1. Introduction
The alveolar bone undergoes two successive processes after extraction or loss of a dental element: resorption and atrophy. This leads to a reduction in the alveolar ridge in the first six months in the horizontal dimension and then in the vertical dimension. Therefore, the bone is often inadequate for implant placement [
1,
2].
The guided bone regeneration (GBR) procedure, due to its numerous advantages, such as osteogenic stability and multidirectional osteogenesis capability, appears to be one of the most used and reliable techniques to restore bone deficits in height and/or width in association with implant treatment [
3,
4].
Currently, the GBR technique involves the employment of membranes, resorbable or non-resorbable, combined with bone substitute materials, depending on bone defect features [
5].
Bone grafts, membranes, and biological materials have been tested for their regenerative characteristics for intrabony defect treatment, as well as furcation defects, peri-implantitis sites, alveolar ridge preservation, and implant site development [
6,
7,
8,
9].
Throughout the GBR procedure, osteoblasts can favorably and selectively enter the site of the defect to stimulate and regenerate the affected bone. Indeed, barrier membranes have the purpose of inhibiting early epithelial and connective cells’ colonization of the area, while bone-filling materials direct and control osteoblastic progenitor cells’ proliferation and differentiation [
5,
10].
Thanks to their excellent mechanical properties, titanium meshes are broadly used in the surgical field. Stiffness and strength help the osteogenesis process, stability permits bone-filling materials to maintain their volume during healing, and elasticity may decrease oral mucosa’s compression [
11,
12].
Bone-augmentation techniques that require titanium mesh and implant placement can occur synchronically or delayed, as well as GBR with other bone-grafting techniques [
11,
13,
14,
15,
16].
When using surgical meshes, the main complication is wound dehiscence and subsequent mesh exposure during the healing process. Mesh exposure can be classified as early exposure occurring within 4 weeks post-surgery and delayed mesh exposure occurring after 4 weeks post-surgery. Early dehiscence manifestation is related to a reduction in new bone formation and synchronic increment in fibrous tissue; when this event occurs, the grid should be quickly eliminated, and disinfection procedures carried out [
17,
18]. On the other hand, late mesh exposure could potentially create substitute materials’ resorption, leading to a decrease in bone dimension and inadequate quantity. However, the mesh can be left in place, as disinfection with chlorhexidine, plaque management, and smoothing of the sharp edges could solve the problem without alterations in the process of bone regeneration [
19,
20,
21].
Standardized meshes are products with pre-determined characteristics such as thickness and width; hence they must be manually modeled to adapt to the alveolar ridge of the specific patient. This procedure presents many drawbacks, such as longer surgery, imprecise fitting, infection, pain, flap laceration, and possible future mesh exposure [
22,
23,
24].
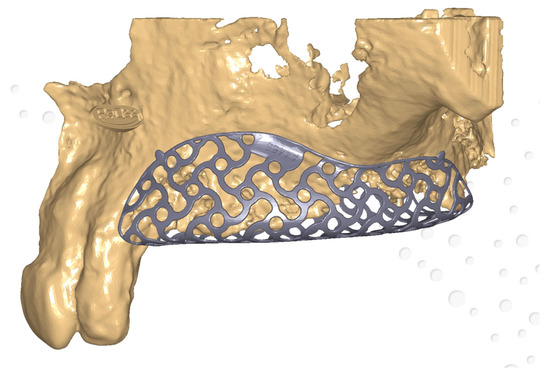
Therefore, recent clinical research has focused more on customized titanium mesh, thanks to the latest digitalization trends and technologies available on the market (
Figure 1). Pre-operative cross-sectional imaging (cone beam computed tomography-CBCT) and 3D digital models have to be collected; thus, the patient’s alveolar ridge can be virtually reconstructed with CAD technology [
25].
Custom-made titanium mesh can be produced with different protocols: CAD/CAM-3D printing or mesh-preforming on patients’ 3D jaws models [
26,
27].
Personalized meshes showed numerous advantages, such as quicker surgery, tailored fitting, less retention used to pin the mesh, smoother edges, and subsequent mucosal stress reduction [
11,
28].
In the last decade, research has concentrated on customized mesh applications in the surgical field.
2. Bone Defect Dimension
The 3D technology and additive manufacturing procedure development permitted the creation of a patient-specific grid for GBR, established on the bone defect dimension, with notable properties, being physical or biological [
27,
61]. Contrary to standard Ti-mesh, the 3D-printed ones have smooth margins, with the chance of reducing mucosal detriment and consequential mesh exposure, the main complication occurring after GBR surgery. Moreover, bone deficits could be reconstructed more accurately and patient-specifically [
28,
62].
Some studies showed that 3D precision of bone increment is not significantly related to bone deficit dimensions, being minor or major bone defects [
51]. Large combined alveolar bone defects in a horizontal and vertical dimension and simultaneous implant placement could be safely and predictably treated with virtual planning and CAD/CAM patient-specific mesh manufacturing [
53]. The 3D patient models used for shaping the customized mesh permit a correct fitting to the alveolar bone.
Vertical bone deficiency can be efficiently treated with up to a 90% bone regeneration rate [
45,
46]. In complex bone defects, patient-specific Ti-mesh has been demonstrated to potentially concur to significant bone augmentation up to 11.48 mm in horizontal and 8.90 mm in vertical dimensions, suggesting laser-sintered CAD/CAM mesh as a reliable alternative in GBR procedure related to extended atrophic alveolar ridges [
49].
3. Aesthetic Aspects
Maxillary and mandibular defects, being related to traumatic, tumoral, or congenital conditions, can significantly impact functional and aesthetic aspects of patients’ lives; thus, their reconstruction is essential [
63]. A key factor to consider when restoring aesthetic and functional features is the application of a grid, which permits obtaining and reinforcing 3D bone reconstruction.
Digital planning of the surgical procedure and tailored mesh permit the maintenance of bone shape. Additionally, they cooperate in the correct positioning of graft material to place implant fixtures and enhance the precision of bone augmentation and maxillary interconnection [
50,
64]. Regarding the anterior maxillary region, aesthetic considerations need to be conducted.
Implant placement is strictly related to an adequate volume of alveolar bone. Thus, individualized mesh seems to give promising results as far as it concerns bone augmentation and aesthetics [
56].
In patients who present critical concavities of the vestibular bone, virtual bone volume augmentation and customized titanium mesh fabrication through 3D-printing technology showed a notable bone augmentation (after 6 months 3.7 mm
SD ± 0.59 and after 12 months 4.3 mm (
SD ± 0.83) [
54].
When positioning a personalized 3D Ti-mesh, it is important to consider the chance of obtaining good soft tissue management as well as good aesthetic results with voluminous and healthy tissue characteristics without any signs of scar or fibrosis [
52].
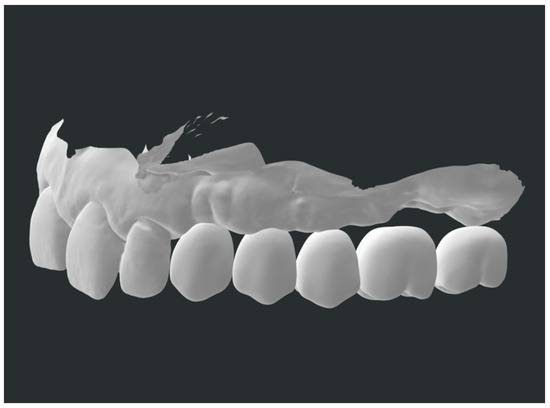
A possible solution to ensure a complex bone regeneration in the aesthetic area could be a fully digital protocol that some clinicians already apply. This combines patient-specific titanium mesh with a prosthetically guided regeneration (PGR) to achieve predictable and satisfactory outcomes (
Figure 1 and
Figure 2) [
57].
Figure 1. Customized mesh—virtual planning.
Figure 2. Prosthetically guided regeneration.
Specifically, overlaying a digital diagnostic wax-up can make the bone reconstruction procedure prophetically guided, allowing the maintenance of an adequate buccal cortical to ensure a satisfactory esthetic outcome [
65,
66].
4. Biological Considerations
Considering the histological characteristics of augmented alveolar bone, thanks to digital and individualized meshes, the freshly regenerated bone appeared mineralized at different stages. Close to the bone substitute materials residues in the connective tissue or medullary cavities, no signs of inflammation were noticed, leading to a newly regenerated tissue with structure, organization, vitality, and functioning processes of remodeling and assimilation of grafting materials [
47].
Associated with bone regeneration, in the case of custom-made grid positioning, rapid and natural re-epithelialization under the intern portion of the mesh was noticed. This sign may be related to the initial bone augmentation with limited depletion [
49].
5. Clinical Success and Complications
Virtual planning and personalized grid manufacturing associated with flap layout and its control are crucial aspects to consider in order to achieve clinical success in the GBR procedure [
55]. Individualized Ti-meshes are more rigid than standard ones; thus, mesh exposure could happen eventually, even with this digital procedure [
67].
This may be due to mechanical stress to the mucosal tissue’s flap, post-surgical removable prosthesis positioning, or eventually, the digital software learning curve and grid-projecting procedures [
48].
Thus, a prudent approach must be adopted to ensure the clinical success of the procedure and avoid complications. Some authors showed that the application of a resorbable membrane above the customized mesh could reduce healing complication rates (13.3% vs. 33.3%) [
43].
6. Early and Late Complication Management
In the case of mesh exposure, correct management can still lead to GBR success. The treatment consists of pharmacological or mechanical procedures.
Mesh exposure that occurs within 4 weeks after the surgical procedure is usually treated with chlorhexidine 0.2% (CHX) gels applied two to four times daily, followed by curettage of the interested site until tissue healing. Bone augmentation for implant positioning purposes is not limited in any way [
21,
68].
Alternatively, for CHX gel applications, the literature also suggests CHX mouthwashes or CHX spray with heterogeneous concentrations. However, gel preparations seem to be more effective than mouthwashes [
69].
In the case of suspects of graft infection, topical antibiotic administration becomes relevant, while in the occurrence of mesh exposure, antibiotic administration is scarcely reported in the literature. This condition requires immediate mesh removal because of infection and pus. Plaque control and correct oral hygiene are also fundamental in these stages. Hence, saline washes and toothbrushes allow plaque removal [
21].
For late exposure management, CHX 0.2% or, in some cases, 1% gel application two times a day until tissue healing appears to be useful and permits the maintenance of the mesh [
20,
70].
Mechanical smoothing of mesh edges with carbide or diamond burs for late exposure helps to create secondary healing of the wound [
71,
72].
7. New Materials
Despite titanium mesh being the most utilized material in guided-bone-regeneration processes, recently, the research has focused on different materials. Since PEEK material is starting to be broadly applied in the surgical field—orthopedic, traumatological, or even craniomaxillofacial—due to its inertness and biocompatibility, it could also be used in regenerative approaches [
73,
74].
In GBR procedures, customized PEEK grids have been applied to three-dimensional alveolar bone defects to place implant fixtures, and it has been demonstrated that there are no statistical differences (
p-value = 0.2) between PEEK and pre-bent Ti-mesh, as far as it concerns bone regenerative processes [
44].
Full-digital meshes represent one component of a digitization process that includes other stages that complete a surgical case, such as case design, CAD/CAM abutments and crowns, and other 3D-printed components [
75,
76,
77,
78].
This entry is adapted from the peer-reviewed paper 10.3390/prosthesis5020033