Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Matt Walczak | -- | 2505 | 2022-04-20 06:24:52 | | | |
| 2 | Matt Walczak | + 55 word(s) | 2560 | 2022-04-20 06:26:16 | | | | |
| 3 | Rita Xu | Meta information modification | 2560 | 2022-04-20 08:01:54 | | | | |
| 4 | Rita Xu | Meta information modification | 2560 | 2022-04-22 07:50:53 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Walczak, M.; Boro, R.; Iye, P.; Jang, J. Coccidioidomycosis. Encyclopedia. Available online: https://encyclopedia.pub/entry/21972 (accessed on 01 August 2026).
Walczak M, Boro R, Iye P, Jang J. Coccidioidomycosis. Encyclopedia. Available at: https://encyclopedia.pub/entry/21972. Accessed August 01, 2026.
Walczak, Matt, Ryan Boro, Prema Iye, Jeachul Jang. "Coccidioidomycosis" Encyclopedia, https://encyclopedia.pub/entry/21972 (accessed August 01, 2026).
Walczak, M., Boro, R., Iye, P., & Jang, J. (2022, April 20). Coccidioidomycosis. In Encyclopedia. https://encyclopedia.pub/entry/21972
Walczak, Matt, et al. "Coccidioidomycosis." Encyclopedia. Web. 20 April, 2022.
Copy Citation
Coccidioidomycosis, also known as Valley fever, is an endemic fungal infection commonly found in the southwestern parts of the United States. However, the disease has seen an increase in both in its area of residency and its prevalence. This entry compiles some of the latest information on the epidemiology, current and in-development pharmaceutical approaches to treat the disease, trends and projections, diagnostic concerns, and the overlapping dynamics of coccidioidomycosis and COVID-19, including in special populations. This entry provides an overview of the current diagnostic and therapeutic strategies and identifies areas of future development.
antifungal agents
coccidioidomycosis
Coccidioides spp.
1. Introduction
Coccidioidomycosis (CM), also known as San Joaquin Valley fever or Valley fever, is a fungal disease endemic in certain parts of the Unites States, predominantly in California and Arizona [1][2]. Valley fever is caused by Coccidioides, a dimorphic fungus, first described in 1892 [3]. Since 2002, it has been recognized as two separate species, including the previously categorized C. immitis, and the newer designated C. posadasii [4]. C. immitis mainly resides in California, Washington State, Arizona, and Utah, while C. posadasii is mostly found in Arizona, New Mexico, Texas, Northern Mexico (Baja California, Chihuahua, Nuevo León, Sinaloa, Sonora, and Tamaulipas), and parts of Central (Guatemala and Honduras) and South America (Northern and Central Argentina, Bolivia, Colombia, Northeastern Brazil, Paraguay, and Venezuela) [5][6][7][8] (Figure 1).

The Coccidioides spp. is a dimorphic fungus that grows as a mold in the environment at temperatures below 37 °C, and as a spherule in the host (Figure 2) [9]. Coccidioides exists as a saprotroph in the soil, feeding off decayed organic matter such as hyphae, and forms asexual spores known as arthroconidia. Soil disturbance distributes the arthroconidia into the air, and once inhaled by a living host, it converts to a parasitic state, ciphering nourishment from the host and forming endospores. The endospores eventually transform into spherules containing their own endospores, and, once ruptured, spread their contents to restart the parasitic cycle in the host, and possibly re-enter the soil in the environment [10]. More recent findings, including genomic analysis [11], support an alternative hypothesis, where the species acts as an endozoan living in mammalian hosts without causing detectable disease. Then, once the host dies, the organism establishes itself in the environment, utilizing its prior host’s dead biological matter to flourish [12]. Some mammals, such as dogs [13], appear to be reservoirs of the disease [14], but no evidence exists for zoonotic transmission [1].
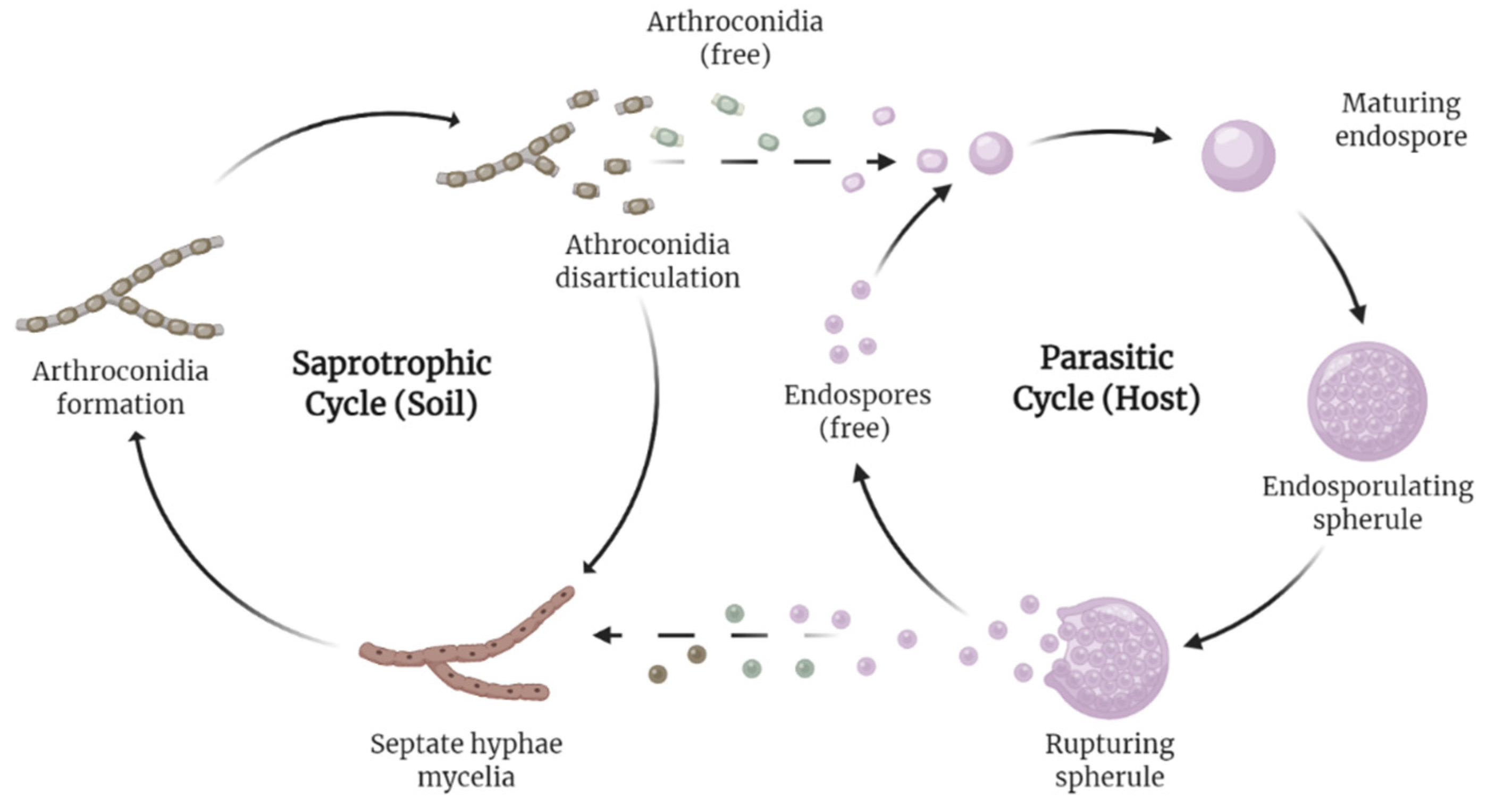
Figure 2. Life cycle of Coccidioides. The fungus possesses a dimorphic life cycle, living saprotrophically in soil and parasitically in its host at different intervals of the cycle. Recently, an alternative hypothesis formed, suggesting the species may be endozoan.
2. Burden and Projections
Trends and projections reveal a situation where CM appears to be an increasing concern. Case occurrence increased immensely, moving from an age-adjusted incidence of 5.3 cases in endemic areas in 1998 to 42.6 per 100,000 in 2011 [15]. Cases may be underreported, with only 22 U.S. states having the disease reportable. It is suggested the true numbers of symptomatic cases are 6 to 14 times greater than what is reported to public health authorities [16]. While, as stated previously, the disease resides mostly in CA and AZ, more recent evidence of local infection in Washington [17] and environmental demonstration in Utah appeared [18]. The first documented case of CM in Africa occurred in a patient without a prior history of traveling outside of Uganda [19]. Latin America poses an emerging phenomenon for CM as the area historically contains an underserved population, surveillance of the disease is poor, and the numbers are observed less than they are officially recorded [20]. Much of the research done geographically exists in the areas of Mexico bordering the United States [20]. In Central America, the arid and semiarid countries of Guatemala and Honduras possess the largest presence of CM relative to the rest of the area [20]. Within South America, Brazil, with its established resources geared towards mycology research, contains some of the highest reported CM data relative to its neighboring nations [20]. The endemic areas observed in Argentina, while large in size, contained a small number of cases before the year 2000, with 63 of the 128 documented cases of CM occurring after 2000 [6].
Coccidioidomycosis manifests itself in the human population across the spectrum of clinical severity. Patients may present as asymptomatic in its mildest form, trending worse in presentation as pneumonic, pulmonary, fibro-cavitary, and disseminated [15]. An estimated 60% of all CM cases are asymptomatic [15], and the number of infections per year has risen to approximately 150,000 (one-half to two-thirds being subclinical) [1]. Most patients are protected from secondary infections [1]. Out of these estimated cases, 50,000 likely produced an illness warranting medical attention, 10,000–20,000 are diagnosed and reported, 2000–3000 produced pulmonary sequelae, 600–1000 moved to disseminated infection (spreading beyond pulmonary), and 160 resulted in death [21]. Because the most common clinical syndrome resulting from infection is community-acquired pneumonia (CAP), proper early diagnosis proves difficult due to many possible causes of CAP [22]. Disseminated disease can occur in virtually any site of infection, but most commonly seen as osteomyelitis, synovitis, lymphadenitis, soft tissue infections, cutaneous disease, peritonitis, and meningitis [23]. Disseminated disease results in the most serious cases, and while the overall occurrence of disseminated cases appears <1% [24], the high-risk population could be as high as 15% [25]. High-risk population includes exogenous immunosuppression (i.e., steroids and biologics), pregnancy, certain racial/ethical groups, and specific genetic defects within the IL-12/IFN-γ axis and STAT3-mediated pathway (the last appears to be essential in the immune response against CM) [26]. Meningitis-associated disease includes some of the worst clinical scenarios, occurring in nearly one-half of cases of disseminated disease, and may appear rarely years after primary infection [27].
Even with the high occurrence of manageable disease, CM cost remains substantial. Almost 75% of patients miss work or school due to infection and 40% require hospitalization [16]. In California, the estimated total costs consist of $429 million in direct and $271 million in indirect cost for a lifetime of cases reported each year [28]. A projected financial burden tied to climate projections illustrated the potential financial impact of the disease [29]. The estimated current annual medical costs, lost income, and economic welfare losses in the United States are as high as $400,000 per case, and the annual average total cost is $3.9 billion per year. In addition, the total annual burden can increase up to 164% by year 2050 and up to 380% by 2090 when higher greenhouse gas predictions and population growth estimates are included.
It has been observed that changing climate can affect the ability of fungi to cause harm, growth in the areas of concern, and prevalence of the afflicting fungi [30]. A specific example is Candida auris, first identified as a drug-resistant fungus in 2009 [31]. The researchers proposed that, among other factors driving its ability to thrive, the increasing temperature associated with climate change select for fungi which are more tolerant of higher temperatures. Therefore, the fungi become better suited for the body of a human host. Climate concerns appear to be important for CM as well. Recent analysis suggested remapping the area stricken with endemic fungal infections associated with CM in addition to histoplasmosis, blastomycosis, paracoccidioidomycosis, and talaromycosis [32]. The authors ascribe the change to climate change, in addition to other hypothesized global factors of agricultural techniques, occupational hazard, forest erosion, human migrating patterns, and soil dispersion, medical aspects of immune suppressants, higher disease recognition, and better diagnostic tests. Another study suggested an increasing impact of climate change in CM infections in California [33]. To compound the problem, research suggested communicating climate and CM dynamics can be difficult in the state, partly due to political views in areas heavily impacted by CM correlating with climate change denialism [34]. In a series of primary cutaneous CM cases, the authors linked their occurrences in Southern California to climate change [35]. The cases of note happened after an extended drought period followed by heavy rainfall in areas of Orange County in 2016 and early 2017, a place not associated with the endemic disease. The authors concluded that the unusual weather pattern was the culprit for the infections, as it has been demonstrated previously how robust C. immitis can be in drought epochs in comparison to other fungi [36]. Doctors at the University of California San Francisco reported a similar circumstance of increased CM diagnoses around the same time, mentioning the largest amount of CM diagnoses in the state since 1995 per the CA Department of Health [37]. Combined climate and mammalian reservoir modelling, specifically rodents, concluded a future increase in habitat suitability for the Coccidioides spp. [36]. A recent climate projection analysis by Gorris et al. [38] painted a significant increase in the temperature of a suitable climate for Coccidioides residency in the United States in addition to increased case occurrence. The study found that climate patterns would increase the regions affected by CM northward by 2100 into the states of North Dakota, South Dakota, Idaho, Wyoming, Montana, and Nebraska, in addition to yearly CM case counts by 50%. Projections for CM would not be complete without mentioning recent statistical reports published to predict future caseloads [39].
With the uptrend in cannabis legalization in the United States over the past decades [40], it is important to assess its impact on the incidence of fungal infections, including CM. Many who use marijuana for medicinal purposes do so under a potentially immunocompromised situation, such as for pain, nausea relief, and/or appetite stimulation due to cancer, transplant, or HIV [41]. These circumstances leave the patient susceptible to many types of infections, including those linked to fungal contamination in cannabis [42].
3. Diagnosis
Initial diagnosis of CM based on the signs and symptoms proves to be an issue because of its similarity to other lung diseases. Many people infected with CM have no or minimal symptoms, including mild to severe respiratory symptoms, joint pain, malaise, fatigue, and fever. If symptoms occur, they usually can be observed one to three weeks after exposure and can last from a few weeks to a few months. Patients infected with CM have a mild respiratory illness with infiltrates or can have pulmonary disease presenting as nodules, cavities, or fibrocaviatary disease. In immunocompromised or otherwise healthy but genetically predisposed patients, CM can present as disseminated disease [26][43]. Recently published cases with atypical presentations provided evidence of further diagnostic complications, and this included initial mimicry for testicular cancer [44], rare aortic infection [45], polyarticular septic arthritis [46], CM of the vocal cords [47], and septic shock with multiorgan failure [48]. A study by Pu et al. [49] assessed delayed CM diagnosis and utilized CM cases over three years within a large Arizona health care system. The group implemented a diagnostic manual to overtly assist primary, urgent, and emergency healthcare providers in detecting CM, employing data from two years prior and one year after the implementation. Overall, 72.9% of diagnoses were made during hospital admission, 21.7% in ambulatory clinics, 3.2% in emergency units, and 0.5% in urgent care units. The study concluded that a large number of hospital admissions, attendant costs, and unneeded antibacterial drugs would have been avoided if improvements could be made to initially diagnose the disease. The implemented program resulted in increase of positive tests, but the modest outcomes suggest that an alternative method may be better for improving the timing of initial diagnosis.
Another aspect of diagnosis centers upon the correct tools to ensure accurate CM identification. Historically, antibody testing remains the mainstay of CM diagnosis, with research aimed towards perfecting the test in addition to other tools such as PCR and antigen testing [50][51]. A report by Kassis et al. [52] is a retroactive study that was performed to evaluate a combined antigen and antibody testing for progressive pulmonary and disseminated CM. Testing for antigens, a method first introduced in 2007, may provide better sensitivity in situations where antibody testing fails [51]. The study assessed the antibody, serum antigen, and urine antigen testing and concluded the most accurate diagnosis consisted of a combination of all the above rather than each alone or other combinations of assessment. The entry ultimately highlights the need for further research for better protocols in diagnostic accuracy.
4. Currently Approved Drugs
A variety of compounds relevant in CM therapy at various levels of pharmaceutical development and targeting various pathways are known (Figure 3 and Figure 4). Current recommendations by the Infectious Diseases Society of America (IDSA) for antifungal treatment of CM consist of fluconazole or itraconazole as initial therapy and amphotericin B (AmB) for disease of a worse prognosis [53]. The evidence-based treatment guidelines for CM from the IDSA consist of a lower-quality variety when assessed on the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) scale [54]. Present FDA labeling reflects the statement, with the FDA citing only preclinical evidence for AmB usage in CM, while not mentioning the disease with fluconazole and itraconazole [55][56][57].
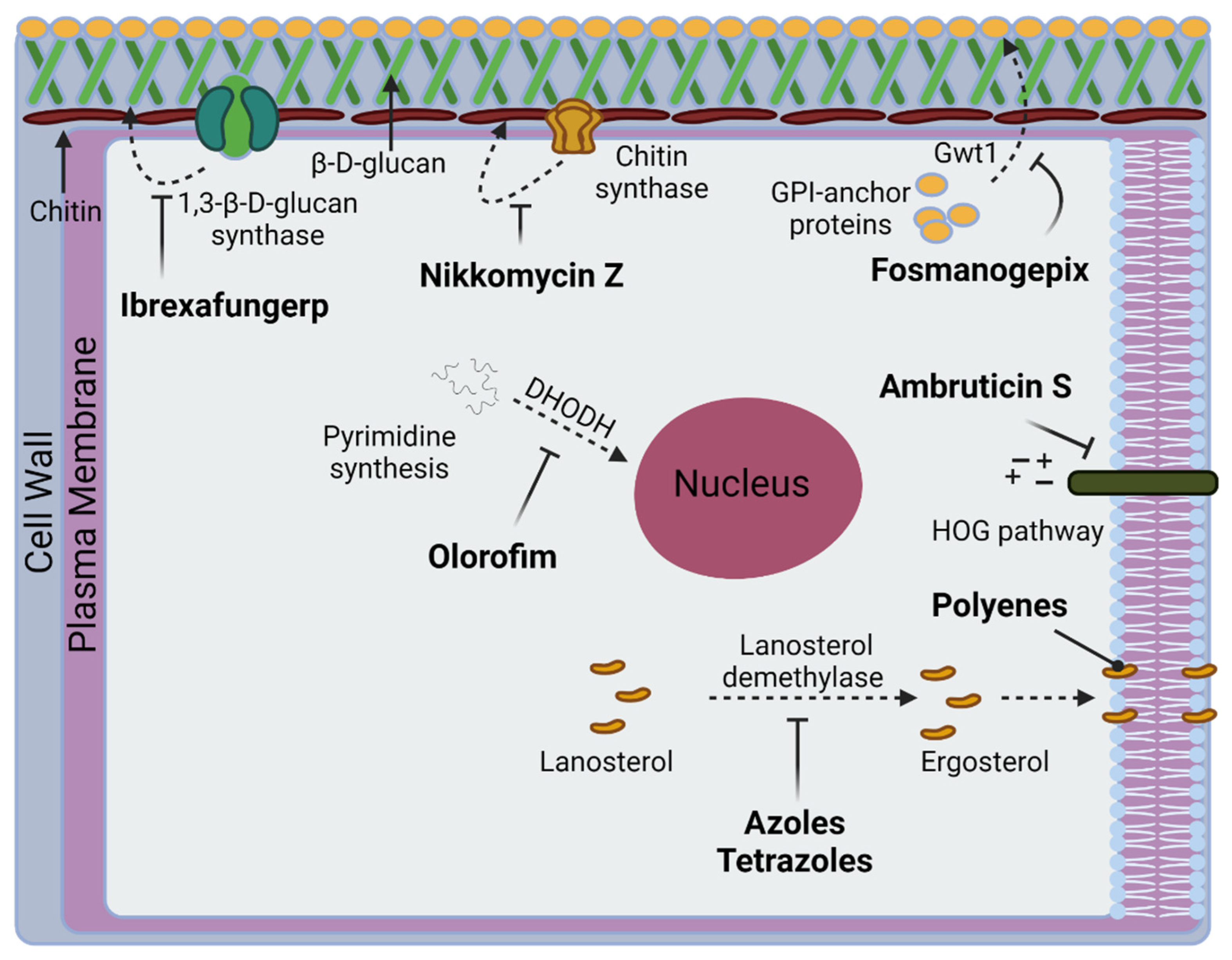
Figure 3. Fungal targets relevant to CM in current treatment, clinical trials, or preclinical development.
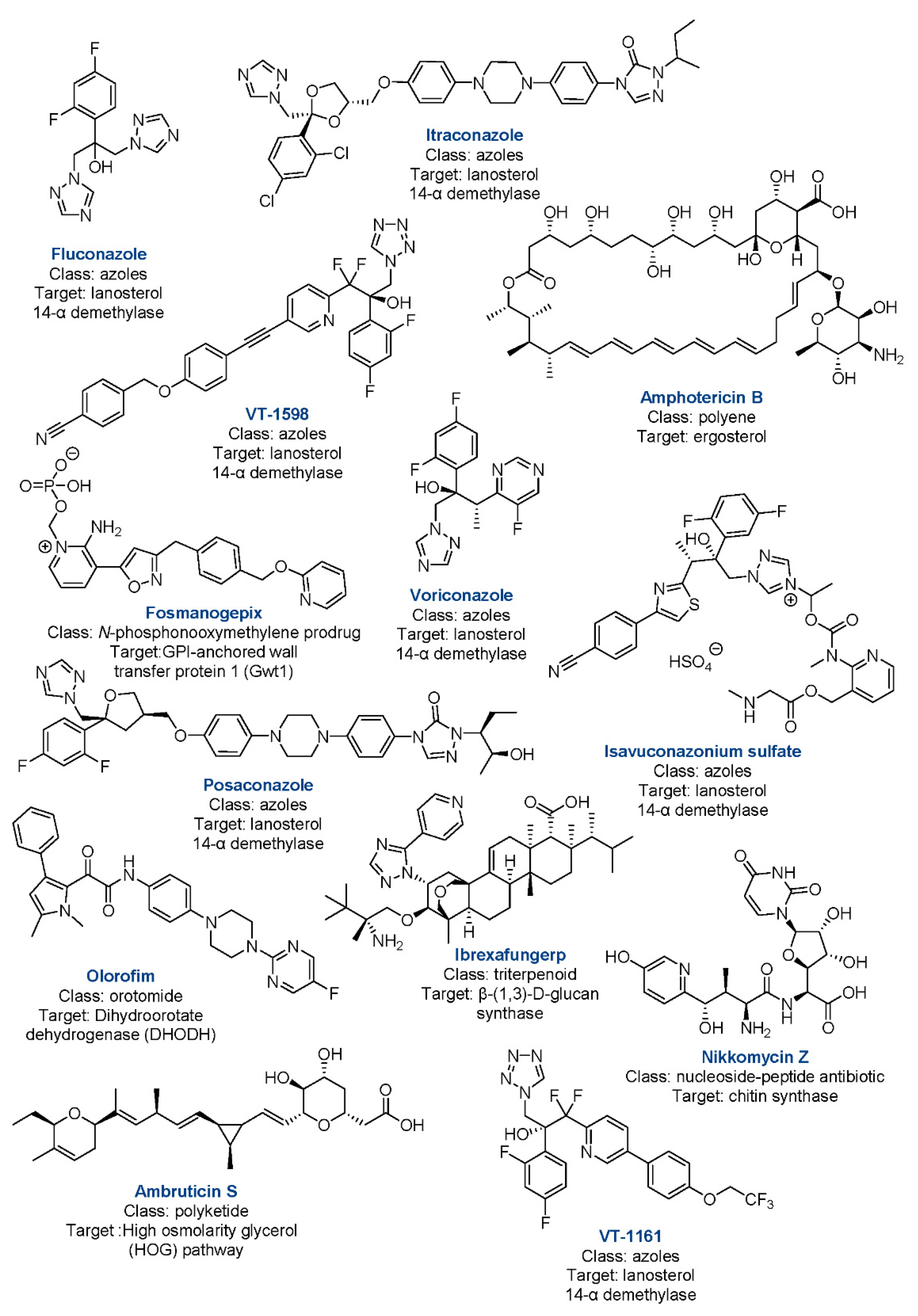
Figure 4. Drugs relevant to CM in current treatment, clinical trials, or preclinical development with class and targets.
A. Azoles. The azole drugs act by inhibiting 14-α-demethylation of the CYP51 enzyme (present in humans and in the fungi), foiling the conversion of lanosterol to ergosterol [58]. Many adverse effects of azoles can be contributed to cross-inhibition of human enzymes such as CYP3A4, 2C9, and 2C19—all of which extensively metabolize other medications [58]. Furthermore, teratogenicity of this class of drugs can be contributed to CYP51 inhibition, leading to the recommendation of avoiding treatments in the first trimester of pregnancy [59]. Typically, first-line therapy consists of oral daily doses for patients with normal renal function [53]. Therapy may become prolonged or lifelong depending on the patient’s disease burden, clinical response, and host immune factors, with xerosis, alopecia, and fatigue being the most common adverse reactions [60]. Daily doses of itraconazole as the initial therapy are also recommended. However, sufficient absorption and increased chance of additional drug–drug interactions compared to fluconazole may be of concern [60].
Questions with respect to how best utilize additional azoles remain minimally answered, particularly in the face of evidence suggesting resistance to the first-line fluconazole [61]. Traditionally reserved for salvage therapy, voriconazole and posaconazole possess some positive evidence in the disease; however, no randomized controlled clinical trials addressing CM exist [58]. Both compounds have their limitations, with voriconazole demonstrating drug–drug interactions, bioavailability issues, and long term toxicity concerns, whereas posaconazole possesses poor CNS penetration and no proven clinical advantage compared to the less costly fluconazole and itraconazole [58]. More recent attempts were made to better understand the potential role of isavuconazonium sulfate (isavusulf) against CM. Isavusulf, a prodrug formulation of isavuconazole, is a second-generation triazole with activity against a broad spectrum of clinically important fungi [62]. Isavuconazole demonstrated potent in vitro activity against clinical isolates of Coccidioides [63]. Furthermore, a previous series of nine patients demonstrated improvement utilizing the drug as salvage therapy in refractory disseminated CM [64]. In a study by Kovanda et al., the researchers highlighted the lack of experimental modeling in isavuconazole in addition to recommended antifungals for CM [65]. This work attempted to address the problem by creating survival and pharmacodynamic-pharmacokinetic (PD-PK) murine models utilizing isavulsulf, fluconazole, and no treatment groups. The study demonstrated that isavulsulf and fluconazole caused a significant reduction in fungal burden in mice compared to the no treatment control in a dose-dependent manner. They also demonstrated that increasing exposure to the drugs resulted in decrease in fungal burden over time in a PK-PD model. In the end, the study provides much needed data in a preclinical CM experimental model that can guide future developments.
References
- Brown, J.; Benedict, K.; Park, B.J.; Thompson, G.R., 3rd. Coccidioidomycosis: Epidemiology. Clin. Epidemiol. 2013, 5, 185–197.
- Park, J.; Chaffee, A.W.; Harrigan, R.J.; Schoenberg, F.P. A non-parametric Hawkes model of the spread of Ebola in west Africa. J. Appl. Stat. 2020, 49, 621–637.
- Posadas, A. Un nuevo caso de micosis fungoidea con posrospemias. Ann. Cir. Med. Argent 1892, 15, 585–597.
- Fisher, M.C.; Koenig, G.L.; White, T.J.; Taylor, J.W. Molecular and phenotypic description of Coccidioides posadasii sp. nov., previously recognized as the non-California population of Coccidioides immitis. Mycologia 2002, 94, 73–84.
- Bajwa, A.K.; Rongkavilit, C. Update on Coccidioidomycosis in the United States and Beyond. Glob. Pediatr. Health 2020, 7, 2333794x20969282.
- Laniado-Laborín, R.; Arathoon, E.G.; Canteros, C.; Muñiz-Salazar, R.; Rendon, A. Coccidioidomycosis in Latin America. Med. Mycol. 2019, 57, S46–S55.
- Morais, J.; Borges, M.C.M.; Cavalcante, L.; Motoyama, P.V.P.; Libório, M.P.; Távora, L.G.F. Coccidioidomycosis in a reference center in Northeast Brazil: Clinical/epidemiological profile and most common radiological findings. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200249.
- Lockhart, S.R.; Toda, M.; Benedict, K.; Caceres, D.H.; Litvintseva, A.P. Endemic and Other Dimorphic Mycoses in The Americas. J. Fungi 2021, 7, 151.
- Huppert, M.; Sun, S.H.; Harrison, J.L. Morphogenesis throughout saprobic and parasitic cycles of Coccidioides immitis. Mycopathologia 1982, 78, 107–122.
- Nguyen, C.; Barker, B.M.; Hoover, S.; Nix, D.E.; Ampel, N.M.; Frelinger, J.A.; Orbach, M.J.; Galgiani, J.N. Recent advances in our understanding of the environmental, epidemiological, immunological, and clinical dimensions of coccidioidomycosis. Clin. Microbiol. Rev. 2013, 26, 505–525.
- Sharpton, T.J.; Stajich, J.E.; Rounsley, S.D.; Gardner, M.J.; Wortman, J.R.; Jordar, V.S.; Maiti, R.; Kodira, C.D.; Neafsey, D.E.; Zeng, Q.; et al. Comparative genomic analyses of the human fungal pathogens Coccidioides and their relatives. Genome Res. 2009, 19, 1722–1731.
- Taylor, J.W.; Barker, B.M. The endozoan, small-mammal reservoir hypothesis and the life cycle of Coccidioides species. Med. Mycol. 2019, 57, S16–S20.
- Shubitz, L.E.; Butkiewicz, C.D.; Dial, S.M.; Lindan, C.P. Incidence of coccidioides infection among dogs residing in a region in which the organism is endemic. J. Am. Vet. Med. Assoc. 2005, 226, 1846–1850.
- Shubitz, L.F. Comparative aspects of coccidioidomycosis in animals and humans. Ann. N. Y. Acad. Sci. 2007, 1111, 395–403.
- Wilson, L.; Ting, J.; Lin, H.; Shah, R.; MacLean, M.; Peterson, M.W.; Stockamp, N.; Libke, R.; Brown, P. The Rise of Valley Fever: Prevalence and Cost Burden of Coccidioidomycosis Infection in California. Int. J. Environ. Res. Public Health 2019, 16, 1113.
- Increase in reported coccidioidomycosis—United States, 1998–2011. MMWR Morb. Mortal. Wkly. Rep. 2013, 62, 217–221.
- Oltean, H.N.; Springer, M.; Bowers, J.R.; Barnes, R.; Reid, G.; Valentine, M.; Engelthaler, D.M.; Toda, M.; McCotter, O.Z. Suspected Locally Acquired Coccidioidomycosis in Human, Spokane, Washington, USA. Emerg. Infect. Dis. 2020, 26, 606–609.
- Johnson, S.M.; Carlson, E.L.; Fisher, F.S.; Pappagianis, D. Demonstration of Coccidioides immitis and Coccidioides posadasii DNA in soil samples collected from Dinosaur National Monument, Utah. Med. Mycol. 2014, 52, 610–617.
- Yoo, S.D.; Lusiba, J.K.; Lukande, R.; Shin, K. Disseminated Coccidioidomycosis in Africa. Eur. J. Case Rep. Intern. Med. 2020, 7, 001659.
- Hernandez, H.; Erives, V.H.; Martinez, L.R. Coccidioidomycosis: Epidemiology, Fungal Pathogenesis, and Therapeutic Development. Curr. Trop. Med. Rep. 2019, 6, 132–144.
- Huang, J.Y.; Bristow, B.; Shafir, S.; Sorvillo, F. Coccidioidomycosis-associated Deaths, United States, 1990–2008. Emerg. Infect. Dis. 2012, 18, 1723–1728.
- Valdivia, L.; Nix, D.; Wright, M.; Lindberg, E.; Fagan, T.; Lieberman, D.; Stoffer, T.; Ampel, N.M.; Galgiani, J.N. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg. Infect. Dis. 2006, 12, 958–962.
- Johnson, R.H.; Sharma, R.; Kuran, R.; Fong, I.; Heidari, A. Coccidioidomycosis: A review. J. Investig. Med. 2021, 69, 316–323.
- Galgiani, J.N.; Ampel, N.M.; Blair, J.E.; Catanzaro, A.; Johnson, R.H.; Stevens, D.A.; Williams, P.L. Coccidioidomycosis. Clin. Infect. Dis. 2005, 41, 1217–1223.
- Johnson, R.; Caldwell, J.; Welch, G.; Einstein, H. The great coccidioidomycosis epidemic: Clinical features. In Proceedings of the Coccidioidomycosis: Fifth International Conference; National Foundation for Infectious Diseases: Washington, DC, USA, 1996.
- Odio, C.D.; Marciano, B.E.; Galgiani, J.N.; Holland, S.M. Risk Factors for Disseminated Coccidioidomycosis, United States. Emerg. Infect. Dis. 2017, 23, 308–311.
- Goldstein, E.J.C.; Johnson, R.H.; Einstein, H.E. Coccidioidal Meningitis. Clin. Infect. Dis. 2006, 42, 103–107.
- McCotter, O.Z.; Benedict, K.; Engelthaler, D.M.; Komatsu, K.; Lucas, K.D.; Mohle-Boetani, J.C.; Oltean, H.; Vugia, D.; Chiller, T.M.; Sondermeyer Cooksey, G.L.; et al. Update on the Epidemiology of coccidioidomycosis in the United States. Med. Mycol. 2019, 57, S30–S40.
- Gorris, M.E.; Neumann, J.E.; Kinney, P.L.; Sheahan, M.; Sarofim, M.C. Economic Valuation of Coccidioidomycosis (Valley Fever) Projections in the United States in Response to Climate Change. Weather Clim. Soc. 2021, 13, 107–123.
- Gnat, S.; Łagowski, D.; Nowakiewicz, A.; Dyląg, M. A global view on fungal infections in humans and animals: Infections caused by dimorphic fungi and dermatophytoses. J. Appl. Microbiol. 2021, 131, 2688–2704.
- Casadevall, A.; Kontoyiannis, D.P.; Robert, V. On the Emergence of Candida auris: Climate Change, Azoles, Swamps, and Birds. mBio 2019, 10, e01397-19.
- Ashraf, N.; Kubat, R.C.; Poplin, V.; Adenis, A.A.; Denning, D.W.; Wright, L.; McCotter, O.; Schwartz, I.S.; Jackson, B.R.; Chiller, T.; et al. Re-drawing the Maps for Endemic Mycoses. Mycopathologia 2020, 185, 843–865.
- Pearson, D.; Ebisu, K.; Wu, X.; Basu, R. A Review of Coccidioidomycosis in California: Exploring the Intersection of Land Use, Population Movement, and Climate Change. Epidemiol. Rev. 2019, 41, 145–157.
- Matlock, M.; Hopfer, S.; Ogunseitan, O.A. Communicating Risk for a Climate-Sensitive Disease: A Case Study of Valley Fever in Central California. Int. J. Environ. Res. Public Health 2019, 16, 3254.
- Shiu, J.; Thai, M.; Elsensohn, A.N.; Nguyen, N.Q.; Lin, K.Y.; Cassarino, D.S. A case series of primary cutaneous coccidioidomycosis after a record-breaking rainy season. JAAD Case Rep. 2018, 4, 412–414.
- Zender, C.S.; Talamantes, J. Climate controls on valley fever incidence in Kern County, California. Int. J. Biometeorol. 2006, 50, 174–182.
- Coates, S.J.; Fox, L.P. Disseminated coccidioidomycosis as a harbinger of climate change. JAAD Case Rep. 2018, 4, 424–425.
- Gorris, M.E.; Treseder, K.K.; Zender, C.S.; Randerson, J.T. Expansion of Coccidioidomycosis Endemic Regions in the United States in Response to Climate Change. Geohealth 2019, 3, 308–327.
- Wang, J.; Harrigan, R.J.; Schoenberg, F.P. Point Process Models for the Spread of Coccidioidomycosis in California. Infect. Dis. Rep. 2021, 13, 52.
- Mitchell, W.; Bhatia, R.; Zebardast, N. Retrospective cross-sectional analysis of the changes in marijuana use in the USA, 2005–2018. BMJ Open 2020, 10, e037905.
- McHardy, I.; Romanelli, A.; Harris, L.J.; Opp, G.; Gaudino, R.; Torres, A.; Polage, C.R.; Tuscano, J.M.; Thompson, G.R., 3rd. Infectious risks associated with medicinal Cannabis: Potential implications for immunocompromised patients? J. Infect. 2018, 76, 500–501.
- Shapiro Bb Md, M.P.H.; Hedrick, R.; Vanle, B.C.; Becker, C.A.; Nguyen, C.; Underhill, D.M.; Morgan, M.A.; Kopple, J.D.; Danovitch, I.; IsHak, W.W. Cryptococcal meningitis in a daily cannabis smoker without evidence of immunodeficiency. BMJ Case Rep. 2018, 2018, bcr-2017.
- Akram, S.M.; Koirala, J. Coccidioidomycosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021.
- Balderas-Sosa, E.Y.; De la Torre, J.L.; Soualhi, A.; Leyva-Moraga, F.A.; Leyva-Moraga, F.; Leyva-Moraga, E. Coccidioidomycosis mimicking testicular cancer: A case report. Andrologia 2021, 53, e14151.
- Huang, J.; Cano, E.J.; Shweta, F.; Shah, A.S.; Schuetz, A.N.; Bois, M.; Gurram, P.R. Infected Aneurysm of the Native Aorta due to Coccidioides posadasii. Open Forum Infect. Dis. 2021, 8, ofab266.
- Nasrawi, F.; Heidari, A.; Aljashamy, T.; Mangat, N.; Bhaika, J.; Kaur, S.; Kuran, R.; Johnson, R. Disseminated Coccidioidomycosis Presenting as Polyarticular Septic Arthritis: A Case Report. J. Investig. Med. High Impact Case Rep. 2020, 8, 2324709620974894.
- Converse, C.; Dey, A.; Decker, S.; Arabian, S.; Neeki, M. Coccidioidomycosis of the Vocal Cords Presenting in Sepsis: A Case Report and Literature Review. Case Rep. Crit. Care 2020, 2020, 8025391.
- Aduroja, O.; Okudo, J.; Padilla, A. Disseminated Coccidioidomycosis Presenting as Septic Shock with Multiorgan Failure. Case Rep. Infect. Dis. 2021, 2021, 8837493.
- Pu, J.; Donovan, F.M.; Ellingson, K.; Leroy, G.; Stone, J.; Bedrick, E.; Galgiani, J.N. Clinician Practice Patterns that Result in the Diagnosis of Coccidioidomycosis Before or During Hospitalization. Clin. Infect. Dis. 2020, 73, e1587–e1593.
- Durkin, M.; Connolly, P.; Kuberski, T.; Myers, R.; Kubak, B.M.; Bruckner, D.; Pegues, D.; Wheat, L.J. Diagnosis of Coccidioidomycosis with Use of the Coccidioides Antigen Enzyme Immunoassay. Clin. Infect. Dis. 2008, 47, e69–e73.
- Saubolle, M.A. Laboratory Aspects in the Diagnosis of Coccidioidomycosis. Ann. N. Y. Acad. Sci. 2007, 1111, 301–314.
- Kassis, C.; Durkin, M.; Holbrook, E.; Myers, R.; Wheat, L. Advances in Diagnosis of Progressive Pulmonary and Disseminated Coccidioidomycosis. Clin. Infect. Dis. 2020, 72, 968–975.
- Galgiani, J.N.; Ampel, N.M.; Blair, J.E.; Catanzaro, A.; Geertsma, F.; Hoover, S.E.; Johnson, R.H.; Kusne, S.; Lisse, J.; MacDonald, J.D.; et al. 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis. Clin. Infect. Dis. 2016, 63, e112–e146.
- Greiner, B.; Essex, R.; Wheeler, D. An analysis of research quality underlying IDSA clinical practice guidelines: A cross-sectional study. J. Osteopath. Med. 2021, 121, 319–323.
- DIFLUCAN (Fluconazole). New York, New York: Pfizer. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/019949s051lbl.pdf (accessed on 24 February 2022).
- Amphotericin, B. Big Flats, NY: X-Gen Pharmaceuticals, Inc. Available online: http://xgenpharmadjb.com/wp-content/uploads/sites/21/2021/12/ampho.pdf. (accessed on 24 February 2022).
- SPORANOX (Itraconazole). Raritan, NJ: Ortho-McNeil-Janssen Pharmaceuticals, Inc. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/020083s063lbl.pdf (accessed on 24 February 2022).
- Thompson, G.R., III; Lewis, J.S., II; Nix, D.E.; Patterson, T.F. Current Concepts and Future Directions in the Pharmacology and Treatment of Coccidioidomycosis. Med. Mycol. 2019, 57, S76–S84.
- Bercovitch, R.S.; Catanzaro, A.; Schwartz, B.S.; Pappagianis, D.; Watts, D.H.; Ampel, N.M. Coccidioidomycosis During Pregnancy: A Review and Recommendations for Management. Clin. Infect. Dis. 2011, 53, 363–368.
- Davis, M.R.; Nguyen, M.-V.H.; Donnelley, M.A.; Thompson, G.R., III. Tolerability of long-term fluconazole therapy. J. Antimicrob. Chemother. 2018, 74, 768–771.
- Thompson, G.R.; Barker, B.M.; Wiederhold, N.P. Large-Scale Evaluation of In Vitro Amphotericin B, Triazole, and Echinocandin Activity against Coccidioides Species from U.S. Institutions. Antimicrob. Agents Chemother. 2017, 61, e02634-02616.
- Decembrino, N.; Perruccio, K.; Zecca, M.; Colombini, A.; Calore, E.; Muggeo, P.; Soncini, E.; Comelli, A.; Molinaro, M.; Goffredo, B.M.; et al. A Case Series and Literature Review of Isavuconazole Use in Pediatric Patients with Hemato-oncologic Diseases and Hematopoietic Stem Cell Transplantation. Antimicrob. Agents Chemother. 2020, 64, e01783-01719.
- Thompson, G.R., 3rd; Wiederhold, N.P. Isavuconazole: A comprehensive review of spectrum of activity of a new triazole. Mycopathologia 2010, 170, 291–313.
- Heidari, A.; Quinlan, M.; Benjamin, D.J.; Laurence, B.; Mu, A.; Ngai, T.; Hoffman, W.J.; Cohen, S.H.; McHardy, I.; Johnson, R.; et al. Isavuconazole in the Treatment of Coccidioidal Meningitis. Antimicrob. Agents Chemother. 2019, 63, e02232-02218.
- Kovanda, L.L.; Sass, G.; Martinez, M.; Clemons, K.V.; Nazik, H.; Kitt, T.M.; Wiederhold, N.; Hope, W.W.; Stevens, D.A. Efficacy and Associated Drug Exposures of Isavuconazole and Fluconazole in an Experimental Model of Coccidioidomycosis. Antimicrob. Agents Chemother. 2021, 65, e02344-02320.
More
Information
Subjects:
Mycology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
2.4K
Revisions:
4 times
(View History)
Update Date:
22 Apr 2022
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No