A well-designed domestic cradle for babies should be technically feasible, meet aesthetic requirements, offer adequate functionality, and be safe to use. The technical feasibility of a cradle, like any other piece of furniture, is achieved by a properly prepared technical design
[1][2][3][4][5][6]. Furniture aesthetic design quality, including cradles, depends on many subjective factors, such as culture, fashion, and personal sense of aesthetics
[7][8]. A significant problem in the design of the cradle is effectively “incorporating” all human factors into the product. The application of psychological and physiological determinants to the products include human error resistance, proper functionality, enhanced safety of use, and comfort
[6].
Cradles can pose a threat to children and their safety. Falling out of the cradle has the highest injury risk rate for children ages 6 to 8 months
[9]. The materials used for cradle construction, wood, wood-derived materials, metals, plastic, adhesives, varnishes, and their emissions could pose a danger when used, such as improper cradle operation due to missing elements, overuse, or improper assembly. Although different furniture materials could be used in cradles, the significance of using safe materials is high since infants or babies are involved. The design requirements for cradles are listed in the EN 1130: 2019, ASTM F 2194–16e1: 2016, and ISO 2631-1: 1997 standards. These standards hold the minimum requirements for rigid element spacing, static loads, stability, foam pad thickness and dimensions, side height, mattress flatness, rocking angles, prohibit the use of accessible small parts, sharp edges, or self-assembly components, and include appropriate usage information.
2. The Proposed Categorization of Cradle Types Based on State of the Art and Types of Cradles
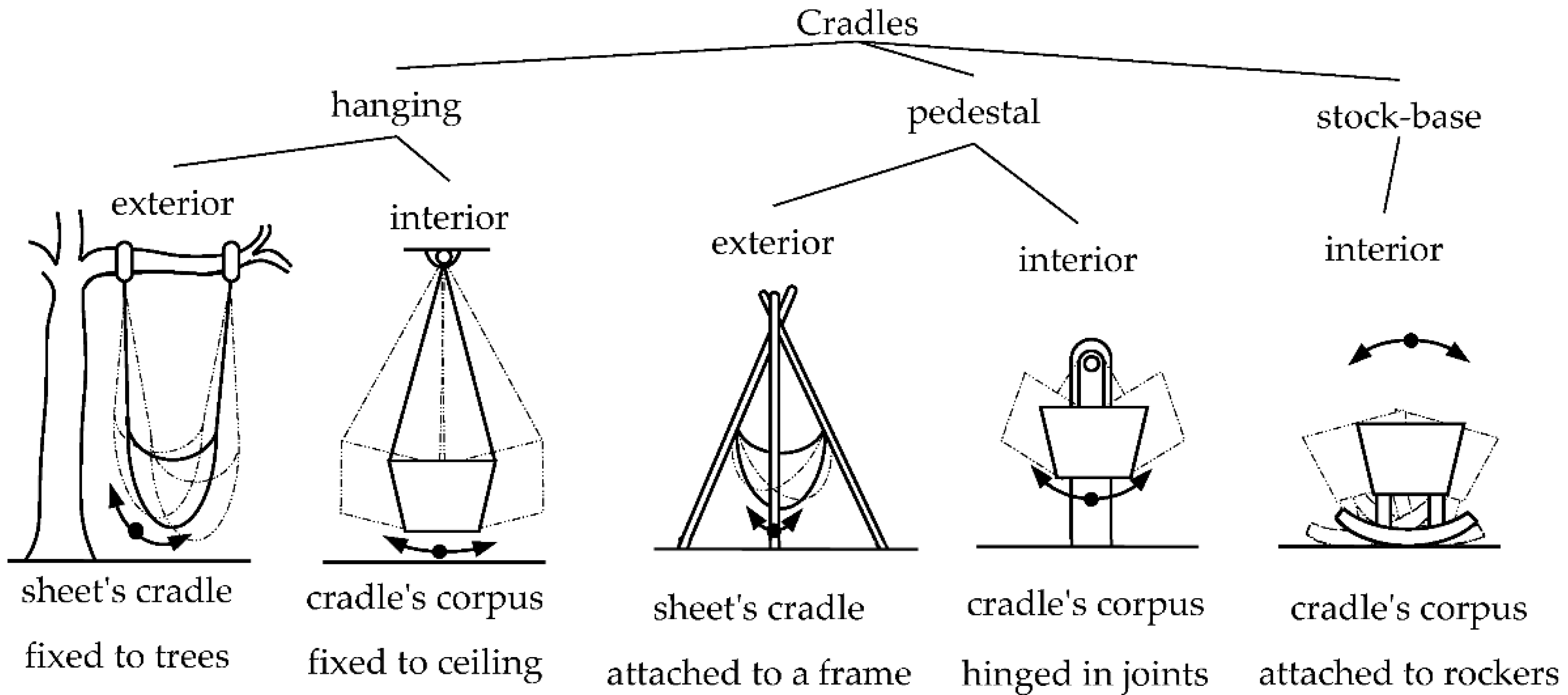
Understanding how cradles are typically designed is crucial to understanding how to improve existing designs and potential automation. Veselovský and Baďura analyzed the history of the development of cradle forms and distinguished three main categories: hanging cradles, pedestal cradles, and base cradles. The hanging cradles were hung inside or outside of the rooms. The pedestal cradles consisted of two subassemblies, a fixed pedestal, and a movable bed, while the base cradles had a “single-body” structure
[11]. The typology of cradles used in the 19th and the first half of the 20th century, according to Veselovský and Baďura, is presented in
Figure 1.
Figure 1. Types of the most common cradles in the 19th century and the first half of the 20th century (inspired by
[11]).
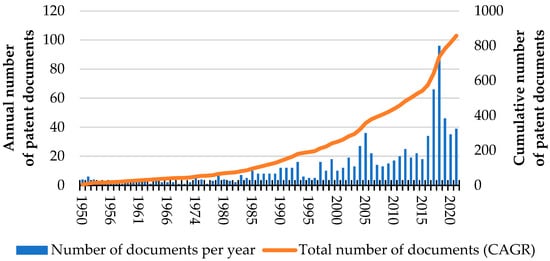
Contemporary cradles are furniture of various structures. There have been 967 patent documents filed within patent office databases relating to cradles for babies (TAC “cradle” and CPC classification code A47D9/02, searched by The Lens (Query: “class_cpc.symbol:A47D9\/* AND (title:(cradle) OR abstract:(cradle) OR claim:(cradle))”, range 1950–2021)). They represent 722 patent families. Figure 2 shows the annual increase in the number of patent documents related to cradles for babies.
Figure 2. The number of patents documents published between 1950 and 2021 with CPC classification code A47D9/02 (cradles for babies).
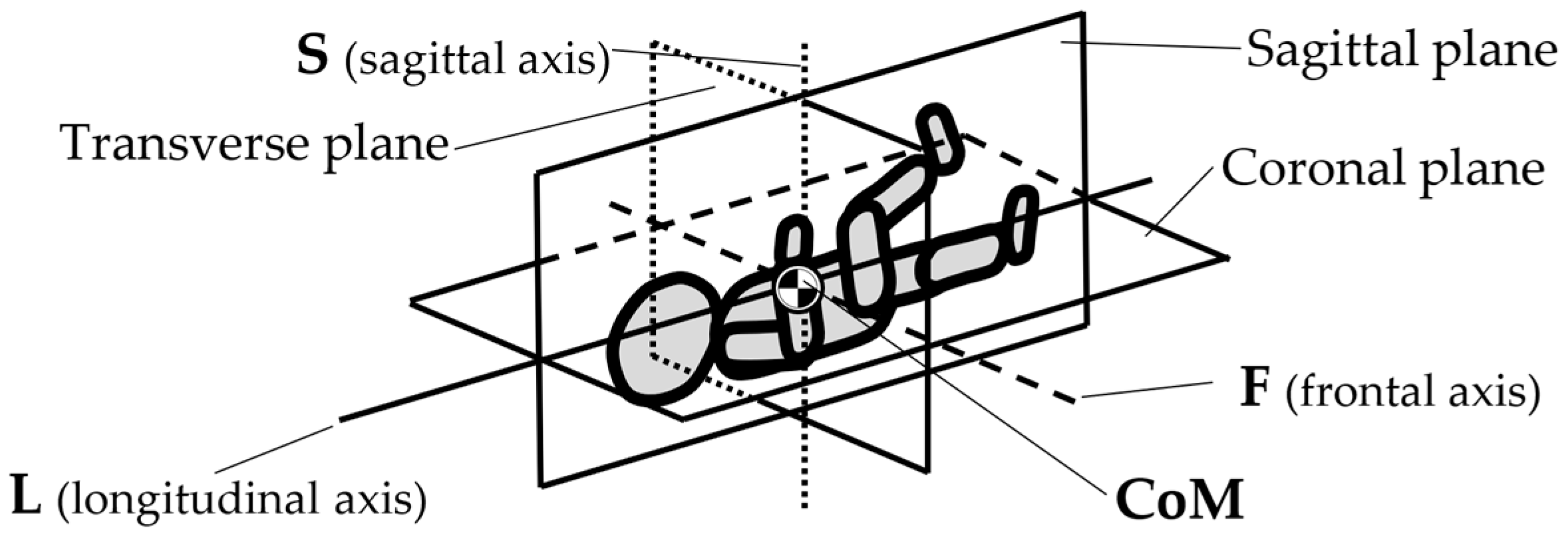
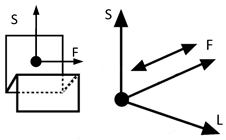
However, inventions do not always become genuine products. Therefore, the review and analysis of the furniture market would provide a strong basis for the constructional classification of cradles for children. The most useful from the point of view of mechanics is the classification of cradles related to the anatomical axes and planes of the human body. Anatomical planes introduced and named by Anderson (1892)
[12], and anatomical axes are shown in
Figure 3.
Figure 3. Anatomical planes and axes with the child’s Center of Mass (CoM) location.
The cardinal planes divide the body into equal portions. The cardinal sagittal plane (frontal axis) divides the body into the right and left parts. The cardinal coronal/frontal plane divides the body into anterior and posterior parts (sagittal axis). The cardinal transverse (horizontal) plane divides the body into superior and inferior parts (longitudinal axis). The axes of the body are related to the cardinal planes.
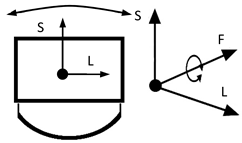
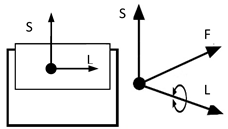
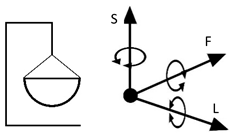
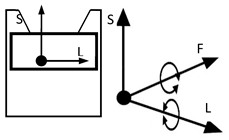
A review of state of the art in the field of cradles combined with the anatomical planes and reference axes allows for proposing a new classification of cradles. The classification of cradles, with photographs and characteristics of physical movement, is presented in Table 1.
In Table 1, a typical notation of the anatomical planes and directions of the human body is used, as shown in Figure 3. Table 1 shows that there are six types of cradles: (a) tilting—tilts forward and backward because it has two transverse rockers, (b) yawing—swivels left and right because it has two longitudinal rockers, (c) hammock cradle, (d) sarong cradle (or one pendulum cradle), (e) swing cradle (or two pendulum cradle) and (f) surging or four-pendulum cradle. According to the classification proposed in Table 1, cradles supply different possibilities for setting the human body in motion. They allow movement in selected planes and rotate along chosen body axes. This is summarized in Table 2.
Table 2. The type and number of degrees of freedom for each type of cradle.
| |
Longitudinal Axis (LA) |
Sagittal Axis (SA) |
Frontal Axis (FA) |
Transverse Plane (TP) |
Sagittal Plane (SP) |
Coronal Plane (CP) |
No. Degrees of Freedom (DoF) |
| Cradle a |
✓ |
(–) |
(–) |
✓ |
(–) |
(–) |
2 |
| Cradle b |
(–) |
(–) |
✓ |
(–) |
✓ |
(–) |
2 |
| Cradle c |
✓ |
(–) |
(–) |
✓ |
(–) |
(–) |
2 |
| Cradle d |
✓ |
✓ |
✓ |
✓ |
✓ |
(–) |
5 |
| Cradle e |
✓ |
(–) |
✓ (–) |
✓ |
✓ (–) |
(–) |
3 + 1 (–) |
| Cradle f |
✓ (–) |
(–) |
(–) |
(–) |
(–) |
✓ |
1 + 1 (–) |
As shown in
Table 2, the most common cradles (a–c) offer two independent movements (having two degrees of freedom). The Sarong cradle (d) is deemed the most dangerous
[13], with up to five degrees of freedom. The e-type cradle, suspended on two handles, has three degrees of freedom, plus one degree highly restricted. On the other hand, the least mobile is the four-pendulum cradle (f), which can move only in one plane and one direction.
The presented analysis shows that more degrees of freedom of the cradle’s corpus cause the highest risk of accidents (based on the Sarong cradle) and lead to an increased risk of a childs overstimulation.
4. Mechatronic Cradle Designs in the Scientific Literature
Many hours of rocking the cradle are arduous, and attempts have been made to mechanize this activity; an early example may be the invention of Marie R. Harper, La Mirada, and Maxine R. Blea, “Automatically rocking baby cradle”, US 3769641, 1973, or the invention of Gim Wong, “Automatic baby crib rocker” US 3952343, 1976. These hnological developments made it possible to construct mechatronic cradles, which relieve the parents of the child and eliminate the risk of spontaneous suffocation of a child left unattended in an excessively tilted cradle
[14][15]. The system for automatic monitoring and correction of the child’s body position, as described by Sudharsanan and Karthikeyan (2013), may be helpful for this purpose. The authors proposed placing an accelerometer on the child’s forehead to monitor its body position while sleeping. If an incorrect body position is detected, two servomotors can automatically correct it by tilting the cradle in the proper direction. Therefore, this cradle is designed to prevent SIDS
[16] automatically.
Offering solutions based on the Internet of Things (IoT) is relatively popular within the literature. With the developments of computer science, automatic adaptive systems are proposed using various sensors: sound, a child’s body temperature, the environment, air humidity, heart rate, or the amount of carbon dioxide in the exhaled air. Some sensors can also detect unusual baby movements or incorrect positions. The alarm signal can be generated by software that detects irregularities; the mechatronic cradle executive systems will activate and adjust the rocking parameters of the cradle, while the data acquisition system, using cloud techniques, archives the sensor readings. One of the first systems to detect and identify the types of crying from a baby was proposed by Chau-Kai-Hsieh and Chiung Lin, with the title of their invention filed in 1997 as “Baby Cry Recognizer” US 5668780. Table 3 lists numerous scientific publications describing the various concepts of remote supervision of automatic cradles.
Table 3. Swing Automation Systems in Mechatronic Cradles.
| Bibliographic Reference, Publication Year and No. of Citations in Scopus |
The Essence of the Concept |
| [17], 1997, 2 |
Pendulum swinging system. Swing parameters are in the range of 0.4–1 Hz and 0.36–3.6° |
| [18], 1998, 0 |
A swinging system with a noncontact magnetic driving force and various programmable swinging patterns. The band of frequency is limited from 0.4 Hz to 1 Hz, desired swing amplitude of ±0.0018 rad (±0.1°) |
| [19], 2000, 2 |
A “static” (nonadaptive) system of a remote swing program selection. Swing parameters within the range 45–50 cycles/min. were used (0.75–83 Hz). The system should not be operated for more than 30 min. |
| [20], 2009, 1 |
Motion sensors, a microphone for recording a baby’s cry, and a system that performs the movement with parameters selected by the algorithm. The cradle movement limits have not been specified. |
| [21], 2011, – |
A system detects the baby’s crying, then activates swinging and colored lights. Cradle movement limits the use of parameters that have not been specified (San Jose State University project, not indexed in Scopus). |
| [22], 2013, 4 |
A real-time baby sleeping position monitoring and correction system to avoid SIDS (the cradle motors prevent the baby against to sleep in its prone position). Cradle movement limits parameters have not been specified |
| [23], 2015, 6 |
Electrically driven cradle with infant cry recognition. The cradle drive uses resonance to reduce energy consumption during use. The desired movement parameters were not specified |
Automatic “intelligent” rocking programs, e.g., automatic start swinging when the baby cries, if the baby stops crying before the specified time, the cradle will stop if no alarm or message will be sent to baby caretakers. |
| [24], 2016, – |
Electric-powered cradle with baby cry recognition and mattress wet alarm. |
| [25], 2017, 1 |
The mother’s motion while sleeping with her baby on her lap was modeled and re-created in the cradle. A maximum speed of 0.04 m/s was adopted, and 2 m/s2 was the starting acceleration of the cradle. |
| [26], 2018, 0 |
The crying detection and classification (hungry, pain, sleepy, non-crying) system saves the collected data on the server and shares them via the mobile application. Three types of cradle operation: rocking, activating calming music, and alarm. The swing motion parameters have not been specified. |
| [27], 2019, 0 |
Infant cry detector and wet mattress sensor, then swinging or sending a message to caregivers. The swing motion parameters have not been specified. |
| [28], 2019, 30 |
Remote supervision of a child in the cradle using a laptop or smartphone. Infant crying detection and automatic swing activation. Supervise the humidity and temperature of the air and turn on the fan if it exceeds 28 °C. Possibility of remote switching on calming music. The cradle movement parameters used are not reported. |
| [29], 2020, 0 |
Automatic rocking when the baby cries (if the baby stops crying before the specified time has elapsed, the cradle will stop). Alarm or information to caregivers if the baby cries for more than a specific time and when the mattress is wet. Remote monitoring of infant body temperature, heart rate, air temperature, and humidity). Incubator for hospital and home use. |
| [30], 2020, 0 |
The web camera, humidity and temperature sensor, cry detector, remote monitoring, and automatic swing system. The swing motion parameters have not been specified. |
| [31], 2020, 1 |
When a cry is detected, the cradle can sway automatically or display a warning light when an abnormality is detected. The swing motion parameters haven’t been specified. |
| [32], 2020, 1 |
The user can control the cradle’s swing in manual mode and start music playing using a smartphone. The cradle detects crying, in the following, swings automatically, plays calming music, and send messages to the designated phone. |
| [33], 2021, 0 |
Android-based, remote monitoring system with a motor to swing the cradle, a cry detector, and a wet mattress sensor. |
| [34], 2021, 0 |
A remote monitoring system with sensors identifying a baby’s cry, body temperature, heart rate, and motion and posture status of the infant. The cradle offers electronic swinging, pleasant sounds, and other features, e.g., switching the fan on or off. |
| [35], 2022, 0 |
The remote monitoring system of a baby cry, body temperature, and wet mattress sensors. A cradle is equipped with pre-fitted air purification system. The cradle works based on the Internet of Things (IoT) principles and offers electronic swinging, pleasant sounds, and other features, e.g., self-activated automated eye-catching moving toys. |
| [36], 2022, 0 |
A machine learning remote monitoring system with baby’s vital signs and ambient parameters sensors. The system automatically swings the infant’s cradle. |
Table 4 shows that the number of scientific publications describing mechatronic cradle systems has increased in recent years. In addition to these publications, there have been attempts to reproduce the rocking movement in the mother’s arms through a mechanized cradle. They focused on the motion analysis of a mother’s embrace while rocking a baby, the development of an excitation apparatus
[23], and the rocking motion of the baby sleeping on the mother’s lap
[11]. A common feature of the systems described in
Table 4 included the detection and appropriate classification of the types of crying from a baby. Based on this, the device can run at an appropriate operating program
[37][38][39][40].
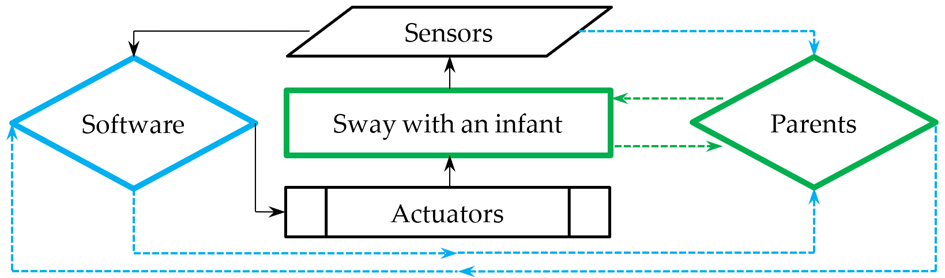
Figure 4 shows the operation scheme and data flow structures connected to the mechatronic cradles described in the scientific publications. Each cradle was equipped with actuators that put the cradle in sway mode. Built-in sensors monitored the temperature, air humidity, sound, body position, and mattress moisture. With the help of cameras, a video was transmitted directly to the parents’ devices such as their smartphones or laptops. The collected data was automatically sent to the system, which, thanks to the constantly updated data, was able to change the sway mode of the child or send a message to the parent at the time of danger. At the same time, after receiving information from the system, the parent could decide to introduce or not introduce changes in sway mode, turning on a light, fan, or calming music. A flow diagram of the mechatronic cradles described in Table 4 is shown in Figure 4.
Figure 4. The information flow diagram in mechatronic cradles (summary of Table 4).
The center of the diagram shown in Figure 4 represents the sway of an infant. The sway is set in motion through actuators. The parameters of the cradle’s movement and the baby’s current needs are read by sensors, and the entire system’s operation is managed by software. Parents can directly or indirectly supervise the work of the described system and the baby directly or remotely using its sensors (video, sound, and others). They can adjust the software signals by interrupting or changing their operations. The black arrows indicate the automatic flow of information between the mechatronic cradle and (IoT) elements. Blue arrows indicate the flow of information between the mechatronic devices, and the parents. Green arrows indicate the flow of information between the child and the parents.
5. Kinematics of the Gait of a Pregnant Woman: A Brief Review of the Literature and Basic Calculations
A fetus in intrauterine life is stimulated kinematically by the gait of the pregnant woman. The gait of a pregnant woman is modeled by changes in the position of the center of mass (CoM) within her body while walking at a comfortable speed, the so-called physiological. The first step in evaluating gait is to establish the value of the velocity of various body heights in the advanced pregnancy stage. Knowing the velocity value produced during walking makes it possible to compute the parameters of harmonic movement (amplitude and frequency) concerning the body’s center of gravity. Attaining these parameters allow ilding a cradle with a mechanically forced motion corresponding to the “anthropo-mechanical” parameters. According to Gedliczka and Pochopień, nonpregnant women between the ages of twenty and forty, with a height of 1.61 m, had an average speed of 1.49 m/s while walking
[41]. The angular range of motion within the joints of the lower limbs of a pregnant woman did not change significantly when compared to the studied control group; however, a change in the length of stride was observed by 3 to 4 cm shorter than the control.
[42]. The average total length of a pregnant woman’s right and left steps (in the third trimester) was 1.247 m, and the duration of one gait cycle was 1.086 s
[43].
The inverted pendulum model, a standard human gait model, can determine the approximate characteristics of the movement of the center of mass within the examined body
[44]. This movement follows a roulette described by the trochoid equation or a specific trochoid like a cycloid. The epicycloid represents the path of a point at the end of the radius on a wheel that rolls without skidding on a flat surface.
Figure 5 depicts a graphic representation of this movement.
Figure 5. The center of mass (CoM) of a walking pregnant woman with a fetus.
The cycloid is defined by two parametric Cartesian equations:
x=R ⋅ θ−r ⋅ sin(θ) and
z=z0−r ⋅ cos(θ). In the equations,
θ is the angle between the radius of the circle and the vertical direction,
R is the radius of the circle,
r is the distance of the point attached to the radius from the center of the circle, and
zo is the height of the center of the circle. The variables x and z define a point’s coordinates attached to the radius. The first derivative of the trajectory
θ corresponds to the angular velocity
ω of the cycloids
[44].
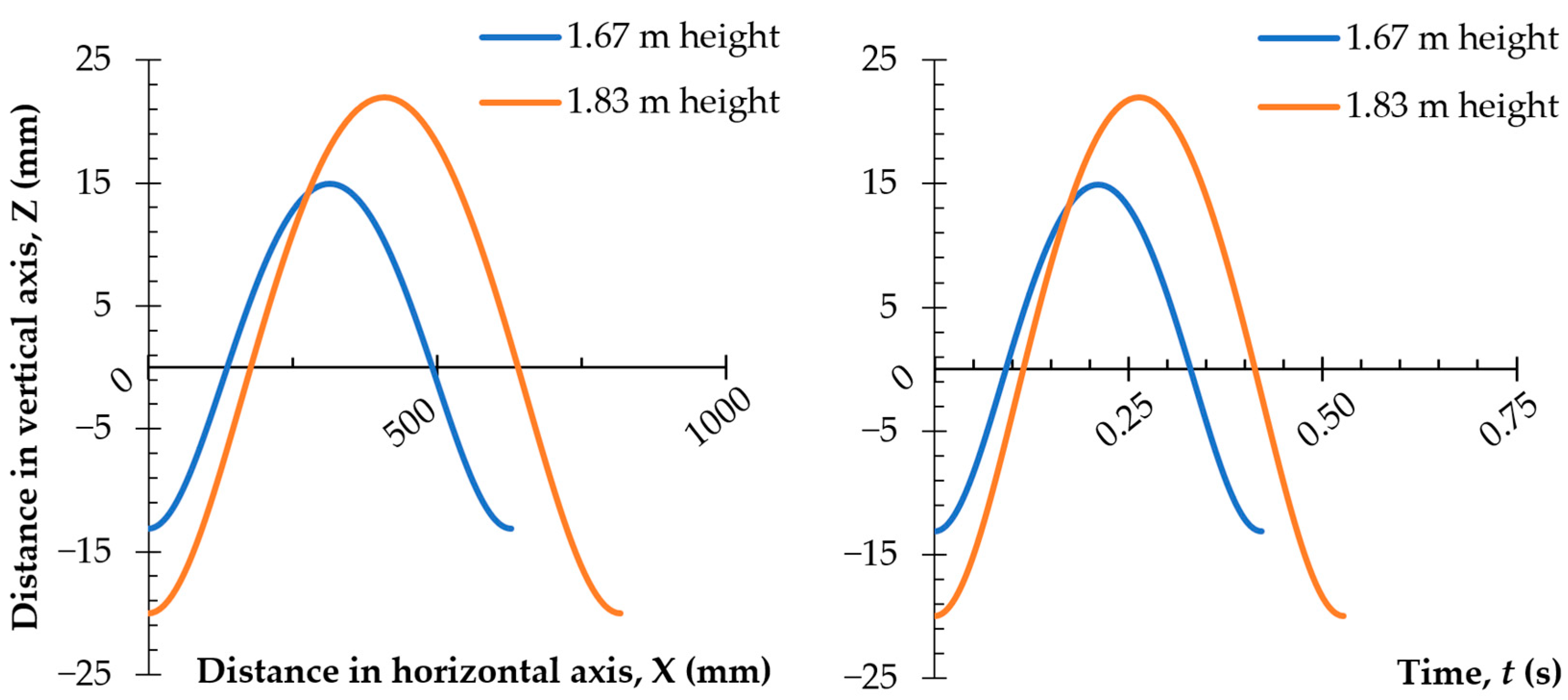
Considering the data provided by Carpentier
[44], a graph on the dependence of the vertical coordinate on the horizontal coordinate, at the center of gravity of two women, with two body heights was prepared (1.67 m and 1.83 m—
Figure 6). The dependence of the change in position of the center of mass (CoM) in time is shown in
Figure 6. The graphical interpretation of the cycloid equations based on the adopted constants is showed in
Table 6.
Figure 6. The calculated changes of the center of mass (CoM) for two women with different heights: dependent on the distance traveled and time.
Table 4. Data adopted in the cycloid equations.
| Height of the Woman (m) |
Radius of the Circle R (mm) |
Distance of the Point Attached to the Radius from the Center of the Circle r (mm) |
Height of the Center of the Circle zo (mm) |
| 1.67 |
100 |
14 |
0.91 |
| 1.83 |
130 |
21 |
1 |
The graphs presented in Figure 6 show that in a woman with a height of 1.67 m, whose step is about 600 mm, the coordinate position of the center of mass varied from −13 mm through +15 mm. This change occurred in 0.48 s, which translates into movement of the center of mass (CoM) at a frequency of about 2 Hz. The presented relationships make it possible to design the trajectory of cradle movement to correspond to the spatial positioning of the pelvis. The cradle could be equipped with a mechanism allowing for frequency fluctuations to be programmed according to the natural swing cycle of the baby in the womb while depending on the woman’s height and changes in the position of her body’s center of gravity.
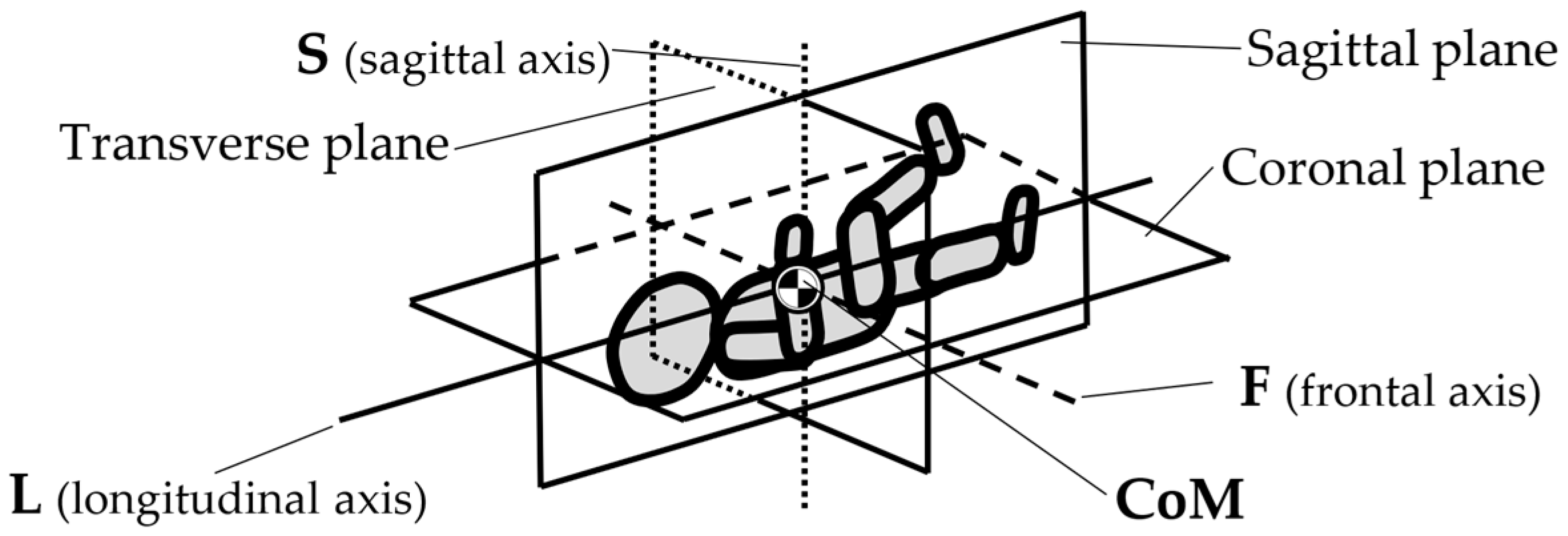
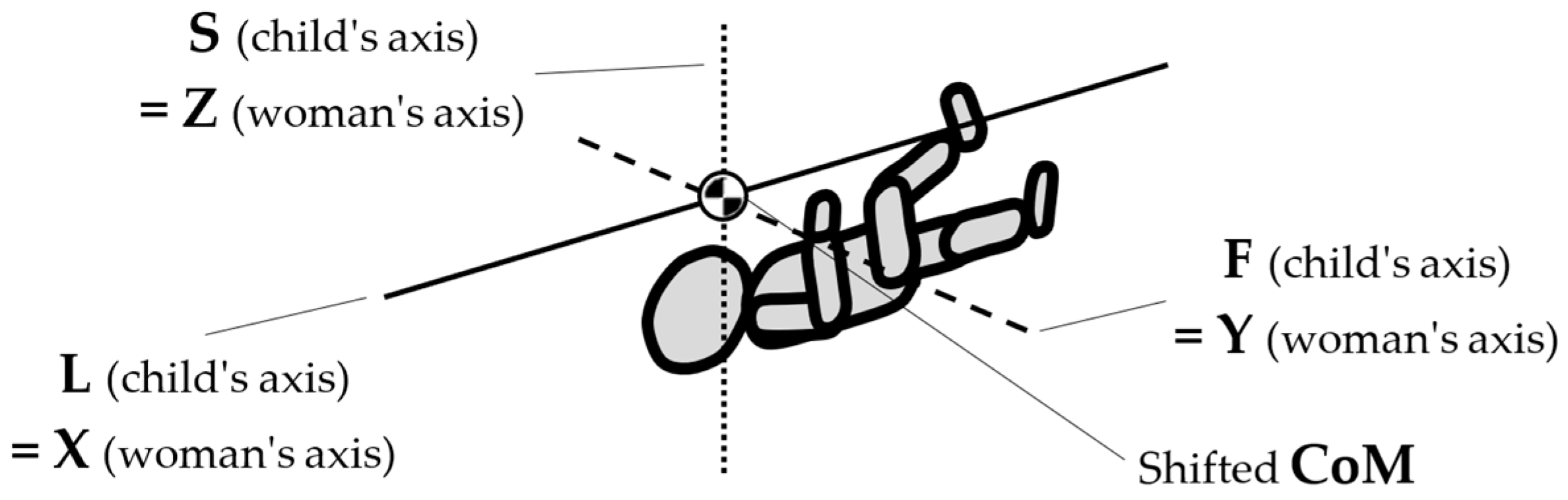
To map the changes in a walking woman’s CoM, and the child’s movement, the planes and anatomical axes of the child’s body within the cradle should be shifted so that their zero point coincides with the CoM of the pregnant woman. The shifted system of the anatomical childs axes is shown in Figure 7.
Figure 7. Shifted arrangement of child axes and anatomical planes.
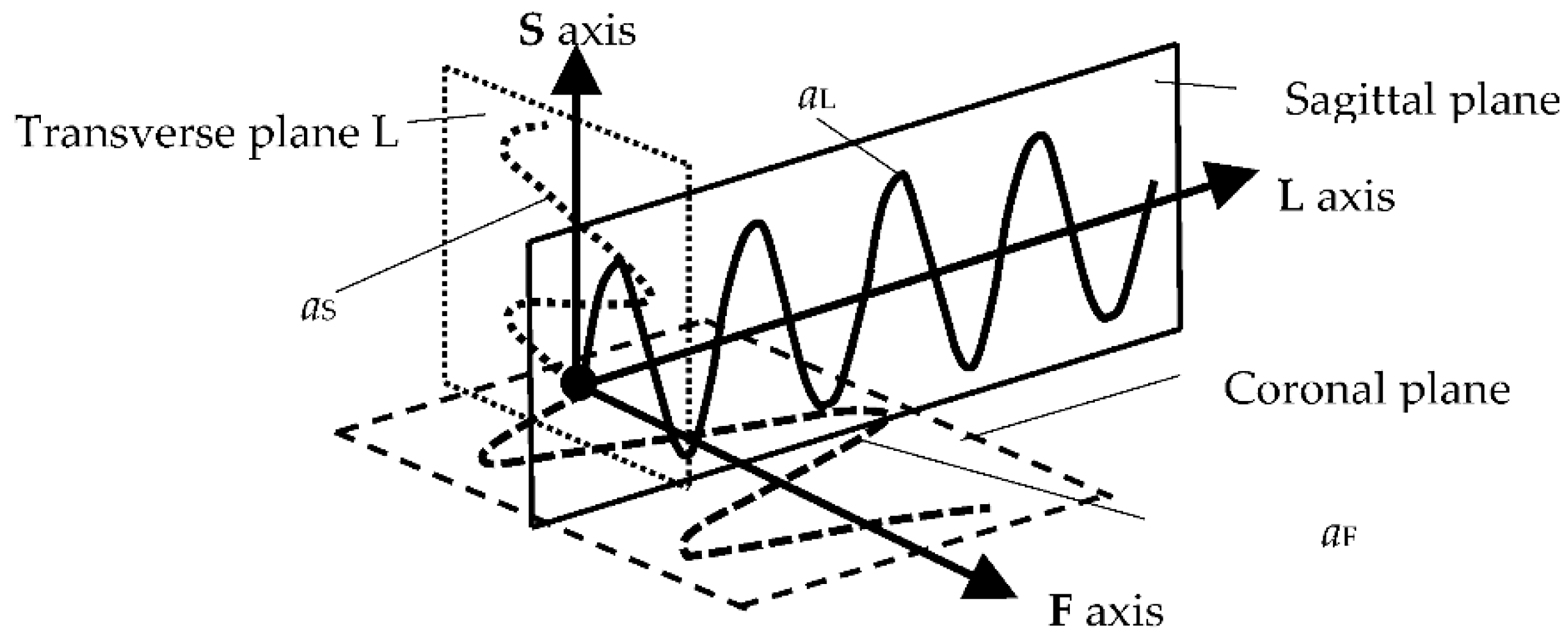
The characteristics of the anthropo-mechanical cradle motion are shown in
Figure 8. Schematically shown elements of the acceleration, within the mother’s gait, regarding her center of mass (CoM),
aL,
aF, and
aS, are acting in three orthogonal axes, L, F, and S (X, Y, and Z). This figure was prepared based on data provided by Jansen et al. in
Figure 1 in the reference
[45] and in association with
Figure 3,
Figure 5 and
Figure 7.
Figure 8. Schematic representation of the action of the accelerations aL, aF and aS acting in the three axes L, F, and S on the child during the mother’s gait.
The following insights for the design of anthropo-mechanical cradles are as mentioned:
-
When selecting the parameters of the movement of the anthropo-mechanical cradle, apart from the amplitude in the vertical axis (Z axis in mm) and the frequency (in Hz), it is worth taking into account the remaining parameters of the dynamics of the movement of the woman’s center of mass (CoM) while walking, i.e., amplitudes and accelerations acting on the three anatomical axes of the body (L, F, and S).
-
At each tilt, the directions of the accelerations aL, aF, and aS change in the cradle. The direction of the CoM acceleration vector changes only for the S (vertical) and F (transverse) axes during the mother’s gait. For the L axis, the direction of the acceleration vector is constant. Thus, the resultant movement of CoM is quite complex. It takes place simultaneously within the three axes L, F, and S. The challenge would be to obtain a cradle movement where the position of the fetus during pregnancy and the parameters of the physiological gait of a given mother would be correlated. It would then be possible to program the cradle to adjust to each child individually and imitate the movement of being in its mother’s womb. It seems that typical cradles (Table 3) do not best reflect the movement of the CoM within a pregnant woman’s gait. Therefore, a new solution for the cradle structure should be proposed.
-
The frequency of the cradle’s motion must not exceed the resonant frequency of the baby’s organs, as it could pose a danger to the child’s health. Fortunately, these frequencies are larger than the postulated range (up to 2 Hz). As is known, the resonant frequency of the human body ranges from 5 to 10 Hz—depending on the individual’s body structure and position—lying, standing, or sitting
[46]. However, excitations of a lower frequency can stimulate the abdominal organs to experience strong vibrations
[47].
The recommended rocking parameters of a child include an amplitude (
A) of 28 mm and a frequency (
f) of up to 2 Hz, which are confirmed in the literature. Byrne et al. studied the effects of rocking on 36 full-term infants (24–72 h of age) on the experimenter’s shoulder. When they used horizontal rocking movements, with 30 cycles per minute (
f = 2 Hz) and a duration of up to 3 min, they obtained the best effects of calming the child
[48]. Peak acceleration level (
amax) may be computed by using the formula:
amax=4π2 ⋅ f2 ⋅ A32 (m/s
2). Therefore, the recommended rocking motion parameters mentioned above result in
amax = 0.07 m/s
2. Vrugt and Pederson recommend
amax values between 0.025 and 0.075 m/s
2 [49].
Inappropriate motor stimulation, such as inharmonious shaking or rocking, can be fatal or cause permanent disability. Shaking can cause complications such as brain damage, cerebral palsy, hearing loss, blindness, learning difficulties, seizures, and paralysis
[50]. Babies between the ages of 2 and 4 months are most at risk of shaking injuries. Accidental stimulation leads to an emotional disturbance in the child. Rhythmic stimuli allow for the synchronization of rhythms, leading to the facilitation of selective attention and the learning of perception
[51]. At the time of birth, significant environmental changes occur, differing from what life has been in the womb of the baby’s mother. Increasing attention has been paid to environmental and ectopic changes, indicating a significant role in developmental and behavioral outcomes such as optimal growth and development
[52].
The calming effect of walking by the mother on children was reported in the literature. Esposito et al. monitored the responses of 12 healthy infants aged 1–6 months. The scientists wanted to compare holding a crying baby with carrying an infant while walking for 30 s or longer. The study found that the babies that were carried were more relaxed and soothed than the babies whose mothers sat and held them. Thus, maternal walking is more effective in calming infants than other non-rhythmic motions
[53]. Infant carrying is a biological norm for human caregiving and results in a carrying-induced calming response for the child
[54]. Carrying during walking is a well-known intuitive and multicultural mother’s reaction to a baby crying. The effectiveness of this effect has been confirmed by scientific research
[55]. Therefore, using motion parameters in the cradle that resemble the walking mother positively affects the infant without the risk of overstimulation.
6. Conclusions
The harmonic movement has a beneficial calming effect on normal developing babies and a beneficial therapeutic effect on premature babies. The literature cited of the article highlights that constant stimulation of babies’ vestibular system due to systematic rocking improves development and the formation of a restful and consistent sleep cycle. Thus, rocking allows for the transition from being awake to sleeping easier. However, using cradles could increase the risk of suffocation and injury if a limb gets stuck or the baby falls out. Therefore, cradles should meet the minimum requirements described in the standards cited in the Introduction.
Mechatronic cradles that mechanize a rocking movement have been described in the literature (usually having an added remote supervision function). However, such devices can be dangerous and may have excessive movement on the child. The information and calculations within the cited literature made it possible to use physiological movements that do not increase the risk of overstimulation; therefore, the parameters of this movement were calculated, and five innovative concepts of cradle design were proposed:
-
The harmonic movement has a beneficial effect on babies; in particular, rhythmic rocking of the cradle has a positive impact on the development of an infant’s brain and a beneficial therapeutic effect on premature babies. Cradle rocking can naturally link a baby’s two stages of life: when the fetus is rocked in the womb by the mother’s motion of locomotion and the period of independent walking.
-
A crucial component of a cradle’s design involves the safety requirements to prevent falls and entrapment. To avoid the risk of the child falling out: footholds in the cradles are not allowed, minimum side heights are strictly defined, and the maximum age of a child sleeping in the cradle is five months. An excessive tilt of the cradle greater than 10° should be avoided to prevent strangulation or suffocation risks.
-
The multidisciplinary literature review and kinematic analyses suggest that cradles should be classified from the point of view of the possibilities and limitations of a child’s rocking motion parameters and not from a view of the external forms. That is why researchers proposed a classification of cradles into six types, offering from 2 to 5 degrees of freedom in various configurations (tilting, yawing, hammock, Sarong, swing, and surging cradle).
-
Modern technology enables the design of cradle movement to include more thoughtful parameters and ensure the safety of the child. This includes calculating the approximate movement characteristics of the center of mass within the human body while in motion, as well as designing the limits of a cradle’s tilt to correspond with the directions and parameters of the spatial positions of the pelvis during human gait patterns.
-
Compared to mechanically driven cradles, it is preferable to use “anthropo-mechanical” cradle movements to prevent a child from being overstimulated. Child movement in an “anthropo-mechanical” cradle should be maintained within the parameters of the passive motion, and speed performed within the mother’s womb while walking can be considered safe. The movement parameters in such a safe cradle should be determined based on the mother’s height. According to the analysis, safe cradle movements could be achieved by having a vertical amplitude ranging from −13 to +15 mm and a frequency of up to 2 Hz. The frequencies of the cradle’s movement must not coincide with the resonant frequencies of the baby’s organs, as it can pose dangerous effects on the child’s health.
 +1 credit
+1 credit