Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Lydia Giménez-Llort | -- | 2126 | 2022-06-08 15:10:35 | | | |
| 2 | Lydia Giménez-Llort | -516 word(s) | 1610 | 2022-06-08 16:26:30 | | | | |
| 3 | Lydia Giménez-Llort | + 8 word(s) | 1618 | 2022-06-08 16:36:00 | | | | |
| 4 | Rita Xu | -7 word(s) | 1611 | 2022-06-09 03:38:10 | | | | |
| 5 | Rita Xu | -3 word(s) | 1608 | 2022-06-10 08:39:32 | | | | |
| 6 | Rita Xu | -73 word(s) | 1535 | 2022-06-10 09:55:48 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Giménez-Llort, L.; Ferrer, A.; Ferrer-Torres, A. Misophonia. Encyclopedia. Available online: https://encyclopedia.pub/entry/23840 (accessed on 26 July 2026).
Giménez-Llort L, Ferrer A, Ferrer-Torres A. Misophonia. Encyclopedia. Available at: https://encyclopedia.pub/entry/23840. Accessed July 26, 2026.
Giménez-Llort, Lydia, Antonia Ferrer, Antonia Ferrer-Torres. "Misophonia" Encyclopedia, https://encyclopedia.pub/entry/23840 (accessed July 26, 2026).
Giménez-Llort, L., Ferrer, A., & Ferrer-Torres, A. (2022, June 08). Misophonia. In Encyclopedia. https://encyclopedia.pub/entry/23840
Giménez-Llort, Lydia, et al. "Misophonia." Encyclopedia. Web. 08 June, 2022.
Copy Citation
Misophonia is a complex neurophysiological and behavioral disorder of multifactorial origin and is characterized by an increased physiological and emotional response produced by intolerance to specific auditory stimuli.
misophonia
epidemiology
etiology
1. Introduction
It has also been described as a form of sound intolerance, in which hyper-reactivity and selective aversion to one type of sound are present [1]. Additionally, misophonia has been considered a new mental disorder [2][3]. There is currently debate whether misophonia is an auditory or psychiatric disorder per se. The main reason for the reluctance to include misophonia among mental disorders is the danger of stigmatizing and “pathologizing” the medical picture [4]. On the other hand, it is considered that misophonia cannot be classified as an auditory disorder since no relationship has been found between it and hearing thresholds, as the disorder can occur in people with normal hearing, with hearing loss, or with some auditory pathology [4]. Furthermore, misophonia can develop in the absence of any peripheral or central auditory pathology [5]. Additionally, the specificity of the triggering stimuli suggests that the symptoms are unlikely to be caused by an alteration of the auditory system [6].
Although the prevalence of misophonia is not precisely known, the figure is estimated to be close to 20% of the population or 6% showing significant associated functional impairment as reported in clinical settings [7]. Misophonia may coexist with other hearing and psychiatric disorders, and it can be confused with other hearing conditions, so the percentage of affected individuals may be higher [7][8][9], with it being considered an underdiagnosed disorder. Misophonia has a significant impact on the sufferer’s life, as their maladaptive and avoidant behaviors interfere with the performance of work or academic tasks and cause significant impairment in their interpersonal relationships [1]. In response to exposure to the triggering stimulus, the individual experiences a series of physical and emotional reactions of such intensity that they affect their functionality and well-being (see Figure 1). The intensity of the misophonic responses varies depending on the emitting source, being more intense when the sound is produced by family members or acquaintances [4][10]. Research and health care regarding misophonia are currently scarce but slowly increasing in recent years, and the first consensus definition has been published [11]. First, there is a lack of sufficient diagnostic criteria to aid in the correct classification of misophonia and its recognition as a distinct disorder. In addition, little is known about its etiology, and insufficient assessment tools are available to measure misophonic symptoms accurately. As expected, there are no protocols for its treatment that are scientifically supported through randomized clinical trials.
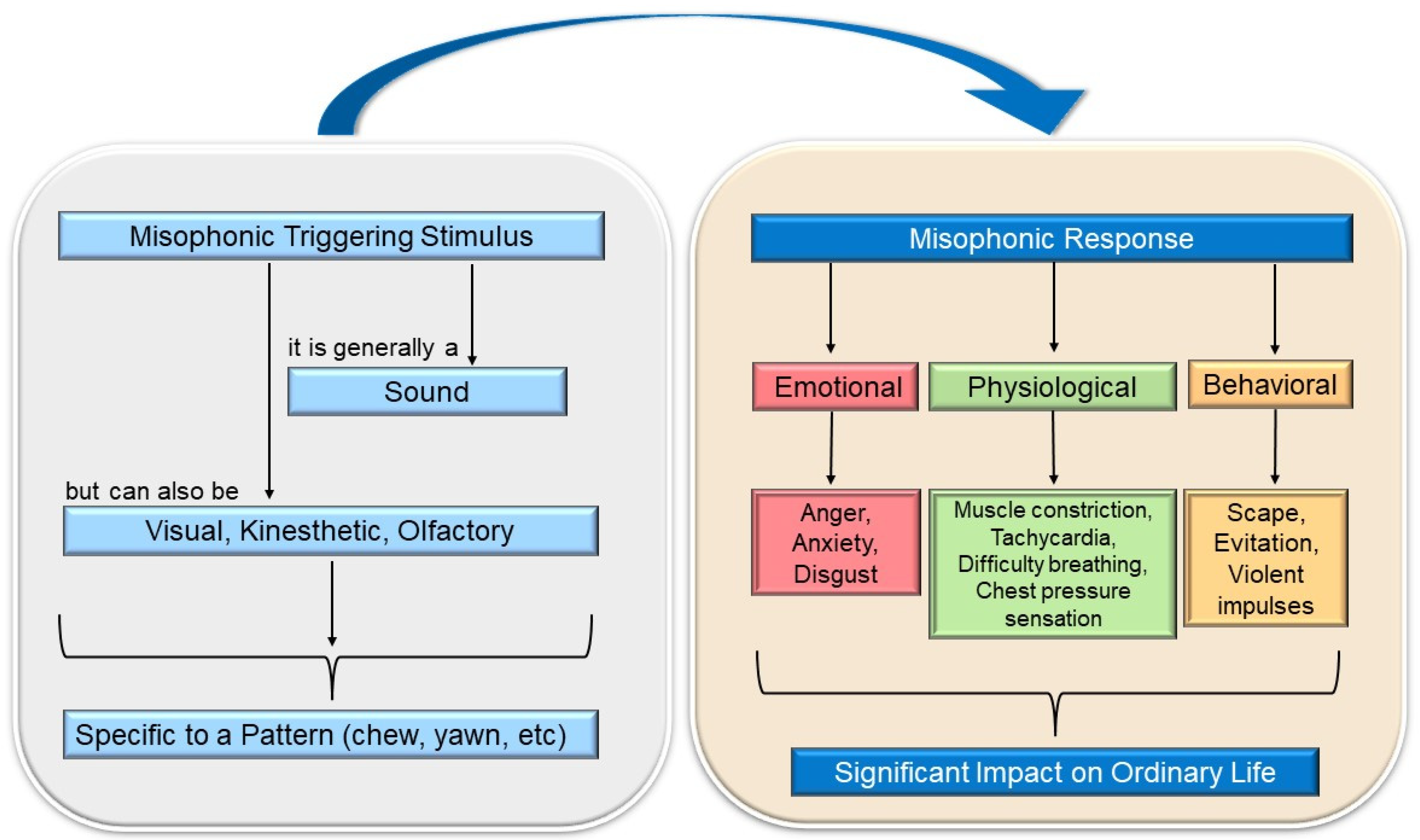
Figure 1. Brief explanatory diagram of misophonia (own elaboration, from 10.3390/ijerph19116790).
2. Triggering or Misophonic Stimulus and Symptomatology
The stimuli that trigger the aversive reaction are called “triggering sounds”, “misophonic stimuli”, or “misophonic sounds” and are characterized by sharing the same pattern, regardless of the decibel level [12]. The individual’s responses following the exposure to the misophonic stimulus are referred to as “misophonic responses” . These can be physical and/or emotional in nature. The former is often muscle constriction and increased heart rate [1][13]; although one may also experience a feeling of pressure in the chest, arms, head, or throughout the body, as well as increased body temperature, physical pain, or shortness of breath . On the other hand, the emotional misophonic response may manifest with reactions such as anger, anxiety, disgust, avoidance behavior, escape, and/or feelings of being overwhelmed. The person suffering from misophonia recognizes that their responses are unwanted, uncontrolled, sometimes excessive, and unacceptable [14], but they still feel offended by those emitting the misophonic stimulus [4]. Despite this, too, they may have violent impulses toward the source of the misophonic sound [15]. In fact, anger is the primary emotional response to misophonia. One study reported that irritation (59.9%) was the most common misophonic response, and 28.6% of patients reported aggressive verbal behaviors. Even 16.7% admitted physical aggression towards objects [14].
The set of emotional reactions leads the individual to carry out maladaptive behaviors, such as asking the person emitting the misophonic stimulus to stop, arguing with them, or presenting an excessive desire to escape from the stimulus [16]. Avoidance behaviors are frequent, and although they provide the individual with momentary comfort, they worsen and maintain the symptomatology [17]. In addition, misophonia can contribute to the development of other health problems, such as behavioral disorders, emotional reactivity , difficulties in regulating emotions [10][18], and impaired quality of life [1][10]. It also appears to be common for people with misophonia to suffer abuse from others due to their symptoms and maladaptive behaviors. For example, it has been noted that misophonic patients routinely share on internet forums that they are accused of being “crazy” or “troublemakers” by people in their immediate environment [1].
It has been defined that the stimuli that trigger the aversive reaction called “triggering sounds” or “misophonic sounds”, are characterized by sharing the same pattern, regardless of their physical properties such as intensity, frequency, harshness, or decibel level . Empirical studies have shown that misophonia is not limited to an aversion to loud, sharp, or harsh sounds; since even soft sounds can trigger the misophonic response (e.g., slurping sounds) [4]. In addition, misophonic sounds vary between people, so they are believed to be conditioned to individual, learning, and contextual differences. This indicates that the auditory stimulus does not produce the adverse reaction simply because of its sonic properties but is also significantly influenced by who or what elicits it . Initially, it was proposed that the patient’s discomfort was elicited by the presence or anticipation of a specific sound produced by a person [14]. However, years later, it was found that the triggering sounds did not always come from human activities but were everyday sounds [1] influenced by the context and individual characteristics of the patient [19][20] as well as sounds emitted by animals or objects [20][21].
The most frequent triggering stimuli for misophonic symptoms are sounds emitted while eating [23] (e.g., chewing, crunching food, slurping, etc.), nasal sounds (e.g., breathing, sniffing, sneezing), and sounds made with the throat (such as throat clearing) [24]. Machine-related sounds are also common, such as those emitted by the computer keyboard, the ticking of the clock, the coffee maker, the stapler, or hair dryers, among others [25]. These are some examples, but it should be noted that triggering sounds are very varied and, although they are usually everyday [17][26], they are influenced by the context and the individual characteristics of the patient [20]. Recent research has found that the triggering stimulus can have different sensory modalities, not limited to sound alone [21][27]. That is, visual or kinesthetic stimuli related to the triggering auditory stimulus can also elicit the aversive response. For example, a person whose misophonic sound is the sound of chewing may generalize the aversive behavior to visual stimuli associated with the image of a particular food, e.g., fried food. In addition, another study has found that imagining a misophonic sound can trigger symptoms very similar to those experienced when hearing the actual sound [13].
Consequently, probably the best term to use is “triggering stimulus” or “misophonic stimulus”, since the concept of misophonic sound does not refer only to an auditory sensory modality. An unresolved unknown is whether the misophonic stimulus also produces aversive reactions when produced by the same patient. Although in a study with a sample of 92 misophonic patients, it was indicated that most do not experience symptoms when they themselves emit the triggering sound (e.g., chewing) [28].
3. The Evolution of the Study of Misophonia
Figure 2 illustrates the timeline of the outstanding studies related to misophonia. In the 1990s, Marsha Johnson, an American audiologist, described for the first time what she called ‘Sensitivity to Soft Sound or Selective Sound Sensitivity Syndrome’, abbreviated as 4S syndrome [15]. With this label, she described a syndrome characterized by an evident intolerance to specific sounds unique to each individual [29]. Johnson called the annoying sound a “trigger sound”, and emphasized that associated visual or olfactory stimuli could also provoke the misophonic response [15].
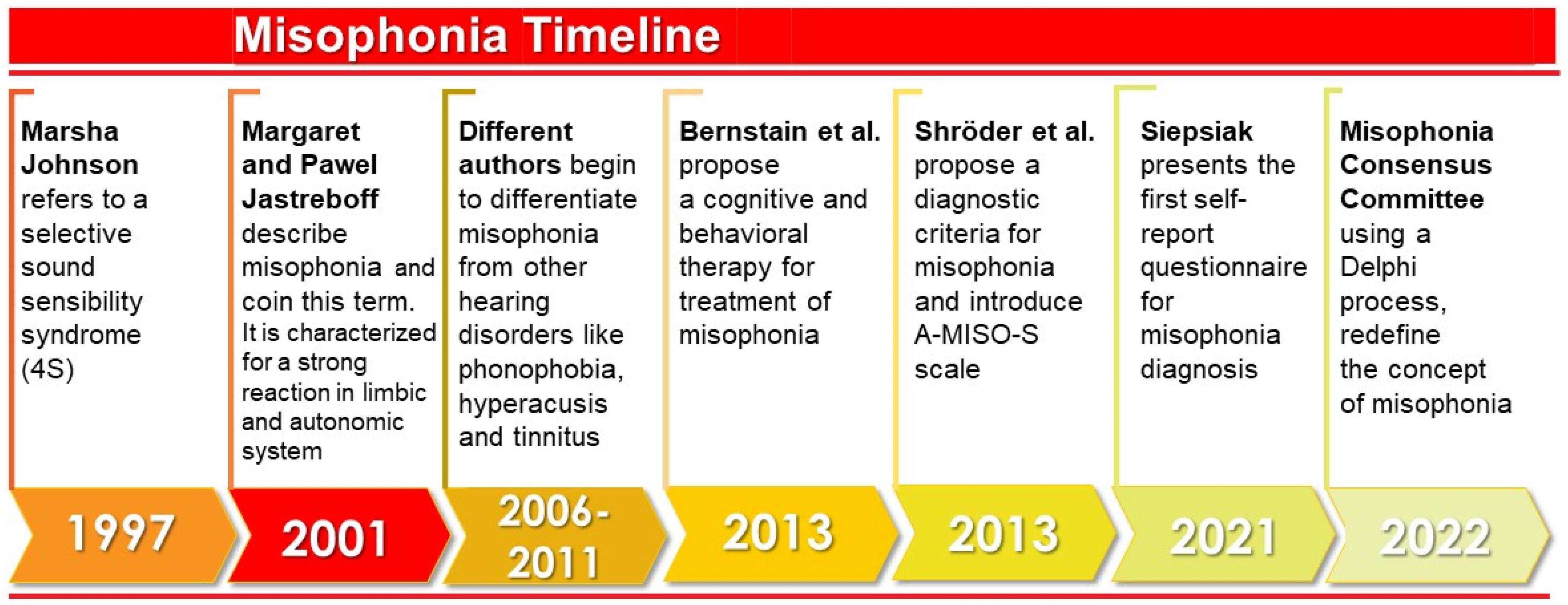
Figure 2. Timeline of outstanding studies related to misophonia (Own elaboration).
In 2001, the authors Margaret and Pawel Jastreboff first used the term misophonia to describe a series of negative limbic and autonomic system reactions resulting from perceiving specific sounds . It was suggested that this response was caused by increased functional connections between the auditory system and the limbic system. According to these authors, the auditory system functions normally, but at the behavioral level negative reactions are evoked. In other words, misophonia does not imply an increased activation of the auditory system, but the problem lies in the emotional response of the patients to the triggering sound .
In later years, findings made it possible to differentiate misophonia from other diagnoses such as hyperacusis or phonophobia. It was determined that misophonia was a separate disorder since, unlike hyperacusis (decreased tolerance to sound), the symptomatology was associated exclusively with one type of sound; and it was distinct from phonophobia (fear of sounds) because the primary emotional response differed [5]. Although misophonia can occur in conjunction with these pathologies, it is also seen in isolation [5].
With sufficient evidence to consider misophonia as an independent disorder, outreach efforts began in the medical community to publicize this condition and raise awareness of its impact on the individual’s life [25]. In addition, work was done to understand the prevalence of misophonia [24] and to understand the experience of misophonic individuals through case studies [29][30][31].
References
- Siepsiak, M.; Dragan, W. Misophonia—A Review of Research Results and Theoretical Conceptions. Psychiatr. Polska 2019, 53, 447–458.
- Daniels, E.C.; Rodriguez, A.; Zabelina, D.L. Severity of misophonia symptoms is associated with worse cognitive control when exposed to misophonia trigger sounds. PLoS ONE 2020, 15, e0227118.
- Cassiello-Robbins, C.; Anand, D.; McMahon, K.; Brout, J.; Kelley, L.; Rosenthal, M.Z. A preliminary investigation of the association between misophonia and symptoms of psychopathology and personality disorders. Front. Psychol. 2021, 11, 3842.
- Taylor, S. Misophonia: A new mental disorder? Med. Hypotheses 2017, 103, 109–117.
- Møller, A.R. Misophonia, Phonophobia, and Exploding Head Syndrome. In Textbook of Tinnitus; Springer: New York, NY, USA, 2011; pp. 25–27.
- Duddy, D.F.; Oeding, K.A.M. Misophonia: An Overview. Semin. Hear. 2014, 35, 84–91.
- Ferrer-Torres, A.; Giménez-Llort, L. Confinement and the Hatred of Sound in Times of COVID-19: A Molotov Cocktail for People with Misophonia. Front. Psychiatry 2021, 12, 663.
- Potgieter, I.; MacDonald, C.; Partridge, L.; Cima, R.; Sheldrake, J.; Hoare, D.J. Misophonia: A scoping review of research. J. Clin. Psychol. 2019, 75, 203–1218.
- Naylor, J.; Caimino, C.; Scutt, P.; Hoare, D.J.; Baguley, D.M. The Prevalence and Severity of Misophonia in a UK Undergraduate Medical Student Population and Validation of the Amsterdam Misophonia Scale. Psychiatr. Q. 2020, 92, 609–619.
- Guetta, R.E.; Cassiello-Robbins, C.; Trumbull, J.; Anand, D.; Rosenthal, M.Z. Examining emotional functioning in misophonia: The role of affective instability and difficulties with emotion regulation. PLoS ONE 2022, 17, e0263230.
- Swedo, S.E.; Baguley, D.M.; Denys, D.; Dixon, L.J.; Erfanian, M.; Fioretti, A.; Jastreboff, P.J.; Kumar, S.; Rosenthal, M.Z.; Rouw, R.; et al. Consensus Definition of Misophonia: A Delphi Study. Front. Neurosci. 2022, 224, 841816.
- Jastreboff, M.M.; Jastreboff, P.J. Components of decreased sound tolerance: Hyperacusis, misophonia, phonophobia. ITHS News Lett. 2001, 2, 1–5.
- Ferrer-Torres, A.; Giménez-Llort, L. Sounds of Silence in Times of COVID-19: Distress and Loss of Cardiac Coherence in People with Misophonia Caused by Real, Imagined or Evoked Triggering Sounds. Front. Psychiatry 2021, 12, 638949.
- Schröder, A.; Vulink, N.; Denys, D. Misophonia: Diagnostic Criteria for a New Psychiatric Disorder. PLoS ONE 2013, 8, e54706.
- Bernstein, R.E.; Angell, K.L.; Dehle, C.M. A brief course of cognitive behavioural therapy for the treatment of misophonia: A case example. Cogn. Behav. Ther. 2013, 6, E16.
- Sanchez, T.G.; Da Silva, F.E. Familial misophonia or selective sound sensitivity syndrome: Evidence for autosomal dominant inheritance? Braz. J. Otorhinolaryngol. 2018, 84, 553–559.
- Palumbo, D.B.; Alsalman, O.; De Ridder, D.; Song, J.-J.; Vanneste, S. Misophonia and Potential Underlying Mechanisms: A Perspective. Front. Psychol. 2018, 9, 953.
- Cassiello-Robbins, C.; Anand, D.; McMahon, K.; Guetta, R.; Trumbull, J.; Kelley, L.; Rosenthal, M.Z. The mediating role of emotion regulation within the relationship between neuroticism and misophonia: A preliminary investigation. Front. Psychiatry 2020, 11, 847.
- Hansen, H.A.; Leber, A.B.; Saygin, Z.M. What sound sources trigger misophonia? Not just chewing and breathing. J. Clin. Psychol. 2021, 77, 2609–2625.
- Jastreboff, P.J.; Jastreboff, M.M. Tinnitus retraining therapy: A different view on tinnitus. ORL J. Oto-Rhino-Laryngol. Its Relat. Spec. 2006, 68, 23–29.
- Cavanna, A.E.; Seri, S. Misophonia: Current perspectives. Neuropsychiatr. Dis. Treat. 2015, 11, 2117–2123.
- Dozier, T.H.; Lopez, M.; Pearson, C. Proposed Diagnostic Criteria for Misophonia: A Multisensory Conditioned Aversive Reflex Disorder. Front. Psychol. 2017, 8, 1975.
- Vitoratou, S.; Uglik-Marucha, N.; Hayes, C.; Erfanian, M.; Pearson, O.; Gregory, J. Item Response Theory Investigation of Misophonia Auditory Triggers. Audiol. Res. 2021, 11, 51.
- Zhou, X.; Wu, M.S.; Storch, E.A. Misophonia symptoms among Chinese university students: Incidence, associated impairment, and clinical correlates. J. Obs.-Compuls. Relat. Disord. 2017, 14, 7–12.
- Schwartz, P.; Leyendecker, J.; Conlon, M. Hyperacusis and misophonia: The lesser-known siblings of tinnitus. Minn. Med. 2011, 94, 42–43.
- McGeoch, P.D.; Rouw, R. How everyday sounds can trigger strong emotions: ASMR, misophonia and the feeling of wellbeing. BioEssays 2020, 42, 2000099.
- Webb, J. β-Blockers for the Treatment of Misophonia and Misokinesia. Clin. Neuropharmacol. 2022, 45, 13–14.
- Quek, T.; Ho, C.; Choo, C.; Nguyen, L.; Tran, B.; Ho, R. Misophonia in Singaporean Psychiatric Patients: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1410.
- Dozier, T.H. Etiology, composition, development and maintenance of misophonia: A conditioned aversive reflex disorder. Psychol. Thought 2015, 8, 114–129.
- Tunç, S.; Başbuğ, H.S. An extreme physical reaction in misophonia: Stop smacking your mouth. Psychiatry Clin. Psychopharmacol. 2017, 27, 416–418.
- Vidal, C.; Vidal, L.M.; Lage, M. Misophonia: Case report. Eur. Psychiatry 2017, 41, 644.
More
Information
Subjects:
Psychology, Clinical
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.4K
Revisions:
6 times
(View History)
Update Date:
10 Jun 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No