 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Foteini Christidi | -- | 2459 | 2022-11-23 09:37:20 | | | |
| 2 | Lindsay Dong | Meta information modification | 2459 | 2022-11-23 10:04:52 | | |
Video Upload Options
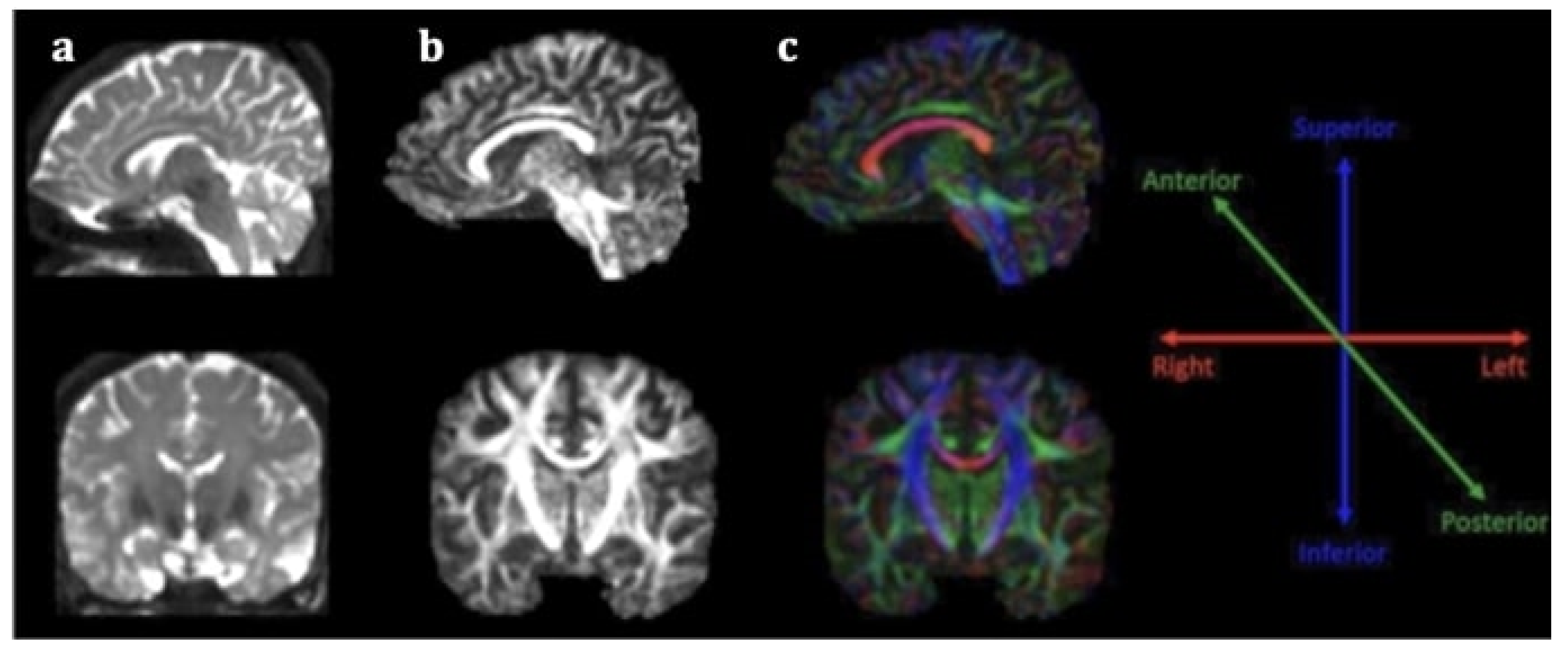
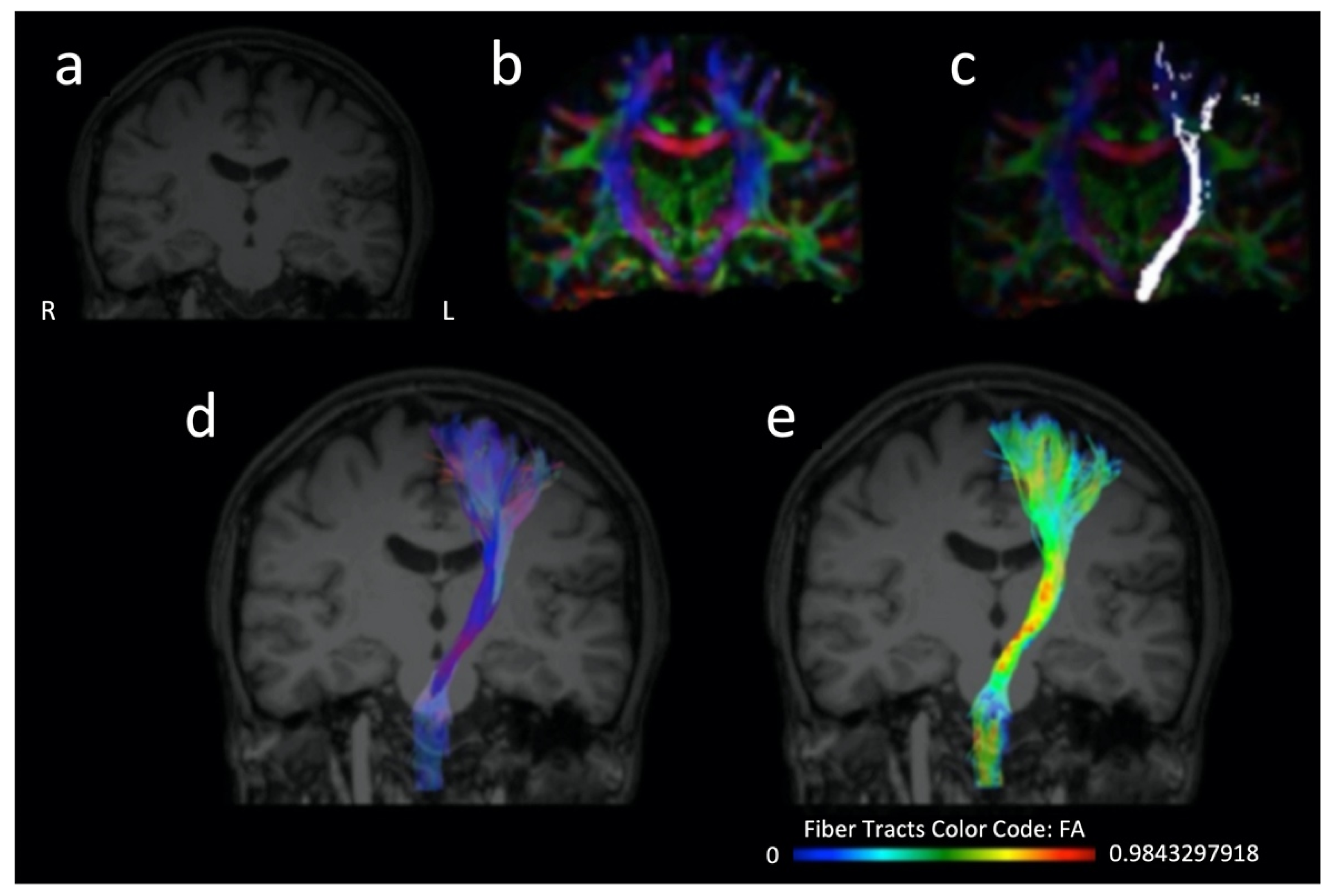
Clinical manifestation of stroke is characterized by great diversity, ranging from minor disability to considerable neurological impairment interfering with activities of daily living and even death. Prognostic ambiguity has stimulated the interest for implementing stroke recovery biomarkers, including those provided by structural neuroimaging techniques, i.e., diffusion tensor imaging (DTI) and tractography for the study of white matter (WM) integrity. Diffusion tensor imaging (DTI) is an extension of magnetic resonance imaging (MRI) for in vivo mapping of white matter (WM) directionality and organization, allowing the qualitative and quantitative evaluation of major WM tracts and their microstructural integrity. DTI is based on the random diffusion of water molecules. Research on DTI metrics as stroke outcome biomarker is not limited to the acute and subacute phases, as it is also implemented on chronic stroke patients. Direct visualization of long tracts and their potential disruption provides insight into pathogenesis of functional deficits in stroke survivors as well as compensatory mechanisms on a microstructural level. Such knowledge may elucidate which group of patients is most likely to benefit from rehabilitation, and even help personalize treatment plans after the acute stroke phase according to each individual’s needs.
1. Introduction
Clinical manifestation of stroke is characterized by great diversity, ranging from minor disability to considerable neurological impairment interfering with activities of daily living (ADL) and even causing death. Prognostic ambiguity has stimulated an interest in implementing stroke recovery biomarkers. Ideally, prognostic markers hold high sensitivity and specificity, enabling appropriate management of healthcare resources and individualization of rehabilitation treatments. Efficiency of the selected biomarker is also based on its capacity to accurately depict underlying mechanisms of disease. Moreover, it should be non-invasive, readily accessible to patients and clinicians, easily interpreted by physicians, reproducible, and cost-effective [1][2].
2. Diffusion Tensor Imaging as a Prognostic Tool for Recovery in Acute and Hyperacute Stroke
2.1. Prediction of Recovery Using Different DTI Parameters in Studies with Ischemic Cohorts: The Role of FA
2.2. Prediction of Recovery Using Different DTI Parameters in Studies with Ischemic Cohorts: The Role of the FA Ratio
With regards to the FA ratio (rFA), Ali and colleagues [19] investigated 21 patients and demonstrated that an FA ratio between the affected and unaffected side under 0.8 at admission was associated with deficient motor recovery at discharge. Additionally, they visualized WM tracts using DTI tractography and found that patients with whole involvement of pyramidal tract exhibited higher NIHSS at discharge compared with the groups with intact and partial involvement.
2.3. Prediction of Recovery Using Different DTI Parameters in Studies with Ischemic Cohorts: The Role of MD
2.4. Prediction of Recovery Using Different DTI Parameters in Studies with Ischemic Cohorts: The Role of AD
2.5. Prediction of Recovery Using Different DTI Parameters in Studies with Ischemic Cohorts: The Role of Fiber Number Ratio
2.6. Prediction of Recovery Using Different DTI Parameters in Studies with Hemorrhagic Cohorts: The Role of FA
2.7. Prediction of Recovery Using Different DTI Parameters in Studies with Hemorrhagic Cohorts: The Role of FA Ratio
2.8. Prediction of Recovery Using Different DTI Parameters in Studies with Hemorrhagic Cohorts: The Role of Qualitative Assessment of CST Integrity
2.9. Prediction of Recovery Using Different DTI Parameters in Studies with Both Ischemic and Hemorrhagic Cohorts: The Role of FA and the FA Ratio
3. Conclusions
References
- Karatzetzou, S.; Tsiptsios, D.; Terzoudi, A.; Aggeloussis, N.; Vadikolias, K. Transcranial magnetic stimulation implementation on stroke prognosis. Neurol. Sci. 2022, 43, 873–888.
- Gkantzios, A.; Tsiptsios, D.; Karatzetzou, S.; Kitmeridou, S.; Karapepera, V.; Giannakou, E.; Vlotinou, P.; Aggelousis, N.; Vadikolias, K. Stroke and Emerging Blood Biomarkers: A Clinical Prospective. Neurol. Int. 2022, 14, 65.
- Moura, L.M.; Luccas, R.; de Paiva, J.P.Q.; Amaro, E., Jr.; Leemans, A.; Leite, C.D.C.; Otaduy, M.C.G.; Conforto, A.B. Diffusion Tensor Imaging Biomarkers to Predict Motor Outcomes in Stroke: A Narrative Review. Front. Neurol. 2019, 10, 445.
- Mori, S.; Zhang, J. Principles of diffusion tensor imaging and its applications to basic neuroscience research. Neuron 2006, 51, 527–539.
- Chung, H.W.; Chou, M.C.; Chen, C.Y. Principles and limitations of computational algorithms in clinical diffusion tensor MR tractography. AJNR Am. J. Neuroradiol. 2011, 32, 3–13.
- Winklewski, P.J.; Sabisz, A.; Naumczyk, P.; Jodzio, K.; Szurowska, E.; Szarmach, A. Understanding the Physiopathology Behind Axial and Radial Diffusivity Changes-What Do We Know? Front. Neurol. 2018, 9, 92.
- Jang, S.H. The corticospinal tract from the viewpoint of brain rehabilitation. J. Rehabil. Med. 2014, 46, 193–199.
- Jang, S.H. The role of the corticospinal tract in motor recovery in patients with a stroke: A review. NeuroRehabilitation 2009, 24, 285–290.
- Puig, J.; Blasco, G.; Schlaug, G.; Stinear, C.M.; Daunis, I.E.P.; Biarnes, C.; Figueras, J.; Serena, J.; Hernandez-Perez, M.; Alberich-Bayarri, A.; et al. Diffusion tensor imaging as a prognostic biomarker for motor recovery and rehabilitation after stroke. Neuroradiology 2017, 59, 343–351.
- Bhasin, A.; Srivastava, P.; Kumaran, S.S. Correlation of DTI-Derived Measures to Therapy-Mediated Recovery after Stroke: Preliminary Findings. Neurol. India 2021, 69, 1210–1216.
- Alegiani, A.C.; MacLean, S.; Braass, H.; Siemonsen, S.; Gerloff, C.; Fiehler, J.; Cho, T.H.; Derex, L.; Hermier, M.; Berthezene, Y.; et al. Comprehensive analysis of early fractional anisotropy changes in acute ischemic stroke. PLoS ONE 2017, 12, e0188318.
- Berndt, M.T.; Purner, D.; Maegerlein, C.; Wunderlich, S.; Friedrich, B.; Zimmer, C.; Sepp, D.; Kaesmacher, J.; Boeckh-Behrens, T. Basal Ganglia versus Peripheral Infarcts: Predictive Value of Early Fiber Alterations. AJNR Am. J. Neuroradiol. 2021, 42, 264–270.
- Xia, Y.; Huang, G.; Quan, X.; Qin, Q.; Li, H.; Xu, C.; Liang, Z. Dynamic Structural and Functional Reorganizations Following Motor Stroke. Med. Sci. Monit. 2021, 27, e929092.
- Mahmoud, B.E.; Mohammad, M.E.; Serour, D.K. What can DTI add in acute ischemic stroke patients? Egypt. J. Radiol. Nucl. Med. 2019, 50, 67.
- Liu, G.; Dang, C.; Chen, X.; Xing, S.; Dani, K.; Xie, C.; Peng, K.; Zhang, J.; Li, J.; Zhang, J.; et al. Structural remodeling of white matter in the contralesional hemisphere is correlated with early motor recovery in patients with subcortical infarction. Restor. Neurol. Neurosci. 2015, 33, 309–319.
- Takenobu, Y.; Hayashi, T.; Moriwaki, H.; Nagatsuka, K.; Naritomi, H.; Fukuyama, H. Motor recovery and microstructural change in rubro-spinal tract in subcortical stroke. Neuroimage Clin. 2014, 4, 201–208.
- Keser, Z.; Sebastian, R.; Hasan, K.M.; Hillis, A.E. Right Hemispheric Homologous Language Pathways Negatively Predicts Poststroke Naming Recovery. Stroke 2020, 51, 1002–1005.
- Forkel, S.J.; de Schotten, M.T.; Dell’Acqua, F.; Kalra, L.; Murphy, D.G.; Williams, S.C.; Catani, M. Anatomical predictors of aphasia recovery: A tractography study of bilateral perisylvian language networks. Brain 2014, 137, 2027–2039.
- Ali, G.G.; Elhameed, A.M.A. Prediction of motor outcome in ischemic stroke involving the pyramidal tract using diffusion tensor imaging. Egypt. J. Radiol. Nucl. Med. 2012, 43, 25–31.
- Liu, G.; Guo, Y.; Dang, C.; Peng, K.; Tan, S.; Xie, C.; Xing, S.; Zeng, J. Longitudinal changes in the inferior cerebellar peduncle and lower limb motor recovery following subcortical infarction. BMC Neurol. 2021, 21, 320.
- Etherton, M.R.; Wu, O.; Giese, A.K.; Lauer, A.; Boulouis, G.; Mills, B.; Cloonan, L.; Donahue, K.L.; Copen, W.; Schaefer, P.; et al. White Matter Integrity and Early Outcomes After Acute Ischemic Stroke. Transl. Stroke Res. 2019, 10, 630–638.
- Moulton, E.; Amor-Sahli, M.; Perlbarg, V.; Pires, C.; Crozier, S.; Galanaud, D.; Valabregue, R.; Yger, M.; Baronnet-Chauvet, F.; Samson, Y.; et al. Axial Diffusivity of the Corona Radiata at 24 Hours Post-Stroke: A New Biomarker for Motor and Global Outcome. PLoS ONE 2015, 10, e0142910.
- Moulton, E.; Magno, S.; Valabregue, R.; Amor-Sahli, M.; Pires, C.; Lehericy, S.; Leger, A.; Samson, Y.; Rosso, C. Acute Diffusivity Biomarkers for Prediction of Motor and Language Outcome in Mild-to-Severe Stroke Patients. Stroke 2019, 50, 2050–2056.
- Jang, S.H.; Lee, J.; Lee, M.Y.; Park, S.M.; Choi, W.H.; Do, K.H. Prediction of motor outcome using remaining corticospinal tract in patients with pontine infarct: Diffusion tensor imaging study. Somatosens. Mot. Res. 2016, 33, 99–103.
- Ma, C.; Liu, A.; Li, Z.; Zhou, X.; Zhou, S. Longitudinal study of diffusion tensor imaging properties of affected cortical spinal tracts in acute and chronic hemorrhagic stroke. J. Clin. Neurosci. 2014, 21, 1388–1392.
- Wang, D.M.; Li, J.; Liu, J.R.; Hu, H.Y. Diffusion tensor imaging predicts long-term motor functional outcome in patients with acute supratentorial intracranial hemorrhage. Cerebrovasc. Dis. 2012, 34, 199–205.
- Gong, Z.; Zhang, R.; Jiang, W.; Fu, Z. Integrity of The Hand Fibers of The Corticospinal Tract Shown by Diffusion Tensor Imaging Predicts Hand Function Recovery After Hemorrhagic Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105447.
- Imura, T.; Nagasawa, Y.; Inagawa, T.; Imada, N.; Izumi, H.; Emoto, K.; Tani, I.; Yamasaki, H.; Ota, Y.; Oki, S.; et al. Prediction of motor outcomes and activities of daily living function using diffusion tensor tractography in acute hemiparetic stroke patients. J. Phys. Ther. Sci. 2015, 27, 1383–1386.
- Nakashima, A.; Moriuchi, T.; Mitsunaga, W.; Yonezawa, T.; Kataoka, H.; Nakashima, R.; Koizumi, T.; Shimizu, T.; Ryu, N.; Higashi, T. Prediction of prognosis of upper-extremity function following stroke-related paralysis using brain imaging. J. Phys. Ther. Sci. 2017, 29, 1438–1443.
- Koyama, T.; Koumo, M.; Uchiyama, Y.; Domen, K. Utility of Fractional Anisotropy in Cerebral Peduncle for Stroke Outcome Prediction: Comparison of Hemorrhagic and Ischemic Strokes. J. Stroke Cerebrovasc. Dis. 2018, 27, 878–885.



