplantation and flap mobilization. J. Craniomaxillofac. Surg. 2019, 47, 1633–1644.
- Tallarico, M.; Park, C.J.; Lumbau, A.I.; Annucci, M.; Baldoni, E.; Koshovari, A.; Meloni, S.M. Customized 3D-Printed Titanium Mesh Developed to Regenerate a Complex Bone Defect in the Aesthetic Zone: A Case Report Approached with a Fully Digital Workflow. Materials 2020, 13, 3874.
- Farronato, D.; Pasini, P.M.; Orsina, A.A.; Manfredini, M.; Azzi, L.; Farronato, M. Correlation between Buccal Bone Thickness at Implant Placement in Healed Sites and Buccal Soft Tissue Maturation Pattern: A Prospective Three-Year Study. Materials 2020, 13, 511.
- Chiapasco, M.; Casentini, P. Horizontal bone-augmentation procedures in implant dentistry: Prosthetically guided regeneration. Periodontol. 2000 2018, 77, 213–240.
- Dellavia, C.; Canciani, E.; Pellegrini, G.; Tommasato, G.; Graziano, D.; Chiapasco, M. Histological assessment of mandibular bone tissue after guided bone regeneration with customized computer-aided design/computer-assisted manufacture titanium mesh in humans: A cohort study. Clin. Implant Dent. Relat. Res. 2021, 23, 600–611.
- De Santis, D.; Luciano, U.; Donadello, D.; Faccioni, P.; Zarantonello, M.; Alberti, C.; Verlato, G.; Gelpi, F. Custom Bone Regeneration (CBR): An Alternative Method of Bone Augmentation-A Case Series Study. J. Clin. Med. 2022, 11, 4739.
- Lorenz, J.; Al-Maawi, S.; Sader, R.; Ghanaati, S. Individualized Titanium Mesh Combined With Platelet-Rich Fibrin and Deproteinized Bovine Bone: A New Approach for Challenging Augmentation. J. Oral Implantol. 2018, 44, 345–351.
- Ciocca, L.; Lizio, G.; Baldissara, P.; Sambuco, A.; Scotti, R.; Corinaldesi, G. Prosthetically CAD-CAM-Guided Bone Augmentation of Atrophic Jaws Using Customized Titanium Mesh: Preliminary Results of an Open Prospective Study. J. Oral Implantol. 2018, 44, 131–137.
- Cucchi, A.; Vignudelli, E.; Franceschi, D.; Randellini, E.; Lizio, G.; Fiorino, A.; Corinaldesi, G. Vertical and horizontal ridge augmentation using customized CAD/CAM titanium mesh with versus without resorbable membranes. A randomized clinical trial. Clin. Oral Implant. Res. 2021, 32, 1411–1424.
- Lizio, G.; Corinaldesi, G.; Marchetti, C. Alveolar ridge reconstruction with titanium mesh: A three-dimensional evaluation of factors affecting bone augmentation. Int. J. Oral Maxillofac. Implant. 2014, 29, 1354–1363.
- Canullo, L.; Laino, L.; Longo, F.; Filetici, P.; D’Onofrio, I.; Troiano, G. Does chlorhexidine prevent complications in extractive, periodontal, and implant surgery? A systematic review and meta-analysis with trial sequential analysis. Int. J. Oral Maxillofac. Implant. 2020, 35, 1149–1158.
- Roccuzzo, M.; Ramieri, G.; Spada, M.C.; Bianchi, S.D.; Berrone, S. Vertical alveolar ridge augmentation by means of a titanium mesh and autogenous bone grafts. Clin. Oral Implant. Res. 2004, 15, 73–81.
- Al-Ardah, A.J.; AlHelal, A.; Proussaefs, P.; AlBader, B.; Al Humaidan, A.A.; Lozada, J. Managing titanium mesh exposure with partial removal of the exposed site: A case series study. J. Oral Implantol. 2017, 43, 482–490.
- Her, S.; Kang, T.; Fien, M.J. Titanium mesh as an alternative to a membrane for ridge augmentation. J. Oral Maxillofac. Surg. 2012, 70, 803–810.
- Suresh, V.; Anolik, R.; Powers, D. The Utility of Polyether-Ether-Ketone Implants Adjacent to Sinus Cavities after Craniofacial Trauma. J. Oral Maxillofac. Surg. 2018, 76, 2361–2369.
- Honigmann, P.; Sharma, N.; Okolo, B.; Popp, U.; Msallem, B.; Thieringer, F.M. Patient-Specific Surgical Implants Made of 3D Printed PEEK: Material, Technology, and Scope of Surgical Application. Biomed. Res. Int. 2018, 2018, 4520636.
- Mounir, M.; Shalash, M.; Mounir, S.; Nassar, Y.; El Khatib, O. Assessment of three-dimensional bone augmentation of severely atrophied maxillary alveolar ridges using prebent titanium mesh vs customized poly-ether-ether-ketone (PEEK) mesh: A randomized clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 960–967.
- Salem, D.; Reher, P.; Evans, J.L.; Mansour, M.H. Exploring digital technologies used in the design and manufacture of craniofacial implant surgical guides: A scoping review. J. Prosthet. Dent. 2023, in press.
- Thakur, J.; Parlani, S.; Shivakumar, S.; Jajoo, K. Accuracy of marginal fit of an implant-supported framework fabricated by 3D printing versus subtractive manufacturing technique: A systematic review and meta-analysis. J. Prosthet. Dent. 2023, 129, 301–309.
- Gallo, S.; Pascadopoli, M.; Pellegrini, M.; Pulicari, F.; Manfredini, M.; Zampetti, P.; Spadari, F.; Maiorana, C.; Scribante, A. CAD/CAM Abutments versus Stock Abutments: An Update Review. Prosthesis 2022, 4, 468–479.
- Cabello-Domínguez, G.; Pérez-López, J.; Veiga-López, B.; González, D.; Revilla-León, M. Maxillary zirconia and mandibular composite resin-lithium disilicate-modified PEEK fixed implant-supported restorations for a completely edentulous patient with an atrophic maxilla and mandible: A clinical report. J. Prosthet. Dent. 2020, 124, 403–410.
More
Information
Subjects:
Dentistry, Oral Surgery & Medicine
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
685
Revisions:
2 times
(View History)
Update Date:
26 May 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No