Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Martina Zibetti | -- | 3278 | 2023-04-17 10:10:52 | | | |
| 2 | Sirius Huang | + 1 word(s) | 3279 | 2023-04-18 03:27:22 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Tomaiuolo, R.; Zibetti, M.; Di Resta, C.; Banfi, G. Traumatic Brain Injuries Biomarkers in Sports-Related Context. Encyclopedia. Available online: https://encyclopedia.pub/entry/43112 (accessed on 29 June 2026).
Tomaiuolo R, Zibetti M, Di Resta C, Banfi G. Traumatic Brain Injuries Biomarkers in Sports-Related Context. Encyclopedia. Available at: https://encyclopedia.pub/entry/43112. Accessed June 29, 2026.
Tomaiuolo, Rossella, Martina Zibetti, Chiara Di Resta, Giuseppe Banfi. "Traumatic Brain Injuries Biomarkers in Sports-Related Context" Encyclopedia, https://encyclopedia.pub/entry/43112 (accessed June 29, 2026).
Tomaiuolo, R., Zibetti, M., Di Resta, C., & Banfi, G. (2023, April 17). Traumatic Brain Injuries Biomarkers in Sports-Related Context. In Encyclopedia. https://encyclopedia.pub/entry/43112
Tomaiuolo, Rossella, et al. "Traumatic Brain Injuries Biomarkers in Sports-Related Context." Encyclopedia. Web. 17 April, 2023.
Copy Citation
Traumatic brain injury (TBI) affects 69 million people every year. One of the main limitations in managing TBI patients is the lack of univocal diagnostic criteria, including the absence of standardized assessment methods and guidelines. Immediacy and accuracy in diagnosis and management of TBIs are critically unmet medical needs. Especially in the context of sports-associated TBI, there is a strong need for prognostic indicators to help diagnose and identify at-risk subjects to avoid their returning to play while the brain is still highly vulnerable. Fluid biomarkers may emerge as new prognostic indicators to develop more accurate prediction models, improving risk stratification and clinical decision-making.
traumatic brain injury (TBI)
sports-related TBI
brain injury markers/biomarkers
TBI biomarker
outcome assessment
1. Introduction
Every year, 69 million people worldwide suffer from traumatic brain injury (TBI) [1], defined by the WHO Neurotrauma Task Force as a blow to the head that causes acute impairment of brain function. Higher rates of TBI are seen in the adult population over 75, in children under 5, and in adolescents between 15 and 24 years of age [2].
TBI is a high-risk condition with a significant public health and socioeconomic impact because of its high mortality rate, morbidity, and disability rate [1].
The diagnosis of TBI is usually made in the emergency room using the Glasgow Coma Scale (GCS), universally recognized in the classification of TBI. The GCS allows classification of patients into three presumptively homogeneous groups for risk of post-traumatic cerebral hematoma, need for neurosurgery, and prognosis: severe head injury (GCS 3–8), moderate head injury (GCS 9–13), and mild head injury (GCS 14–15) [3].
Computed axial tomography (CT) is the leading method of radiological examination [4], it is estimated to have a sensitivity of 100%, with a positive predictive value of 10%, a negative predictive value of 100%, and a specificity of 51% [5]. MRI can also be used to assess traumatic brain injuries; it is more sensitive than CT in identifying the precise location and extent of intracranial haemorrhage and associated edema [6]. Nevertheless, conventional CT remains the initial imaging modality of choice since it is more available and cost effective, it requires shorter imaging time, and it is easier to perform [7]. However, the systematic carrying out of CT scanning in all patients is undesirable due to the limited prevalence of positivity, radiological risk of exposure, extended stay in emergency departments, inefficient use of resources, and its high cost and complexity [4].
Altogether, 90% of brain injuries are classified as mild TBI (mTBI) [8], about 15 times more frequent than moderate and over 20 times more than severe [3]. The main manifestations of this trauma are a brief loss of consciousness (less than 30 min), confusion, or post-traumatic amnesia not attributable to other factors, such as psychological trauma or intoxication from alcohol or drugs [2].
The Mild TBI Committee of the American Congress of Rehabilitation Medicine, revised by the World Health Organization (WHO), declared that “mTBI is defined by a Glasgow Coma Scale score between 13 and 15 at 30 min post-injury, and one or more of the following symptoms: <30 min loss of consciousness; <24 h post-traumatic amnesia (PTA); impaired mental state at the time of the accident (confusion, disorientation, etc.); and/or transient neurological deficit” [9].
It is essential to consider that mTBI can sometimes be associated with severe intracranial injuries: the patient can face the risk of complications, in particular intracranial bleeding, at various times: immediately up to about 48–72 h, in the medium term up to 4–8 weeks, and in the long term up to a few months. For this reason, risk stratification is essential for diagnosis based on integrating clinical anamnestic data, trauma (dynamics) data, and drug history [10]. mTBI may also give rise to neurodegenerative disorders and increase survivors’ risk of developing chronic behavioral and neurological impairment affecting the quality of their lives [11]. mTBIs are commonly observed in collision sports athletes and military personnel, and can also result from falls, motor vehicle accidents, or assaults [12].
Exposure to repeated mTBIs may lead to debilitating long-term neurological conditions: When the brain has not fully recovered from previous trauma, it can be highly vulnerable to repeated mTBIs. There is a significant clinical need for objective tests that could help to diagnose mTBIs and identify ‘‘at-risk’’ people. The clinical management of mTBI must be based on the probability of developing neurological complications (evolutionary risk), considering the absence or presence of one or more pre-existing or consequent risk factors [4]. In addition to the primary injury that arises immediately after the trauma, there may be secondary injuries resulting in a series of molecular and cellular reactions that last for a long time after the trauma, leading to neuronal and astroglia injuries, axonal disruption, and inflammation [11].
There is a strong need for prognostic indicators of long-term outcomes following mTBI, to identify at-risk subjects to avoid their return to play or duty while the brain is still highly vulnerable. Fluid biomarkers may emerge as new prognostic indicators to develop more accurate prediction models, improving risk stratification and clinical decision-making [12][13]. Much progress has been made in understanding the cellular sources, temporal profiles, and potential utility of key and emerging blood protein biomarkers.
2. Current Guidelines
There is no uniformity concerning the guidelines to be followed nationally and internationally. There are significant between-center variations in policies for diagnostics, admission, and discharge decisions in patients with TBI in the emergency department and hospital ward [14].
Commonalities between the different guidelines include the focus of evaluation mainly on assessing the patient’s mental status, cranial nerves, sensory awareness, motor functions, and reflexes. Patients receiving antiplatelet/anticoagulant therapy should have treatment suspended for the entire duration of the observation [14]. Neurological imaging is essential to identify a patient with head trauma caused by acute injury or persistent symptoms, and computed tomography is the primary method of radiological examination [4].
Each country has its directives for CT use; for instance, in Europe and Canada, CT for minor head injury cases is used very selectively. In Italy in particular, CT is only recommended if a fracture has been shown by skull radiography; in Denmark, it is rarely ordered and then only by a neurosurgeon; in the UK and Spain, CT is only recommended for cases with a documented skull fracture, focal neurological deficit, or deterioration in mental status [15].
The most frequently used guidelines are the Canadian CT Head Rule, the Scandinavian Guidelines, the New Orleans Criteria for TC scan in mild head injury, the guidelines of the National Institute for Health and Care Excellence (NICE 2014), and those of the Neurotramatology Committee of the World Federation of Neurosurgical Societies (NCWFS) [14]. These guidelines differ in terms of the parameters taken into consideration, as shown in Table 1: The Canadian CT rules are based on five high-risk and two medium-risk criteria [15]; the Scandinavian guidelines also consider the serum levels of S100 calcium-binding protein B (S100B) [16][17]; the New Orleans Criteria for TC scan (NOC) included seven items and were only developed for use in patients with a GCS score of 15 [18]; the guidelines of the National Institute for Health and Care Excellence (NICE 2014) are based upon the Canadian CT head rule and lead to more CT scans being performed, but fewer skull radiographs and admissions [19][20][21]; and lastly, the Neurotraumatology Committee of the World Federation of Neurosurgical Societies (NCWFS) protocol is similar to the NICE guidelines. However, it is less strict and leads to more CTs [22][23].
Table 1. Comparison between the already-in-use prediction rules for traumatic brain injury. NICE: National Institute for Health and Care Excellence; NCWFS: Neurotraumatology Committee of the World Federation of Neurosurgical Societies. High risk: risk factor is present in the prediction rule as a major criterion; medium risk: risk factor is present in the prediction rule as a minor criterion; blank: the variable is not a risk factor in the model.
| Risk Factor | New Orleans Criteria | Canadian CT Head Rule | NICE 2014 | NCWFS | Scandinavian |
|---|---|---|---|---|---|
| Headache | High risk | High risk | Medium risk | ||
| Vomiting | High risk | High risk | High risk | High risk | Medium risk |
| Post-traumatic seizure | High risk | High risk | High risk | ||
| Intoxication (drug or alcohol) | High risk | High risk | |||
| Persistent anterograde amnesia | High risk | High risk | |||
| Age | High risk > 60 years | High risk > 65 years | High risk > 65 years | ||
| Clinical signs of skull fracture | High risk | High risk | High risk | High risk | High risk |
| Contusion of the skull | High risk | High risk | High risk | High risk | High risk |
| Signs official fracture | High risk | ||||
| Contusion of the face | High risk | ||||
| GCS score deterioration | High risk | High risk | High risk | ||
| Pedestrian versus vehicle | Medium risk | High risk | |||
| Ejected from vehicle | Medium risk | High risk | |||
| Fall from height | Medium risk | High risk | |||
| Prolonged post-traumatic amnesia | Medium risk | High risk | High risk | Medium risk | |
| GCS < 15 at presentation | High risk | High risk | High risk | ||
| Loss of consciousness | High risk | Medium risk | |||
| Neurologic deficit | High risk | High risk | Medium risk | ||
| Anticoagulation therapy | High risk | High risk | High risk | ||
| High-energy trauma | |||||
| Multiple injuries | |||||
| Pre-traumatic seizure | High risk | ||||
| Unclear trauma mechanism | |||||
| Previous neurosurgery | High risk | ||||
| S100B ≥ 0.1 μg/L | Medium risk |
3. Markers
An ideal biomarker should be easy to measure in accessible bodily fluids such as cerebrospinal fluid or blood (serum/plasma); it should allow repeated detection for monitoring the initial brain injury in the hours that follow, and its elevated levels should correlate directly with the presence of brain trauma and the degree of severity of traumatic brain injury. Therefore, all the substances that can be released because of neuronal cell injury, glial cell injury, axonal injury, and inflammation are potential biomarkers for TBI.
Research into blood-based TBI biomarkers has accelerated rapidly in the past decade, leading to the identification of proteins resulting from axonal, neuronal, or glial cell injuries and released into the interstitial fluid (ISF), cerebrospinal fluid (CSF), and blood circulation due to altered function of the blood–brain barrier (BBB) after TBI [12].
Neuroimaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) can identify gross head injuries but not minute neural and structural changes typical of mild TBI. Conversely, fluid biomarkers are accurate tools that can be used to assess mild TBI pathophysiology [11]: increased understanding of individual biomarker trajectories in the hours, days, and weeks post-injury will enable a greater understanding of diagnostic windows from acute and chronic perspectives. It will furthermore allow studies to investigate the best potential biomarkers for predicting outcomes and tracking pathophysiological recovery or measuring response to treatment in mTBI clinical trials [12].
The following paragraphs report the current understanding of the cellular sources, temporal profile, and potential utility of leading and emerging blood-based protein biomarkers of TBI (Figure 1). Attention is focused on the characteristics that may favor use of these markers as surrogates for imaging techniques in the case of sports-related traumatic brain injuries.
3.1. Markers of Neuronal Cell Body Injury
Neuron-specific enolase (NSE) is a neuronal cytoplasmatic enzyme necessary for the glycolytic pathway. NSE serum concentration rises in the first 12 h after TBI and declines within hours or days. The main drawback of using NSE as a TBI diagnostic tool is its high erythrocyte concentration. Therefore, it can also be elevated without TBI, for instance, in hemolysis or multi-trauma conditions [11]. Hemolysis of blood samples, extracranial injury, and physical exercise may generate false positives [12].
Ubiquitin C-terminal hydrolase-L1 (UCH-L1) is a neuronal cytoplasmatic deubiquitinating enzyme needed to remove abnormal neuronal proteins in physiological and pathological conditions. The increased serum concentration of UCH-L1 increases within the first 6–24 h after TBI and correlates with injury severity and clinical outcomes, including GCS score at admission and CT lesions [11]. In CT-positive patients, serum levels 6–12 h post-injury were greater in those with unfavorable neurological outcomes [12]. It is, therefore, a potential prognostic and diagnostic biomarker for mild, moderate, and severe TBIs.
3.2. Markers of Glial Cell Injury
S100 calcium-binding protein B (S100B) is a calcium-binding protein within astroglial cells, which can be released in the extracellular space following trauma and ischemic events. Studies of moderate-to-severe TBI show peaks of S100B serum around 24–48 h after injury; however, a recent study found elevated levels at 1 h but not at 12 or 36 h post-concussion [12]. High levels of S100B are related to injury severity and predict the occurrence of post-concussion syndrome after mild TBI, poor clinical outcomes, and increased mortality. S100B protein is currently used in the early control of minimal, mild, and moderate TBI in Scandinavia, according to their head injury management guidelines (2007), to predict normal CT after mTBI, reducing unnecessary CT scans when S100B < 0.1 μg/L [11]. A limitation in using S100B as a prognostic biomarker after TBI is the extra-neural injury release from cardiac muscle, adipose tissue, and skeletal muscles. S100B is also present in melanocytes, and patients with darker skin show higher levels of the biomarker. Nonetheless, strenuous exercise and extracranial injury can increase blood S100B levels, thus potentially reducing their utility as a biomarker in sports-related concussions and polytrauma. Another pitfall relating to S100B is its short half-life of 90 min, making it difficult to use as a biomarker for brain injury [12][24][25].
Glial fibrillary acidic protein (GFAP) is an intermediate filament within astroglial cells that is needed to maintain their structure and to activate glial cells. After TBI, astroglial cells are activated and induce gliosis or glial scar formation, increasing the expression of GFAP [11]. There is a positive correlation between GFAP levels and TBI severity; therefore, GFAP can be used to assess mTBI severity and evaluate the need for neuroimaging with CT and MRI, predicting poor outcomes and the risk of developing cognitive and psychiatric disabilities [11]. Blood levels of GFAP peak within the first 24–48 h after mTBI, and the acute measures of blood GFAP in isolation or combined with UCH-L1 are susceptible to intracranial lesions in mTBI patients: this combination was recently approved by the FDA to reduce radiation exposure by CT [26]. Elevated UCH-L1 and GFAP measured within 12 h of injury indicate intracranial lesions requiring CT [12].
3.3. Markers of Axonal Injury
Neurofilament proteins (NFs) are the primary components of the neuronal cytoskeleton. Phosphorylated filaments interact with each other in order to increase neuronal stability. However, after TBI, there is an increase in intracellular calcium levels that activate various calcium-dependent enzymes such as proteases, calpains, and phosphatase calcineurin, leading to NFs dephosphorylation, proteolysis, dissociation, and release in the extracellular space, then to CSF and blood [11]. NFs are formed by three different polypeptide subunits: light (NF-L, 68 kDa), medium (NF-M, 160 kDa), and heavy (NF-H, 200 kDa) [27]. Evidence suggests that NF levels, and in particular NF-L levels, rise throughout the first few weeks (12 d) post-injury, accurately distinguishing patients with TBI from controls up to six months post-injury and, even more impressively, between patients with mild, moderate, and severe TBI at 30 d post-injury [12][24]. NFs are specific for neurons and axons and are not affected by body trauma or strenuous physical activity; therefore, their extra-neural detection indicates neural death and axonal disintegration and lasts for days after the trauma, predicting poor outcomes, CT lesions, and the occurrence of chronic morbidities and cognitive disability [11][25].
Myelin basic protein (MBP) is a oligodendroglial protein released in the blood following axonal damage; it is not specific for CNS injury, because peripheral nerve injury also increases MBP blood levels. Its release is delayed (1–3 days after injury), and the initial levels do not correlate with the GCS. MBP would be an inaccurate diagnostic and prognostic biomarker, unsuitable for emergency room screenings [11][25].
Tau protein is a microtubule-associated protein (MAP) expressed mainly in the neurons to stabilize axonal microtubules. Within the context of TBI, microtubules release tau in response to mechanical stress, proteolytic cleavage by calpains and caspases, and calcium-dependent protein kinase activation, resulting in decreased microtubule binding and increased tau phosphorylation [24]. TBI increases tau release in CSF, and CSF tau concentration positively correlates with TBI severity and poor outcomes. Serum tau protein peaks only two days after TBI, reflecting injury severity and predicting the clinical outcome. Nevertheless, some studies reported that serum tau does not correlate with CT lesions and cannot predict post-concussion syndrome. CSF tau is, therefore, a more accurate diagnostic and prognostic tool than serum tau [11]. However, the release of tau from extracranial sources and after physical activity may limit the utility of tau in the context of sports-related mTBI. In addition to measures of total tau, quantification of tau in its phosphorylated form (p-tau) has also recently shown encouraging results as an acute marker indicator of mTBI, with elevated plasma levels found within 24 h of injury [12].
3.4. Markers of Inflammation
Inflammation-associated proteins can function as blood mTBI biomarkers, becuase mTBI pathobiology is characterized by glial activation and release of proinflammatory cytokines [12]. Circulating cytokine changes appear to be restricted to the first few hours post-mTBI: interleukin-6 (IL-6) levels appear to be elevated within the first 6–8 h but return to control levels by 24–48 h after mTBI. Moreover, IL-6 was associated with CT and MRI findings and longer duration of symptoms after mTBI [28]. Interestingly, the temporal profile of IL-6 points to a distinctly different inflammatory profile in sports-related concussion (SRC) and military concussion versus the general unselected population with mTBI; athletes show early acute elevation (<8 h) with a return to baseline within 48 h, highlighting an earlier resolution of the inflammatory response in comparison with the general unselected population showing alterations lasting up to six months after injury. An explanation could be that the inflammatory response is milder in the relatively young and healthy athlete population than in the average mTBI patient [28][29][30]. Moreover, blood IL-1 receptor antagonist levels increase in the first few hours post-mTBI, remaining elevated for 24–48 h [29]. Other cytokines such as IL-8, IL-10, and TNF-α are excessively produced after TBI, but their correlation with injury severity and outcomes is yet to be confirmed; the best biomarker for mTBI is, therefore, IL-6 [11].
It should be emphasized that the inflammatory response is sensitive to age (immunosenescence leads to a higher basal level of inflammatory markers) [31], sex (women generally have milder neuroinflammatory responses after TBI compared with males), and prior brain injuries (it is believed that a brain injury might ‘prime’ microglia into a more active state influencing the inflammatory response) [32].
Studies of mTBI have been limited to measuring inflammatory markers in less invasive fluid compartments such as blood. However, the concentration of blood-based inflammatory markers is much lower than concentrations identified in the cerebrospinal fluid (CSF) [32].
Importantly, given that inflammatory-associated proteins are produced by cells throughout the body in response to any disease-causing cellular injury, they are not highly specific for TBI. Inflammatory markers may be better suited as part of a multiple biomarker panel, including markers of other pathophysiological processes post-TBI, also having potential for decisions regarding athletes’ return to play or for predicting neuropsychological outcomes following mTBI.
3.5. Other Markers
Extracellular vesicles (EVs) are emerging as biomarkers, as they can be secreted from all types of brain cells and exhibit specific markers on their surface. Intraluminal DNA, RNA, protein, and metabolites are indicators of the state of the cell of origin. The major pitfall in using EVs as biomarkers is their isolation: the presence of other components of biological fluid, including lipoproteins, chylomicrons, and microvesicles, interferes with the isolation process, and this, together with EVs’ nanoscale size and difficulties in separating particular sub-types, makes isolation a very challenging process [11].
MicroRNA abnormalities are also relevant to many neurodegenerative diseases and brain injuries such as TBI. Dysregulated levels correlate with impaired memory, learning, cognition, and neuropsychiatric disorders [33]. However, the current limitation to the use of miRNA biomarkers is their variable expression between different individuals; this high heterogeneity makes it difficult to determine the optimal cut-off values for using miRNA biomarkers for TBI diagnosis and prognosis [11].
Exosomes and miRNAs have recently gained considerable attention as promising biomarkers for TBI. However, despite the current knowledge of their potential, these biomarkers have not yet been optimized for clinical practice.
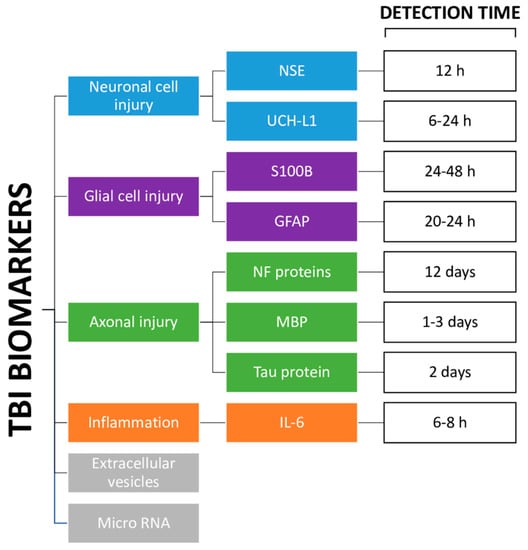
Figure 1. Diagram of the different types of TBI biomarkers. NSE: neuron-specific enolase [8]; UCH-L1: ubiquitin C-terminal hydrolase-L1 [8]; S100B: S100 calcium-binding protein B [9]; GFAP: glial fibrillary acidic protein [23]; NF: neurofilament proteins [9][21]; MBP: myelin basic protein [8][22]; Tau protein [8]; IL-6: interleukin-6 [25].
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2019, 130, 1080–1097.
- Holm, L.; Cassidy, J.D.; Carroll, L.; Borg, J. Summary of the WHO collaborating centre for neurotrauma task force on mild traumatic brain injury. J. Rehabil. Med. 2005, 37, 137–141.
- Stein, S.C.; Spettell, C.; Young, G.; Ross, S.E. Limitations of neurological assessment in mild head injury. Brain Inj. 1993, 7, 425–430.
- Easter, J.S.; Haukoos, J.S.; Meehan, W.P.; Novack, V.; Edlow, J.A. Will Neuroimaging Reveal a Severe Intracranial Injury in This Adult with Minor Head Trauma? JAMA 2015, 314, 2672.
- Shackford, S.R.; Wald, S.L.; Ross, S.E.; Cogbill, T.H.; Hoyt, D.B.; Morris, J.A.; Mucha, P.A.; Pachter, H.L.; Sugerman, H.J. The clinical utility of computed tomographic scanning and neurologic examination in the management of patients with minor head injuries. J. Trauma Inj. Infect. Crit. Care 1992, 33, 385–394.
- Langfitt, T.W.; Obrist, W.D.; Alavi, A.; Grossman, R.I.; Zimmerman, R.A.; Jaggi, J.; Uzzell, B.P.; Reivich, M.; Patton, D.R. Computerized tomography, magnetic resonance imaging, and positron emission tomography in the study of brain trauma. J. Neurosurg. 1986, 64, 760–767.
- Lee, B.; Newberg, A. Neuroimaging in traumatic brain imaging. Neurorx 2005, 2, 372–383.
- Eisele, A.; Hill-Strathy, M.; Michels, L.; Rauen, K. Magnetic Resonance Spectroscopy following Mild Traumatic Brain Injury: A Systematic Review and Meta-Analysis on the Potential to Detect Posttraumatic Neurodegeneration. Neurodegener. Dis. 2020, 20, 2–11.
- Lefevre-Dognin, C.; Cogné, M.; Perdrieau, V.; Granger, A.; Heslot, C.; Azouvi, P. Definition and epidemiology of mild traumatic brain injury. Neurochirurgie 2020, 67, 218–221.
- Danna-Dos-Santos, A.; Mohapatra, S.; Santos, M.; Degani, A.M. Long-term effects of mild traumatic brain injuries to oculomotor tracking performances and reaction times to simple environmental stimuli. Sci. Rep. 2018, 8, 4583.
- Ghaith, H.S.; Nawar, A.A.; Gabra, M.D.; Abdelrahman, M.E.; Nafady, M.H.; Bahbah, E.I.; Ebada, M.A.; Ashraf, G.M.; Negida, A.; Barreto, G.E. A Literature Review of Traumatic Brain Injury Biomarkers. Mol. Neurobiol. 2022, 59, 4141–4158.
- McDonald, S.J.; Shultz, S.R.; Agoston, D.V. The Known Unknowns: An Overview of the State of Blood-Based Protein Biomarkers of Mild Traumatic Brain Injury. J. Neurotrauma 2021, 38, 2652–2666.
- Helmrich, M.I.R.A.R.; Lingsma, H.F.; Turgeon, A.F.; Yamal, J.-M.; Steyerberg, E.W. Prognostic Research in Traumatic Brain Injury: Markers, Modeling, and Methodological Principles. J. Neurotrauma 2021, 38, 2502–2513.
- Foks, K.A.; Cnossen, M.C.; Dippel, D.W.; Maas, A.I.; Menon, D.; van der Naalt, J.; Steyerberg, E.W.; Lingsma, H.F.; Polinder, S.; on behalf of CENTER-TBI investigators and participants. Management of Mild Traumatic Brain Injury at the Emergency Department and Hospital Admission in Europe: A Survey of 71 Neurotrauma Centers Participating in the CENTER-TBI Study. J. Neurotrauma 2017, 34, 2529–2535.
- Stiell, I.G.; Wells, G.A.; Vandemheen, K.; Clement, C.; Lesiuk, H.; Laupacis, A.; McKnight, R.D.; Verbeek, R.; Brison, R.; Cass, D.; et al. The Canadian CT Head Rule for patients with minor head injury. Lancet 2001, 357, 1391–1396.
- Ingebrigtsen, T.; Romner, B.; Kock-Jensen, C. Scandinavian Guidelines for Initial Management of Minimal, Mild, and Moderate Head Injuries. J. Trauma Inj. Infect. Crit. Care 2000, 48, 760–766.
- Undén, J.; the Scandinavian Neurotrauma Committee (SNC); Ingebrigtsen, T.; Romner, B. Scandinavian guidelines for initial management of minimal, mild and moderate head injuries in adults: An evidence and consensus-based update. BMC Med. 2013, 11, 50.
- Stiell, I.; Clement, C.M.; Rowe, B.H.; Schull, M.; Brison, R.; Cass, D.; Eisenhauer, M.A.; McKnight, R.D.; Bandiera, G.; Holroyd, B.; et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in Patients with Minor Head Injury. JAMA 2005, 294, 1511–1518.
- Goodacre, S. Hospital admissions with head injury following publication of NICE guidance. Emerg. Med. J. 2008, 25, 556–557.
- Yates, D.; Aktar, R.; Hill, J. Assessment, investigation, and early management of head injury: Summary of NICE guidance. BMJ 2007, 335, 719–720.
- National Institute for Health and Care Excellence (NICE). Head Injury: Assessment and Early Management. Guidance. Available online: https://www.nice.org.uk/guidance/cg176 (accessed on 17 December 2022).
- Fabbri, A.; Servadei, F.; Marchesini, G.; Dente, M.; Iervese, T.; Spada, M.; Vandelli, A. Clinical Performance of NICE Recommendations versus NCWFNS Proposal in Patients with Mild Head Injury. J. Neurotrauma 2005, 22, 1419–1427.
- Servadei, F.; Teasdale, G.; Merry, G. Defining Acute Mild Head Injury in Adults: A Proposal Based on Prognostic Factors, Diagnosis, and Management. J. Neurotrauma 2001, 18, 657–664.
- Huibregtse, M.E.; Bazarian, J.J.; Shultz, S.R.; Kawata, K. The biological significance and clinical utility of emerging blood biomarkers for traumatic brain injury. Neurosci. Biobehav. Rev. 2021, 130, 433–447.
- Shahim, P.; Zetterberg, H. Neurochemical Markers of Traumatic Brain Injury: Relevance to Acute Diagnostics, Disease Monitoring, and Neuropsychiatric Outcome Prediction. Biol. Psychiatry 2021, 91, 405–412.
- FDA Authorizes Marketing of First Blood Test to Aid in the Evaluation of Concussion in Adults. 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-marketing-first-blood-test-aid-evaluation-concussion-adults (accessed on 16 December 2022).
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2018, 14, 577–589.
- Nitta, M.E.; Savitz, J.; Nelson, L.D.; Teague, T.K.; Hoelzle, J.B.; McCrea, M.A.; Meier, T.B. Acute elevation of serum inflammatory markers predicts symptom recovery after concussion. Neurology 2019, 93, e497–e507.
- Meier, T.B.; Huber, D.L.; Bohorquez-Montoya, L.; Nitta, M.E.; Savitz, J.; Teague, T.K.; Bazarian, J.J.; Hayes, R.L.; Nelson, L.D.; McCrea, M.A. A Prospective Study of Acute Blood-Based Biomarkers for Sport-Related Concussion. Ann. Neurol. 2020, 87, 907–920.
- Edwards, K.A.; Gill, J.M.; Pattinson, C.L.; Lai, C.; Brière, M.; Rogers, N.J.; Milhorn, D.; Elliot, J.; Carr, W. Interleukin-6 is associated with acute concussion in military combat personnel. BMC Neurol. 2020, 20, 209.
- Shaw, A.C.; Goldstein, D.R.; Montgomery, R.R. Age-dependent dysregulation of innate immunity. Nat. Rev. Immunol. 2013, 13, 875–887.
- Visser, K.; Koggel, M.; Blaauw, J.; van der Horn, H.J.; Jacobs, B.; van der Naalt, J. Blood-based biomarkers of inflammation in mild traumatic brain injury: A systematic review. Neurosci. Biobehav. Rev. 2021, 132, 154–168.
- Wang, W.; Kwon, E.J.; Tsai, L.-H. MicroRNAs in learning, memory, and neurological diseases: Figure 1. Learn. Mem. 2012, 19, 359–368.
More
Information
Subjects:
Neurosciences
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
735
Revisions:
2 times
(View History)
Update Date:
18 Apr 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No