Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Andrew Young Chang | -- | 1095 | 2022-05-17 20:12:04 |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Chang, A.; Rwebembera, J. History of Rheumatic Fever/ Rheumatic Heart Disease Control. Encyclopedia. Available online: https://encyclopedia.pub/entry/23023 (accessed on 24 July 2026).
Chang A, Rwebembera J. History of Rheumatic Fever/ Rheumatic Heart Disease Control. Encyclopedia. Available at: https://encyclopedia.pub/entry/23023. Accessed July 24, 2026.
Chang, Andrew, Joselyn Rwebembera. "History of Rheumatic Fever/ Rheumatic Heart Disease Control" Encyclopedia, https://encyclopedia.pub/entry/23023 (accessed July 24, 2026).
Chang, A., & Rwebembera, J. (2022, May 17). History of Rheumatic Fever/ Rheumatic Heart Disease Control. In Encyclopedia. https://encyclopedia.pub/entry/23023
Chang, Andrew and Joselyn Rwebembera. "History of Rheumatic Fever/ Rheumatic Heart Disease Control." Encyclopedia. Web. 17 May, 2022.
Copy Citation
Rheumatic heart disease and rheumatic fever (RHD/RF) contributed to a substantial health burden upon the entire globe in the 19th and 20th centuries. As advances in public health improved throughout regions of the world now considered to be high-income countries (HICs), it was largely eradicated in these settings. Regrettably, RHD/RF remain endemic in low- and middle-income countries (LMICs). The historical context within which RHD/RF control was achieved in HICs may be of interest to researchers and policymakers active in the resurgent interest in RHD/RF seen in the prior two decades.
RHD
Rheumatic Heart Disease
Public Health
History of Medicine
History of Science
I. Historical Context of Advances in Rheumatic Heart Disease and Rheumatic Fever Control
Much of what is known today about the pathogenesis, diagnosis, prevention, and treatment of this disease continuum originates from what are now considered high-income countries in the mid-20th century, where improved socioeconomic standards and access to healthcare (boosted by extensive biomedical research) resulted in a striking reduction of disease burden. Once the disorder was all but wiped out from high-income nations, however, it receded from public and academic attention, leading to a stagnation in control in low-and middle-income countries (LMICs). This period lasted for nearly a generation, but the past two decades have seen a reemergence of global RHD research and advocacy, which has largely been grassroots, conducted in low-resource settings in populations where RHD remains endemic. Figure 1 provides an overview of these sequential phases, which are discussed in greater detail in the subsequent sections.
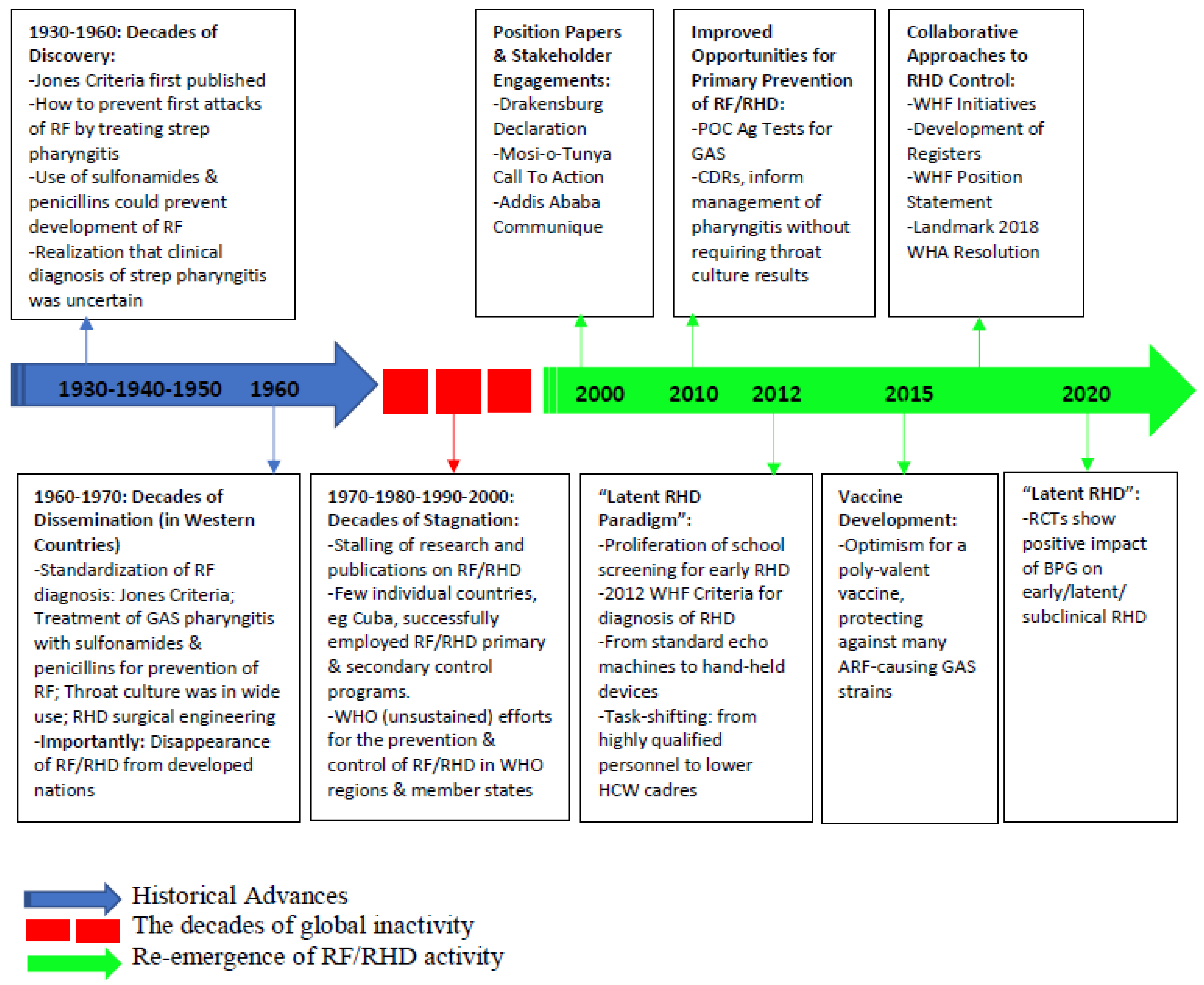
Figure 1. Abbreviations: GAS, group A Streptococcus; RF, rheumatic fever; ARF, acute rheumatic fever; RHD, rheumatic heart disease; POC, point of care; Ag, antigen; CDR, clinical decision rule; BPG, benzyl benzathine penicillin; HCW, health care worker; RCT, randomized clinical trial; WHA, World Health Assembly; WHF, World Heart Federation; WHO, World Health Organization.
1. Decades of Discovery: 1930s–1950s
Concurrent with the growth and advancement of the discipline of microbiology, Streptococcus [1], and shortly thereafter, Streptococcus pyogenes (group A strep, GAS), were first identified during the ‘golden age of bacteriology’ [2] in the late 19th and early 20th century. Simultaneously, RF was gaining attention as the leading cause of death among individuals between 5 and 20 years, even in nations now considered to be high-income countries [3,4], with the critical link between RF and GAS established by 1889 [5]. By 1944, the diagnosis of RF was standardized by Dr. T. Duckett Jones, (The Jones Criteria [6,7,8]), although treatment remained limited to salicylates and bedrest [4]. By the 1950s, antibiotics became even more widely available [9,10] and strong evidence emerged that proper treatment of GAS pharyngitis, both with sulfonamides [4,9] and penicillins [11], could prevent the development of RF [4,12,13,14]. Thus, the utility of secondary antibiotic prophylaxis to prevent RF recurrence was established [15,16,17], with long-acting intramuscular formulations developed [18], and a monthly administration of this medication was found to effectively suppress RF recurrences [16,19,20,21,22]. Monthly injections of intramuscular long-acting benzathine penicillin G (BPG) were subsequently shown to be superior to daily oral penicillin G in the prevention of streptococcal infections and recurrences of RF [23], establishing a key tenet of RHD management which is still accepted as dogma today. In addition to the medical management of RHD, this time period was also an era of significant pioneering in the surgical management of valvular RHD sequelae. For example, the first recorded valvotomy for aN RHD patient was performed at the House of the Good Samaritan (HGS), an RF/RHD specialty hospital, in 1923 [4].
2. Decades of Dissemination: 1960s–1970s
While improved living conditions in high-resource settings (less household crowding, better personal hygiene, and improved public health infrastructure) drove down the incidence of RF even before many of the scientific advances described above were realized [24,25,26], targeted advocacy, education, and awareness of the diseases in the second half of the 20th century further accelerated progress toward eradication. Among the leading advocates of such measures was the American Heart Association, which had largely coalesced to fight what it dubbed ‘Childhood’s Greatest Enemy' [27]. By the 1970s, the annual incidence of RF in the United States had plummeted to 0.6 per 100,000 population in those aged 5 to 19 years [28,29], Similar gains were seen during this time in other high-income countries (much of Europe and Australia), and in some isolated lower income countries (such as Cuba [25] and Costa Rica [30]) which implemented comprehensive RF prevention programs without the benefit of improved socio-economic conditions at that point in time.
3. Decades of Stagnation: 1970s–2000s
Following this period of rapid advancement, RF and RHD were largely controlled in high-income countries. As such, appetite for new research (and funding for such research) in RF/RHD largely dissipated. Regrettably, this waning of interest and investigative efforts [31] only reflected the reduction in RF/RHD burden among a fraction of the world’s population. More unfortunately, those left behind represented those at highest social risk for developing--and suffering adverse outcomes from--the disese. During this period, the World Health Organization (WHO) briefly invested in a large-scale program to disseminate knowledge and best practices around the globe [32,33,34,35,36]. However, these efforts were not sustained, as the problem of RF/RHD was progressively overshadowed and ultimately dwarfed by the epidemics of malaria, tuberculosis, yellow fever, and especially—HIV/AIDS. Consequently, despite the persistent burden (and known interventions known to reduce this burden) of RF/RHD, it was steadily relegated to the status of a ‘neglected tropical disease’.
4. A Renewal of Attention: 2000s to Present
The last two decades, however, have seen an encouraging resurgence of interest in RF/RHD. This has, in large part, been due to both the growth of global health as a discipline as well as the development of cardiac imaging technologies suited for use in low-resource settings. In particular, echocardiography ultrasound devices have become cheaper, lighter, and more portable (by incorporating small-form factors and rechargeable battery power supplies), resulting in their use to unmask a substantial number of children and adults living with previously-undiagnosed RHD in LMICs [37,38,39,40,41]. This has provided irrefutable evidence of the persistent and disparate global burden of the ongoing RHD epidemic. In response, calls to action began to emerge from research groups and professional societies [31,42,43], particularly in sub-Saharan Africa, were regional meetings were convened and produced critical position papers and guiding statements to drive the global RHD control agenda [44,45,46]. These, among other regional academic and advocacy efforts, were crowned by the 2018 World Health Assembly Resolution to end RHD [47]. In response, global research and funding opportunities have steadily increased, particularly calls for action to apply exciting modern technologies and research methodologies to build new knowledge in the RHD management cascade.
This article was adapted from the MDPI article by the authors at: https://www.mdpi.com/2076-0817/11/2/179
Information
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.6K
Entry Collection:
Hypertension and Cardiovascular Diseases
Revision:
1 time
(View History)
Update Date:
17 May 2022
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No