 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Silvia Bianchi | -- | 2757 | 2022-08-12 18:28:49 | | | |
| 2 | Lindsay Dong | Meta information modification | 2757 | 2022-08-15 03:15:12 | | |
Video Upload Options
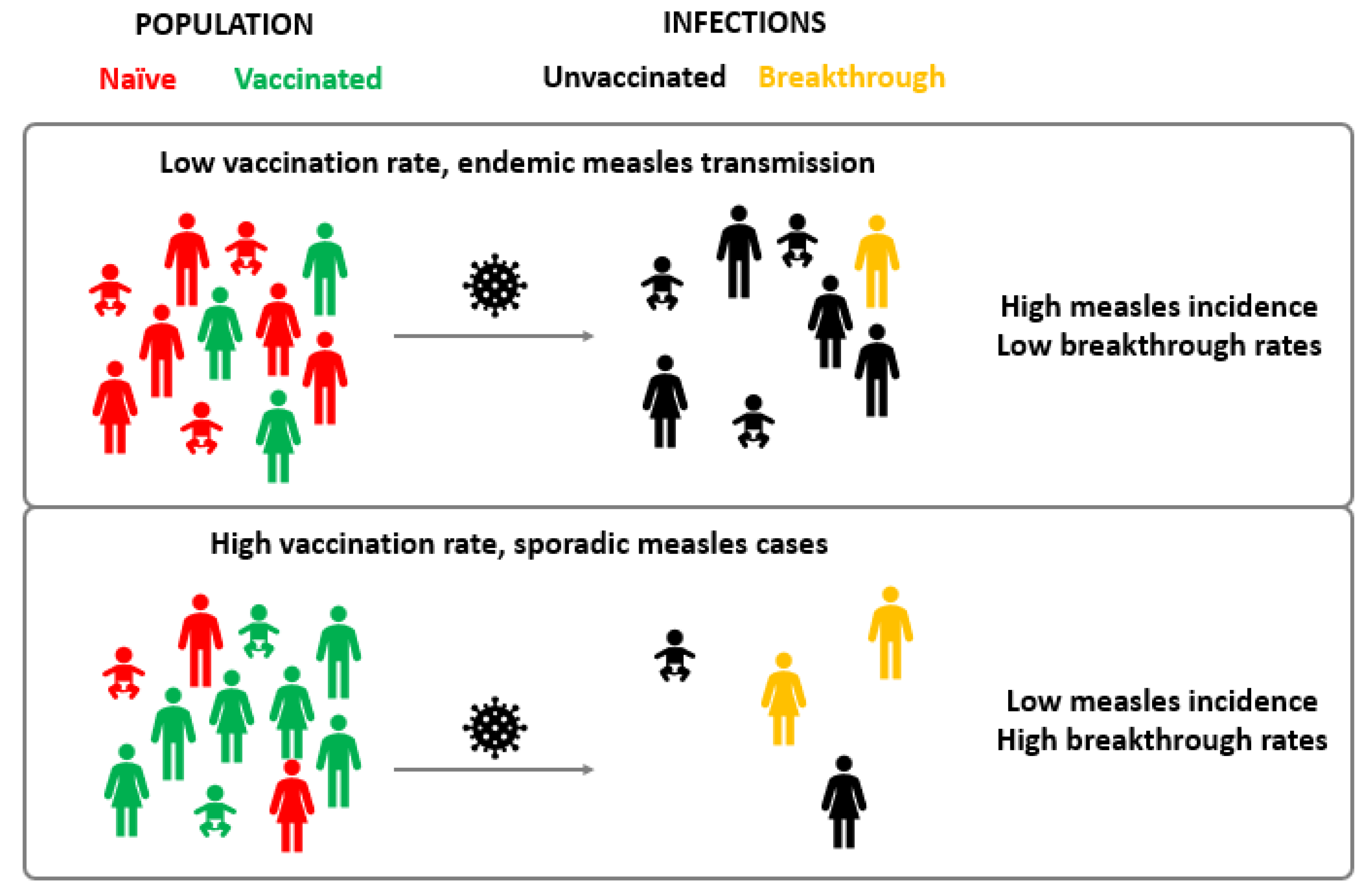
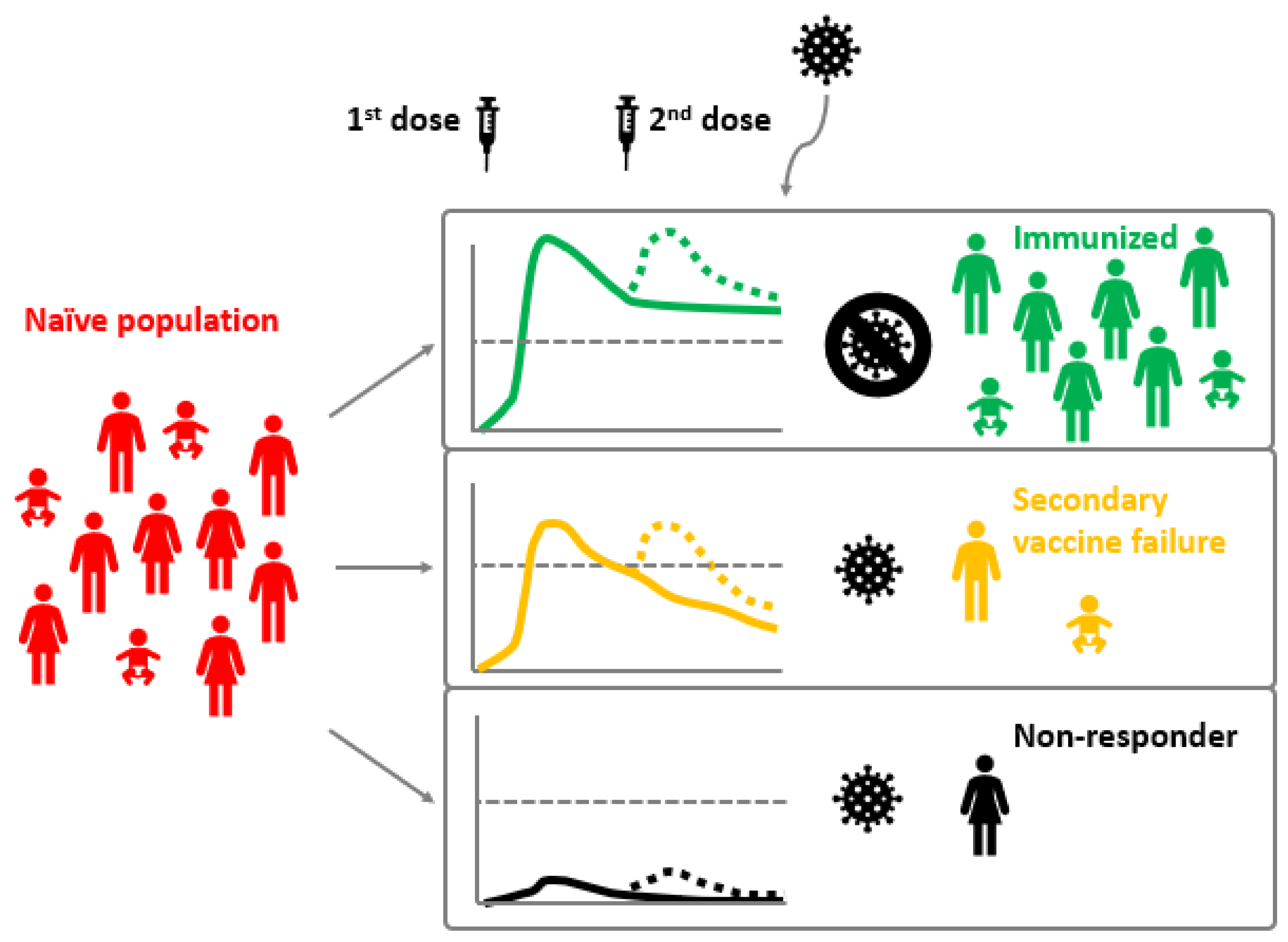
Measles is one of the most contagious diseases known to man. Despite the existence of a safe and effective live attenuated vaccine, measles can appear in vaccinated individuals. Paradoxically, breakthrough cases increase as vaccination coverage in the general population rises. In measles endemic areas, breakthrough cases represent less than 10% of total infections, while in areas with high vaccination coverage these are over 10% of the total. Two different vaccination failures have been described: primary vaccination failure, which consists in the complete absence of humoral response and occurs in around 5% of vaccinated individuals; and secondary vaccination failure is due to waning immunity or incomplete immunity and occurs in 2–10% of vaccinees. Vaccination failures are generally associated with lower viral loads and milder disease (modified measles) since vaccination limits the risk of complicated disease. Vaccination failure seems to occur between six and twenty-six years after the last vaccine dose administration.
1. Introduction
2. Measles Vaccines and Immunization Programs
3. Measles Virus Infection and Vaccine Failure
4. Vaccine Failure Classification
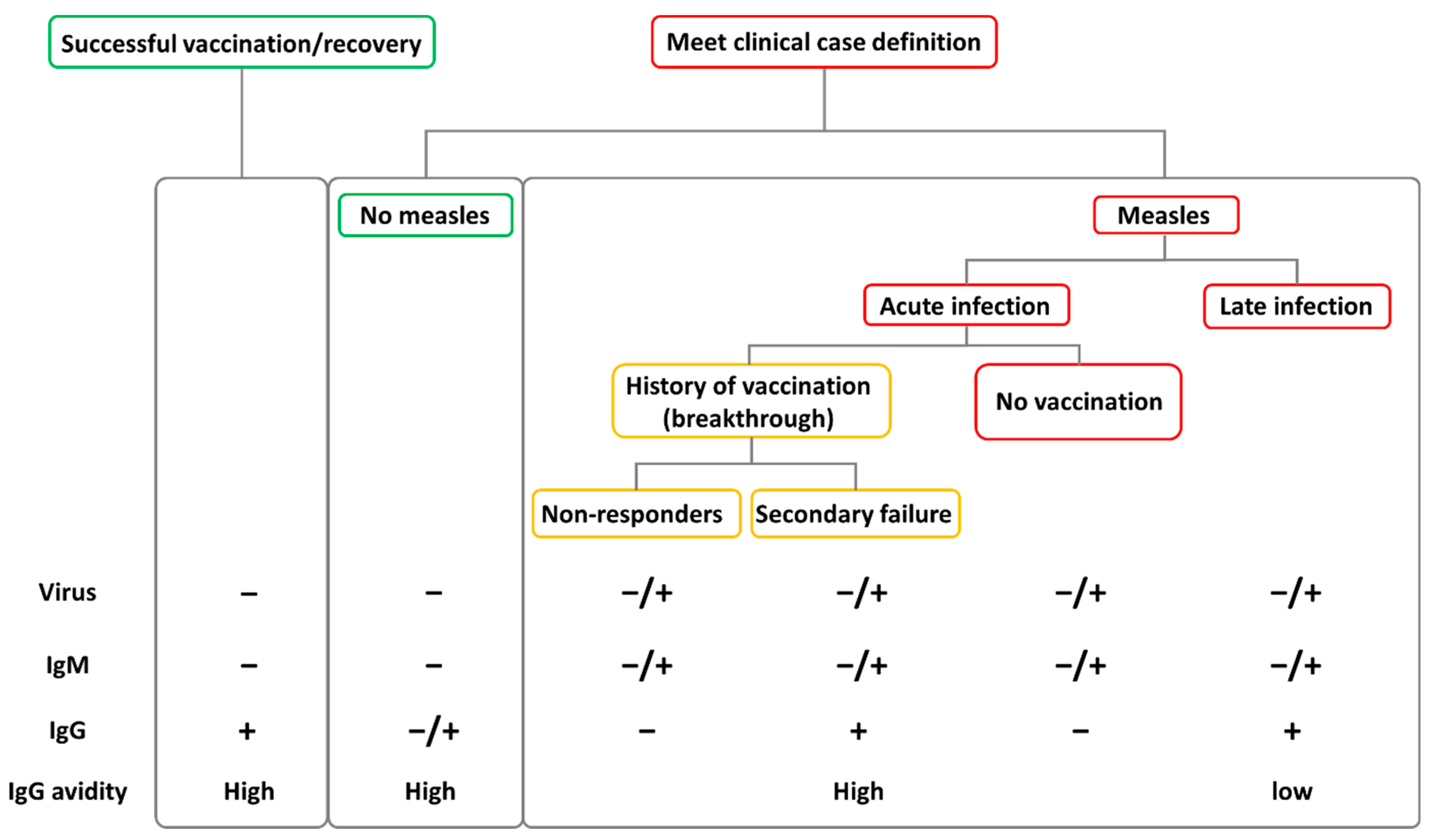
5. Clinical Manifestations of Breakthrough Cases and Diagnostic Challenges
6. Onward Transmission from Breakthrough Cases
Although rare, transmission from vaccine failure cases is possible, with vaccinated people acting both as index cases as well as secondary transmitters. Onward transmission from vaccinated cases to susceptible individuals seems to be limited to specific settings where close contacts are more common, such as familiar or nosocomial environments. The low rate of transmission from breakthrough cases may be associated with the elevated and rapid production of neutralizing antibodies that quickly reduce the viral load, but also with the manifestation with milder symptoms (i.e., mild, or unproductive cough) that reduces the likelihood of an effective transmission of the virus [32]. Nevertheless, the fact that a MV infection and onward transmission can both occur for subjects with vaccine failures, underscores the need to maintain a high index of suspicion for measles during an outbreak and to monitor all subjects despite (presumed) prior vaccination or disease [36]. Specifically, the same effort in tracing contacts should be dedicated to identifying possible infections amongst vaccinated and unvaccinated subjects and vaccinated cases should also carefully follow virus containment procedures. This is of particular importance in health care settings.
7. Booster Doses and Catch-Up Vaccination
References
- Measles. Available online: https://www.who.int/news-room/fact-sheets/detail/measles (accessed on 21 May 2022).
- Moss, W.J.; Griffin, D.E. Global Measles Elimination. Nat. Rev. Microbiol. 2006, 4, 900–908.
- Rima, B.; Balkema-Buschmann, A.; Dundon, W.G.; Duprex, P.; Easton, A.; Fouchier, R.; Kurath, G.; Lamb, R.; Lee, B.; Rota, P.; et al. ICTV Virus Taxonomy Profile: Paramyxoviridae. J. Gen. Virol. 2019, 100, 1593–1594.
- World Health Organization. Manual for the Laboratory Diagnosis of Measles and Rubella Virus Infection; WHO/IVB/07.01; World Health Organization: Geneva, Switzerland, 2007.
- Minnich, L.L.; Goodenough, F.; Ray, C.G. Use of Immunofluorescence to Identify Measles Virus Infections. J. Clin. Microbiol. 1991, 29, 1148–1150.
- World Health Organization. Guidelines for Measles and Rubella Outbreak Investigation and Response in the WHO European Region; World Health Organization: Geneva, Switzerland, 2013; p. 39.
- Hashiguchi, T.; Maenaka, K.; Yanagi, Y. Measles Virus Hemagglutinin: Structural Insights into Cell Entry and Measles Vaccine. Front. Microbiol. 2011, 2, 247.
- Baldo, A.; Galanis, E.; Tangy, F.; Herman, P. Biosafety Considerations for Attenuated Measles Virus Vectors Used in Virotherapy and Vaccination. Hum. Vaccines Immunother. 2016, 12, 1102–1116.
- Ciceri, G.; Canuti, M.; Bianchi, S.; Gori, M.; Piralla, A.; Colzani, D.; Libretti, M.; Frati, E.R.; Baggieri, M.; Lai, A.; et al. Genetic Variability of the Measles Virus Hemagglutinin Gene in B3 Genotype Strains Circulating in Northern Italy. Infect. Genet. Evol. 2019, 75, 103943.
- Woelk, C.H.; Jin, L.; Holmes, E.C.; Brown, D.W.G.Y. Immune and Artificial Selection in the Haemagglutinin (H) Glycoprotein of Measles Virus. J. Gen. Virol. 2001, 82, 2463–2474.
- Xu, S.; Zhang, Y.; Zhu, Z.; Liu, C.; Mao, N.; Ji, Y.; Wang, H.; Jiang, X.; Li, C.; Tang, W.; et al. Genetic Characterization of the Hemagglutinin Genes of Wild-Type Measles Virus Circulating in China, 1993–2009. PLoS ONE 2013, 8, e73374.
- Bianchi, S.; Canuti, M.; Ciceri, G.; Gori, M.; Colzani, D.; Dura, M.; Pennati, B.M.; Baggieri, M.; Magurano, F.; Tanzi, E.; et al. Molecular Epidemiology of B3 and D8 Measles Viruses through Hemagglutinin Phylogenetic History. Int. J. Mol. Sci. 2020, 21, 4435.
- Bianchi, S.; Gori, M.; Fappani, C.; Ciceri, G.; Canuti, M.; Colzani, D.; Dura, M.; Terraneo, M.; Lamberti, A.; Baggieri, M.; et al. Characterization of Vaccine Breakthrough Cases during Measles Outbreaks in Milan and Surrounding Areas, Italy, 2017–2021. Viruses 2022, 14, 1068.
- Pacenti, M.; Maione, N.; Lavezzo, E.; Franchin, E.; Dal Bello, F.; Gottardello, L.; Barzon, L. Measles Virus Infection and Immunity in a Suboptimal Vaccination Coverage Setting. Vaccines 2019, 7, 199.
- Moss, W.J. Measles. Lancet 2017, 390, 2490–2502.
- WHO Recommendations for Routine Immunization—Summary Tables. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/policies/who-recommendations-for-routine-immunization---summary-tables (accessed on 12 June 2022).
- Cherry, J.D.; Feigin, R.D.; Lobes, L.A.; Hinthorn, D.R.; Shackelford, P.G.; Shirley, R.H.; Lins, R.D.; Choi, S.C. Urban Measles in the Vaccine Era: A Clinical, Epidemiologic, and Serologic Study. J. Pediatr. 1972, 81, 217–230.
- Cherry, J.D.; Feigin, R.D.; Shackelford, P.G.; Hinthorn, D.R.; Schmidt, R.R. A Clinical and Serologic Study of 103 Children with Measles Vaccine Failure. J. Pediatr. 1973, 82, 802–808.
- Plotkin, S.A. Failures of Protection by Measles Vaccine. J. Pediatr. 1973, 82, 908–911.
- LeBaron, C.W.; Beeler, J.; Sullivan, B.J.; Forghani, B.; Bi, D.; Beck, C.; Audet, S.; Gargiullo, P. Persistence of Measles Antibodies after 2 Doses of Measles Vaccine in a Postelimination Environment. Arch. Pediatr. Adolesc. Med. 2007, 161, 294–301.
- Arima, Y.; Oishi, K. Letter to the Editor: Measles Cases among Fully Vaccinated Persons. Eurosurveillance 2018, 23, 1800449.
- Cherry, J.D.; Zahn, M. Clinical Characteristics of Measles in Previously Vaccinated and Unvaccinated Patients in California. Clin. Infect. Dis. 2018, 67, 1315–1319.
- López-Perea, N.; Fernández-García, A.; Echevarría, J.E.; de Ory, F.; Pérez-Olmeda, M.; Masa-Calles, J. Measles in Vaccinated People: Epidemiology and Challenges in Surveillance and Diagnosis in the Post-Elimination Phase. Spain, 2014–2020. Viruses 2021, 13, 1982.
- Risco-Risco, C.; Masa-Calles, J.; López-Perea, N.; Echevarría, J.E.; Rodríguez-Caravaca, G. Epidemiology of Measles in Vaccinated People, Spain 2003-2014. Enferm. Infect. Microbiol. Clin. 2017, 35, 569–573.
- Sundell, N.; Dotevall, L.; Sansone, M.; Andersson, M.; Lindh, M.; Wahlberg, T.; Tyrberg, T.; Westin, J.; Liljeqvist, J.-Å.; Bergström, T.; et al. Measles Outbreak in Gothenburg Urban Area, Sweden, 2017 to 2018: Low Viral Load in Breakthrough Infections. Eurosurveillance 2019, 24, 1900114.
- Wiedermann, U.; Garner-Spitzer, E.; Wagner, A. Primary Vaccine Failure to Routine Vaccines: Why and What to Do? Hum. Vaccines Immunother. 2016, 12, 239–243.
- Javelle, E.; Colson, P.; Parola, P.; Raoult, D. Measles, the Need for a Paradigm Shift. Eur. J. Epidemiol. 2019, 34, 897–915.
- Sniadack, D.H.; Crowcroft, N.S.; Durrheim, D.N.; Rota, P.A. Roadmap to Elimination—Standard Measles and Rubella Surveillance. Wkly. Epidemiol. Rec. 2017, 9, 10–92.
- Pannuti, C.S.; Morello, R.J.; de Moraes, J.C.; Curti, S.P.; Afonso, A.M.S.; Camargo, M.C.C.; de Souza, V.A.U.F. Identification of Primary and Secondary Measles Vaccine Failures by Measurement of Immunoglobulin G Avidity in Measles Cases during the 1997 São Paulo Epidemic. Clin. Vaccine Immunol. 2004, 11, 119–122.
- Mercader, S.; Garcia, P.; Bellini, W.J. Measles Virus IgG Avidity Assay for Use in Classification of Measles Vaccine Failure in Measles Elimination Settings. Clin. Vaccine Immunol. 2012, 19, 1810–1817.
- Hubiche, T.; Brazier, C.; Vabret, A.; Reynaud, S.; Roudiere, L.; del Giudice, P. Measles Transmission in a Fully Vaccinated Closed Cohort: Data From a Nosocomial Clustered Cases in a Teenage Psychiatric Unit. Pediatr. Infect. Dis. J. 2019, 38, e230.
- World Health Organization. Manual for the Laboratory-Based Surveillance of Measles, Rubella, and Congenital Rubella Syndrome; World Health Organization: Geneva, Switzerland, 2018.
- Edmonson, M.B.; Addiss, D.G.; McPherson, J.T.; Berg, J.L.; Circo, S.R.; Davis, J.P. Mild Measles and Secondary Vaccine Failure During a Sustained Outbreak in a Highly Vaccinated Population. JAMA 1990, 263, 2467–2471.
- Iwamoto, M.; Hickman, C.J.; Colley, H.; Arciuolo, R.J.; Mahle, C.E.; Deocharan, B.; Siemetzki-Kapoor, U.; Zucker, J.R.; Rosen, J.B. Measles Infection in Persons with Secondary Vaccine Failure, New York City, 2018–2019. Vaccine 2021, 39, 5346–5350.
- Measles and Rubella Strategic Framework: 2021–2030. Available online: https://www.who.int/publications-detail-redirect/measles-and-rubella-strategic-framework-2021-2030 (accessed on 17 May 2022).
- Martha Iwamoto; Carole J. Hickman; Heather Colley; Robert J. Arciuolo; Christine E. Mahle; Bisram Deocharan; Ulrike Siemetzki-Kapoor; Jane R. Zucker; Jennifer B. Rosen; Measles infection in persons with secondary vaccine failure, New York City, 2018–19. Vaccine 2021, 39, 5346-5350, 10.1016/j.vaccine.2021.07.078.
- Augusto, G.F.; Silva, A.; Pereira, N.; Fernandes, T.; Leça, A.; Valente, P.; Calé, E.; Aguiar, B.A.; Martins, A.; Palminha, P.; et al. Report of Simultaneous Measles Outbreaks in Two Different Health Regions in Portugal, February to May 2017: Lessons Learnt and Upcoming Challenges. Eurosurveillance 2019, 24, 1800026.
- Atrasheuskaya, A.V.; Kulak, M.V.; Neverov, A.A.; Rubin, S.; Ignatyev, G.M. Measles Cases in Highly Vaccinated Population of Novosibirsk, Russia, 2000–2005. Vaccine 2008, 26, 2111–2118.
- Dine, M.S.; Hutchins, S.S.; Thomas, A.; Williams, I.; Bellini, W.J.; Redd, S.C. Persistence of Vaccine-Induced Antibody to Measles 26–33 Years after Vaccination. J. Infect. Dis. 2004, 189 (Suppl. S1), S123–S130.
- Holzmann, H.; Hengel, H.; Tenbusch, M.; Doerr, H.W. Eradication of Measles: Remaining Challenges. Med. Microbiol. Immunol. 2016, 205, 201–208.
- Gaythorpe, K.A.; Abbas, K.; Huber, J.; Karachaliou, A.; Thakkar, N.; Woodruff, K.; Li, X.; Echeverria-Londono, S.; VIMC Working Group on COVID-19 Impact on Vaccine Preventable Disease; Ferrari, M.; et al. Impact of COVID-19-Related Disruptions to Measles, Meningococcal A, and Yellow Fever Vaccination in 10 Countries. Elife 2021, 10, e67023.
- Venkatesan, P. Worrying Global Decline in Measles Immunisation. Lancet Microbe 2022, 3, e9.

