 +1 credit
+1 credit
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Raya Algonaiman | -- | 2193 | 2022-06-14 19:10:55 | | | |
| 2 | Raya Algonaiman | + 1578 word(s) | 3771 | 2022-06-14 19:38:30 | | | | |
| 3 | Raya Algonaiman | + 88 word(s) | 3859 | 2022-06-14 19:49:12 | | | | |
| 4 | Raya Algonaiman | Meta information modification | 3859 | 2022-06-14 19:50:22 | | | | |
| 5 | Peter Tang | -447 word(s) | 3412 | 2022-06-15 05:04:37 | | | | |
| 6 | Raya Algonaiman | -154 word(s) | 3258 | 2022-06-15 09:38:34 | | |
Video Upload Options
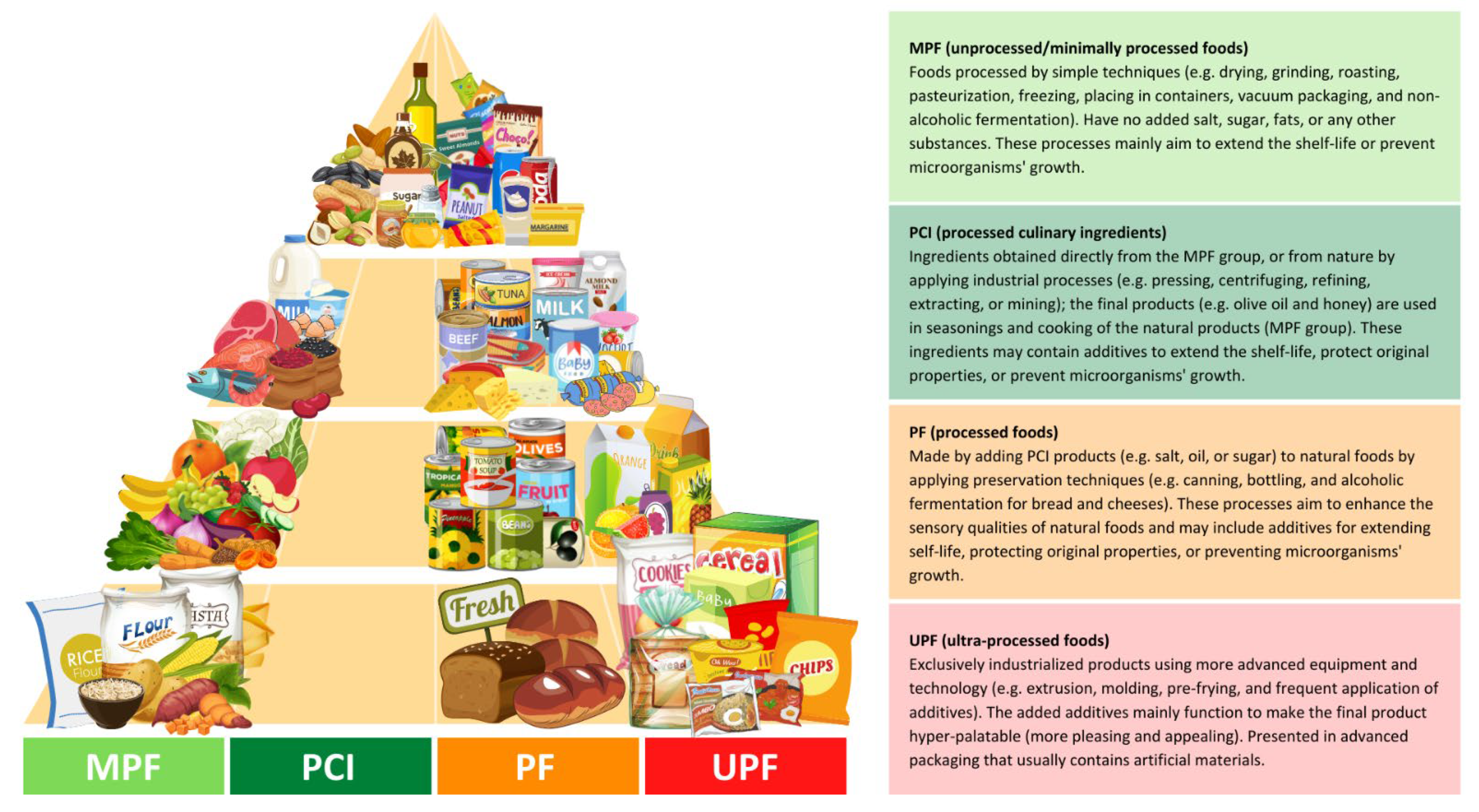
Ultra-processed foods (UPFs) are products that have undergone a series of industrial processes, including physical, biological, or chemical processes, coupled with the use of additives such as colorings, emulsifiers, and preservatives. UPF consumption has grown dramatically over the last few decades worldwide. This growth is accompanied by the increasing prevalence of non-communicable diseases (NCDs) such as cardiovascular diseases, hypertension, and type 2 diabetes. UPFs represent three main health concerns: (i) they are generally high in non-nutritive compounds such as sugars, sodium, and trans fat and low in nutritional compounds such as proteins and fibers, (ii) they contain different types of additives that may cause severe health issues, and (iii) they are presented in packages made of synthetic materials that may also cause undesirable health side-effects.
1. Introduction
2. An Overview of Ultra-Processed Foods
3. Ultra-Processed Foods and Health Outcomes
4. Ultra-Processed Foods and Risk of Diabetes
|
Study Design/Follow-Up/ |
UPF Intake Assessment |
Main Results |
References |
|---|---|---|---|
|
Participant Characteristics |
|||
|
Cross-sectional/- n = 13,608 adults (age ≥ 19 years) Diabetic (7%) (50% women) |
24 h recalls/NOVA/ proportion of TEI |
↑ DM risk by 37% (with high vs. low intake, 73% vs. 24% of TEI) An absolute 10% increase in UPF intake increases the risk by 6% (p < 0.05) |
Nardocci et al. [28] (2021, Canada) |
|
Prospective cohort/6 years n = 104,707 adults (age ≥ 18 years) Non-diabetic (79.2% women) |
24 h recalls/NOVA/ proportion of weight |
An absolute 10% increase in UPF intake was associated with 15% higher risk of T2D (p = 0.001) |
Srour et al. [31] (2020, France) |
|
Prospective cohort/5.4 years n = 21,730 adults (age 40–69 years) Non-diabetic (52.9% women) |
24 h recalls/NOVA/ proportion of weight |
↑ T2D risk by 44% (with high vs. low intake, 41.9% vs. 7.7% of diet proportion) (p < 0.028) |
Levy et al. [32] (2020, UK) |
|
Prospective cohort/12 years n = 20,060 adults (age ≥ 18 years) Non-diabetic (61.5% women) |
FFQ/NOVA/ proportion of weight |
↑ T2D risk by 53% (with high vs. low intake, >323.3 vs. <214.6 g/day of diet proportion) (p = 0.024) |
Llavero-Valero et al. [33] (2021, Spain) |
|
Prospective cohort/41 months n = 70,421 adults (age 35–70 years) Non-diabetic at baseline (58.6% women) |
FFQ/NOVA/ proportion of weight |
↑ T2D risk by 80% (with high vs. low intake, 48.7% vs. 23.7% of diet proportion) An absolute 10% increase in UPF intake increases the risk by 25% (p < 0.001) |
Duan et al. [34] (2020, The Netherlands) |
|
Cross-sectional/- n = 785 pregnant women (age ≥ 20 years) Non-diabetic at baseline |
24 h recalls/*/ proportion of TEI |
↑ gestational obesity risk by 3 times (with high vs. low intake, 47% vs. 18% of TEI) (p < 0.05) No association with GDM (p > 0.05) |
Sartorelli et al. [35] (2019, Brazil) |
|
Prospective cohort/7.2 years n = 3730 pregnant women (age 18–49 years) Non-diabetic |
FFQ/NOVA/ proportion of weight |
↑ GDM risk by 10% (with high vs. low intake, >4.5 vs. <3.3 serving/day)(p = 0.818) women aged ≥30 years had a doubled risk (p = 0.041) |
Leone et al. [36] (2021, Spain) |
|
Cohort/- n = 42 pregnant women (age ≥ 20 years) pre-gestational diabetics |
FFQ/NOVA/ proportion of TEI |
Each 1 kcal from UPF in the 3rd trimester (mean intake, 15.2% of TEI): ↑ 1-h PPG level by 0.143 (p = 0.011) ↑ HbA1c by 0.007% (p = 0.025) ↑ gestational weight by 0.11 kg (p = 0.006) |
Silva et al. [37] (2021, Brazil) |
Abbreviations: UPF: Ultra-processed foods; FFQ: Food frequently questionnaires; TEI: Total energy intake; DM: Diabetes mellitus; T2D: Type 2 diabetes; GDM: Gestational diabetes mellitus; PPG: Postprandial glucose; HbA1c: glycosylated hemoglobin; (↑): Increased. *Classified based on the 2014 Guia Alimentar para a População Brasileira; see Louzada et al. [38] for the detailed method.
References
- Marino, M.; Puppo, F.; Del Bo’, C.; Vinelli, V.; Riso, P.; Porrini, M.; Martini, D. A systematic review of worldwide consumption of ultra-processed foods: Findings and criticisms. Nutrients 2021, 13, 2778.
- Baker, P.; Machado, P.; Santos, T.; Sievert, K.; Backholer, K.; Hadjikakou, M.; Russell, C.; Huse, O.; Bell, C.; Scrinis, G. Ultra-processed foods and the nutrition transition: Global, regional and national trends, food systems transformations and political economy drivers. Obes. Rev. 2020, 21, e13126.
- Popkin, B.M.; Ng, S.W. The nutrition transition to a stage of high obesity and noncommunicable disease prevalence dominated by ultra-processed foods is not inevitable. Obes. Rev. 2022, 23, e13366.
- Chen, X.; Zhang, Z.; Yang, H.; Qiu, P.; Wang, H.; Wang, F.; Zhao, Q.; Fang, J.; Nie, J. Consumption of ultra-processed foods and health outcomes: A systematic review of epidemiological studies. Nutr. J. 2020, 19, 86.
- Matos, R.A.; Adams, M.; Sabaté, J. Review: The Consumption of Ultra-Processed Foods and Non-communicable Diseases in Latin America. Front. Nutr. 2021, 8, 622714.
- Schulze, K.; Adams, J.; White, M. Associations Between Sales of Ultra-Processed Food Products and Prevalence of Adiposity and Diabetes Mellitus: A Panel Analysis of 76 Countries Between 2001–2016. SSRN Elect. J. 2019.
- De Araújo, T.P.; de Moraes, M.M.; Magalhães, V.; Afonso, C.; Santos, C.; Rodrigues, S.S.P. Ultra-Processed Food Availability and Noncommunicable Diseases: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7382.
- Martini, D.; Godos, J.; Bonaccio, M.; Vitaglione, P.; Grosso, G. Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples. Nutrients 2021, 13, 3390.
- Monteiro, C.A.; Cannon, G.; Lawrence, M.; Louzada, M.L.C.; Machado, P.P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; Food and Agriculture Organization of the United Nations: Rome, Italy, 2019; pp. 6–9.
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; de Castro, I.R.R.; Cannon, G. A new classification of foods based on the extent and purpose of their processing. Cad. Saude Publica 2010, 26, 2039–2049.
- Dicken, S.J.; Batterham, R.L. The Role of Diet Quality in Mediating the Association between Ultra-Processed Food Intake, Obesity and Health-Related Outcomes: A Review of Prospective Cohort Studies. Nutrients 2021, 14, 23.
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.C.; Louzada, M.L.C.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941.
- Machado, P.P.; Steele, E.M.; Levy, R.B.; Sui, Z.; Rangan, A.; Woods, J.; Gill, T.; Scrinis, G.; Monteiro, C.A. Ultra-processed foods and recommended intake levels of nutrients linked to non-communicable diseases in Australia: Evidence from a nationally representative cross-sectional study. BMJ 2019, 9, 29544.
- Rauber, F.; da Costa Louzada, M.L.; Steele, E.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008–2014). Nutrients 2018, 10, 587.
- Steele, E.M.; Juul, F.; Neri, D.; Rauber, F.; Monteiro, C.A. Dietary share of ultra-processed foods and metabolic syndrome in the US adult population. Prev. Med. 2019, 125, 40–48.
- Rico-Campà, A.; Martínez-González, M.A.; Alvarez-Alvarez, I.; De Deus Mendonça, R.; De La Fuente-Arrillaga, C.; Gómez-Donoso, C.; Bes-Rastrollo, M. Association between consumption of ultra-processed foods and all cause mortality: SUN prospective cohort study. BMJ 2019, 365, l1949.
- Schnabel, L.; Kesse-Guyot, E.; Allès, B.; Touvier, M.; Srour, B.; Hercberg, S.; Buscail, C.; Julia, C. Association Between Ultraprocessed Food Consumption and Risk of Mortality Among Middle-aged Adults in France. JAMA Intern. Med. 2019, 179, 490–498.
- Kazmi, Z.; Fatima, I.; Perveen, S.; Malik, S.S. Monosodium glutamate: Review on clinical reports. Int. J. Food Prop. 2017, 20, 1807–1815.
- Singh, K.; Ahluwalia, P. Effect of monosodium glutamate on lipid peroxidation and certain antioxidant enzymes in cardiac tissue of alcoholic adult male mice. J. Cardiovasc. Dis. Res. 2012, 3, 12–18.
- Shukry, M.; El-Shehawi, A.M.; El-Kholy, W.M.; Elsisy, R.A.; Hamoda, H.S.; Tohamy, H.G.; Abumandour, M.M.; Farrag, F.A. Ameliorative Effect of Graviola (Annona muricata) on Mono Sodium Glutamate-Induced Hepatic Injury in Rats: Antioxidant, Apoptotic, Anti-inflammatory, Lipogenesis Markers, and Histopathological Studies. Animals 2020, 10, 1996.
- Ogbuagu, E.O.; Airaodion, A.I.; Okoroukwu, V.N. Hyperglycemic and hypocholesterolemic effect of monosodium glutamate in Wistar rats. Int. J. Res. Rept. Hematol. 2019, 2, 1–7.
- Bhattacharyya, S.; O-Sullivan, I.; Katyal, S.; Unterman, T.; Tobacman, J.K. Exposure to the common food additive carrageenan leads to glucose intolerance, insulin resistance and inhibition of insulin signalling in HepG2 cells and C57BL/6J mice. Diabetologia 2012, 55, 194–203.
- Pepino, M.Y.; Tiemann, C.D.; Patterson, B.W.; Wice, B.M.; Klein, S. Sucralose affects glycemic and hormonal responses to an oral glucose load. Diabetes Care 2013, 36, 2530–2535.
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of ultra-processed foods and health status: A systematic review and meta-Analysis. Br. J. Nutr. 2021, 125, 308–318.
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultra-processed food intake and risk of cardiovascular disease: Prospective cohort study (NutriNet-Santé). BMJ 2019, 365, l1451.
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Santé prospective cohort. BMJ 2018, 360, k322.
- Gómez-Donoso, C.; Sánchez-Villegas, A.; Martínez-González, M.A.; Gea, A.; de Deus Mendonça, R.; Lahortiga-Ramos, F.; Bes-Rastrollo, M. Ultra-processed food consumption and the incidence of depression in a Mediterranean cohort: The SUN Project. Eur. J. Nutr. 2020, 59, 1093–1103.
- Nardocci, M.; Polsky, J.Y.; Moubarac, J.-C. Consumption of ultra-processed foods is associated with obesity, diabetes and hypertension in Canadian adults. Can. J. Public Health 2021, 112, 421–429.
- Beslay, M.; Srour, B.; Méjean, C.; Allès, B.; Fiolet, T.; Debras, C.; Chazelas, E.; Deschasaux, M.; Wendeu-Foyet, M.G.; Hercberg, S.; et al. Ultra-processed food intake in association with BMI change and risk of overweight and obesity: A prospective analysis of the French NutriNet-Santé cohort. PLoS Med. 2020, 17, e1003256.
- Maggio, C.A.; Pi-Sunyer, F.X. Obesity and type 2 diabetes. Endocrinol. Metab. Clin. 2003, 32, 805–822.
- Srour, B.; Léopold, K.F.; Kesse-Guyot, E.; Allès, B.; Debras, C.; Druesne-Pecollo, N.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultraprocessed Food Consumption and Risk of Type 2 Diabetes Among Participants of the NutriNet-Santé Prospective Cohort. JAMA Intern. Med. 2020, 180, 283–291.
- Levy, R.B.; Rauber, F.; Chang, K.; da Costa Louzada, M.L.; Monteiro, C.A.; Millett, C.; Vamos, E.P. Ultra-processed food consumption and type 2 diabetes incidence: A prospective cohort study. Clin. Nutr. 2020, 40, 3608–3614.
- Llavero-Valero, M.; Escalada-San Martín, J.; Martínez-González, M.A.; Basterra-Gortari, F.J.; de la Fuente-Arrillaga, C.; Bes-Rastrollo, M. Ultra-processed foods and type-2 diabetes risk in the SUN project: A prospective cohort study. Clin. Nutr. 2021, 40, 2817–2824.
- Duan, M.-J.; Vinke, P.C.; Navis, G.; Corpeleijn, E.; Dekker, L.H. Ultra-processed food and incident type 2 diabetes: Studying the underlying consumption patterns to unravel the health effects of this heterogeneous food category in the prospective Lifelines cohort. BMC Med. 2022, 20, 7.
- Sartorelli, D.S.; Crivellenti, L.C.; Zuccolotto, D.C.C.; Franco, L.J. Relationship between minimally and ultra-processed food intake during pregnancy with obesity and gestational diabetes mellitus. Cad. Saude. Publica 2019, 35, e00049318.
- Leone, A.; Martínez-González, M.Á.; Craig, W.; Fresán, U.; Gómez-Donoso, C.; Bes-Rastrollo, M. Pre-gestational consumption of ultra-processed foods and risk of gestational diabetes in a mediterranean cohort. The SUN project. Nutrients 2021, 13, 2202.
- Silva, C.F.M.; Saunders, C.; Peres, W.; Folino, B.; Kamel, T.; dos Santos, M.S.; Padilha, P. Effect of ultra-processed foods consumption on glycemic control and gestational weight gain in pregnant with pregestational diabetes mellitus using carbohydrate counting. PeerJ 2021, 9, e10514.
- Da Costa Louzada, M.L.; Baraldi, L.G.; Steele, E.M.; Martins, A.P.B.; Canella, D.S.; Moubarac, J.-C.; Levy, R.B.; Cannon, G.; Afshin, A.; Imamura, F. Consumption of ultra-processed foods and obesity in Brazilian adolescents and adults. Prev. Med. 2015, 81, 9–15.
- McRae, M.P. Dietary Fiber Intake and Type 2 Diabetes Mellitus: An Umbrella Review of Meta-analyses. J. Chiropr. Med. 2018, 17, 44–53.
- Partula, V.; Deschasaux, M.; Druesne-Pecollo, N.; Latino-Martel, P.; Desmetz, E.; Chazelas, E.; Kesse-Guyot, E.; Julia, C.; Fezeu, L.K.; Galan, P.; et al. Associations between consumption of dietary fibers and the risk of cardiovascular diseases, cancers, type 2 diabetes, and mortality in the prospective NutriNet-Santé cohort. Am. J. Clin. Nutr. 2020, 112, 195–207.
- Gbadamosi, M.A.; Tlou, B. Modifiable risk factors associated with non-communicable diseases among adult outpatients in Manzini, Swaziland: A cross-sectional study. BMC Public Health 2020, 20, 665.
- Sarmento, R.A.; Antonio, J.P.; de Miranda, I.L.; Nicoletto, B.B.; de Almeida, J.C. Eating Patterns and Health Outcomes in Patients With Type 2 Diabetes. J. Endocr. Soc. 2018, 2, 42–52.
- Garshick, M.; Mochari-Greenberger, H.; Mosca, L. Reduction in dietary trans fat intake is associated with decreased LDL particle number in a primary prevention population. Nutr. Metab. Cardiovasc. 2014, 24, 100–106.
- Kesse-Guyot, E.; Chaltiel, D.; Fezeu, L.K.; Baudry, J.; Druesne-Pecollo, N.; Galan, P.; Deschamps, V.; Touvier, M.; Julia, C.; Hercberg, S. Association between adherence to the French dietary guidelines and the risk of type 2 diabetes. Nutrition 2021, 84, 111107.
- Michaud, M.; Balardy, L.; Moulis, G.; Gaudin, C.; Peyrot, C.; Vellas, B.; Cesari, M.; Nourhashemi, F. Proinflammatory Cytokines, Aging, and Age-Related Diseases. J. Am. Med. Dir. Assoc. 2013, 14, 877–882.
- Müller, L.; Benedetto, S.D.; Pawelec, G. The immune system and its dysregulation with aging. Subcell Biochem. 2019, 91, 21–43.

