Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Stefana Maria Moisa | -- | 1271 | 2022-12-02 09:19:52 | | | |
| 2 | Dean Liu | Meta information modification | 1271 | 2022-12-06 02:26:45 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Trandafir, L.M.; Moisa, S.M.; Vlaiculescu, M.V.; Butnariu, L.I.; Boca, L.O.; Constantin, M.M.L.; Lupu, P.M.; Brinza, C.; Temneanu, O.R.; Burlacu, A. Factors Influencing Insulin Pump Therapy Adherence in Children. Encyclopedia. Available online: https://encyclopedia.pub/entry/37847 (accessed on 24 June 2026).
Trandafir LM, Moisa SM, Vlaiculescu MV, Butnariu LI, Boca LO, Constantin MML, et al. Factors Influencing Insulin Pump Therapy Adherence in Children. Encyclopedia. Available at: https://encyclopedia.pub/entry/37847. Accessed June 24, 2026.
Trandafir, Laura Mihaela, Stefana Maria Moisa, Mihaela Victoria Vlaiculescu, Lacramioara Ionela Butnariu, Laura Otilia Boca, Maria Magdalena Leon Constantin, Paula Madalina Lupu, Crischentian Brinza, Oana Raluca Temneanu, Alexandru Burlacu. "Factors Influencing Insulin Pump Therapy Adherence in Children" Encyclopedia, https://encyclopedia.pub/entry/37847 (accessed June 24, 2026).
Trandafir, L.M., Moisa, S.M., Vlaiculescu, M.V., Butnariu, L.I., Boca, L.O., Constantin, M.M.L., Lupu, P.M., Brinza, C., Temneanu, O.R., & Burlacu, A. (2022, December 02). Factors Influencing Insulin Pump Therapy Adherence in Children. In Encyclopedia. https://encyclopedia.pub/entry/37847
Trandafir, Laura Mihaela, et al. "Factors Influencing Insulin Pump Therapy Adherence in Children." Encyclopedia. Web. 02 December, 2022.
Copy Citation
Several key factors might improve adherence to insulin pump therapy: efficient communication between care provider and patients (including home-based video-visits), continuous diabetes education, family support and parental involvement, as well as informational, practical assistance, and emotional support from the society.
type 1 diabetes mellitus
adherence
insulin pump therapy
pediatric population
1. Introduction
The past few decades came with a rise in the prevalence of chronic diseases in children, and one of the most prevalent chronic diseases in this age group is type 1 diabetes mellitus (T1D). T1D, which is also the most prevalent endocrine condition in children and teenagers, is brought on by an autoimmune response that targets pancreatic beta cells over the course of several months or years. As a result, insulin output declines, which can result in a partial or, more frequently, an absolute deficit. The patients must receive exogenous insulin for the remainder of their lives [1][2][3].
For patients and their caregivers, keeping the blood glucose level within the normal range can prove to be a challenge. This has served as motivation to find effective strategies to control T1D and prevent its consequences ever since insulin was discovered in 1921 [4]. The rapid development of diabetes technology over the past few decades includes continuous subcutaneous insulin infusion (CSII) as one of the most notable developments. The Diabetes Control and Complications Trial highlighted the value of rigorous therapy during childhood as it avoids and delays microvascular complications, despite the fact that the first insulin pump was created in the early 1970s [5]. This led to an increase in the popularity of the device.
Notably, following extensive research in the last decades on insulin delivery systems, the International Society for Pediatric and Adolescents Diabetes (ISPAD) advocated for insulin pump therapy for diabetes management in children of all ages [6]. Also, ISPAD recommended insulin pumps to improve glycemic controls, reduce the risk of chronic complications, and reduce episodes of hypoglycemia. In addition, real-time glucose sensors could be used to achieve better glycemic control [6].
Nevertheless, ISPAD guidelines highlighted some barriers that should be addressed in adopting device-based therapy for children with diabetes [6]. Adherence to insulin pump therapy was reported in 4% of cases, mainly due to pump wearability and anxiety. This issue could be overcome by adequate training by care providers, including progressive teaching from basic to advanced skills, and family support. Other barriers were linked to device-linked complications, such as malfunction, infusion failure, alarms, system occlusion, risk of ketoacidosis, and lipohypertrophy. Efficient communication and education offered by care providers and parents could be the solution to all these limitations, as insulin pump therapy benefits outweigh potential adverse events [6].
2. Adherence Obstacles
The American Diabetes Association classifies adherence barriers into three categories: patient, medication, and system barriers [7]. Good adherence to diabetes management is related to a better glycemic control. A meta-analysis that included 21 studies and 2429 adolescents concluded that better adherence is associated with better glycemic control, regardless of socioeconomic factors [8][9]. All the factors and barriers involved in achieving optimal adherence to insulin pumps are opportunities for intervention to increase glycemic control and, consequently, to increase the quality of life of young patients (Figure 1).
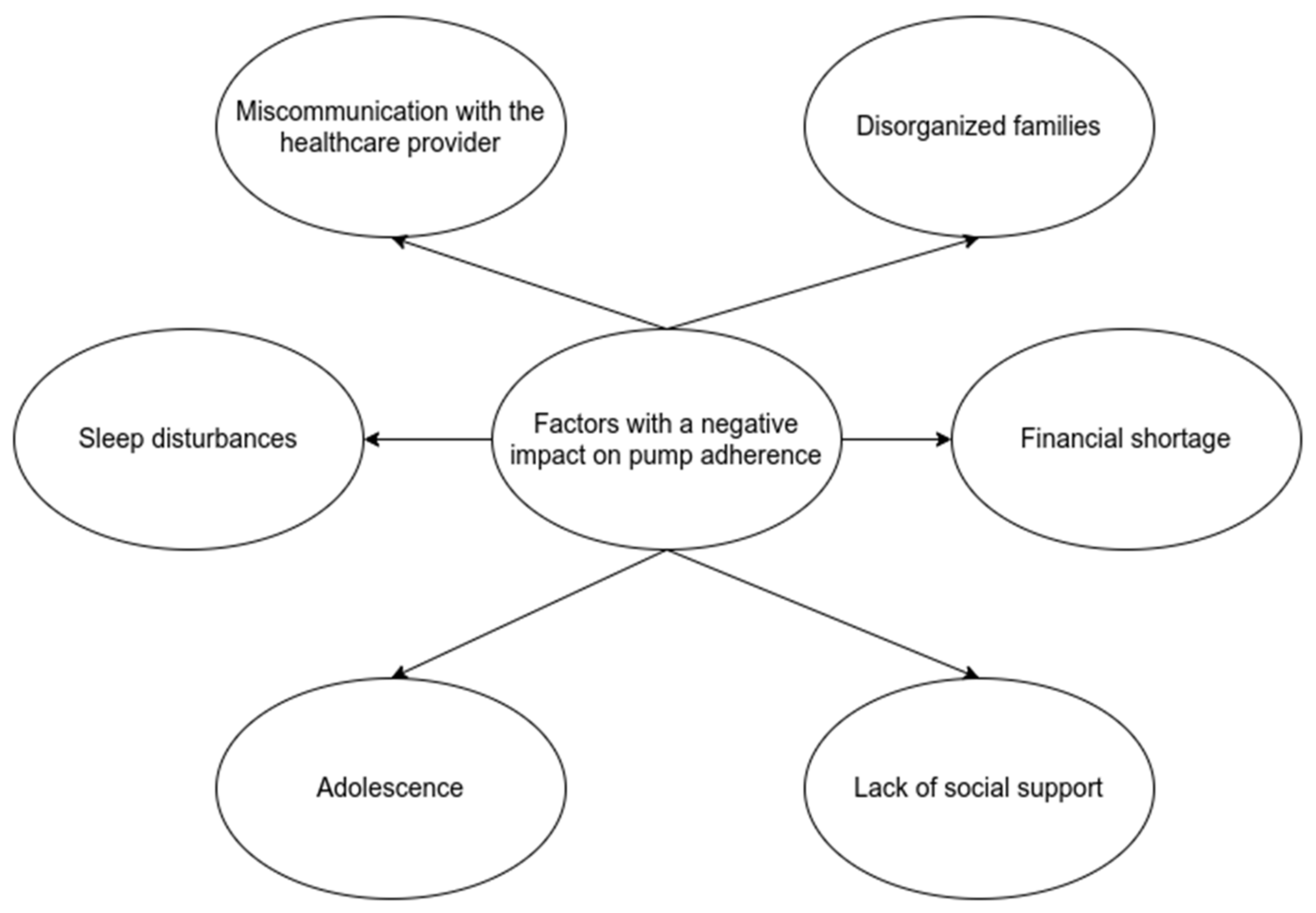
Figure 1. Factors with a negative impact on pump adherence.
3. Care Provider-Patient Relationship
When discussing with young patients and their parents, the term adherence is preferred over the term compliance. Efficient communication with doctors is part of successful therapy. Furthermore, a patient actively involved in making decisions regarding health issues has an increased adherence [7][10]. Studying the SEARCH cohort of young patients with type 1 diabetes, researchers found that 48% of families felt that the providers did not discuss questions and concerns, 43% reported that communication with the diabetologist was insufficient, and 48% complained about the costs [11].
Miscommunication and misunderstanding of the recommendations negatively influence the child’s adherence to treatment. This is an excellent intervention opportunity to increase glycemic control, and practitioners should try to eliminate communication barriers. In addition, closely related to communication is diabetes education. Studies emphasize the role of continuous diabetes education delivered by a multidisciplinary team, proving that it reduces hospitalization rates, emergencies, and complications [12].
A small non-randomized study including 57 children with T1D concluded that home-based video visits are an excellent intervention to decrease HbA1c levels and increase adherence to treatment [13]. Another study documented similar results, as telehealth improved glucose control in children and adolescents with type 1 diabetes [14]. Moreover, one study reported excellent social receptivity regarding telephone and virtual visits for routine pediatric diabetes care [15]. In addition, adherence is better when patients and their parents undergo insulin pump training in a pediatric endocrinology center [16]. Therefore, telemedicine visits with both, parents and adolescents are feasible and can improve adherence to insulin pump therapy and glycaemic control. Nevertheless, these data are limited to small observational studies and large randomized controlled trials are required to confirm the results.
4. Family Role
Regarding the pediatric population and its adherence to therapy, it is crucial to consider that children are not the only managers of their treatment. Parents, other family members, teachers, and friends play an essential and decisive role in optimal diabetes management. Cross-sectional and prospective studies reported that patients with parents who are supportive, cohesive, collaborative in solving the problems, and willing to share the tasks, with an authoritative style of parenting, have good results in maintaining optimal metabolic control [6][10][17].
On the other hand, patients with disorganized families, who must face conflicts with parents who are over or under-involved in a child’s disorder, are linked with poor treatment adherence [8][18]. In addition, conflictual family relationships lead to depression among young people, while a collaborative parent-child relationship is associated with better adherence to CSII therapy and emotional stability [6]. Another aspect consists of the socio-demographic characteristics of each family. For example, lower family income, ethnic and racial issues, and numerous members lead to less parental involvement in diabetes management with negative consequences. A low income is associated with less interaction between patients and doctors [19][20].
5. Adolescence Period
Adolescents’ demand to feel autonomous rises as they mature, and, as a result, they start to take on more responsibilities related to their illness. Although the transfer in responsibility is a realistic aim, it is also associated with decreased adherence once parental supervision is reduced, particularly if parental disengagement occurs too soon. Despite the fact that children become more independent from their families once they grow up, thus impacting adherence to therapy, carbohydrate counting has a fundamental role in glycaemic control improvement [21][22][23][24][25][26].
Psychosocial, emotional, and hormonal changes that occur during adolescence have an impact on therapeutic compliance. An ideal serum glucose level must be maintained despite insulin resistance brought on by hormonal changes. According to data from medical literature, the transition to self-care throughout adolescence is when glycemic control is least likely to be achieved. Only 21% of teenagers had HbA1c levels that were within the desired range [27]. Parental participation appears to improve glycemic control and treatment adherence for diabetes, but it relies on how their children interpret this association: if the involvement is viewed as invasive, adherence declines; if it is viewed as collaborative, adherence improves [17][27].
6. Social Support
Each child or adolescent’s social interactions are a crucial component of their lives, and they have an impact on how well they use their insulin pumps. Recently, social support for young individuals with diabetes has received more attention. There are three sorts of social support discussed: informational (advice), practical assistance, and emotional support. Young diabetics’ adherence to pump therapy is likely to worsen when they must deal with their peers’ unfavorable comments about managing their diabetes. Stigma is still a real issue that harms a child’s emotional well-being. However, although quantitative research links stigma with worsening glycemic control, qualitative investigations have produced mixed outcomes [6][28][29].
References
- Los, E.; Wilt, A.S. Diabetes mellitus type 1 in children. In StatPearls; Internet; StatPearls Publishing: Treasure Island, FL, USA, 2021.
- Westen, S.C.; Warnick, J.L.; Albanese-O’Neill, A.; Schatz, D.A.; Haller, M.J.; Entessari, M.; Janicke, D.M. Objectively measured adherence in adolescents with type 1 diabetes on multiple daily injections and insulin pump therapy. J. Pediatr. Psychol. 2019, 44, 21–31.
- Ergun-Longmire, B.; Clemente, E.; Vining-Maravolo, P.; Roberts, C.; Buth, K.; Greydanus, D.E. Diabetes education in pediatrics: How to survive diabetes. Dis. Mon. 2021, 67, 101153.
- Shalitin, S.; Phillip, M. The use of insulin pump therapy in the pediatric age group. Horm. Res. Paediatr. 2008, 70, 14–21.
- Berget, C.; Messer, L.H.; Forlenza, G.P. A clinical overview of insulin pump therapy for the management of diabetes: Past, present, and future of intensive therapy. Diabetes Spectr. 2019, 32, 194–204.
- Sherr, J.L.; Tauschmann, M.; Battelino, T.; de Bock, M.; Forlenza, G.; Roman, R.; Hood, K.K.; Maahs, D.M. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetes technologies. Pediatr. Diabetes 2018, 19, 302–325.
- Sarbacker, G.B.; Urteaga, E.M. Adherence to insulin therapy. Diabetes Spectr. 2016, 29, 166–170.
- Nevo-Shenker, M.; Shalitin, S. The Impact of Hypo-and Hyperglycemia on Cognition and Brain Development in Young Children with Type 1 Diabetes. Horm. Res. Paediatr. 2021, 94, 115–123.
- Hood, K.K.; Peterson, C.M.; Rohan, J.M.; Drotar, D. Association between adherence and glycemic control in pediatric type 1 diabetes: A meta-analysis. Pediatrics 2009, 124, e1171–e1179.
- Papadakis, J.L.; Anderson, L.M.; Garza, K.; Feldman, M.A.; Shapiro, J.B.; Evans, M.; Thompson, L.G.; Weissberg-Benchell, J. Psychosocial aspects of diabetes technology use: The child and family perspective. Endocrinol. Metab. Clin. 2020, 49, 127–141.
- Valenzuela, J.M.; Seid, M.; Waitzfelder, B.; Anderson, A.M.; Beavers, D.P.; Dabelea, D.M.; Dolan, L.M.; Imperatore, G.; Marcovina, S.; Reynolds, K. Prevalence of and disparities in barriers to care experienced by youth with type 1 diabetes. J. Pediatr. 2014, 164, 1369–1375.e1361.
- Haas, L.; Maryniuk, M.; Beck, J.; Cox, C.E.; Duker, P.; Edwards, L.; Fisher, E.B.; Hanson, L.; Kent, D.; Kolb, L. National standards for diabetes self-management education and support. Diabetes Care 2014, 37, S144–S153.
- Crossen, S.S.; Marcin, J.P.; Qi, L.; Sauers-Ford, H.S.; Reggiardo, A.M.; Chen, S.T.; Tran, V.A.; Glaser, N.S. Home visits for children and adolescents with uncontrolled type 1 diabetes. Diabetes Technol. Ther. 2020, 22, 34–41.
- Döğer, E.; Bozbulut, R.; Soysal Acar, A.; Ercan, Ş.; Kılınç Uğurlu, A.; Akbaş, E.D.; Bideci, A.; Çamurdan, O.; Cinaz, P. Effect of Telehealth System on Glycemic Control in Children and Adolescents with Type 1 Diabetes. J. Clin. Res. Pediatr. Endocrinol. 2019, 11, 70–75.
- Fung, A.; Irvine, M.; Ayub, A.; Ziabakhsh, S.; Amed, S.; Hursh, B.E. Evaluation of telephone and virtual visits for routine pediatric diabetes care during the COVID-19 pandemic. J. Clin. Transl. Endocrinol. 2020, 22, 100238.
- Cespedes, C.; Pavia, M.; Forero, C.; Coll, M.; Duran, P. Follow-up of Patients with Type 1 Diabetes Mellitus who Underwent Insulin Pump Training in a Pediatric Endocrinology Center. Proc. Horm. Res. Paediatr. 2019, 92, 20.
- Perlberg, M.; Katz, I.; Loewenthal, N.; Kahil, N.; Haim, A.; Chechik, T.; Hershkovitz, E. The role of autonomy-supportive parenting in the competence, adherence and glycemic control of adolescents with type 1 diabetes. Diabetes Res. Clin. Pract. 2021, 173, 108679.
- Fox, D.A.; Bone, J.N.; Keidar, S.; Amed, S. Family conflict in type 1 diabetes: Who is at risk? Pediatr. Diabetes 2020, 21, 1575–1582.
- Helgeson, V.S.; Vaughn, A.K.; Seltman, H.; Orchard, T.; Libman, I.; Becker, D. Featured article: Trajectories of glycemic control over adolescence and emerging adulthood: An 11-year longitudinal study of youth with type 1 diabetes. J. Pediatr. Psychol. 2018, 43, 8–18.
- Snyder, L.; Stafford, J.; Dabelea, D.; Divers, J.; Imperatore, G.; Law, J.; Lawrence, J.; Pihoker, C.; Mayer-Davis, E. Socio-economic, demographic, and clinical correlates of poor glycaemic control within insulin regimens among children with type 1 diabetes: The SEARCH for diabetes in youth study. Diabet. Med. 2019, 36, 1028–1036.
- Spaans, E.; Kleefstra, N.; Groenier, K.H.; Bilo, H.J.G.; Brand, P.L.P. Adherence to insulin pump treatment declines with increasing age in adolescents with type 1 diabetes mellitus. Acta Paediatr. 2020, 109, 134–139.
- Palmer, D.L.; Berg, C.A.; Butler, J.; Fortenberry, K.; Murray, M.; Lindsay, R.; Donaldson, D.; Swinyard, M.; Foster, C.; Wiebe, D.J. Mothers’, fathers’, and children’s perceptions of parental diabetes responsibility in adolescence: Examining the roles of age, pubertal status, and efficacy. J. Pediatr. Psychol. 2009, 34, 195–204.
- Wiebe, D.J.; Chow, C.M.; Palmer, D.L.; Butner, J.; Butler, J.M.; Osborn, P.; Berg, C.A. Developmental processes associated with longitudinal declines in parental responsibility and adherence to type 1 diabetes management across adolescence. J. Pediatr. Psychol. 2014, 39, 532–541.
- King, P.S.; Berg, C.A.; Butner, J.; Butler, J.M.; Wiebe, D.J. Longitudinal trajectories of parental involvement in Type 1 diabetes and adolescents’ adherence. Health Psychol. 2014, 33, 424–432.
- Goethals, E.R.; Oris, L.; Soenens, B.; Berg, C.A.; Prikken, S.; Van Broeck, N.; Weets, I.; Casteels, K.; Luyckx, K. Parenting and Treatment Adherence in Type 1 Diabetes Throughout Adolescence and Emerging Adulthood. J. Pediatr. Psychol. 2017, 42, 922–932.
- Silva, K.; Miller, V.A. The Role of Cognitive and Psychosocial Maturity in Type 1 Diabetes Management. J. Adolesc. Health 2019, 64, 622–630.
- Datye, K.A.; Moore, D.J.; Russell, W.E.; Jaser, S.S. A review of adolescent adherence in type 1 diabetes and the untapped potential of diabetes providers to improve outcomes. Curr. Diabetes Rep. 2015, 15, 51.
- Peters, L.W.; Nawijn, L.; van Kesteren, N. How adolescents with diabetes experience social support from friends: Two qualitative studies. Scientifica 2014, 2014, 415849.
- Aiello, E.M.; Deshpande, S.; Özaslan, B.; Wolkowicz, K.L.; Dassau, E.; Pinsker, J.E.; Doyle III, F.J. Review of automated insulin delivery systems for individuals with type 1 diabetes: Tailored solutions for subpopulations. Curr. Opin. Biomed. Eng. 2021, 19, 100312.
More
Information
Subjects:
Pediatrics
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.1K
Revisions:
2 times
(View History)
Update Date:
06 Dec 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No