Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Gisela Marta Oliveira | -- | 1513 | 2022-07-14 16:55:18 | | | |
| 2 | Rita Xu | Meta information modification | 1513 | 2022-07-15 07:28:49 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Mata, T.M.; Felgueiras, F.; Martins, A.A.; Monteiro, H.; Ferraz, M.P.; Oliveira, G.M.; Gabriel, M.F.; Silva, G.V. Indoor Air Quality in Elderly Centers. Encyclopedia. Available online: https://encyclopedia.pub/entry/25167 (accessed on 26 July 2026).
Mata TM, Felgueiras F, Martins AA, Monteiro H, Ferraz MP, Oliveira GM, et al. Indoor Air Quality in Elderly Centers. Encyclopedia. Available at: https://encyclopedia.pub/entry/25167. Accessed July 26, 2026.
Mata, Teresa M., Fátima Felgueiras, António A. Martins, Helena Monteiro, Maria Pia Ferraz, Gisela M. Oliveira, Marta Fonseca Gabriel, Gabriela Ventura Silva. "Indoor Air Quality in Elderly Centers" Encyclopedia, https://encyclopedia.pub/entry/25167 (accessed July 26, 2026).
Mata, T.M., Felgueiras, F., Martins, A.A., Monteiro, H., Ferraz, M.P., Oliveira, G.M., Gabriel, M.F., & Silva, G.V. (2022, July 14). Indoor Air Quality in Elderly Centers. In Encyclopedia. https://encyclopedia.pub/entry/25167
Mata, Teresa M., et al. "Indoor Air Quality in Elderly Centers." Encyclopedia. Web. 14 July, 2022.
Copy Citation
The elderly segment of the population is more vulnerable to adverse environmental conditions. Indoor air quality is one of the most relevant health determinant, especially for elders resident in Care Centers because elders spend most time indoors. The recent COVID-19 pandemic contributed greately to raise awareness on the importance of breathing safe air without biological and physical-chemical contaminants. The heath effects on elders of the main pollutants are discussed in this topic.
indoor air quality
elderly care centers
1. Introduction
Indoor air quality (IAQ) and its negative health effects is a main public health issue. Substances found in the indoor environment are among the main determinants of an individual’s health, whether they are [1]:
- chemicals:
-
- volatile organic compounds (VOCs): esters, alcohols (e.g., ethanol, isopropanol), ketones (e.g., acetone), aldehydes (e.g., hexanal) and terpenes (e.g., limonene)
- formaldehyde (CH2O)
- ozone (O3)
- nitrogen dioxide (NO2)
- carbon monoxide (CO)
- sulfur dioxide (SO2)
- particulate matter (PM) of aerodiameter <10, <2.5, and <0.1 μm (PM10, PM2.5, PM0.1, respectively)
- asbestos
- radon
- tobacco smoke
- biocontaminants (e.g., bacteria, fungi, viruses, molds, allergens) [1].
IAQ and thermal comfort, which are key factors affecting occupants’ health and well-being, are influenced by ambient parameters, such as outdoor temperature, atmospheric pressure, buildings surrounding surfaces temperature, air movement, ventilation, relative humidity, and carbon dioxide (CO2) concentration [2][3][4].
The world population is increasingly ageing and, in 2019,1 out of 11 people was above 65 years old [5]. This global growing trend [6] urgently calls for effective actions, to ensure the protection of this demographic group that is more vulnerable to adverse environmental conditions. Elders spend comparatively more time indoors than younger generations; therefore, the quality of indoor air is a very important health determinant and wellbeing factor, especially for those that are enduring their final years with limiting disease. The vulnerability of elders is a natural consequence of inherent deterioration of biological functions, including immune defenses, but it is often aggravated by poor health conditions such as respiratory or circulatory illness; therefore, elders have a greater predisposition to respiratory infections [7]. In addition to natural ageing, elders have an accumulated lifelong exposure to pollution and other environmental conditions [8]. Due to their reduced mobility, they tend to spend most of their time indoors (95% in average) [9], usually in bedrooms and living–dining rooms, corresponding to about 19 to 20 h/day [10]. This is particularly critical to residents in geriatric facilities who are potentially at higher risk of exposure to indoor air pollution [11]. Therefore, the indoors environment is likely to influence the health of elderly people, who are a vulnerable group to air pollutants exposure. Indoor air accumulates several types of pollutants normally associated with specific compounds originating from the various household products used, such as in cleaning, disinfection, hygiene, and healthcare activities, and also emitted from building materials and furnishings [12]. Cleaning solutions and detergents frequently used in nursing homes and healthcare institutions, reduce the risk of infections but increase the levels of total volatile organic compounds (TVOC) in the air [9]. Therefore, keeping elderly people healthy is a challenge that requires better understanding of health consequences exposure to air pollutants [8].
So far, the respiratory health effects of indoor air pollution have been well documented in the general population but less analyzed in elderly people living in elderly centers, nursing homes, and other care facilities [13][14]. There are few data on exposure to indoor air pollutants and related effects on respiratory health in the elderly population. Few studies relate exposure to internal air pollutants with effects on the respiratory function, such as wheezing, breathlessness, cough, asthma, or lung cancer [15]. Data on the effects of indoor allergens on respiratory health in the elderly are scarce [16].
Studies have shown that the elderly, particularly those over 80 years, are more likely to have health impairments, even with moderate levels of indoor air pollutants [7][17]. One of the most effective methods to reduce the concentration of pollutants is the dilution effect by simply increasing the rate of air exchange (ventilation) of the indoor spaces [18][19]. Almeida-Silva et al. [9] characterized the indoor air quality in 10 elderly care centers (ECCs) in Portugal to assess the elders’ daily exposure to air pollutants, showing that due to insufficient room ventilation, the concentration of some substances (CO2, VOCs, O3, and PM10) exceeded the legal limit values.
Concerning the emerging compounds, Arnold et al. [20] carried out a study at ECCs in the United States and in Portugal to determine the concentrations of organophosphate esters (OPEs), brominated flame retardants (BFRs), polycyclic aromatic hydrocarbons (PAHs), organochlorine pesticides (OCPs), and polychlorinated biphenyls (PCBs) in dust samples collected indoors from fourteen facilities. This study results revealed that OPEs, PAHs, and BFRs were the most abundant and OCPs and PCBs were the least abundant semi-volatile organic compounds (SVOCs) groups in the collected dust.
Concerning biological contaminants, airborne microorganisms, such as bacteria and fungi, are often present in the indoor air. In particular, the indoor habitat harbors microorganisms that are not commonly found outdoors, which is also influenced by the air temperature, relative humidity, architectural design, and the source of air ventilation [21]. In this case, the ventilation of spaces and the density of occupants can influence the abundance of these microorganisms and also the transmission of some pathogenic microbes [22]. A study [23] of indoor air in a large hospital building revealed that the most common bacterial strains belonged to genera Staphylococcus, Micrococcus, Kocuria, Aerococcus, Kytococcus, Bacillus, Pseudomonas, Corynebacterium, and Streptococcus, while the most abundant fungal genera included Cladosporium, Aspergillus, Penicillium, Alterneria, Geotrichium, and Ulocladium. Frequent cleaning is an important factor for maintaining a low microbial load in the air.
The European Union (EU) has established legislation on air quality specifications for both atmospheric and indoor air. In the scope of the European Green Deal implementation and the EU Climate and Energy policies [24], alongside the economic crisis brought by the COVID-19 pandemic and the present energy crisis, it is rather obvious that energy consumption and supply security are top and urgent priorities in the EU. Presently, energy efficiency and security policies are receiving public attention, and the EU legal framework for energy consumption in the buildings sector is being recast with a strong focus on energy efficiency as the main goal. The principle that “energy efficiency comes first” is a precious one that should always be implemented; however, energy savings in Heating, Ventilating and Air Conditioning (HVAC) systems cannot be achieved by reducing the ambition to continuously raise the quality of indoor air standards.
2. Characteristics of Elderly Centers as Built Environments
Some characteristics of the built environment may significantly affect IAQ of elderly centers. The likelihood of exposure to different indoor air pollutants is influenced by factors such as:
- building design
- construction and furniture components and materials
- management and maintenance of operational systems (e.g., HVAC, mechanical ventilation)
- density of occupants
- occupants’ activities.
Insufficient ventilation may result in poor air quality with high concentration of indoor air pollutants, since these are not able to be diluted or dissipated by air convenction. Assuring an adequate ventilation in space is fundamental, especially in buildings where users spend most of their time indoors, such as elders and people with physical or mobility disabilities, who end up being exposed to indoor air conditions for prolonged periods of time (Figure 1).
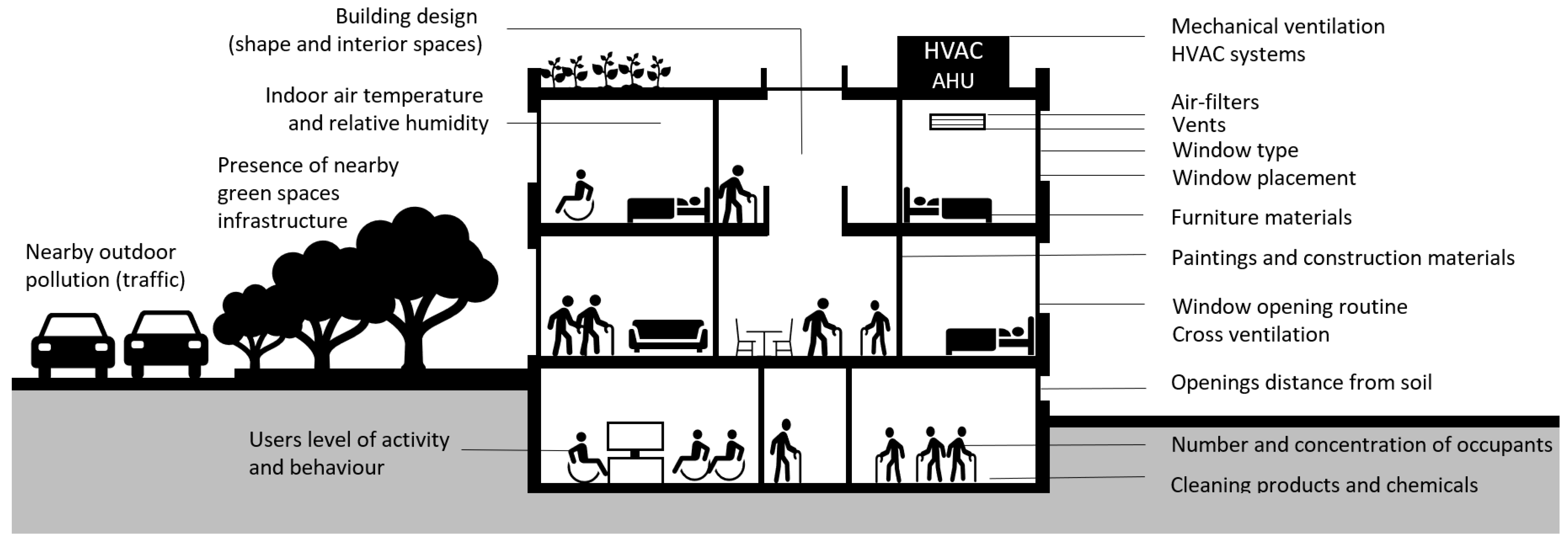
Figure 1. Factors influencing IAQ in elderly centers (authors’ own creation).
Building design can affect users' life quality. Window sizing, orientation, openings, and vents determine not only the natural sunlight but also the natural fresh-air availability that the different interior spaces may have, which are critical for interior pollutants removal by natural ventilation. A few studies have analyzed how the presence of nearby green spaces (i.e., gardens, lawns, trees, flower bushes, shrubs, green walls and roofs) may improve not only aesthetics but also air quality of elderly centers [24]. A few studies have shown that green spaces may partially filter and remove air pollutants in urban areas [25], being especially useful to reduce PM at pedestrian level in buildings close to main roads [26].
Mendes et al. [2] monitored IAQ and thermal comfort parameters (CO, CO2, PM10, PM2.5, TVOC, formaldehyde, bacteria, fungi, room air temperature, humidity) of 22 elderly centers located in Porto (Portugal) during summer and winter. This study results enabled the comparison of reference values from existing standards (national and international) and the variability among spaces (i.e., bedroom, living room, medical office) within the same building and between different buildings. The authors also tried to find correlations between the building characteristics and IAQ parameters. For that purpose, an inventory of building properties was collected for each building monitored, such as type of construction components (brick or stone masonry), the presence or absence of envelope thermal insulation, the windows type (single or double glazing) and sealants, ventilation type (natural, mechanical, or both), heating system (central or local heaters), and the presence of observable building pathologies (condensations). The building characteristics that mostly influenced the IAQ and thermal comfort were the window frame type, heating, ventilation, and thermal insulation. The indoor air quality parameters most affected were the presence of microorganisms (bacteria and fungi), relative humidity, and indoor temperature. It is important to note that many buildings were not originally projected to be elderly centers; instead, they were adapted for such function.
References
- Bonnefoy, X.R.; Braubach, M.; Moissonnier, B.; Monolbaev, K.; Röbbel, N. Housing and Health in Europe: Preliminary Results of a Pan-European Study. Am. J. Public Health 2003, 93, 1559–1563.
- Mendes, A.; Bonassi, S.; Aguiar, L.; Pereira, C.; Neves, P.; Silva, S.; Mendes, D.; Guimarães, L.; Moroni, R.; Teixeira, J.P. Indoor air quality and thermal comfort in elderly care centers. Urban Clim. 2015, 14, 486–501.
- Mendes, A.; Pereira, C.; Mendes, D.; Aguiar, L.; Neves, P.; Silva, S.; Batterman, S.; Teixeira, J.P. Indoor air quality and thermal comfort—Results of a pilot study in elderly care centers in Portugal. J. Toxicol. Environ. Health Part A Curr. Issues 2013, 76, 333–344.
- Ormandy, D.; Ezratty, V. Health and thermal comfort: From WHO guidance to housing strategies. Energy Policy 2012, 49, 116–121.
- United Nations. World Population Ageing 2019: Highlights; Department of Economic and Social Affairs Population Division: New York, NY, USA, 2019; p. 46.
- European Union. Ageing Europe—Looking at the Lives of Older People in the EU; European Union: Maastricht, The Netherlands, 2020; ISBN 978-92-76-21520-2.
- Bentayeb, M.; Norback, D.; Bednarek, M.; Bernard, A.; Cai, G.; Cerrai, S.; Eleftheriou, K.K.; Gratziou, C.; Holst, G.J.; Lavaud, F.; et al. Indoor air quality, ventilation and respiratory health in elderly residents living in nursing homes in Europe. Eur. Respir. J. 2015, 45, 1228–1238.
- Simoni, M.; Jaakkola, M.S.; Carrozzi, L.; Baldacci, S.; Di Pede, F.; Viegi, G. Indoor air pollution and respiratory health in the elderly. Eur. Respir. J. Suppl. 2003, 21, 15–20.
- Almeida-Silva, M.; Wolterbeek, H.T.; Almeida, S.M. Elderly exposure to indoor air pollutants. Atmos. Environ. 2014, 85, 54–63.
- Adan, O.C.G.; Ng-A-Tham, J.; Hanke, W.; Sigsgaard, T.; van den Hazel, P.; Wu, F. In search of a common European approach to a healthy indoor environment. Environ. Health Perspect. 2007, 115, 983–988.
- van den Berg, M.E.L.; Winsall, M.; Dyer, S.M.; Breen, F.; Gresham, M.; Crotty, M. Understanding the barriers and enablers to using outdoor spaces in nursing homes: A systematic review. Gerontologist 2020, 60, e254–e269.
- Spengler, J.; Adamkiewicz, G. Indoor air pollution: An old problem with new challenges. Int. J. Environ. Res. Public Health 2009, 6, 2880–2882.
- Annesi-Maesano, I.; Norback, D.; Zielinski, J.; Bernard, A.; Gratziou, C.; Sigsgaard, T.; Sestini, P.; Viegi, G. Geriatric study in Europe on health effects of air quality in nursing homes (GERIE study) profile: Objectives, study protocol and descriptive data. Multidiscip. Respir. Med. 2013, 8, 1–10.
- Bentayeb, M.; Simoni, M.; Norback, D.; Baldacci, S.; Maio, S.; Viegi, G.; Annesi-Maesano, I. Indoor air pollution and respiratory health in the elderly. J. Environ. Sci. Health Part A Toxic/Hazardous Subst. Environ. Eng. 2013, 48, 1783–1789.
- Mendes, A.; Papoila, A.L.; Carreiro-Martins, P.; Bonassi, S.; Caires, I.; Palmeiro, T.; Aguiar, L.; Pereira, C.; Neves, P.; Mendes, D.; et al. The impact of indoor air quality and contaminants on respiratory health of older people living in long-term care residences in Porto. Age Ageing 2016, 45, 136–142.
- Maio, S.; Sarno, G.; Baldacci, S.; Annesi-Maesano, I.; Viegi, G. Air quality of nursing homes and its effect on the lung health of elderly residents. Expert Rev. Respir. Med. 2015, 9, 671–673.
- Baudet, A.; Baurès, E.; Blanchard, O.; Le Cann, P.; Gangneux, J.-P.; Florentin, A. Indoor Carbon Dioxide, Fine Particulate Matter and Total Volatile Organic Compounds in Private Healthcare and Elderly Care Facilities. Toxics 2022, 10, 136.
- Baurès, E.; Blanchard, O.; Mercier, F.; Surget, E.; Le Cann, P.; Rivier, A.; Gangneux, J.P.; Florentin, A. Indoor air quality in two French hospitals: Measurement of chemical and microbiological contaminants. Sci. Total Environ. 2018, 642, 168–179.
- Arnold, K.; Teixeira, J.P.; Mendes, A.; Madureira, J.; Costa, S.; Salamova, A. A pilot study on semivolatile organic compounds in senior care facilities: Implications for older adult exposures. Environ. Pollut. 2018, 240, 908–915.
- Kembel, S.W.; Jones, E.; Kline, J.; Northcutt, D.; Stenson, J.; Womack, A.M.; Bohannan, B.J.M.; Brown, G.Z.; Green, J.L. Architectural design influences the diversity and structure of the built environment microbiome. ISME J. 2012, 6, 1469–1479.
- Wan, G.H.; Chung, F.F.; Tang, C.S. Long-term surveillance of air quality in medical center operating rooms. Am. J. Infect. Control 2011, 39, 302–308.
- Asif, A.; Zeeshan, M.; Hashmi, I.; Zahid, U.; Bhatti, M.F. Microbial quality assessment of indoor air in a large hospital building during winter and spring seasons. Build. Environ. 2018, 135, 68–73.
- European Commission. The European Green Deal; Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions. COM(2019) 640 final; European Union: Brussels, Belgium, 2019; p. 24.
- Wu, H.; Kumar, P.; Cao, S. Implementation of green infrastructure for improving the building environment of elderly care centres. J. Build. Eng. 2022, 54, 104682.
- Wang, Y.; Bakker, F.; de Groot, R.; Wörtche, H. Effect of ecosystem services provided by urban green infrastructure on indoor environment: A literature review. Build. Environ. 2014, 77, 88–100.
- Viecco, M.; Jorquera, H.; Sharma, A.; Bustamante, W.; Fernando, H.J.S.; Vera, S. Green roofs and green walls layouts for improved urban air quality by mitigating particulate matter. Build. Environ. 2021, 204, 108120.
More
Information
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.8K
Entry Collection:
Environmental Sciences
Revisions:
2 times
(View History)
Update Date:
15 Jul 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No